
Abstract
Background:
Lung cancer is the most diagnosed cancer worldwide and is associated with various unmet supportive care needs. To address these needs, a 6-week virtual program called Inspire Now was developed, integrating yoga, education, and group support. The primary objective of this mixed-methods observational study was to evaluate the program’s impact on quality of life (QOL). Secondary objectives included changes in participant-identified concerns, participants’ qualitative experiences, and acceptability of virtual delivery.
Methods:
Eligible participants included people with primary lung cancer enrolled in the program. Questionnaires were administered at baseline and program completion. QOL and patient-identified concerns were evaluated by within-person changes in Functional Assessment of Cancer Therapy – Lung (FACT-L) and Measure Yourself Concerns and Wellbeing (MYCaW). Qualitative experiences and feasibility of virtual delivery were obtained by MYCaW and an internally developed questionnaire. FACT-L and MYCaW were analyzed using paired t-tests, and qualitative data was evaluated by an inductive thematic analysis.
Results:
Forty-five participants were enrolled and 31 were eligible for analysis. Most were female (87%), had stage IV disease (68%), and were on active treatment (74%). Significant improvements were observed in FACT-General and Lung scores (mean changes: +6.1, 95% CI 2.2- 10.0, P = .003; +5.9, 95% CI 1.1-10.7, P = .02, respectively). MYCaW concerns and overall wellbeing were significantly improved. Participants viewed the virtual format favorably. Emotional support and connection were the most valued aspects of the program.
Conclusions:
A 6-week virtual program of yoga, education, and group support improved QOL, patient-specific concerns, and wellbeing for those with lung cancer.
Keywords
Introduction
Lung cancer is the most commonly diagnosed cancer and the leading cause of cancer mortality both in Canada and worldwide.1,2 Although mortality remains high, advances in treatment and detection have led to improved survival rates, resulting in a growing number of lung cancer survivors compared to previous decades. 3 Evidence shows that people with lung cancer and lung cancer survivors report high symptom burdens, mental health concerns, unmet supportive care needs, and impaired quality of life (QOL).4 -7
Lung cancer survivors frequently report high symptom burdens, including pain, fatigue, and dyspnea. 4 In addition to physical symptoms, people with lung cancer experience higher rates of anxiety and depression compared to the general public, 4 and higher rates of suicide compared to other cancers. 8 Furthermore, various studies have evaluated the unmet supportive care needs in this population and identified gaps related to physical, emotional, psychological, spiritual and existential, informational, and social needs.6,7,9 This is important, as unmet supportive care needs, in particular psychological and physical needs, are strongly correlated with lower QOL.4,5
Despite the high impact of lung cancer on patients and survivors, it often receives less funding and charitable donations compared to other cancer types relative to its burden.10 -13 Stigma, stemming from the association between lung cancer and smoking, may contribute to these funding disparities, and to mental health and social challenges faced by survivors.4,5,14 Collectively, this highlights a persistent gap between patient needs and the resources available to support them.
Home-based multimodal programs have been evaluated in other cancer types as a method to support QOL with encouraging results, but data in lung cancer is limited. The content of existing programs varies, but frequently includes educational content, movement/physical components, and psychological support. 15 In lung cancer populations, it has been reported that among various unmet supportive care needs, psychological and/or psychosocial support are commonly reported and are associated with poorer QOL.4,13 Thus, the psychological and psychosocial aspects are important to address in those with lung cancer. With this in mind, in 2019, The Centre for Health Innovation developed a 6-week program to provide support to people living with lung cancer. The multimodal program, called Inspire Now, included elements of group support, yoga, and educational content. In 2019, we evaluated this program in a pilot study to assess feasibility and identify outcomes which may be positively influenced through participation in the program. 16 The study, which included 8 participants, showed improvements in almost all aspects of QOL and overall wellbeing. Qualitatively, the group support and social interactions were highly valued by participants. With this information, the program underwent minor adjustments based on participant feedback, and we planned to conduct a larger study to assess QOL.
In this follow up and expanded study, we aim to evaluate the efficacy of the Inspire Now program. The primary objective is to assess QOL. Secondary objectives include participant-identified concerns and wellbeing, determining the feasibility and acceptability of a virtual program delivery, and describing program expectations and satisfaction.
