
Abstract
Interest in integrative oncology (IO) is growing globally. Patients with cancer are actively using traditional complementary and integrative medicine (TCIM) as part of their cancer and survivorship care. Published studies from around the world report increasing use of TCIM by people living with cancer. This article summarizes the presentations that took place during a symposium titled, “Integrative Oncology: International Perspectives” at the International Research Congress on Integrative Medicine and Health in Baltimore, 2018. The purpose of the presentations was to examine whether cancer services across a variety of geographical regions, including Australia, Canada, the United States, and the European Union, were actively responding to cancer survivors’ demand for TCIM. The presenters highlighted utilization rates and both facilitators and barriers to the provision of IO services in their respective countries and regions. The audience discussion following the presentations drew out many noteworthy perspectives.
Keywords
Introduction
Advances in cancer treatment and prevention have led to the reduction in mortality from cancer, but as cancer survivors live longer, they are often left with side effects related to their conventional treatments or symptoms resulting from their cancer. Survivors frequently seek to address these needs with traditional complementary and integrative medicine (TCIM). A meta-analysis of surveys describing TCIM use in adult cancer patient populations from Australia, Canada, Europe, New Zealand, and the United States reported a rise from an estimated 25% in the 1970s and 1980s to more than 32% in the 1990s and to 49% after 2000. 1
Integrative oncology (IO) has emerged within hospitals and community settings in response to the increasing role that people with cancer and survivors have in managing their own care, the growing usage and evidence-base of TCIM, and the importance of a therapeutic alliance between conventional cancer care and TCIM that respects the treatment preferences and values of patients (Box 1). 2 The development of IO services, however, is often ad hoc and fragmented, reflecting local factors rather than coordinated regional or national planning and policy. Consequently, despite the overall high use and demand for TCIM, at least for some countries, there continues to be a mismatch between patients’ needs and IO service provision.3-5
Definition of Integrative Oncology.

In this article, leading health care professionals and researchers from 3 continents (North America, Europe, and Australia) present an overview of IO service provision in their regions and its implications for clinical practice, health service delivery, education, and research. We have sought to identify common trends and future directions for IO service provision; gain insight into unmet patient needs and the financial, informational, cultural, and logistical facilitators and barriers for IO; and obtain knowledge about organizational and educational aspects, including strategies and policies, to support the development and uptake of IO services.
The article draws on the Integrative Oncology: International Perspectives symposium presented at the 2018 International Congress on Integrative Medicine and Health in partnership with the Academic Consortium for Integrative Medicine and Health, held in Baltimore in May 2018. Table 1 provides a summary of the information provided by each speaker.
International Comparison of IO Services.

Abbreviations: TCIM, traditional complementary and integrative medicine; IO, integrative oncology; NCI, National Cancer Institute; NHS, National Health Services; NHP, Natural Health Practititoners; KOKON, Competence Network for Complementary Medicine in Oncology; ECIBC, European Commission Initiative on Breast Cancer; CALD, Culturally and linguistically diverse.
United States IO Landscape
Estimated TCIM use in the United States is 38% across the general population. 6 Prevalence is even higher among cancer patients and survivors, with 50% to 60% using TCIM. 1 Both hospital and independent IO clinics offer various forms of TCIM services, including mind and body practices, natural products and dietary supplements, and lifestyle modifications (dietary consultation/exercise programs). In hospital and cancer centers, TCIM is mainly offered in a coordinated, integrative manner alongside conventional cancer services (see Box 1).
