
Abstract
Background:
Lung cancer is the leading cause of cancer mortality in Canada, yet patients are often under-supported. A six-week program called Inspire Now, created to address unmet supportive care needs, was evaluated in this study. Feasibility and preliminary outcomes were assessed in order to inform future changes to the program.
Objectives:
(1) Assess the feasibility of the program and its evaluation; (2) pilot the collection of patient-reported outcomes; (3) identify outcomes that may be positively influenced; and (4) inform program modifications.
Methods:
Participants were recruited from the first session of Inspire Now for an observational pilot study. The primary outcome was feasibility. Secondary outcomes included within-person changes in Functional Assessment of Cancer Therapy – Lung (FACT-L) and Measure Yourself Concerns and Wellbeing (MYCaW), and program satisfaction and qualitative experiences of participants and facilitators through internally-developed questionnaires and semi-structured interviews. Analysis was primarily descriptive, within person changes in FACT-L and MYCaW were analyzed using the Wilcoxon signed-rank test and qualitative data was assessed for common themes.
Results:
The program and its evaluation were feasible; 8 of 9 (89%) participants consented to the study, median attendance was 6 of 6 sessions (IQR 4.5-6), and questionnaire completion was 100% at baseline and 75% at follow-up. There were clinically meaningful improvements in MYCaW concern 1 (−1.2, 95% CI −2.0 to −0.4) and overall wellbeing (−0.9, 95% CI −2.1 to 0.4). Seven of eight FACT-L sub-sections trended toward improvement, with absolute changes ranging from −1.7 to 10.8%. Participant feedback was overwhelmingly positive; group support and social interactions were highly valued.
Conclusions:
The group intervention for people with lung cancer was feasible to both run and evaluate. Participants responded positively to the program. Findings will inform changes to future sessions and an analysis of multiple sessions is planned.
Keywords
Introduction
Lung cancer accounts for the greatest incidence of cancer and cancer mortality worldwide, 1 and in Canada is the leading cause of cancer death.2,3 Beyond a high mortality rate, people treated for lung cancer often experience psychological distress, physical disability, and increased health care needs. 4 Despite the burden of lung cancer on Canadians and high mortality rates, it receives less research funding5,6 and charitable donations 7 compared to other cancers. This speaks to a larger problem of a lack of support for people with lung cancer. These imbalances may reflect a “blame the victim” mentality (ie, an assumption that choosing to smoke is the cause for lung cancer), 6 which may lead to stigma associated with the disease. This presents a unique and distressing situation for people diagnosed with lung cancer: having an aggressive cancer with a poor prognosis combined with little support.
Supportive care is an important aspect of cancer management that can be defined as helping a patient and their family cope with cancer and its treatment. 4 A variety of unmet supportive care needs for people with lung cancer have been identified.4,8,9 A systematic review of 53 studies on unmet needs for lung cancer broadly classified these as: physical, daily living, psychological and emotional, spiritual and existential, informational, practical, communication, social and family-related, and cognitive. 8 Among physical needs, fatigue, shortness of breath, and pain are often reported. Common unmet psychological and emotional needs include anxiety, sadness, guilt, and feeling like a burden to others. Spiritual and existential concerns include uncertainty, fear of the future, finding meaning and purpose, and balancing hope and despair. Patients with lung cancer express a need for information regarding ways they can help to improve their health and manage side effects, 4 with an emphasis on wanting information related to lifestyle factors such as diet, physical exercise, and breathing activities, 8 as well as complementary and alternative medicine. 10 Patients value services such as peer-support and counseling to reduce social isolation and loneliness that may in part develop due to a perceived stigma associated with lung cancer. 8
To address unmet needs and provide direct support to people living with lung cancer, a program, called Inspire Now, was developed and facilitated by a certified yoga therapist (C-IAYT) at the Ottawa Integrative Cancer Centre (OICC) with the help of the clinic director and two survivor advocates from Lung Cancer Canada and The Ottawa Hospital (Supplementary material 1.0). The six-week program strived to address multiple needs by providing group and social support, exploring fear, stigma, and grief through facilitator-led discussions and mind-body therapies, addressing information gaps through multidisciplinary presentations, and teaching yoga techniques and breathing practices to support psychological and physical concerns. A clinical practice guideline for complementary therapies in lung cancer recommends that mind-body therapies be suggested as part of a multidisciplinary approach to reduce anxiety, mood disturbance, pain, nausea and vomiting, and improve sleep and quality of life (QOL). 11 Yoga was specifically recommended to reduce fatigue and sleep disturbance, and improve mood and QOL. Since the publication of this guideline, several other small studies of yoga and yoga breathing techniques for patients with lung cancer have been published, which continue to support yoga and breath practice in this population.12-15
In this pilot study, we evaluated the feasibility of recruiting people for Inspire Now and the feasibility of a research evaluation of the program. We piloted the collection of patient-reported outcomes and subjective feedback from recruited participants, and identified specific outcomes that may be positively influenced by this program for evaluation in future sessions. Information gathered from this pilot study will help to modify the structure and content of future Inspire Now program sessions to best address patient needs.