Methods
This manuscript follows the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for reporting of observational studies 17 and the Checklist Standardizing the Reporting of Interventions for Yoga (CLARIFY) guidelines for describing the yoga delivered in the program. 18
Study Design
This was an uncontrolled observational study in people with lung cancer who attended the program “Inspire Now: A Program for People with Lung Cancer” delivered by The Centre for Health Innovation. A mixed methods approach was used to evaluate the program, aiming to provide a greater contextual understanding of the quantitative findings and a more patient-centered perspective.19,20 Participants completed questionnaires for QOL, overall wellbeing, and specific concerns, as well as an internally developed questionnaire designed to evaluate satisfaction and qualitative experience with the program. Questionnaires were completed before the onset of the program and shortly after completion. The program ran once a week for 6 weeks. Recruitment and follow-up were prospective.
Setting
This study was conducted by researchers at The Patterson Institute for Integrative Oncology Research, part of the Canadian College of Naturopathic Medicine which is based on Toronto, Canada. The program was held virtually through The Centre for Health Innovation, located in Ottawa, Canada. Data on participant location was not collected. Participants were recruited from 8 consecutive sessions of the program between May 19th, 2020, and March 4th, 2024. Data collection was completed on April 15th, 2024.
Participants
Registration for the program required a diagnosis of primary lung cancer of any stage; all program participants were eligible to take part in the research evaluation. Participants of the program were approached regarding the study if they consented to being contacted by the research team. Consent to contact was obtained by the program facilitator. Signed informed consent was obtained for all participants prior to any study activities.
Regulatory Adherence
Ethics approval for this study was obtained by the Canadian College of Naturopathic Medicine Research Ethics Board, CCNMREB031.Seely.Psihogios, before initiating the study.
Program Overview
The Inspire Now program is a 6-week multimodal program consisting of yoga, education, and group support. The program was developed and facilitated by a certified yoga therapist (C-IAYT) at The Centre for Health Innovation with input from 2 survivor advocates (1 from Lung Cancer Canada and 1 from The Ottawa Hospital), and a naturopathic doctor. Following our pilot session in early 2019, minor modifications were made to the program based on participant feedback. Additionally, due to the COVID-19 pandemic, the format of the program changed to virtual delivery through Zoom.
Each program session included 1 class per week for 6 weeks; each class was 2.5 hours in duration and consisted of 4 parts: (1) group support and facilitator-led discussion, (2) an integrative lecture on various topics of interest to people with lung cancer, (3) yoga and breath work, and (4) a group check-in before session completion. The yoga practice was 30 minutes in duration and consisted of gentle somatic movements (10 minutes) and breath work (pranayama: 20 minutes). The practice was guided with visual and verbal instruction. These practices were recorded and provided to participants for at-home practice. The integrative lectures were delivered by various healthcare providers at the Centre for Health Innovation including a yoga therapist, psychotherapist, naturopathic doctor, physiotherapist, chiropractor, hypnotherapist, and Traditional Chinese Medicine Doctor. Lecture topics included the nervous system, nutrition, environmental influences on health, lifestyle considerations during treatment, communication with family and health care providers, understanding lymph and lungs, and perspectives on grief and death.
Outcomes
Outcomes of this study included:
Changes in validated QOL scores from baseline to program completion (primary outcome),
Changes in validated participant-identified concerns and overall wellbeing scores from baseline to program completion,
Assess the feasibility and acceptability of a virtual program delivery through attendance rates and qualitative responses,
Describe participants’ reasons for joining the program and program expectations through qualitative responses,
Measure program satisfaction, including what participants most valued and areas for improvement, through qualitative responses and a quantitative evaluation.
All outcomes were pre-specified.
Data Sources and Measurements
Participants completed self-reported questionnaires digitally through the Research Electronic Data Capture (REDCap) program. Assessments were completed before the program began and after it ended approximately 5 weeks later. Attendance was obtained from the program facilitator.
