
Abstract
Cancer survivors often face persistent abdominal pain, necessitating optimal pain management. While celiac plexus block (CPB) and botulinum toxin (BT) injection are viable options, traditional methods may encounter challenges due to patient-specific concerns and anatomical complexities. Here, the case of a cancer survivor in his 70 s experiencing recurrent abdominal pain, who declined conventional percutaneous CPB approaches due to anxiety related to aortic puncture, is presented. Following a pancreaticoduodenectomy, the patient developed chronic abdominal pain attributed to adhesions leading to small bowel obstruction. Concurrently, there was notable psychological distress, including anxiety, depression, and heightened concerns regarding tumor recurrence. Considering the patient’s specific concerns, a right-sided unilateral retrocrural single-needle technique was proposed, aimed at alleviating pain, while avoiding conventional CPB approaches. Initial right-sided retrocrural CPB offered short-term relief, prompting a subsequent BT injection using the same approach. Following BT injection, the patient reported significant and sustained pain reduction (from 8 to 1 on an 11-point numerical rating scale) at both 12 and 20 weeks post-procedure. Right-sided retrocrural BT injection offers an alternative approach, addressing patient concerns and demonstrating prolonged pain relief. This may benefit cancer survivors with upper abdominal pain, emphasizing the importance of personalized and innovative pain management strategies.
Keywords
Introduction
Celiac plexus block (CPB) is considered a reliable interventional treatment option for pain management in patients with refractory epigastric pain. 1 Celiac plexus block can be performed using an endoscopic ultrasound-guided technique or through a percutaneous approach guided by computed tomography (CT) or fluoroscopy. 2 Two primary techniques are used In percutaneous CPB using fluoroscopy approaching from the patient’s posterior side: the trans-aortic approach, which targets the celiac plexus in front of the aorta, and the retrocrural approach, focusing on the bilateral splanchnic nerves. 3 Although the transaortic approach through the aorta can be performed without side effects in patients who do not have a bleeding tendency, 3 it may provoke anxiety in some patients due to it passing through the aorta itself. In response to these concerns, a right-sided approach has been developed to avoid the aorta, using a unilateral retrocrural single-needle guided technique. 4
The population of individuals who have emerged as cancer survivors is steadily increasing, with an annual growth rate exceeding 3%. 5 However, this growing cohort of survivors encounters multiple challenges associated with chronic disease management, particularly for chronic pain. 5 The incidence of chronic pain in cancer survivors is nearly two-fold higher than that found in the general population, with rates of 30.8% versus 15.7%, respectively. 6 The increased prevalence of chronic pain among cancer survivors is known to be associated with psychological factors, including depression and anxiety. 6 Therefore, managing chronic pain in cancer survivors necessitates a comprehensive approach, encompassing physical treatments, such as medication and interventional procedures, and also addressing psychological factors. 7
Botulinum toxin (BT) is a well-established therapeutic protein known for its ability to inhibit neurotransmitter release from presynaptic membranes. 8 Apart from its cosmetic applications, it is widely used to treat various pain conditions, such as chronic migraine, chronic low back pain, myofascial pain, and various neuropathic pain syndromes. 9 In particular, BT injection into the sympathetic ganglia has been reported to provide long-term pain relief compared with local anesthetic blocks.10,11 Cho et al., 12 reported that the retrocrural approach for BT injection resulted in long-term pain relief for severe chronic pancreatitis-induced chronic pain. However, to the best of our knowledge, there are no reports on the effectiveness of BT injections using a right-sided unilateral retrocrural single-needle technique for abdominal pain relief. Therefore, the present aim was to report the effects of BT using this technique, particularly with relevance to persistent abdominal pain in cancer survivors.
Case report
In October 2015, a male patient in his 70 s diagnosed with cancer of the ampulla of Vater underwent pancreaticoduodenectomy. Postoperatively, the patient received concurrent chemoradiotherapy and experienced recurrent severe upper abdominal pain, resulting in a diagnosis of adhesive ileus in 2016, 2017, and 2022. Conservative management and antibiotic therapy were administered during a 4-day inpatient stay after the 2016 episode. The patient experienced chronic right upper abdominal pain from 2016, leading to multiple emergency department admissions. In September 2022, he required a week of inpatient care due to recurrent abdominal pain accompanied by nausea and vomiting. Throughout this period, the patient experienced persistent anxiety, depression, and concerns regarding tumor recurrence.
