
Abstract
Background:
Head and neck cancer (HNC) patients undergoing radiation therapy (RT) experience significant side effects, presenting challenging care tasks for their informal (unpaid) caregivers. HNC caregivers report low caregiving self-efficacy, high distress, and interest in supportive care interventions.
Objective:
This randomized pilot trial assessed the feasibility and acceptability of a 6 to 7 week supported self-management intervention (Prepare to Care) offering psychoeducation and stress management skills building for caregivers of patients receiving RT for HNC.
Methods:
Caregivers were randomized to Prepare to Care or standard of care. Primary feasibility measures included participation and retention percentages. Assessments were completed before the intervention, at intervention completion, and 6-weeks later after intervention completion.
Results:
Caregivers (N = 38) were predominantly female (88.6%), an average age of 56 years old, and a spouse/partner to the patient (71.4%). Participation percent was 42.2%; retention at intervention conclusion was 80% and 77% at the 6-week follow-up. Quantitative and qualitative results support acceptability, with 64% to 88% reporting each intervention module was helpful (quite a bit or very). Intervention caregivers reported a significantly greater improvement in self-efficacy for progressive muscle relaxation (PMR).
Conclusions:
Prepare to Care and the randomized pilot trial methods are feasible and acceptable for HNC caregivers of patients receiving RT. A significant treatment effect was observed for self-efficacy for PMR, and findings were in the expected direction regarding improved caregiving self-efficacy. Further research is necessary to determine the efficacy of this intervention with a focus on increased engagement strategies and longer-term outcomes.
Trial Registration:
NCT03032250
Keywords
Introduction
Treatment for the 66 000 people diagnosed with HNC each year in the United States is complex and often includes daily radiotherapy (RT) for 6 to 7 weeks, sometimes in combination with chemotherapy and/or surgery.1,2 Patients experience significant side effects that impede core aspects of daily life and report higher care needs relative to other cancer patients, presenting challenging care tasks for informal caregivers.3-5 Caring for a patient with HNC may include special food preparation (eg, pureeing food) and feeding tube management, as well as more traditional informal caregiving tasks such as providing emotional support, administering medications, managing medical appointments and insurance claims, communicating with health care providers, and providing hands-on medical care with little to no training.3,6-8 Cancer caregivers, including HNC caregivers, commonly report low self-efficacy for specific caregiving tasks. 6 Low self-efficacy (ie, one’s confidence in capacity to engage in a particular behavior) among cancer caregivers has been shown to be associated with worse caregiver distress, strain, coping, quality of life, adaptation, caregiver functioning, and physical health, as well as patient physical and emotional symptom burden.9-11
HNC caregivers also report high rates of and clinically significant emotional distress, caregiver burden, fear of patient cancer recurrence, and poorer physical and mental health compared to patients and the general population.12-16 One study demonstrated that during and shortly following the patient’s course of RT, HNC caregivers reported increased schedule burden, decreased self-esteem, poorer self-reported health, and dysregulation of the psychoneuroendocrine system. 17 Similarly, another study showed that HNC caregivers experienced a steady increase in distress, peaking 5 weeks into the patient’s radiotherapy treatment. 18 Collectively, these findings suggest a critical need to support HNC caregivers during patient radiotherapy, a time of substantial patient care needs.19-21
HNC caregivers have a need for, and are interested in, supportive care interventions.4,22-26 The few existing interventions for HNC caregivers have demonstrated promise, but have focused solely on optimizing delivery of patient care or have intervened on both members of the patient-caregiver dyad.27-30 The majority were time and resource-intensive, requiring several in-person or lengthy telephone sessions. Resource-intensive interventions requiring significant provider or support staff engagement can be costly to deliver and result in limited translation to clinical practice. 31 In supported self-management interventions, the recipient uses self-directed educational materials to learn information and strategies to manage emotions and promote healthy behaviors with the support of a health care provider.32,33 Such interventions are often used for individuals affected by chronic diseases, such as cancer. 34 Supported self-management interventions can be low cost, reduce health care utilization, and have greater dissemination potential.32,35 Further, supported self-management interventions can be used according to the participant’s preferences for place and time and lessen logistical barriers to in-person delivered interventions. As such, they may be especially attractive to HNC caregivers navigating the hectic radiotherapy treatment period. Supported self-management interventions have shown improvements in fatigue, depression, anxiety, and overall quality of life; however, to date, these interventions have largely been applied in cancer patients, particularly among cancer populations not including HNC (eg, breast, lung, prostate), and have been under-utilized in the cancer caregiving field.32-34
In this study, we conducted a randomized pilot trial to evaluate Prepare to Care, a supported self-management intervention that teaches psycho-education and stress-management skills for caregivers of patients receiving radiation therapy. Our primary aim was to assess the feasibility and acceptability of the intervention and the randomized pilot trial methods. We also assessed potential improvements in self-efficacy for caregiving and other caregiver outcomes including distress (anxiety and depression), quality of life, and self-efficacy for abbreviated progressive muscle relaxation.