Over the past 8 years, TCIM use in US cancer centers has steadily increased. According to a recent systematic review, the most frequent services offered within the 45 National Cancer Institute (NCI)-designated comprehensive cancer centers were acupuncture and massage (73.3% each), meditation and yoga (68.9% each), and consultations on nutrition (91.1%), dietary supplements (84.4%), and herbs (66.7%). 7 In comparison to a previous study conducted in 2009, this translates to more than 30% growth in integrative medicine modality offerings: acupuncture (30.3%, P < .005), massage (30.7%, P < .002), meditation (32.8%, P < .001), and yoga (30.6%, P < .002). Compared with the 2009 results, the number of cancer centers providing information on integrative medicine has also increased for all modalities, except guided imagery. In addition, more than 60% of NCI-designated cancer centers now offer physician consultations on integrative medicine. 7
Extensive research on the effectiveness of some TCIM modalities commonly used by cancer survivors has led to several published guidelines on indications for their use.8,9 IO services at US cancer centers utilize these guidelines along with available therapies to provide personalized, evidence-based treatment for patients. In major US IO centers, patients typically meet with an integrative medicine physician for an initial consultation that covers diet, lifestyle, and natural products. Together, the physician and patient develop an individualized integrative medicine prescription that best utilizes appropriate modalities during and after cancer treatment. Often, acupuncture and massage therapy are recommended for pain reduction. Meditation, music therapy, and other types of mind-body approaches are recommended for anxiety and stress reduction. Exercise is typically recommended to all cancer patients and survivors because of robust evidence on its positive impact on quality of life. 10
In the United States, IO services are often grouped with palliative care as a component of supportive care services. In major cancer centers, IO services are offered both within the hospital setting to inpatients and outpatients and at other community locations for outpatients. Financially, TCIM services are typically paid for out-of-pocket. Whereas a few TCIM services such as acupuncture or integrative medicine consultations may be covered by some insurance companies, many are not. Philanthropy may cover the cost of some hospital inpatient TCIM services or group classes, such as yoga. The types of TCIM services offered outside hospital settings by independent clinics, however, can vary significantly and are rarely covered by health insurance.
TCIM literacy in oncology for physicians is being facilitated by the development of specific training courses. Both the University of Michigan 11 and Memorial Sloan Kettering (MSK) 12 offer an IO fellowship for junior physicians. MD Anderson Cancer Center 13 offers integrative medicine program workshops to health care professionals interested in learning about IO care. MSK also offers oncology courses for acupuncturists and provides a comprehensive website on natural products and other TCIM therapies—MSK About Herbs 14 —which has had over 20 million visits to date.
Barriers to the provision of IO services include a lack of sustainable funding for IO research, truly integrative models that implement IO at the time of cancer diagnosis, business models that increase the impact and efficiency to deliver IO care, and formal training programs to cultivate IO practitioners. 7
In summary, IO services offered in the United States by major cancer centers are usually evidence based and focused on major modalities such as diet, lifestyle, mind-body approaches, and natural product advice. The provision of IO services is rising because of a range of factors that include patient demand. Independent clinics also offer TCIM that may or may not be as evidence based and is often not covered by insurance. Further standardization in this field may be warranted to optimize the quality of IO care provided across the United States.
Canadian IO Landscape
A large proportion of Canadian cancer patients and survivors use TCIM but have little access to hospital-based IO services. Estimates for TCIM use by adults with cancer in Canada range from 47% 5 to 61%, 15 and up to 91% in some populations. 16 For pediatric cancer populations, recent surveys indicate that between 29% and 64% use TCIM following diagnosis.17-19
The provision of TCIM services is primarily home- or clinic-based and is available mainly in urban areas. TCIM is typically offered through solo practitioner practices; but some multidisciplinary practices exist. Models of care where TCIM is integrated with the conventional health care system are rare. Indigenous healing traditions have also been minimally addressed within conventional care settings.
Over the past decade, several IO services have emerged in Canada. These IO services typically operate without any formal relationship with a publicly funded cancer center. Two of the most prominent include the following:
InspireHealth: Led by a medical doctor with a team of TCIM and allied health care professionals, this center offers a range of therapies, programs, and classes to patients and their family members. 20 Funding comes from government grants, philanthropy, fee-for-service, volunteers, and membership fees.
Ottawa Integrative Cancer Centre (OICC): The OICC opened in 2011 and is a multipractitioner, naturopathic doctor–led center active in both research and clinical care for patients. It offers a range of services, including acupuncture, clinical nutrition, massage therapy, mind-body medicine, naturopathic medicine, physiotherapy, psychotherapy, traditional Chinese medicine, and yoga therapy.