Methods
Participants and Setting
Participants were recruited from the first session of the Inspire Now program, which was scheduled to run weekly from January 23 to February 27, 2020. Registration for the program required a diagnosis of primary lung cancer; all program participants were eligible to take part in the research evaluation. Participants were approached by a research coordinator prior to the first program session. Signed informed consent was obtained for all participants prior to any study activities.
Study Design
This was an observational study consisting of qualitative and quantitative outcome measures administered at baseline and program completion. The Inspire Now program was not created as part of this observational study, rather, this study evaluated a patient program that had already been created and was in the preliminary stages of implementation. Ethics approval was sought and provided by the Research Ethics Board at the Canadian College of Naturopathic Medicine (CCNMREB031).
Program Overview
The Inspire Now program was developed by a certified yoga therapist (C-IAYT) at the OICC with input from the clinic director and two survivor advocates from Lung Cancer Canada and The Ottawa Hospital. The program is described in supplementary material 1.0. Briefly, the program takes place in-person once weekly over six weeks, for a 3.5-hour session. Each session consists of four parts: (1) group support and facilitator lead discussion; (2) an integrative lecture on various topics of interest to people with lung cancer, (3) yoga and breath work; (4) and closes with a group check-in.
Outcomes and Outcome Measures
The primary outcome was feasibility of the program and its evaluation. Secondary outcomes included within-person changes in validated patient-reported outcome measures (PROMs), program satisfaction, and qualitative experiences of the participants, survivor advocates, and the program facilitator.
Feasibility was measured by program recruitment rates, attendance, willingness to participate in research, and questionnaire completion. PROMs were administered at the beginning (baseline) and end of the program (end of study), and included the Functional Assessment of Cancer Therapy – Lung (FACT-L) Version 4 and the Measure Yourself Concerns and Wellbeing (MYCaW) questionnaires. Both PROMs are validated; the FACT-L has been validated for use in patients with lung cancer to evaluate QOL, 16 and the MYCaW for use in mixed cancer populations to evaluate specific patient concerns. 17 Participant expectations, subjective experiences, and program satisfaction were captured by two distinct, internally-developed questionnaires. The baseline questionnaire included demographic information and three open-ended questions (Supplementary material 2.1). All demographic information was patient-reported; no medical records were reviewed. The end of study questionnaire included a seven-question survey asking participants to rate to what degree they agreed with statements about the program, and three open-ended questions (Supplementary material 2.2). Additional subjective feedback regarding likes, dislikes and overall thoughts of the program was obtained from two survivor advocates (who attended and helped develop the program) and the program facilitator through semi-structured interviews.
Analysis
Outcomes were analyzed using a primarily descriptive approach through frequency distributions and descriptive statistics. All participants were included in this analysis. Within person changes in FACT-L and quantitative MYCaW sections were analyzed using the Wilcoxon signed-rank test for those who completed both the initial and final questionnaires. The FACT-L was scored as per the guidelines set by the owners of the questionnaire (Supplementary material 3.0). MYCaW responses were coded and described according to validated and published guidelines.17-19 Qualitative feedback from MYCaW, internally developed questionnaires, and semi-structured interviews was pooled and assessed for common and unique themes.