Methods
Study Design and Overview
We assessed the feasibility and acceptability of a 6 to 7-week self-management intervention and the randomized pilot trial methods for caregivers of HNC patients undergoing radiation therapy using a parallel group design. Caregivers were randomized 1:1 to the intervention or standard of care control group using a computer-generated randomization scheme with mixed block sizes developed by the biostatistician. Caregivers completed assessments before the intervention (T1), at intervention completion (T2), and 6-week after intervention completion (T3). Intervention caregivers completed a semi-structured qualitative interview at T2. Sociodemographics and caregiving characteristics were collected at recruitment. We also collected clinical characteristics for the patient at study recruitment from the electronic health record. This study was approved by the local Institutional Review Board (IRB00038084) and registered with clinicaltrials.gov (NCT03032250) and adheres to CONSORT recommendations for reporting a pilot feasibility trial. 36
Participants
We approached patient-caregiver dyads at 2 outpatient radiation clinics at the Comprehensive Cancer Center of Wake Forest Baptist Medical Center. If a primary, informal (unpaid) caregiver was not present, with permission of the patient we contacted the caregiver by telephone to gage interest in the study. Though Prepare to Care is a caregiver-directed intervention, at study initiation, both members of the dyad provided written informed consent. In order to increase accrual, we later revised the eligibility criteria so that patient consent was not required for caregiver participation. Patient eligibility included: (1) new or recurrent AJCC stage I to IV squamous cell carcinoma of the upper aerodigestive tract (including lip/oral cavity, nasopharynx, salivary gland, oropharynx, hypopharynx, paranasal sinus, and larynx cancers), (2) planned external beam radiotherapy (± chemotherapy) for 6 to 7 weeks (with curative intent), (3) ≥18 years of age, and (4) having an informal (unpaid) caregiver during RT who is also willing to participate in the study. Patients were excluded if they could not read/communicate in English. Caregivers were eligible if they were: (1) providing the majority of the informal (unpaid) care for an adult meeting the above criteria, and (2) ≥18 years of age. Caregivers were excluded if they (1) had a current cancer diagnosis or (2) could not read/communicate in English. Caregivers received $20 gift cards at the completion of T1, T2, and T3 assessments ($60 in gift cards total).
Intervention Development and Theoretical Underpinnings
Intervention content, timing, and delivery format were developed prior to the current study using a 3-step process including: (1) assessing preferences for wellness programs, including delivery and timing preferences, among a different sample of HNC caregivers 12 ; (2) obtaining input regarding intervention content and delivery from an advisory panel including HNC caregivers and clinicians; and (3) reviewing empirical literature to identify HNC challenges, especially during the radiotherapy period. The Prepare to Care intervention is guided by the self-efficacy construct from Social Cognitive Theory. 11 Self-efficacy refers to one’s confidence in his or her capacity to engage in a particular behavior 11 and is a central component for self-management interventions. 33 Prepare to Care’s self-directed educational modules aim to improve caregiving self-efficacy by promoting the development of skills to manage caregiver emotions and coping, improve communication with the patient and health care providers, promote healthy behaviors, and support patient care.
Intervention Content and Procedures
The multi-component intervention, Prepare to Care, includes: (1) a brief introduction video on a DVD and study website; (2) 8 modules (Table 1) available as a hard copy workbook and on the study website; and (3) CD with audio instructions to facilitate Progressive Muscle Relaxation (PMR) Training (to accompany a module on PMR). PMR training teaches caregivers to identify muscle tension signals and to use the signals as cues to trigger a relaxation response. 37 Prepare to Care is a 6 to 7 week intervention aligned with a patient’s RT (ie, intervention began at the start of radiotherapy and was completed at the end of radiotherapy), in recognition that the severity of multiple RT-related acute toxicities and associated care burdens increase during the treatment regimen. 21 To maximize intervention engagement, modules were designed to be succinct, and study iPads linking directly to the website were available for use at the radiotherapy clinic. Each module includes an introduction and rationale for the topic, strategies to overcome relevant challenges, and an activity to facilitate skills building. Caregiver vignettes are interspersed throughout the modules.