Although independent clinics exist, hospital-based IO services are limited in Canada. Examples include the following:
Tom Baker Cancer Centre, Calgary: The IO Program focuses on mind-body therapies, including mindfulness-based stress reduction, yoga, and expressive arts. Education resources are provided, including a monthly seminar.
Jewish General Hospital, Montréal: The volunteer-run Hope and Cope Program offers supportive care services to patients and caregivers. The iThrive program offers a variety of therapies, including peer support, meditation, exercise, art therapy, nutrition information sessions, and massage. Specialized programs for young families and adults living with cancer are available.
Ontario and Alberta: The Wellspring Program is a community-based network of 9 support centers that provide complementary therapies and supportive services to cancer patients and family members.
The lack of accessible IO programs in Canada means that the majority of patients navigate TCIM services independently, with little guidance from oncology health care professionals. 5 As a result, patients often are misinformed and incur significant costs on ineffective or untested natural products and potentially use therapies that interact negatively with conventional treatments or are unsafe. Stress and anxiety, and loss of trust in the therapeutic relationship with physicians are also consequences.21,22
The Canadian health care system provides no coverage for TCIM services except through private health insurance. Access is limited to those who have coverage or can pay out-of-pocket for TCIM services. The fee-for-service funding model that most TCIM practitioners and clinics rely on creates a significant challenge to TCIM uptake in Canada and the development of IO services. In a health care system where hospital- and community-based medical services are provided at no cost to the user, the idea of paying out-of-pocket for health care services, such as TCIM, is antithetical to the core principles of universality and accessibility. Recently, however, the perceptions regarding a fee-for-service model have changed because of changes to the Canadian health transfer system that may reduce funding for some regions. 23 To be successful, IO services in Canada will need to be creative in seeking funding from government, philanthropic, fee-for-service, and grant sources and utilize fee structures, such as subsidized care or sliding scales for low-income patients, that support equity and accessibility.
There are several additional challenges to IO services in Canada. Overall, the integration of TCIM within the conventional health care system has been limited, despite 80% of Canadians reporting using some form of complementary therapies. 24 Culturally, conventional medicine has not been receptive to TCIM, evidenced by numerous editorials and letters in leading Canadian medical journals and newspapers.25,26 This reluctance may be a consequence of the limited TCIM content in health professional education programs, 5 which in turn may result in conventional health care professionals perceiving there to be a lack of evidence and questioning the value of TCIM.
There have also been several high-profile cases in Canada in which patients of TCIM practitioners have been harmed or died unexpectedly. The subsequent media attention may have affected conventional health care professionals’ attitudes toward TCIM, including the safety of IO. These cases have also raised questions about the regulation of TCIM practitioners in Canada, which differs across provinces and territories with regard to which practitioners are regulated and their scope of practice.
There have been, however, some beginning steps toward IO in Canada. For example, the University of Toronto in 2015 developed a continuing education program for oncology pharmacists that included a TCIM component. The OICC has also provided educational and observation opportunities in IO for health care professionals and students. At a practice level, the Complementary Medicine Education and Outcomes (CAMEO) program opened in 2007 at the British Columbia Cancer Agency with the aim of supporting patients, family members, and oncology health care professionals to make safe and informed decisions about complementary therapies. 27 A wide range of decision support and knowledge translation programs were developed by CAMEO, including a patient and family member education program, a one-on-one decision support program, and a variety of education and synthesis resources. More than 1500 individuals received services from CAMEO in the 7 years it was in operation, and education programs for patients and health care professionals continue to exist online. 28 Finally, the Canadian Cancer Trials Group recently announced the formation of the Symptom Control disease site, which will consider both pharmaceutical and nonpharmaceutical interventions, including TCIM. The acknowledgment of complementary therapies within this conventional research agency bodes well for the future of IO in Canada.
Australian IO Landscape
The prevalence of TCIM use by people with cancer living in Australia increased from 22% in 1996 29 to 65% in 2008.29,30 Whereas the majority of TCIM is accessed in the community, either self-prescribed or from a TCIM practitioner in the primary health care sector, there is evidence of increasing access from specialized cancer services.