The primary outcome of QOL was measured using the Functional Assessment of Cancer Therapy – Lung (FACT-L) questionnaire. 21 FACT-L is a validated, reliable, and widely used tool for evaluating QOL in people with lung cancer. 21 The FACT-L is composed of the FACT-general (FACT-G) questionnaire with the addition of a subsection on lung cancer-specific symptoms. It measures QOL using 5 sub scales: physical, emotional, social, and functional wellbeing, and symptoms specific to lung cancer. The FACT-L is scored in 3 primary ways: the general score (FACT-G), which includes physical, social, emotional, and functional scales; the trial outcome index (TOI), which includes the physical, functional, and symptom scales; and total score (FACT-L Total), which includes all sub scales. The primary endpoint was changes in FACT-G scores. This was selected as the primary endpoint as there is a known minimal important difference (MID) for the FACT-G, 21 whereas this is not established for the FACT-L Total.
Participant-identified concerns and overall wellbeing were measured by the Measure Yourself Concerns and Wellbeing (MYCaW) questionnaire. 22 MYCaW is a valid and reliable patient-reported outcome measure which can capture a broad spectrum of patient concerns which may be missed by standardized tools. 22 MYCaW asks participants to identify up to 2 concerns they hope will be improved and includes an assessment of overall wellbeing, each scored on a scale of zero (as good as it can be) to 6 (as bad as it can be).
The feasibility and acceptability of virtual delivery was obtained from program enrollment, attendance rates, and subjective feedback from participants. Reasons for joining the program, program expectations, and both the qualitative and quantitative evaluation of the program were gathered from our internally developed questionnaire and open-ended questions from the MYCaW questionnaire.
Quantitative Variables
QOL, participant concerns, and overall wellbeing are presented as mean scores. Within-person changes in each metric were compared between baseline and the end of the program using the difference in mean values. MYCaW and FACT were scored according to their respective recommended algorithms.23 -25 For all FACT scores, a higher score is favorable. For all MYCaW scores, a lower score is favorable. Program satisfaction was quantitatively evaluated with 8 items using a Likert scale of 1 (strongly disagree) to 5 (strongly agree). All internally developed questionnaires are present in the Supplemental Materials.
The minimum important difference (MID) for FACT-G has been reported to be 5 to 7 points.26,27 Individual sub scales vary, with MIDs ranging from 0.7 to 2.0 points.26,28 Clinically meaningful changes in MYCaW have been reported to be 0.7 to 1.0 points for both patient-reported symptoms and overall wellbeing.23,25
Qualitative Variables
Qualitative data on program expectations, satisfaction, and the acceptability of virtual delivery were collected using open-ended questions from both the MYCaW questionnaire and an internally developed questionnaire. Patient-identified concerns (MYCaW Concerns 1 and 2) were categorized according to the MYCaW coding framework. 22 Reasons for joining the program and participant expectations were captured through the MYCaW question: “What are you hoping to learn or gain from participating in the program?” Program satisfaction was assessed using 3 questions: 1 from MYCaW (“Reflecting on your time throughout the program, what were the most important aspects for you?”) and 2 from the internal questionnaire (“What did you enjoy most about the program?” and “What would you change about the program?”) Acceptability of the virtual format was explored through 1 question from the internal questionnaire: “How did you feel about the program being held virtually?”
Sample Size
With respect our primary outcome of QOL, power calculations were conducted based on the results from our pilot study and in accordance with validated guidelines for a clinically meaningful change in FACT-G scores. A sample size of 40 participants provided 80% power to detect a difference of 5.0 points on the FACT-G at an alpha of .05.
Statistical Methods
Participants were included in the analyses if they completed both the baseline and follow-up questionnaires. Quantitative changes in QOL, participant concerns, and overall wellbeing were analyzed using paired t tests. Feasibility was analyzed using descriptive statistics. Standard deviation and inter-quartile range (IQR) were used as measures of dispersion for means and medians, respectively. Confidence intervals (CIs) were used as a measure of dispersion for difference in means. Qualitative responses from MYCaW concerns 1 and 2 were analyzed according to the MYCaW coding framework. 22 The framework was applied independently by 2 team members and discussed to reach consensus. Qualitative responses from the other MYCaW questions and internally developed questionnaires were also evaluated independently by 2 team members. An inductive thematic analysis was performed for each question. 29 Commonalities in responses were identified to create initial codes, which were then re-applied to all responses to generate overarching themes. A semantic approach was used, meaning the focus was on summarizing the data as opposed to identifying underlying ideas or assumptions. A strict threshold was not used to define what constituted a prominent theme. Results were put into context based on the number of themes present per question and the number of participants who mentioned each theme.