Description of Prepare to Care Intervention Modules.

After recruitment and randomization, caregivers in the intervention group met with the study interventionist at the radiation clinic or by telephone to review the intervention. All participants were provided access to the online website and hard-copy materials (provided in person or by mail). Interventionist involvement was minimal; sessions were brief (approximately 10 minutes) and supported caregivers’ independent engagement with the materials by checking in on caregivers’ module completion and answering potential questions. Each week, caregivers completed a brief assessment to help guide them to relevant modules, though caregivers were encouraged to complete the modules they felt would be most helpful. The assessment included a 24-item checklist with items that corresponded to topics covered in the 8 modules. Modules with the most items selected were recommended. Participants had the option to complete this with the interventionist or on their own. This preference-based approach empowers caregivers to build skills to address their evolving challenges. Caregivers were asked to complete at least 1 module per week and re-visit modules as needed and did not need to complete all modules as part of their participation. Caregivers were encouraged to utilize intervention materials at a time that best fit their schedule. Modules included time logs to track use. The interventionist also sent weekly text or email reminders to complete modules, based on participants’ communication preferences.
Control Group
Caregivers participating in the control group received standard care, which may have included referral to cancer center support services, though this was not a systematic process. At the conclusion of the study, caregivers participating in the control group were provided with Prepare to Care written materials.
Feasibility and Acceptability
Our primary feasibility measures were participation and retention proportions. Prepare to Care acceptability was assessed with a quantitative survey developed for the study and a semi-structured qualitative interview at T2. The quantitative survey asked caregivers to rate how helpful each component of the intervention was from 0 (“Not at all helpful”) to 4 (“Very much helpful”). Qualitative interviews (lasting approximately 30 minutes to 1 hour) explored factors influencing overall acceptability. Specifically, caregivers were asked about their overall experience with the intervention and what they liked or wished was different about each of the intervention components or features. Interviews were recorded and transcribed verbatim.
Measures
Measures were completed online using REDCap, by telephone, or with paper versions completed in person at the clinic or at home and returned by mail. The Caregiver Inventory (CI) 38 is a 21-item instrument that assesses caregiving self-efficacy including self-efficacy for managing medical information, caring for the patient, caring for oneself, and managing difficult interactions/emotions. The CI uses a 9-point Likert scale (“not at all confident” to “totally confident”). Total scores range from 21 to 189, with higher scores indicating greater caregiving self-efficacy. The CI has demonstrated adequate validity and reliability and has been previously used with HNC caregivers.38,39 Depressive symptoms were assessed with the Center for Epidemiological Studies Depression Scale (CES-D), 40 a 20-item instrument assessing frequency of symptoms associated with depression (ie, restless sleep, poor appetite, and feeling lonely). Scores range from 0 to 60, with higher scores indicating more depressive symptoms. The CES-D has been widely used in caregiver populations.12,41,42 Anxiety was assessed with the PROMIS Emotional Distress Anxiety Short Form- 8a, 43 a brief 8-item assessment of anxiety. T-scores range from 37.1 to 83.1, with higher scores reflecting greater anxiety. We assessed quality of life using the total score of the Caregiver Quality of Life Index-Cancer (CqoL-Canc). The CqoL-Canc is a 35-item instrument that assesses burden, disruptiveness, positive adaptation, and financial concerns and provides a total quality of life score. The CqoL-Canc uses a 5-point Likert scale (“not at all” to “very much”), with scores ranging from 0 to 100 and higher scores indicating better quality of life. The instrument has demonstrated reliability and validity and is strongly recommended as quality of life assessment for cancer caregivers.44,45 Self-efficacy for engaging in progressive muscle relaxation (PMR) was assessed with 3-items developed for the purpose of this study (Cronbach’s alpha .89). The instrument uses a 9-point Likert scale (“not at all confident” to “totally confident”), with scores ranging from 3 to 27. Higher scores reflect greater self-efficacy for PMR. These items assess self-efficacy for: (1) distinguishing between tense and relaxed muscles, (2) relaxing each muscle one by one, and (3) relaxing quickly when in stressful situations.