Results from a 2016 study found that around a quarter of institutions with specialized secondary care cancer services offered some form of IO service.31,32 Like general cancer services, IO services were clustered mainly in urban areas. Compared with earlier surveys,33,34 there was a notable growth in the number of IO services, with a little more than half of the 71 services being introduced in the past 6 years and an additional 12 services in the planning stages.
Although most of the cancer services surveyed in 2016 offered a very limited amount of IO,31,32 at least 10 major IO centers in Australia have been identified. 35 Examples of the different types of IO centers include the following:
Olivia Newton-John Cancer Wellness & Research Center: This is an adjunct to a public hospital where the majority of IO services are funded by the hospital; services include oncology massage, acupuncture, and music therapy.
Solaris Cancer Care: This is a registered charity with around 250 volunteers providing free or low-cost IO services across 5 centers in hospital and community settings; services include massage, reflexology, reiki, yoga, tai chi, and art. 36
Chris O’Brien Lifehouse: This is a not-for-profit cancer hospital that offers subsidized and low-cost IO services, including oncology massage, acupuncture, exercise, yoga, tai chi, meditation, reflexology, and integrative medicine consultations. 37
Similar to the 10 IO centers evaluated in 2015, 35 the vast majority of IO services offered by the cancer services surveyed in 2016 were mind and body practices.31,32 Massage, touch, or body alignment therapies were common (76%), with a little more than half of the massage services being provided by a certified oncology massage therapist. Psychological well-being services such as mindfulness, meditation, art therapy, and music therapy were also very common (72%). Movement modalities such as tai chi, qi gong, and yoga were on offer by 39% of the cancer services. Notably, none of the TCIM practitioners providing these services are statutorily regulated in Australia. Three TCIM professions are statutorily regulated (Chinese medicine practitioners, osteopaths, and chiropractors). However, only 12% of IO services offered acupuncture, and no Chinese herbal medicine, chiropractic, or osteopathic services were provided.
Evidence-based IO advice or consultations from either a medical practitioner or pharmacist were provided by 18% of the IO services.31,32 Other than this, access to natural products or recommendations regarding their use were rarely available. The finding highlighted an obvious mismatch between the low levels of service provision compared with the much higher reported use of natural products. Reasons for this observation are yet to be fully investigated.
Funding for IO in Australia is mixed, with services relying on multiple sources (patient payments, insurance rebates, philanthropy, and volunteers).31,32 Mostly, patients contributed toward the cost of the therapy, with the exception being IO services provided by volunteers. Patients with private health insurance may receive partial reimbursement for some of these IO services, and none of the services provided attracted public health insurance rebates. Equity is, therefore, a concern; cancer survivors have partially attributed the lack of funding to perceptions that IO is a luxury service. 38 However, this notion was strongly refuted by IO users claiming that it is not “just feel good stuff” and is essential to recovery. 38 Others have described IO services as “an oasis in the hospital.” 36
Access to reliable IO information is important not only for patients and their caregivers but for oncology health care professionals. Surveys in Australia consistently find that oncologists have self-identified knowledge gaps and want to learn more about IO.39-41 This finding is not surprising because currently there are no formal IO training programs for health care professionals in Australia. In addition, there is very limited consideration of IO in institutional guidelines and policies. Ironically, the paucity of information, guidelines, and training for health care professionals is contrasted with an exponential growth of research in the field of IO, both in Australia and internationally.
In summary, although the growth of TCIM offered to patients with cancer in a hospital environment appears to be growing in Australia, for the most part, the scope and “integrative” nature of IO services remains limited.32,35,38 Many of the IO services in Australia exist precariously, relying on a base of fundraising and philanthropic donations and high out-of-pocket costs that reflects a lack of top-down policy and funding support from both the public and private health sectors. It is uncertain whether the growth in IO will continue in Australia and the existing centers will prove sustainable.