Results
Participant Characteristics
Eight program participants were enrolled. The mean age was 59.6 years and 7 (88%) participants were female. The median time from initial diagnosis to time of enrolment was 35.6 months (IQR 10.8-56.7). All participants had advanced lung cancer (12.5% stage III, 87.5% stage IV) and the majority (75%) were on active treatment. Table 1 provides a summary of baseline characteristics.
Baseline Characteristics. a .

Patient-reported.
Feasibility
The program ran from January 23rd to March 5th (one session was rescheduled due to inclement weather). Nine people registered for and participated in the program. Eight of nine (89%) consented to the research study. The median number of sessions attended was six out of six (IQR 4.5-6). Five of the eight study participants (62.5%) had 100% attendance. Questionnaire completion rate was 100% at baseline and 6/8 (75%) at end of study.
Validated Patient-Reported Outcome Measures
Within-person changes from baseline to study completion for the FACT-L and MYCaW are presented in Table 2. Of the eight FACT-L sub-sections analyzed, seven exhibited an average increase in mean score, with relative changes in each section ranging from −2.5% to +11.4% and absolute changes ranging from −1.7% to +10.8%. The social domain exhibited the highest absolute and relative change in score, whereas the emotional domain was the only observed domain with an average decrease in score.
Validated Questionnaire Scores.

N = 6.
N = 4. See appendix 1: “How to Score Questionnaires” for information on the scoring algorithms and interpretations.
Participants were asked to identify up to two concerns on the MYCaW at baseline. All eight participants identified one concern and six identified a second for a total of 14 concerns. Psychological and emotional concerns accounted for 35.7% (n = 5) of those reported (eg, “cope mentally” and “social support”). Concerns about wellbeing, which includes issues of living well and maintaining or regaining health, accounted for another 35.7% (n = 5) (eg, “nutrition”, “make peace with dying”). Less commonly reported were physical concerns (14.2%, n = 2), and concerns related to hospital cancer treatment (14.2%, n = 2). Analysis of within person changes demonstrated improvements in mean scores for the first concern (3.5 to 2.3, an average change of −1.2, 95% CI −2.0 to −0.4) and a decline in mean scores for the second concern (3.5 to 3.75, an average change of 0.25, 95% CI −2.8 to 3.3). Mean overall wellbeing scores improved on average by 0.9 (95% CI −2.1 to 0.4), consisting of a 52% relative improvement and a 13% absolute improvement.
At program completion, five of the six participants who completed the MYCaW answered the question: “What has been most important to you?” One participant provided three answers, resulting in seven responses. All responses were positive. Three (42.9%) related to the benefit of being with others, three (42.9%) related to support and understanding provided by the program including the facilitator, and one (14.3%) related to specific educational content. Common themes were support, strength, and comfort gained through interaction with others in the group and through the facilitator. Specific responses included “discussing grief and how to find comfort in death”, “meeting others and knowing there is hope”, and “support and opportunity to build a support network”. Most participants did not identify other factors they perceived as affecting their health, thus this final open-ended MYCaW question was not analyzed.
Program-Specific Evaluation
At the start of the program, participants were most looking forward to gaining new information and connecting with others who shared their diagnosis. The words “learn” or “information” were present in six of eight responses, sometimes referring to general knowledge or information in a specific area (eg, “learning about new adjunctive therapies”). A common theme for “what do you hope to learn” was “learning to cope” with the disease. Prior to starting, participants did not identify concerns to the program material, attending sessions, or participation in general. At the end of the study, participants most enjoyed the social and group support aspects of the program, along with the interactive physical activities and breathing exercises. Two participants expressed wanting more speakers from the broader medical community and two noted the sessions were too long. When asked how they felt now compared to the start of the program, participants had varied responses from feeling the same, to feeling more calm and comforted, to feeling better in many areas.
Table 3 shows the mean scores from the seven end-of-program survey questions that had been developed internally. Mean scores ranged from 4.5 to 5 (out of 5). In the categories “I feel support and acceptance” and “Others would benefit from this program,” all participants responded with a 5 (strongly agree). Out of 42 question responses (7 per survey for 6 participants), 30 (71%) were 5, 11 (26%) were 4, and 1 (3%) was a 3.
End of Study Survey Scores.