Data Analysis
The sample size was based upon the primary outcome of feasibility. For the targeted sample size of 40, two-sided 95% confidence interval around the expected recruitment (70%) and retention (80%) percentages were within ±12%, yielding 95% confidence that the true recruitment percentage would exceed 59% and the true retention percentage would exceed 67%, both of which would indicate a feasible study. Descriptive statistics (means and standard deviations for continuous variable and frequencies/percentages for categorical variables) were used to summarize sociodemographic characteristics and caregiving characteristics at T1. Participation and retention proportions and their associated 95% confidence intervals (CI) were estimated. Participation proportion was estimated as proportion of all eligible screened caregivers who agreed to participate; retention proportions were estimated as proportion of all enrolled participants completing T1 surveys who completed all subsequent (T2 and T3) surveys.
Acceptability of the intervention was summarized quantitatively and qualitatively by caregivers in the intervention arm following the conclusion of the intervention. Percentages of caregivers reporting that an intervention component was quite a bit or very much helpful were calculated to demonstrate acceptability of each intervention component. Qualitative interviews were coded by 2 raters using a thematic analysis procedure.46,47 Specifically, coders read and re-read interview transcripts and identified themes related to acceptability and suggestions for improvement. Discrepancies were resolved with team discussion to achieve consensus.
Finally, though our study was not powered to detect intervention effects, as a secondary goal we examined differences in key outcomes. In an intent-to-treat analysis, we used mixed models with a random subject effect and fixed effects of time (T1, T2, T3, treated as 3 categories), intervention (yes/no), and included the first-order interaction between intervention assignment and time. We used linear contrasts to estimate average within-person changes by time by intervention group. A 2-sided alpha level of .05 was used to indicate statistical significance. Outcomes examined included self-efficacy for caregiving (CI total score as well as the 4 subscales), self-efficacy for progressive muscle relaxation, depression, anxiety, and overall CqoL-Canc total index score). All analyses were conducted in SAS (version 9.4, Cary, NC).
Results
Feasibility
Caregivers were approached for recruitment between May 2017 and December 2019, with brief disruptions due to staffing issues. Of the 90 eligible caregivers, 38 (42.2%, 95% CI 32.0%-52.4%) agreed to participate and were randomized to the Prepare to Care intervention (n = 19) or control group (n = 19). See Table 2 for sociodemographic and caregiving characteristics. Of the 38 caregivers randomized, 35 completed T1 assessments (92%; 95% CI 79%-98%; n = 17 intervention; n = 18 control). The 3 caregivers who did not return T1 surveys or initiate intervention activity are not included in our primary analyses. Of the 35 caregivers who completed T1 (38.9% of the 90 eligible; 95% CI 28.8%-49.0%, n = 17 intervention; n = 18 control), 28 (80%; 95% CI 63.1%-91.6%) were retained at T2 (12 [70.6%; 95% CI 44%-89.7%] intervention; 16 [88.9%; 95% CI 65.3%-98.6%] control). Twenty-seven caregivers (77.1%; 95% CI 63.2%-91.1%) were retained at T3 (12 [70.6%; 95% CI 44%-89.7%] intervention; 15 [83.3%; 95% CI 58.6%-96.4%] control) (See Figure 1). Data collection was completed February 2020, at which point the trial was considered complete.
Baseline Sociodemographic and Caregiving Characteristics.

Other includes unemployed, disabled, or keeping house.
Calculated among caregivers (n = 28 total) who report living with patient.

Study flow diagram.
Acceptability
Eleven of the intervention caregivers (65%) provided quantitative ratings of helpfulness of each intervention component. Given the preference-based nature of the intervention, caregivers only rated helpfulness for modules used. The majority of caregivers rated each of the used modules as quite a bit/ very much helpful, ranging from 64.0% of caregivers (eg, Managing Time Module) to 88.0% of caregivers (Utilizing Resources Module). All modules were completed by all participants who completed the survey, with the exception of the Utilizing Resources Module (completed by 80% of participants) and the Seeking and Accepting Support Module (completed by 91% of participants). See Table 3 for acceptability ratings for modules and other intervention components and features.
Intervention Use and Acceptability Survey Results among Intervention Caregivers who completed the Survey at T2 (n = 11).