The European IO Landscape
TCIM use by patients with cancer in Western Europe is estimated to be 37% but varies considerably across the different European countries, with higher prevalence in German-speaking (41%) and Mediterranean (39%) countries and lower prevalence in the United Kingdom (32%) and Scandinavia (31%). 1
Studies suggest that there has been an exponential increase over the past 15 years in the number of cancer centers offering IO across Europe. A mapping study conducted in 2013 captured those public health services providing IO services. 42 Information from 123 (52.1 %) of the 236 cancer centers contacted found that nearly half of the responding centers (47.5%) provided IO services. IO services were predominantly provided by the public health sector (69.9%), followed by a smaller number of privately owned centers (19.6%).
Many of these centers state that they have treatment protocols to guide therapy.42,43 The most frequently provided therapy was acupuncture (55.3%). In contrast to the high service provision of mind and body practices by IO services in Australia, Canada, and the United States, IO centers in Europe offered more natural products and traditional medicine; the most commonly provided were homeopathy (40.4 %), herbal medicine (38.3 %), and traditional Chinese medicine (36.2%). Treatments were mainly directed at reducing adverse reactions to chemotherapy and radiation (23.9%), in particular nausea and vomiting (13.4%), pain (10.9%) and fatigue (10.9%), secondary symptoms of iatrogenic menopause (8.8%), and anxiety and depression (5.9%). 42
Despite the relatively low prevalence of reported TCIM use by patients with cancer in Italy (22%; 95% CI = 10%-35%), 1 many regions are integrating TCIM into the public hospital systems. These integrative services are available to all patients, including those with cancer. In a survey of the region of Tuscany, 91 public clinics providing TCIM services were identified. Of these 91 clinics, 45 provided acupuncture and traditional Chinese medicine, 23 homeopathy, 13 Western herbal medicine, and 10 other nonconventional therapies (eg, manual therapies). 44 TCIM was provided after the payment of a fee similar to the other medical specialties (24€), but it was free of charge for patients with cancer, with the remaining costs being covered by the public health system. Like many pharmaceuticals, natural products incur out-of-pocket costs (eg, homeopathic, herbal medicines, dietary supplements).
IO services provided by the National Health Service (NHS) in the United Kingdom are considerably different to what is generally offered in Europe. A 2012 survey reported that around 105 NHS cancer services were offering TCIM. 45 In contrast with Europe, mind and body practices were mostly offered. Counseling, which is not typically considered a TCIM therapy, was most frequently provided (82%), followed by reflexology (62.0%), aromatherapy (59.1%), reiki (43.0%), and massage (42.2%). 45
Regarding training and education of health care professionals, European initiatives such as the Competence Network for Complementary Medicine in Oncology have been established to develop, implement, and evaluate an interdisciplinary competence network in IO. Several courses on integrative medicine and IO are available in European universities, with chairs of complementary and integrative medicine at the University Charité in Berlin, University of Bern, University of Duisburg-Essen, University of Frankfurt, University of Zurich, Friedrich Schiller University in Jena, University of Wien. In Italy, the University of G. Marconi in Roma offered a 2-year master’s degree in IO from 2014-2017, which is now operational at the University of Chieti. It also worth noting that every hospital and institution surveyed in 2013 that offered IO services also periodically provides refresher and continuing medical education courses for their health care professionals.