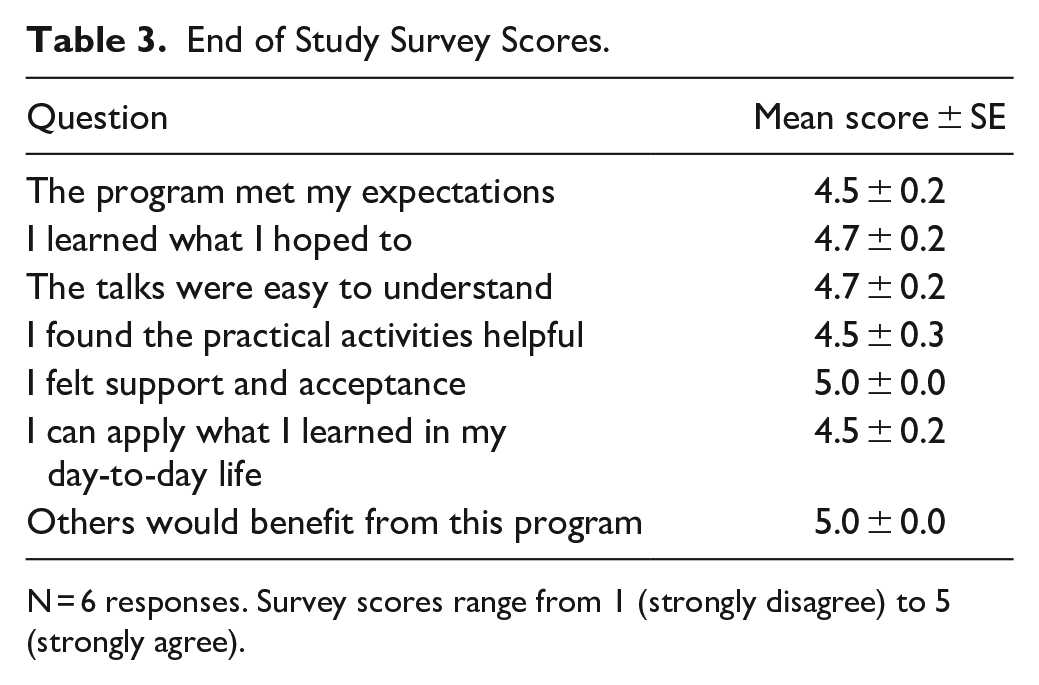
N = 6 responses. Survey scores range from 1 (strongly disagree) to 5 (strongly agree).
Additional Qualitative Findings
Semi-structured interviews with the 2 survivor advocates and course facilitator yielded supplementary information. The survivor advocates enjoyed the intimacy fostered by the small group size combined with a high meeting frequency and opportunities for facilitated individual sharing. Learning within a supportive environment about typically non-mainstream topics, such as breathing exercises to help balance the nervous system, was greatly appreciated, especially those with practical applicability. The openness of the group regarding the discussion of grief and death was specifically mentioned as a strong positive outcome. It was noted that programs and resources are scarce for patients with lung cancer, and this program addressed a significant gap in support. The length of the sessions and a need for consistent presentation structure from guest speakers were mentioned as areas of improvement.
Similar themes were noted by the facilitator, including the receptiveness toward grief and death discussions and the strong value of group support. Compared to baseline, the facilitator noted that participants had increased body awareness (especially held tension and breath), reported reduced anxiety and breathlessness, and relief in discussing grief and dying. The facilitator would alter future program sessions by ensuring that all presenters focused on activities that could be practiced at home, an aspect which participants reported greatly enjoying.
Discussion
Key Findings
The program and program evaluation were feasible. The target recruitment was 8 to 15 people based on room size and previous recruitment rates for other similar programs at our organization. Nine people registered and participated in the program, with participants attending on average 5 out of 6 scheduled sessions. The program evaluation was deemed feasible given 89% of program participants agreed to participate, and the majority filled in all three baseline and follow-up questionnaires. Two consented participants did not complete the follow-up questionnaires as they were not present for the final session.