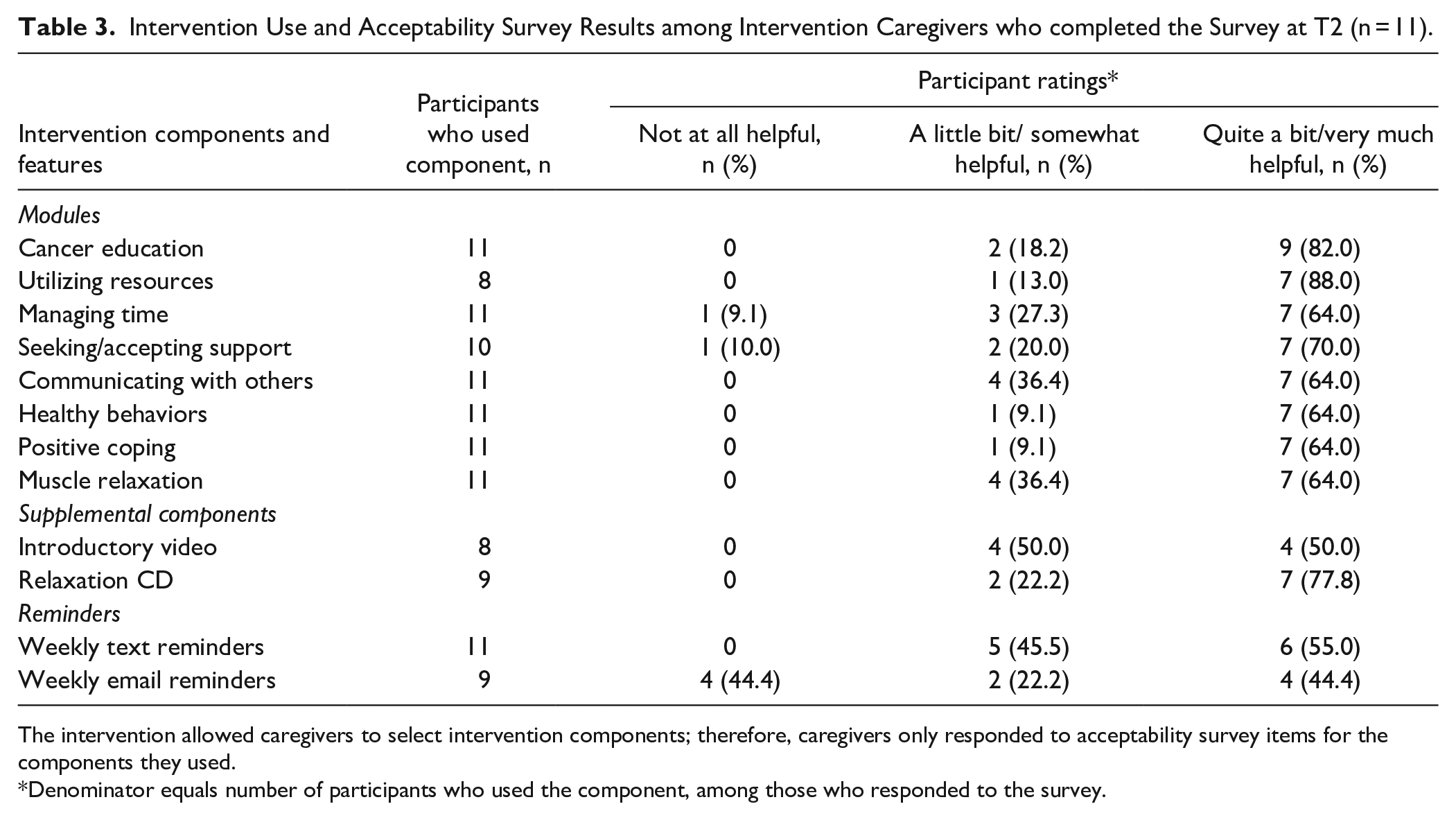
The intervention allowed caregivers to select intervention components; therefore, caregivers only responded to acceptability survey items for the components they used.
Denominator equals number of participants who used the component, among those who responded to the survey.
Qualitative findings (n = 12 intervention caregivers, 71%) provided additional support for caregivers’ acceptance of the Prepare to Care Intervention. All caregivers reported a positive experience using the Prepare to Care Intervention, citing several ways that the intervention was helpful. Caregivers noted that the intervention normalized what they were feeling, prompted them to ask for help, and linked them to additional helpful resources (See Table 4). Caregivers reported the modules increased their understanding of module content and what to expect, which better equipped the caregiver to care for the patient. Similarly, it was noted that the intervention allowed caregivers to focus their energy on their role as a caregiver. Importantly, caregivers also indicated that they developed new skills as a result of Prepare to Care such as relaxing and coping, learning to ask for help, and communicating with their loved one and others. One caregiver expressed that the intervention was a catalyst for a newfound desire to help others in similar situations.
Exemplar Quotes from Caregivers in the Prepare to Care Intervention.