In April 2023, the patient presented at a tertiary hospital pain center in an East Asian country, seeking treatment for refractory right upper abdominal pain that had progressively worsened over the past year. On the 11-point numerical rating scale (NRS), the patient reported a pain score of 8. Abdominal CT revealed small bowel obstruction attributable to adhesions in the anterior abdominal wall, with preservation of bowel enhancement and no tumor recurrence (Figure 1).
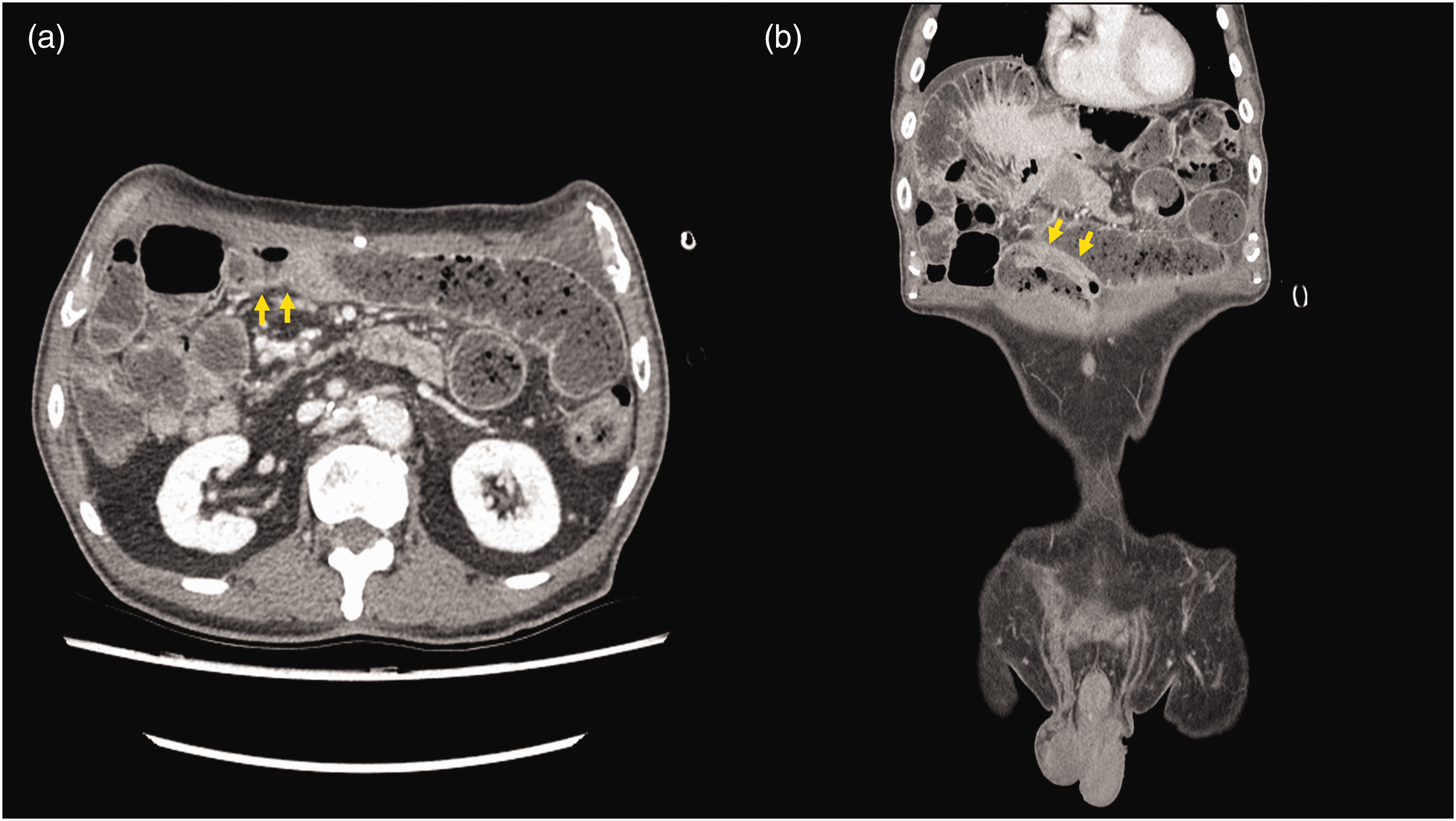
Abdominal computed tomography in a patient in his 70 s with a history of pancreaticoduodenectomy for ampullary cancer, who presented with refractory right upper abdominal pain, before celiac plexus block, showing small bowel obstruction attributable to adhesions at the anterior abdominal wall and bowel obstruction transition point (yellow arrow), with preservation of bowel enhancement: (a) transverse view; and (b) coronal view.