Along with Europe-wide initiatives, countries such as Italy have been proactive in the research and development of IO clinical practice. A national working group of IO was established in 2012. The working group is composed of experts from different TCIM fields who periodically meet to define IO therapeutic protocols aimed at reducing the adverse effects of anticancer treatments and improving the quality of life of cancer patients and survivors. Also, the Association for Research on Integrative Oncological Therapies—ARTOI was founded in 2012 to deepen the study, research, and application of oncological treatments through the integrated use of multiple therapeutic options. 46
The presence of IO services in public and private hospitals across Europe, where oncologists and experts of TCIM work side by side, has helped overcome many cultural barriers and mutual distrust. However, a relative lack of knowledge of IO therapies still exists on the part of many conventional physicians that prevents a full cultural acceptance of this process of integration. Top-down leadership and policy has been observed to help break down these professional cultural barriers. A small but relevant example of positive collaboration between oncologists and experts in TCIM was the Resolution no. 418/2015 passed by the Tuscan Regional Government and promoted by the Tuscan Tumor Institute 47 and the Tuscan Regional Centre of Integrative Medicine. The resolution ratified the use of TCIM to treat some cancer-related symptoms and side effects of anticancer therapy and, in compliance with equality in health care, to guarantee patients the opportunity to integrate TCIM therapies that are considered safe and effective and have few side effects with their usual oncological treatments. 48 As a consequence of this regional policy, there are now at least 8 qualified and accredited IO public hospital clinics working in close collaboration with the oncology departments; all IO consultations provided by these clinics incur no out-of-pocket costs; a patient information flyer about TCIM in oncology was created and is distributed by all the oncology departments of Tuscany 49 ; 2 international IO congresses in 2016 and 2018 were held in collaboration with Tuscany Tumors Institute and attended by hundreds of physicians, including many oncologists; and finally, a specific research program for the evaluation of the effectiveness of TCIM for cancer care was financed with regional funds. 50
Discussion
The range and type of IO cancer services across the 3 continents and the ways in which patients access TCIM as part of their cancer care varied considerably both within and between the countries presented. Notable differences were identified in the types of TCIM services commonly offered by IO centers and associated out-of-pocket costs. Common across all services was the aim to treat the whole person, to be patient centered, and to appropriately integrate TCIM with conventional cancer care. Consistently, patient demand for IO was an important driver that was modified by a variety of cultural attitudes, health service policy, and funding models. The desire to provide safe, evidence-based therapies was only one of many complex factors influencing service provision. Equitable IO services funded by the NHS aimed at minimizing out-of-pocket costs appeared to be more common in Western European countries and the United Kingdom.
Regarding the types of IO services provided, concerns around safety, particularly the risk of interactions with active cancer treatment and insufficient evidence of benefits, are postulated as significant barriers to IO support from oncologists.31,51 This includes uncertainties around quality of care, which is related to the regulation of TCIM practitioners and natural products.
The findings from this symposium session identified various contradictions and factors other than potential benefits and risks that influenced service provision. For example, in Australia, it is unclear why the majority of TCIM practitioners working in IO services were self-regulated or unregulated professions, whereas acupuncturists, a regulated profession with an adequate evidence base and safety profile, were less commonly provided. IO physicians were available in most IO centers in the United States and increasingly in Western Europe, yet IO physicians are few and far between in the 3 Commonwealth countries. Compared with Europe, the services of IO physicians in other countries are restricted largely to the provision of advice and guidance, rather than “prescribing” natural products. The cultural acceptability of natural products and traditional medicine was proposed as a reason why products with sufficient evidence of safety and effectiveness were commonly available in IO services in Western European countries, yet rarely dispensed by IO services in other countries. Potential advantages of an IO service dispensing natural products include improved quality control, 52 greater convenience for the patient, better follow-up care, and potentially lower out-of-pocket costs.
There was evidence suggesting a steady growth in the number of cancer centers offering IO in North America, Australia, and Western Europe. It is likely, however, that in many of the countries and regions reviewed in this article, demand for IO services in general, along with specific TCIM interventions, remains greater than supply. As such, many people will continue to access TCIM therapies and services in ways that are neither coordinated nor integrated with their conventional cancer care, and for some, there will be ongoing inequities with regard to access and affordability.
Access also depends on the patient actually finding the IO service or a provider who is skilled in treating people with cancer and being informed about what TCIM is available and how it might support their cancer care. 38 Information about IO is in the top 5 unmet needs for cancer survivors.53-57 It is estimated that less than one-fifth of cancer patients and survivors who use TCIM have done so at the recommendation of a medical practitioner. 58 For those patients who have heard about TCIM, many seek to have an informative discussion about use and prefer to access these services from a practitioner skilled in treating patients with cancer. 38 Standardized, evidence-informed patient information in paper and online formats; proactive continuing education of TCIM and conventional health professionals; and developing clinical practice guidelines and improving access to reliable, evidence-based information about TCIM indications, interactions, and contraindications for health professionals were used in various ways by all the countries and regions as a means of improving IO knowledge and communication.