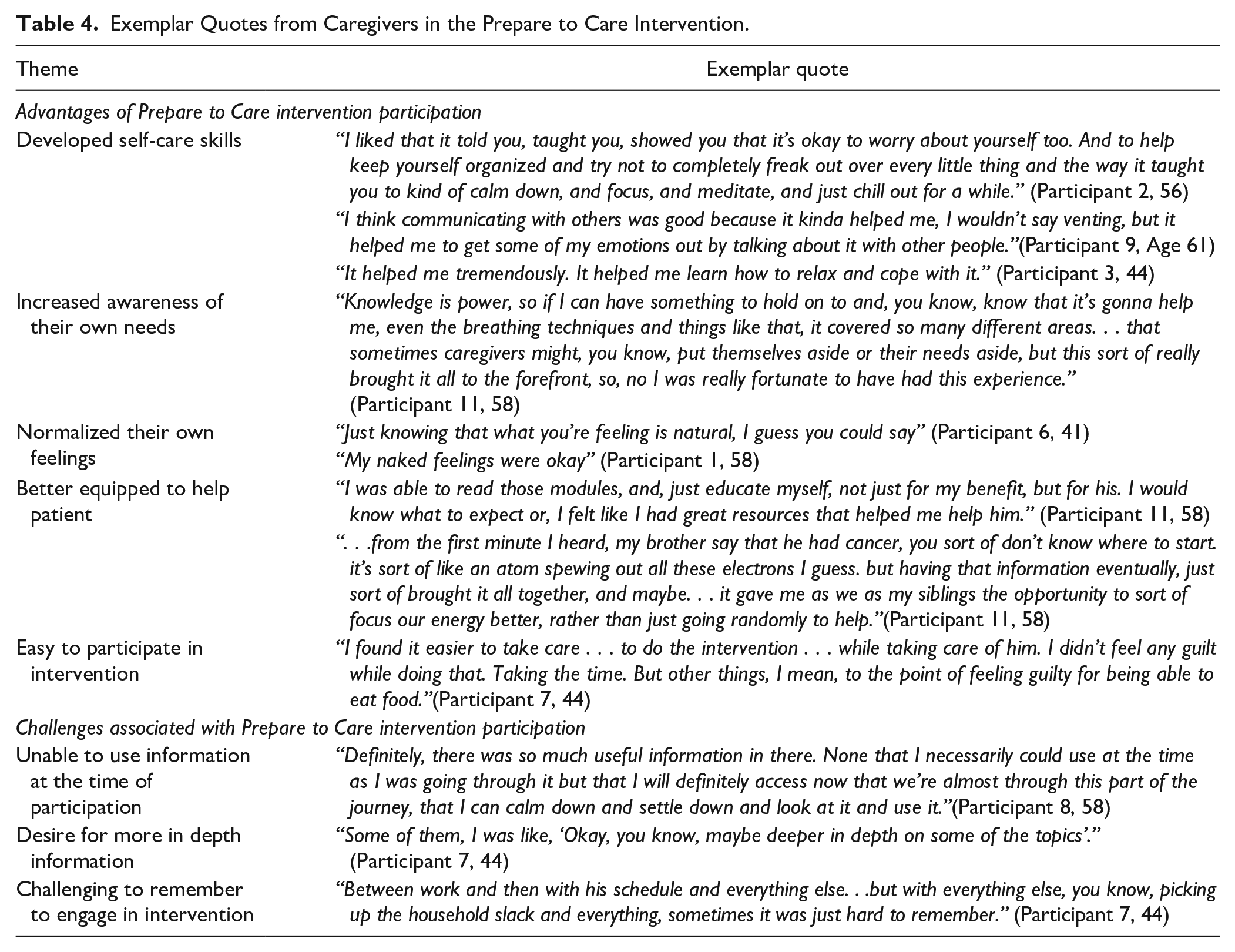
Caregivers also made suggestions for improving the intervention. Though 2 caregivers noted that they would have liked more information, 1 caregiver reported that it was too much information and another caregiver thought the activities were too time consuming. While several caregivers commented on ease of intervention participation, 1 caregiver indicated that they were unable to utilize the information learned at the time, though they were still planning to do so now that their situation was calmer. Some caregivers also commented on how challenging it was to remember to participate and suggested sending additional text reminders or sending the text reminders at a different time of the day. The website was not an appealing option to caregivers, in part because it was duplicative of the hard-copy workbooks; suggestions included developing a website accessible on a cell phone, such as a web-app, and including an option to complete activities on a more interactive website.