The medications prescribed by the surgical department included 200 mg trimebutine maleate, orally, three times daily; 500 mg Bacillus subtilis culture, orally, once daily; 160 mg phloroglucinol hydrate, orally, once daily; and 30 mg motilitone, orally, three times daily. The patient’s medication regimen did not provide pain relief, and due to concerns regarding side-effects, such as abdominal discomfort, the patient refused analgesics. Consequently, the patient was informed of percutaneous CPB procedural treatment options for pain control. However, he declined the transaortic approach because of concerns regarding aortic puncture. Similarly, the patient expressed concerns regarding the retrocrural approach due to the possibility of the needle inserted from the left side puncturing the aorta. The patient reported that there was no abdominal pain on the left side and expressed a strong preference for a CPB approach from the right side only. Considering the CT findings showing significant leftward deviation of the abdominal aorta and prior reports of CPB using a right-sided unilateral approach, treatment with CPB using a right-sided unilateral retrocrural single-needle technique was planned (Figure 2a).
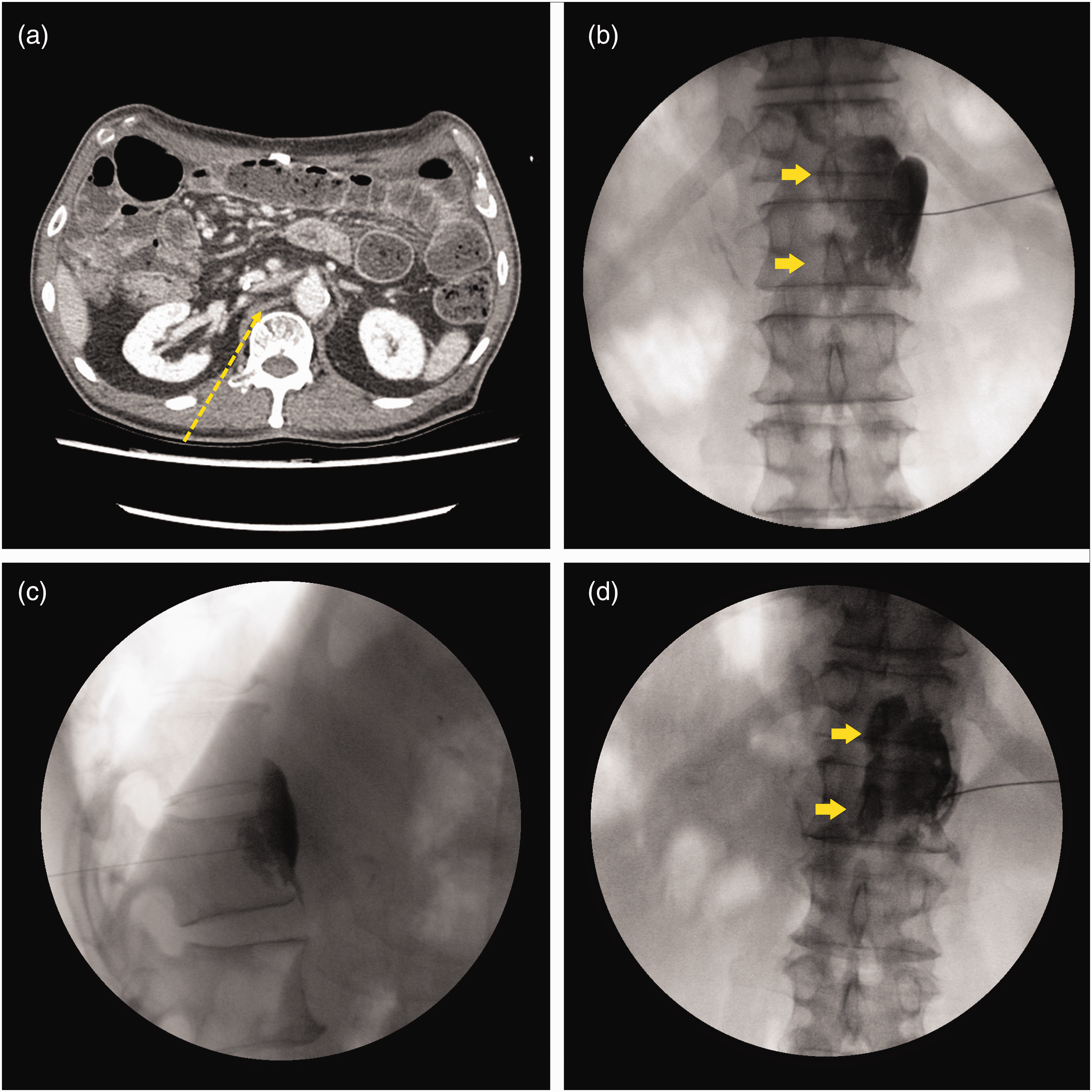
Abdominal computed tomography (CT) in a patient in his 70 s with a history of pancreaticoduodenectomy for ampullary cancer, who presented with refractory right upper abdominal pain, showing: (a) planning of needle insertion point, approach angle, distance to target point using CT; (b) fluoroscopic anteroposterior view after contrast media injection before botulinum toxin injection (contrast media spread to contralateral side, yellow arrow); (c) fluoroscopic lateral view after contrast media injection; and (d) fluoroscopic anteroposterior view after contrast injection. Contrast has flowed into the contralateral one-third of the vertebral body (yellow arrow).
With the patient in the prone position with sterile draping, the needle entry site was anesthetized using 5 ml of 1% lidocaine. A pain specialist (JK) inserted a 22-gauge Chiba needle into the right-sided retrocrural space, targeting the upper level of the L1 vertebra. Needle placement accuracy was confirmed under fluoroscopic guidance. To verify the anatomical extent of local anesthetic spread, 3 ml of radiographic contrast medium was injected, showing contrast dispersion within the ipsilateral retrocrural space and the anterior central region of the vertebral body. Subsequently, 4 ml each of 2% lidocaine and 0.75% ropivacaine were administered (Figure 2b). After injection completion, the needle was safely retracted, and no complications occurred. The patient was prescribed 650 mg acetaminophen, orally, and 75 mg tramadol, orally, as needed (maximum acetaminophen daily dose, 1300 mg and maximum tramadol daily dose, 150 mg) for postprocedural pain management.