Results
Participant Characteristics
Seventy-nine people registered for the program. Sixty registrants were approached for participation in the study, of which 45 were enrolled. Six participants withdrew from both the program and research component, 1 participant was a screen failure (i.e., did not have lung cancer), and 7 were lost to follow up (i.e., did not complete the final questionnaire). Thirty-one participants were analyzed. See Figure 1 for participant flow.

Flow diagram. Program participants were only approached regarding the study if they provided consent to the program facilitator that they were open to being contacted by the research team.
The mean age at enrollment was 61.4 ± 10.2 years. The median time from diagnosis to enrollment was 12.4 months (IQR 7.3-19.3). Most participants identified as female (87%), had stage IV disease (68%), and were currently receiving conventional cancer treatments (74%). All participants received conventional care for their cancer (either during the program or previously) or were scheduled to receive it shortly. Over half of participants (64.5%) had previously attended another cancer-specific program, including support groups (n = 11), exercise programs (n = 6), group therapy (n = 2), and educational webinars (n = 2). Table 1 summarizes baseline characteristics.
Baseline Characteristics.

N = 31. All characteristics are participant-reported.
Quality of Life and Overall Wellbeing
All scores from the FACT-L and MYCaW are shown in Table 2. Participants completed their baseline assessment a median of 2 days (IQR 2-7) before the onset of the program, and follow-up assessment a median of 2 days (IQR 1-2) after completion of the program. Clinically and statistically significant improvements were seen in both FACT-G (6.1, 95% CI 2.2-10.0, P = .003) and FACT-L Total (5.9, 95% CI 1.1-10.7, P = .02). The emotional, social, and functional wellbeing sub domains were also significantly improved. The trial outcome index, physical domain, and lung cancer symptom domain did not show significant improvements. MYCaW overall wellbeing scores improved significantly (−0.9, 95% CI −1.3 to −0.5, P < .001).
Validated Questionnaire Scores.

Abbreviations: FACT-L, Functional Assessment of Cancer Therapy – Lung; CI: confidence interval; MYCaW, Measure Yourself Concerns and Wellbeing; SD, standard deviation.
Participant-Identified Concerns
Participants could record up to 2 concerns, resulting in a total of 60 responses on the MYCaW questionnaire. Missing data left 48 concerns eligible for quantitative analysis. Both concerns 1 and 2 showed statistically and clinically significant improvements in mean scores (see Table 2). Categorically, 29 concerns (48%) were classified as psychological and emotional, 22 (37%) were physical concerns, and 9 (15%) were general wellbeing concerns. No concerns were classified as hospital cancer treatment concerns (eg, relating to side effects of treatments) or practical concerns (eg, finance, work).
Feasibility and Acceptability of Virtual Assessment
A total of 79 patients registered for the program over 8 program sessions (mean 9.9 ± 1.4 patients per session). The minimum number of patients in a session was 7, and the maximum was 14. Participants enrolled in this study attended a mean of 5.0 ± 1.5 of 6 classes. Over half of participants attended all 6 classes, and only 2 participants attended less than half the program classes. Attendance records were missing for 1 program session; thus, data is missing for the 3 participants who had consented to participation in the study for this session.