Preliminary Examination of Intervention Effects
Caregivers participating in the intervention demonstrated a larger improvement in self-efficacy for caregiving (total score and subscales) compared to caregivers in the control group, though this difference was not significant (See Table 5). Among the instrument subscales, the intervention group showed the largest improvements in self-efficacy for caring for oneself and managing difficult interactions/emotions over time. We observed a significant improvement in self-efficacy for progressive muscle relaxation over time in intervention caregivers compared to control group caregivers. Significant intervention effects were not observed for distress or quality of life.
Analyzes of Intervention Effects from Repeated Measures Models (Intent-to-Treat Analysis, N = 35).

Estimated as difference of least squares means from mixed model containing time (T1,T2, T3, corresponding to pre-intervention, intervention conclusion, and 6-week post intervention conclusion weeks) and intervention condition and first-order time × intervention condition interaction terms.
Bolded numbers reflect significant findings.
Discussion
Results from this randomized pilot trial study support the feasibility and acceptability of Prepare to Care for caregivers of patients receiving RT for HNC. The retention percentage (80% at intervention completion and 77% at follow-up) was consistent with the expected percentage and supported the feasibility of the intervention. The participation percentage of 42% was lower than anticipated but consistent with previous studies evaluating psycho-educational interventions including cancer caregivers, although there is wide variability across studies, many of which recruited breast and prostate cancer caregivers.27,48,49 The hypothesized percentage of 70% was based on a prior study that was observational, which may have been an unrealistic estimate for a randomized pilot trial. 50 In this study, many caregivers who declined participation reported feeling overwhelmed. HNC caregivers are an especially vulnerable population tasked with providing complex care and are underrepresented with behavioral intervention approaches. Consequently, when intervening with this population, expectations regarding feasibility metrics such as participation should be considered carefully and in the context of this highly burdensome disease. Further, our recruitment challenges underscore the need for creative strategies to market programs for busy HNC caregivers during patient RT. For example, some cancer centers have caregiver advocates or peer support programs that include volunteers or paid staff that have experience as an individual affected by cancer. These individuals may be particularly well suited to share details about the study to boost recruitment efforts. Another option is partnering with supportive care programs or patient advocacy non-profit groups to advertise psychosocial caregiver interventions.
Our findings demonstrated acceptability of the intervention. Caregivers reported that the intervention modules were helpful and these findings were also supported by qualitative feedback. The highest levels of acceptability were reported for the “Utilizing Resources” and “Cancer Education” modules relative to the other modules. This aligns with reports of high unmet educational/information needs as they pertain to cancer and available resources from prior studies of HNC caregivers.4,12,22,24-26 Importantly, qualitative data highlighted the variability in caregivers’ preferences regarding the amount of information provided, the timing of the intervention and their engagement in intervention activities, highlighting that the preference-based approach of the intervention was appropriate and could be enhanced to potentially improve the intervention. Caregivers also recommended a more interactive website for completing the intervention activities to improve accessibility.
Our findings showed an improvement in caregiving self-efficacy for intervention caregivers relative to control group caregivers, though these findings were not statistically significant. Similarly, other psychosocial interventions for cancer patients and caregivers have successfully improved self-efficacy constructs.38,51,52 Our focus on caregiving self-efficacy for HNC caregivers is especially important, given the challenges associated with caring for this high-needs patient population while simultaneously taking care of oneself.3-6 Our results also suggest that HNC caregivers can engage in PMR skills training during patient RT and improve their PMR-specific self-efficacy. PMR and other integrative medicine modalities have been primarily tested in cancer patient populations rather than HNC caregivers or cancer caregivers more broadly.53,54 Of note, our qualitative data revealed that the Prepare to Care intervention may have influenced some unmeasured outcomes in this study. For example, intervention participants highlighted that the intervention helped caregivers know what to expect, improved their communication with patients, and improved their ability to ask for help. A larger, fully-powered study with a more distal assessment and consideration of additional outcome measures is needed to determine both proximal and distal intervention effects for caregivers.