At the outpatient follow-up 2 weeks after right-sided retrocrural CPB, the patient reported relief from upper abdominal pain for 2 days, followed by its return after 3 days. Considering this recurrence, a decision was made to pursue right celiac plexus neurolysis (CPN; more accurately termed splanchnic nerve neurolysis) for long-term pain relief. However, the patient expressed significant apprehension due to the potential complications associated with neurolytic procedures, including neuritis and erectile dysfunction. 13 Additionally, the patient had alcohol intolerance, a contraindication for ethanol use in CPN. 14 Therefore, based on previous studies demonstrating prolonged pain relief with BT injection targeting sympathetic nerves and prior reports of sustained pain relief with retrocrural BT injection into the celiac plexus,10,11 a BT injection was considered as a suitable alternative to neurolysis. The patient consented to BT injection using the right-sided unilateral retrocrural single-needle technique. The patient was specifically informed of the necessity to lie prone with the needle inserted for approximately 20 min after administration of local anesthetics to assess abdominal pain relief and neurological symptoms before the BT injection. The patient agreed to endure this period, motivated by the previous treatment’s effectiveness and the potential for long-term pain relief. During the procedure, the patient was instructed to inform us immediately of any discomfort or a desire to stop.
In the prone position, sterile draping was applied, and the needle entry site was anesthetized using 5 ml of 1% lidocaine administered with a hypodermic needle. A pain specialist (JK) inserted a 22-gauge Chiba needle into the retrocrural space on the right side, targeting the uppermost level of the L1 vertebra with fluoroscopic guidance to confirm proper needle placement. To assess the anatomical dispersion of local anesthetic, 3 ml of radiographic contrast agent was injected. Following confirmation of contrast diffusion in the ipsilateral retrocrural space and anterior central region of the vertebral body, a mixture of 2% lidocaine (4 ml) and 0.75% ropivacaine (4 ml) was administered (Figure 2c and 2d). After 20 min, with confirmed relief of upper abdominal pain and the absence of motor or sensory deficits, 75 IU of BT type A (Nabota, Daewoong, South Korea) was administered,15,16 and the needle was withdrawn. The patient remained in the prone position for 30 min after the procedure. No complications were observed during the procedure.