Challenges with funding and the provision of affordable IO services was a common and substantial barrier experienced across all 3 continents. Improved survival coupled with an aging population means that cancer prevalence will continue to increase and threaten the sustainability of many cancer services, including IO. Demonstrating the value of IO necessitates that along with providing quality services that are safe, efficacious, and cost-effective, 59 the outcomes that patients consider are important and their experiences with the services they receive will increasingly become the deciding factor. 60 It is critical that the “value proposition” is understood and communicated to the dominant biomedical culture within the health service. What does IO offer? What is IO’s health, social, and economic value? What are the costs and risks (including the risk of not offering IO services and evidence-based advice)? What do patients want and what are their experiences with cancer services that do and do not provide IO?
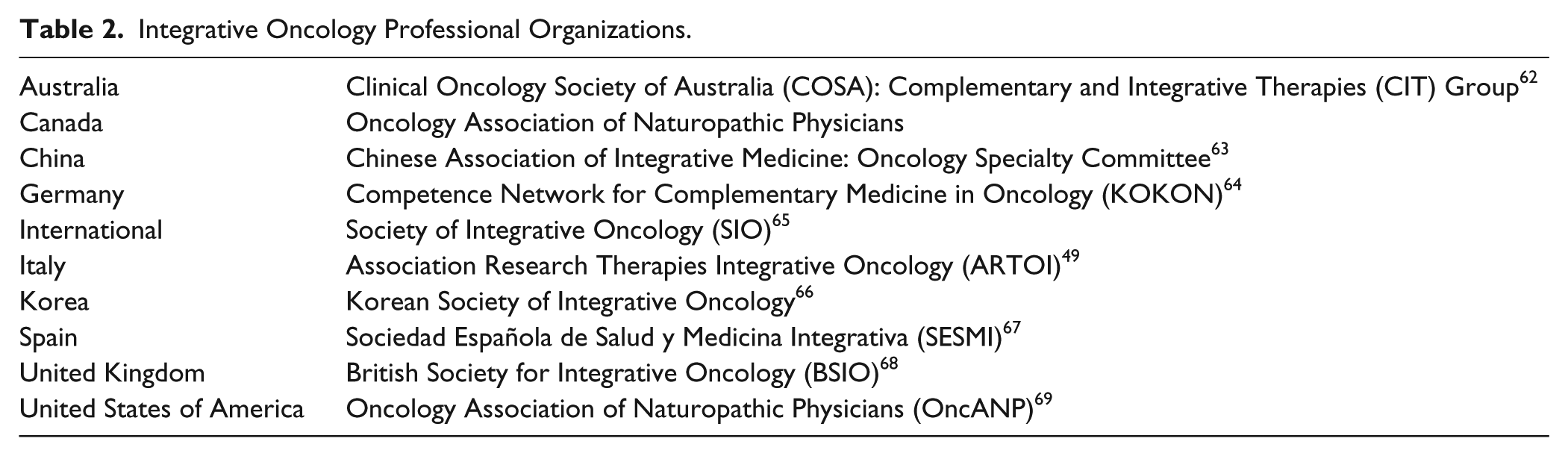
During the symposium presentation and ongoing discussions, the usefulness of comparative research of health services and policies was affirmed as a way to identify overarching strategies to facilitate the establishment or expansion of an IO service. Professional organizations have emerged in many countries in response to the growth of IO and present a way to develop evidence-informed IO (Table 2). Strategies for establishing and expanding IO services identified at the symposium are similar to findings elsewhere 61 (Table 3). In collaborating internationally, we hope to evaluate not just the health care outcomes but the economic and social value of integrating TCIM into cancer services. All presenters spoke to the need to continue discussions and to collaborate internationally on the following:
a minimum data set of questions to include when mapping IO service provision in cancer centers for comparable data between regions and countries, and over time;
a minimum data set of patient-reported outcome measures to be collected and, ideally, pooled for comparison on IO health outcomes and experiences; and
safe and effective approaches to providing biologically based therapies within a supportive cancer care context.
Integrative Oncology Professional Organizations.
Strategies for Establishing and Expanding Integrative Oncology (IO) Services.

Abbreviations: TCIM, traditional complementary and integrative medicine.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.