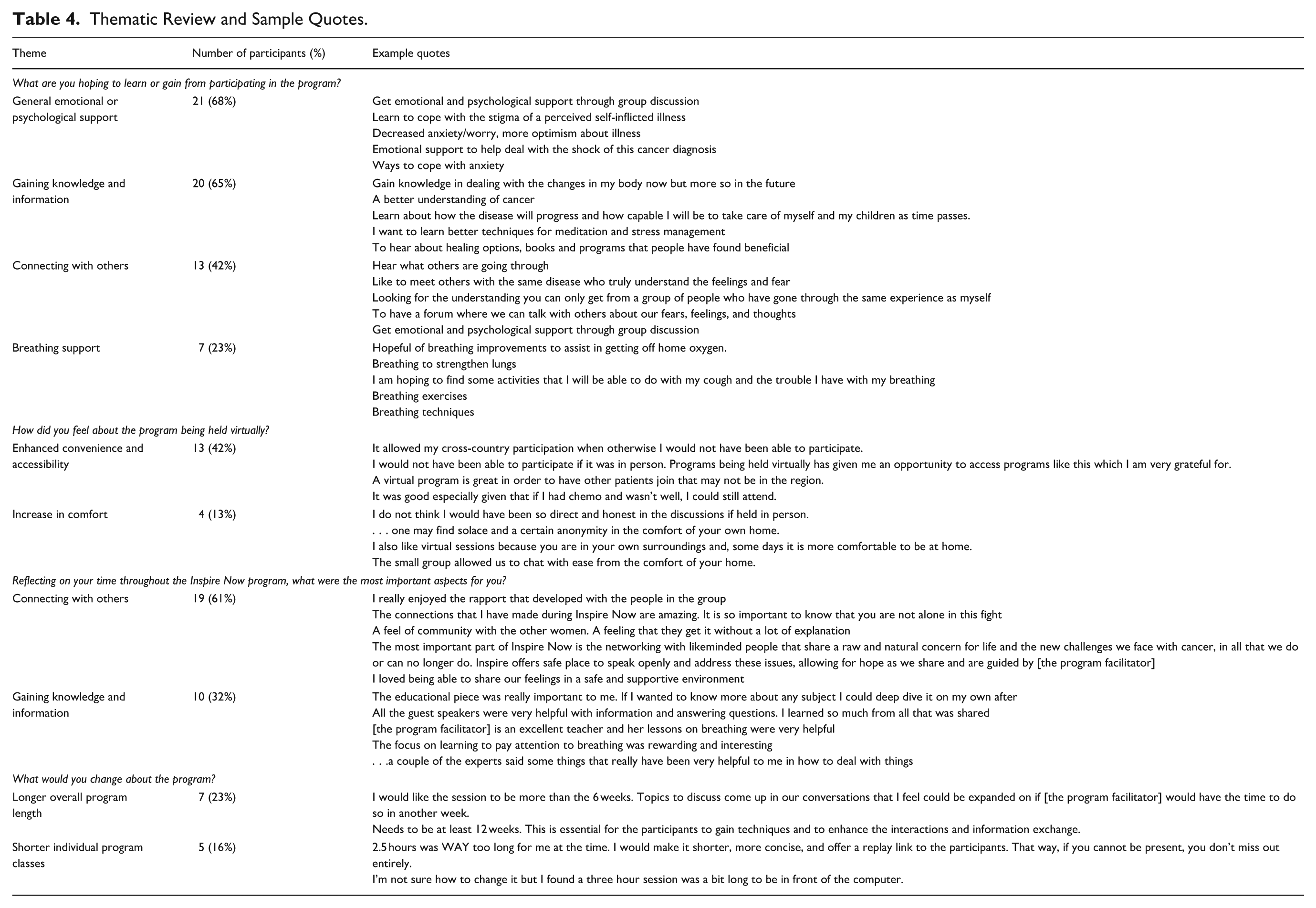
Qualitatively, all participants responded positively to the virtual delivery of the program. The most common theme was that it made the program more convenient and accessible, which was mentioned by 13 participants (45%). Accessibility was most often discussed with regards to distance from the clinic, such as participant 10 stating “It allowed my cross-country participation when I otherwise would not have been able to participate.” Participant 36 noted increased accessibility due to potential symptom burden, “It was good, especially given that if I had chemo and wasn’t well, I could still attend.” Another minor theme identified was an increase in comfort, mentioned by 4 participants (13%). Participant 12 stated “. . .one may find solace and a certain anonymity in the comfort of your own home” and participant 29 said “I do not think I would have been so direct and honest in the discussions if held in person.” None of the 31 participants analyzed expressed any concerns with the virtual format, either from a technological standpoint or value of the program and interactions. It should be noted that 1 participant withdrew from the program due to technical difficulties and was subsequently withdrawn from the research study; thus, they were not able to respond to this question.