At 2 weeks after the right celiac plexus BT injection, the patient reported dramatic improvement in pain, with an 11-point NRS score decreasing from 8 to 1, and no additional medication use. Subsequently, at the 12-week post-procedure outpatient follow-up, the patient indicated that the pain remained well-controlled, with an 11-point NRS score of 1, resulting in an improved quality of life and significant restoration of daily functioning to a level comparable to that before cancer surgery. Furthermore, the patient exhibited effective pain management with a consistently low pain score of 1, which was maintained throughout the 20-week follow-up at the outpatient clinic, indicative of a high level of patient satisfaction.
Ethics statement
This study was approved by the Institutional Review Board of Seoul National University Hospital (IRB No. 2308-066-1457), a tertiary hospital in an East Asian country, and was performed in accordance with the latest version of the Declaration of Helsinki. Written informed consent was obtained from the patient regarding publication of the case report and all accompanying medical images. The reporting of this study conforms to CARE guidelines. 17
Discussion
Celiac plexus block is considered an effective interventional option for patients with upper abdominal pain, including those with cancer.1,4 Although evidence is limited, injecting BT into the celiac plexus may provide long-lasting pain relief. However, such procedures cannot be performed without patient consent. Cancer survivors with chronic abdominal pain often experience unpleasant psychological symptoms, such as anxiety, making it essential to find persuasive and effective methods of treatment. In cancer survivors experiencing persistent upper abdominal pain after surgery coupled with anxiety, such as in the present case, a right-sided unilateral retrocrural approach for CPB may be a promising alternative to reduce the possibility of aortic puncture and alleviate pain. The present report describes the case of a cancer survivor seeking long-term pain relief, in which BT was injected through a right-sided unilateral retrocrural approach, resulting in pain relief lasting up to 20 weeks.
Each CPB approach has inherent advantages and limitations, emphasizing the importance of judicious selection guided by anatomical considerations. When confronted with tumors enveloping the celiac plexus, the classical bilateral retrocrural approach (actually targeting the splanchnic nerve) proves advantageous over other approaches, such as the transaortic approach, as it mitigates the likelihood of trauma to abdominal organs. 18 However, this approach does not mitigate the risks of aortic injury, retroperitoneal hemorrhage, or neurological impairment. 18 In the present study, the patient’s abdominal aorta exhibited a lateralized disposition toward the left, while the retrocrural space on the right exhibited notable expansiveness. Consequently, using a unilateral retrocrural approach offered the potential to achieve effective results while concurrently reducing the risk of aortic and neurological compromise. Alternative techniques, such as the transdiscal approach or reaching the retrocrural space under CT guidance, may also offer potentially safer options. 19 However, the transdiscal approach was not routinely performed at the hospital treating the present case, and the explanation of penetrating the disc may have induced anxiety in this particular patient. Furthermore, procedures guided by CT are primarily conducted by radiologists, whereas in the present hospital, most CPB procedures are performed by pain physicians under fluoroscopy guidance. In analogous studies adopting unilateral techniques, positioning the needle tip at the central axis of the vertebral body facilitated the dispersion of therapeutic agents within the bilateral retrocrural spaces. 20 In the present study, the needle tip was situated medial to the pedicle of L1 on the right side, resulting in a radiographic distribution pattern that extended to approximately one-third of the contralateral aspect of the vertebral body. Anatomically, the splanchnic nerves converge from the lateral aspect of the vertebral body toward the anterior central region, passing through the crus to form the celiac plexus. Consequently, it is plausible that, within the retrocrural space, these nerves tend to be grouped more toward anterior central rather than lateral regions (Figure 3). Therefore, in patients such as described in the present case, where approximately one-third of the contralateral retrocrural space could be covered, approaching from the right side alone may be safe and effective.