This study builds upon the sparse literature for behavioral interventions targeted at HNC caregivers.28-30,49 While most HNC caregiver behavioral interventions have focused solely on optimizing patient care or have been dyadic in nature, Prepare to Care focuses on providing psycho-education and stress-management skills training for caregivers. Another promising self-management pilot intervention targeted both HNC patients and spouse caregivers and demonstrated intervention effects for patient and caregiver depressive symptoms and patient cancer-specific distress. 27 An important question for future caregiver-directed interventions, such as Prepare to Care, is whether or not patient outcomes can be improved by caregiver participation alone, thereby preventing additional burden for HNC patients who are already managing multi-modality treatment and side effects.2,19-21
There are several strengths to this study. Prepare to Care was developed with input from stakeholders including HNC caregivers, providers, and psychosocial oncology professionals, an important consideration for supporting translation into practice. 55 In addition, this study is an important contribution that builds upon the limited psychosocial interventions that have been developed for and tested in HNC caregivers.27-30 Our focus on a vulnerable population of caregivers (ie, HNC caregivers) who care for patients receiving complex treatment, has been highlighted by the National Cancer Institute and National Institute for Nursing Research as an important gap to move the cancer caregiving field forward. 56 Further, the self-management format of Prepare to Care allows the intervention to be easily delivered to those providing care for HNC patients treated at diverse oncology clinics, with potential for adaption to other cancer caregiving populations as well. Caregiving self-efficacy has also not traditionally been a focus of behavioral interventions for HNC caregivers, despite caregivers reporting poor self-efficacy and feeling underprepared for their caregiving roles.6,7 Finally, we supplemented quantitative outcome assessments using validated instruments with qualitative interviews to allow a more in-depth exploration of caregiver experiences.
This feasibility study was limited by a small sample; however, our primary interest was ability to recruit and retain HNC caregivers during patient RT. We were not powered to determine efficacy of our preliminary outcomes and our findings should be interpreted with caution. Since participants could access materials in hard-copy, online, or a mixture of both, we cannot confirm level of intervention engagement among caregivers who were lost to follow-up. For example, it is possible that a caregiver continued to utilize intervention materials despite not completing the T2 assessment. Though our participation percentage is similar or better than other caregiver intervention studies, we did not meet our participation goal of 70%.48,49 In addition, participants were randomized prior to baseline and due to the purpose of the RCT (to compare Prepare to Care with a standard care control group), we were unable to blind participants to their assignment group, introducing the potential for performance bias. 57 Given the scope of this feasibility study, we did not include a long-term follow-up assessment to assess potential sustained or delayed intervention effects, which may be especially important for this population since HNC patients experience morbidity beyond the treatment period. 58 The majority of participants were white females who were a spouse/partner to the patient, limiting the generalizability of these findings to additional caregiver types. However, spouses/partners commonly serve as a caregiver for HNC patients and HNC most commonly afflicts white males.1,14,25 Finally, we did not stratify randomization based on gender in this study and all 4 male caregivers were randomized to the control group. Female cancer caregivers experience greater stress and mental and physical health outcomes compared to male caregivers and we cannot rule out potential gender effects in this study. 59
Conclusions
Prepare to Care, our novel self-management intervention for HNC caregivers of patients receiving RT, and the randomized pilot trial methodology, were feasible and acceptable in this pilot study. This study is an important first step that should be expanded upon in future research. A larger, fully-powered efficacy trial is necessary to determine treatment effects on caregiving self-efficacy, as well as secondary outcomes, including potential impacts on the patients as well. Additionally, a longer follow-up assessment is warranted to determine distal intervention effects and mechanisms of change. In accordance with qualitative feedback, future work should include a more interactive, mobile-accessible website which may also ease participation burden by allowing caregivers to access materials and complete activities on a mobile phone. Though we previously included a DVD introduction that provided a brief overview of the intervention, we recommend including an improved introduction that addresses perceived barriers to engagement to help caregivers prepare with information about what to expect with the intervention and how to best use the intervention within the busy RT schedule. Similarly, to improve engagement, we also suggest making the PMR audio file available on the study website. Finally, testing in diverse community oncology clinics as a multi-site trial would provide valuable information, given the careful consideration to scalability in the intervention development phase of Prepare to Care.
Footnotes
Acknowledgements
We thank the participants for their participation during this challenging time. We also thank Michelle Bishop, PhD, for lending her collaboration in developing the intervention materials and to Sara Boyd, MPH, for her contribution to the qualitative analyses.
Data Available
Data are available by request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Cancer Institute of the NIH under Award Number R03CA208560, through the NCI Community Oncology Research Program (NCORP) under Award Number UG1CA189824, and the Comprehensive Cancer Center of Wake Forest Baptist Medical Center under Award Number P30CA012197. Dr. Nightingale’s effort on this work was in part supported by the National Center for Advancing Translational Sciences of the NIH under Award Number KL2TR001421. This study also received study coordinator support through the Wake Forest Clinical Translational Science Institute (UL1TR001420). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.