Reasons for Joining the Program and Program Expectations
Prior to program initiation, participants were asked what they were hoping to gain or learn from participation. This question was open-ended and resulted in 68 unique responses. The most common themes were general emotional or psychological support (n = 21 participants), gaining knowledge and information (n = 20), connecting with others (n = 13), and breathing support (n = 7). Emotional/psychological support included references to stress management, coping, managing anxiety, and acceptance. Participant 15 mentioned she wanted to “Learn to cope with the stigma of a perceived self-inflicted disease” and participant 20 mentioned “decreased anxiety/worry, more optimism about illness.” The theme of “gaining knowledge and information” was focused on learning more about lung cancer in general and learning about other community supports or treatment options which others have benefited from. For the theme of connecting with others, participants valued the support and connection they might receive from people who may have shared similar experiences. Participant 24 stated:
Finding new ways to connect with individuals that are facing similar challenges. Having the chance to be open about our journey and how it takes a toll on the person both emotional and physically. I want to be a part of something that can make a difference.
For the theme of breathing support, participants were often looking for specific exercises they could do to improve their breathing.
Program Satisfaction
Quantitative Evaluation
Participants answered 8 end-of-study survey questions regarding their experience with the program (Table 3). The mean score for all items was 4.5 ± 0.7 out of 5. For 92% of responses, participants indicated they “agreed” (4/5) or “strongly agreed” (5/5) with the statement. The highest score was for “I felt support and acceptance” (4.8 ± 0.5), while the lowest was for “I learned what I hoped to” (4.2 ± 0.7).
End of Study Survey Scores.

N = 31. Each question used a Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree).
Abbreviation: SD, standard deviation.
What Has Been Most Important to You?
At the end of the program, the MYCaW asks “Reflecting on your time throughout the program, what were the most important aspects for you?” The 2 most prominent themes we identified in the responses were connecting with others and gaining knowledge and information.
Nineteen participants (61%) mentioned the theme of connecting with others in their response. Participants spoke to feeling support during the classes, both from other participants and from the program facilitator. Seven participants (23%) specifically mentioned connecting with others who shared their own experiences with cancer as being important. Participant 31 wrote:
I loved being able to share our true feelings and frustrations in a safe and supportive environment. I must say the 2 hours and 30 minutes flew by and I really looked forward to this time spent with others going through the same disease of lung cancer. It is so helpful to have people who aren’t just sympathetic but empathetic.
Ten participants (32%) mentioned the theme of knowledge and information in their response. Participants valued what they learned during the program, whether it was from the planned education sessions, thoughts and techniques offered by the facilitator, or learning from other participants. Participant 13 wrote “The educational piece was really important to me. If I wanted to know more about any subject I could deep dive it on my own after” and participant 37 wrote “Dealing with grief, [especially] losing other support group members (i.e., watching our future). The program gave me several tools to reduce stress.” With regards to specific skills learned, 5 participants (16%) specifically mentioned aspects related to breathing and 4 participants (13%) mentioned learning new techniques to support their mental health (e.g., stress, anxiety, etc.).
What Did You Enjoy Most About the Program?
Participants were also asked what they enjoyed most about the program on our internally developed questionnaire. Responses heavily overlapped with the MYCaW question of “what was most important to you” in that “connecting with others” and “knowledge and information” were the 2 most common themes. In addition, 9 participants (29%) wrote positive feedback about the facilitator.
What Would You Change About the Program?
Participants were asked what they would change about the program. The most common response, explicitly written by 9 of the 31 participants (29%), was that they would not change anything. The next 2 most common suggestions for improvement included 7 participants (23%) who thought it would be best to make the program longer than 6 weeks, and 4 (13%) who suggested to shorten the duration of each weekly class. Table 4 includes a breakdown of all qualitative questions, including example quotes for each of the prominent themes.
Thematic Review and Sample Quotes.