Representative computed tomography images from a patient in his 70 s with a history of pancreaticoduodenectomy for ampullary cancer, who presented with refractory right upper abdominal pain, showing: (a) schematic anatomical pathways of the greater, lesser, and least splanchnic nerve (yellow double line) toward the celiac plexus (yellow circle) from the thoracic sympathetic chain (yellow vertical line). Spreading of injectate covering the splanchnic nerves (translucent yellow circle); and (b) transverse cross section of splanchnic nerves at the L1 upper level (yellow stars) and spreading of injectate covering the splanchnic nerves (translucent yellow circle).
While the precise mechanisms behind the pain-relieving effects of BT remain unclear, studies in animal models have shown its ability to inhibit pain mediator release, reduce local inflammation, and suppress sodium channel deactivation. 8 Previously published studies of BT applied to the sympathetic nerve, as in the present case, are summarized in Table 1.11,12,15,16,21–23 As shown in Table 1, both BT type A and type B are viable options; however, only type A was available at the present hospital. Furthermore, most of the summarized studies utilized BT type A, and the only randomized controlled trial among them also used BT type A, 16 which was referenced for determining the dosage in the present case. Although there is limited research in this area, the general consensus suggests that BT injections are effective for pain relief with prolonged effects, thus, the topic of pain relief and long-term maintenance through BT injections in sympathetic nerves warrants further investigation.
Previously published studies of botulinum toxin injections into the sympathetic nervous system.

BT-A, botulinum toxin type A; BT-B, botulinum toxin type B; CP, chronic pancreatitis; CRPS, complex regional pain syndrome; G, group; GIB, ganglion impar block; LSGB, lumbar sympathetic ganglion block; NRS, numerical rating score; RCT, randomized controlled trial; RHTN, resistant hypertension.
Heightened psychological factors, such as anxiety, worry, and depression among cancer survivors contribute to the persistence of chronic pain, 6 which was the case with the patient described in the present report, who frequently visited the emergency room because of abdominal pain. Adhesive ileus was consistently observed in the patient’s CT scans following surgery, and when he presented to the emergency room with worsening abdominal pain, ischemic changes and strangulation were not detected. The patient’s abdominal pain appeared to be more severe than expected based on the objective findings on CT, and the degree of pain worsening did not match the extent of the ileus. Therefore, sympathetic neural pain may have been present in addition to the physiological and psychological factors associated with chronic pain previously described in cancer survivors. Considering a reduced tolerance to pain, cancer survivors may have reservations about taking pain medications that might potentially exacerbate their pain. Interventional therapy may be a favorable option in such cases. As in the present case, utilizing the right-sided unilateral retrocrural approach for BT injection, while reducing the patient’s apprehension toward the procedure, may prove to be an effective treatment option for managing upper abdominal pain in cancer survivors.
The results described in the present study may be limited by several factors. First, depending on the patient, there might be adhesions in the retrocrural space, which may prevent the drug from crossing over to the opposite side. If adhesions are present and the contrast media fails to cross over to the contralateral side, the patient may not achieve sufficient pain relief. In the present case, the observation of contrast media extending beyond the central aspect of the vertebral body suggests potential coverage to the contralateral side. However, confirming the extent of coverage to the opposite side after administering the injectant would have provided a clearer understanding of its efficacy. Additionally, such confirmation could have helped ascertain the presence of adhesions more accurately. Secondly, similar to other traditional CPB methods, serious neurological complications may occur due to damage to the anterior spinal artery. Lastly, the BT dosage may have been relatively low. As there remains no established study on the appropriate dosage of BT in CPB, a dosage equivalent to that of other sympathetic blocks was used.15,16 However, it has not been conclusively determined whether this dosage is appropriate, and further future study is required.
Conclusion
A case of long-term pain relief after BT injection using a right-sided unilateral retrocrural single-needle technique in the celiac plexus (splanchnic nerve), in a cancer survivor with upper abdominal pain, is reported. To the best of our knowledge, this is the first reported case of BT injection using only a right-sided retrocrural approach to the celiac plexus in a cancer survivor. We believe that the technique used in this case may be an alternative to conventional procedural treatments for controlling abdominal pain in cancer survivors.
Footnotes
Author contributions
JHY collected and organized patient data and wrote the manuscript. HNL participated in data collection, and table and figure creation. JK supervised manuscript writing and overall editing.
Data availability statement
The data underpinning the results of this study can be obtained from the corresponding author upon reasonable request. However, these data are not publicly accessible due to privacy and ethical constraints.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.