Discussion
In our evaluation of Inspire Now: A Program for People with Lung Cancer, study participants saw significant improvements in QOL, overall wellbeing, and self-identified concerns at the end of the program. To our knowledge, this is the first evaluation of a multimodal home-based group program for people with lung cancer. Given the unique multidimensional nature of the program, it is difficult to find similar comparators. However, our findings are in line with research in other cancer types that have shown improvements in QOL for people attending online, home-based programs. 15 Additionally, several components of the program are supported by evidence in various cancer populations, with the strongest data in breast cancer. Research on yoga for cancer patients has generally been favorable for QOL and specific symptoms such as fatigue and anxiety.30,31 Support groups—both professionally and peer-led, including for those with advanced cancer—are also generally associated with positive outcomes.15,32,33 Mindfulness-based interventions, which share some overlap with yoga, have demonstrated benefit for overall QOL and symptoms such as anxiety, depression, and fatigue in patients with cancer. 34 Finally, the use of virtual delivery for programs and peer-support is becoming more common, and early literature is suggestive of benefit.35,36 Collectively, this data suggests that our findings are in line with existing research in this field.
Both FACT-L Total and FACT-G scores, which measure multidimensional QOL, showed clinically and statistically significant improvements. The emotional, functional, and social domains of the FACT questionnaire all had significant improvements, whereas the physical and lung cancer symptom domains did not. Similarly, participant-identified concerns and overall wellbeing measured by MYCaW were significantly improved. However, in contrast to the FACT data, where physical and lung cancer symptoms did not improve, 15 out of 17 participants noted an improvement in physical concerns on the MYCaW questionnaire. Although we do not know the reason for this discrepancy, there are a few considerations. Firstly, differences in the FACT and MYCaW findings may reflect how these tools are completed by participants. MYCaW asks participants to identify up to 2 concerns they want the program to address. As such, they likely chose issues they believed the program could help with, potentially excluding common cancer symptoms like nausea. Therefore, the program may have been more effective for the specific physical concerns participants reported on MYCaW compared to the broader range of physical concerns assessed by the standardized FACT. Secondly, FACT has multiple symptoms included in the subscale score, which lends itself to less variance. This finding highlights the potential benefit of patient-centered evaluation tools such as the MYCaW in capturing nuanced and personalized health experiences of participants that standardized questionnaires overlook.
The program was well received by participants. The most valued aspects included connecting with others and knowledge gained through the program. Nine participants expressed a desire for the program to either run longer over more weeks, have a shorter duration per session, or both. Therefore, a future consideration for this or similar programs could be to run a program of longer duration (eg, 8-10 weeks) where each class is 2 hours in duration; however, it should be noted that the same number of participants specifically wrote that they would not change the program in any way.
The virtual delivery of the program received an overwhelmingly positive response. The research staff were able to enroll at least 7 patients per session, and those enrolled in the study attended a median of 5 of the 6 classes. Qualitatively, participants noted that the program was more accessible, and some even stated they felt more comfortable participating in group discussions while in the comfort of their own home. Comparing data from this study to the in-person pilot study previously published, 16 attendance rates and program satisfaction scores were comparable, as were changes in QOL and participant-identified concerns. This suggests that the virtual format was feasible and potentially equivalent in efficacy for QOL and patient-identified concerns. While there were no negative responses from our population, it is important to note that participants knew the program would be conducted virtually; thus, those who did not have access to a computer or who were uncomfortable using one would not have enrolled. Although virtual formats may enhance access for people living out of province or in rural communities, there is also evidence that those living in rural areas, especially Indigenous and First Nations communities, have decreased internet access compared to urban areas.37,38 Therefore, while virtual delivery is an excellent option, there are likely still drawbacks that our study was unable to assess.
This program used a combination of yoga therapy and group support. Yoga has ample evidence to support its use for anxiety and depression in people with cancer. 39 Although research specifically in lung cancer populations is more limited, the available data suggests benefits for QOL in various stages of cancer and its treatment.40 -44 Studies have also shown significant associations between social supports and outcomes for people with lung cancer, such as QOL, disease progression, depression, and anxiety.45,46 Group programs are a form of social support; however, the study of multimodal programs in people with cancer is not common, especially for those with lung cancer. A 2017 systematic review in people with non-metastatic breast cancer showed that home-based support programs improved QOL shortly after program completion, but the results did not persist at 1, 3, or 6 months. 15 Continued social and emotional support may be necessary to see sustained changes in QOL. The long-term effects of the program on QOL is not something we are able to assess in this study.
Strengths and Limitations
To our knowledge, this is the first study evaluating a multimodal group program for people with lung cancer. Enrollment over multiple sessions minimizes the possibility that the observed effects were due to a single, unusually effective session. It also reduces the potential impact of unique circumstances, such as the COVID-19 pandemic, which enhances the generalizability of the findings. In addition, the mixed methods evaluation provides a deeper understanding of the effects of the program. The inclusion of validated patient reported outcomes alongside the subjective experience of the program is critical to an intervention of this type and important for its evaluation. The qualitative responses in particular highlight why people seek out these programs and what they most value, which can help guide the development of similar programs to best address patient needs.
This study also has limitations which should be considered. The study participants may not be representative of the broader lung cancer population. Notably, study participants were predominantly female, whereas lung cancer rates are similar among men and women. 47 As this study was observational, there is likely selection bias present which may impact findings. People who are not interested in yoga, group support, or integrative therapies may have been less inclined to enroll. Additionally, people interested in these practices may differ fundamentally from those who are not. For example, people who practice yoga are more likely to be female and of a higher socioeconomic status. 48 As already mentioned, only those comfortable with the virtual delivery would enroll. Collectively, these factors impact the generalizability of our findings. We did not follow participants after program completion; thus, we cannot comment on the long-term durability of the measured outcomes. The structure of the program was developed around the skills of the program facilitator and the availability of experts to give presentations on various topics, which limits the external validity of the program. Participants also did not comment on class size, and it is uncertain if the program could be expanded to include more participants. Data from this study suggests the program is effective for class sizes up to 14 participants. We did not collect information on participant location, particularly whether they resided in urban or rural areas, which could have provided valuable insights to the results. We cannot discern which aspects of the program provided the most or least benefit. Although participants commented on which aspects of the program were most important to them, we cannot infer to what degree these aspects impacted QOL. Our small sample size increases the risk of Type I error (false positive result); however, as the effectiveness of home-based programs for improving QOL in other cancer types has been demonstrated, 15 our confidence in the findings is strong. Finally, given the observational nature of the study, we cannot be certain that the observed benefits were attributable solely to the program, as other interventions or external factors may have influenced the outcomes.
Conclusions
In summary, this 6-week multimodal program of yoga, education, and group support for people with lung cancer improved quality of life, participant-identified concerns, and overall wellbeing upon program completion. Participants highly valued the connections they made and the knowledge they received from the program. The program was feasible to run virtually and received a positive response from almost all participants. Future research should evaluate the sustainability of these outcomes by gathering long-term qualitative and quantitative data after the completion of the program.
Supplemental Material
sj-docx-1-ict-10.1177_15347354251385246 – Supplemental material for Enhancing Quality of Life in People With Lung Cancer: An Integrative Program of Yoga, Education, and Group Support
Supplemental material, sj-docx-1-ict-10.1177_15347354251385246 for Enhancing Quality of Life in People With Lung Cancer: An Integrative Program of Yoga, Education, and Group Support by Ellen Conte, Mark Legacy, Anne Pitman, Mohamed El Sayed and Dugald Seely in Integrative Cancer Therapies
Footnotes
Acknowledgements
We would like to acknowledge the contributions of Anne Pitman, who was instrumental in developing and facilitating the program. We would also like to thank and honor Andrea Redway and Jill Hamer-Wilson for their support in developing and championing this program, and for their lung cancer advocacy.
Ethical Considerations
This study was approved by the research ethics board of the Canadian College of Naturopathic Medicine, CCNMREB031.Seely.Psihogios.
Consent to Participate
All study participants signed an informed consent form prior to taking part in any study activities. The details of the study were explained, and all questions were answered. Each participant was given adequate time to review the consent form. A copy of the signed consent form was given to each participant.
Author Contributions
DS and AP conceived of the study. DS, EC, and ML contributed to study design. EC and ML recruited participants. ML collected and aggregated participant data. EC, ML, ME, and ER contributed to qualitative and quantitative statistical analysis. All authors contributed to data interpretation and manuscript writing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ottawa Integrative Cancer Centre Foundation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Additional data for this study is available by request only. Please contact the senior corresponding author, Dugald Seely, at
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.