The outcome measures were deemed feasible and informative. The collection of PROMs in a group program setting worked well based on participant feedback and questionnaire completion rate. The benefit of PROMs is well-established20-22 as they allow patients to better communicate their physical and psychosocial symptoms, and promote a shift from disease-centered care to person-centered care. 23 FACT-L is commonly used in research studies and provides a rigorous description of overall quality of life (QoL) across several domains that mirrors problems commonly experienced by people with lung cancer. 24 The MYCaW was developed for use in people with cancer and is most often used in integrative care centres. 17 MYCaW has been demonstrated to elicit a wider range of patient concerns compared to other PROMs as it allows patients to self-identify their concerns. 17 Additionally, MYCaW provides qualitative data to enrich other findings, and pairs well with validated QoL tools such as the FACT-L. 17 Semi-structured interviews provided an opportunity to capture other feedback that may not lend itself to questionnaire-based tools.
Participants showed an overwhelmingly positive reaction to taking part in the program. The most anticipated aspect of the program was information – participants were eager to learn as much as they could about managing and coping with their disease. Participants most valued the social support aspects of the program and the knowledge they received. These points were indicated in both the MYCaW follow-up questionnaire responses and the internally developed program evaluation. Survivor advocates involved in the program development spoke in detail about how the small group size and high frequency of meetings fostered a strong feeling of closeness and intimacy between attendees, which is not often present in other larger support group settings. Interest in keeping in touch with participants was expressed. This is encouraging as strong bonds were formed between people in a relatively short period of time. It is also encouraging that the program structure allowed for difficult topics to be openly discussed, such as grieving and death. Participants, advocates and the program facilitator mentioned the willingness to be open about these topics is distinct from other cancer support groups.
Concerns identified on the MYCaW questionnaires were predominantly related to psychological and emotional concerns, as well as concerns about general wellbeing. This supports the focus of the program being peer support with facilitator-led discussions, and general practical information about health and wellness. A clinically meaningful change (considered to be 0.7-1.0 by related literature19,25) was seen in the first concern noted by participants and in overall wellbeing score. Although there was a slight decline in mean scores for the second concern, the results from the MYCaW indicate encouraging trends toward an improvement in participants’ self-identified concerns and overall wellbeing.
Almost all within-person changes of the FACT-L sub-sections were improvements from baseline, indicating that the program may have conferred some benefit to QoL. Clinically meaningful changes (defined as an increase of 5-6 points in major sections and 2 points in minor subsections26,27) were seen in total FACT score (+6.3), lung cancer symptoms (+2.3), and the social domain (+2.6). These results correspond to the structure of the program, which is primarily support-group focused with the addition of breathing and other physical exercises intended for people with lung cancer.
Limitations
As this is a small, uncontrolled pilot study, a rigorous analysis of within-person or comparative changes in QoL is not appropriate. As such, our data cannot provide definitive evidence for the success of the program in improving QoL. Because of this, statistical significance was not our focus. Tables do provide relevant P values for reference; however, no meaningful statements can be made regarding the statistical analysis applied. Another area of caution regarding the overwhelming positive reaction to the program is that most participants were already engaged in another support group for people with lung cancer. This means participants may have been biased in their opinion regarding supportive programs. Alternatively, it could make quantitative changes in QoL less likely if people already had the benefit from another support group at baseline. Although it is not known if participants were diagnosed de novo with late stage disease, the long length of time from diagnosis to enrolment (median 35.6 months) may signal that our sample is not representative of most people with advanced lung cancer.
Generalizability
This evaluation plan can be used to help evaluate and modify other programs for people with cancer, especially new programs. Despite a sound evaluation plan, our data cannot provide certainty regarding the impact of the program on the participants or generalizability of findings due to our small and potentially biased sample as discussed above.
Future Directions
Findings from this pilot study will inform changes to future Inspire Now sessions. Feedback suggests shorter sessions and changes to the content of some of the presentations to better address participant needs are warranted. The most prominent outcomes seem to be social support and general wellbeing. In the future, we plan to evaluate multiple sessions of the Inspire Now program together in a single analysis. We aim to describe the population of participants who take part in the program with more confidence and provide more robust data on the feasibility and success of the program. A larger population will allow for a more rigorous analysis of within-person changes in QoL from FACT-L and MYCaW. Given that program participants tended to show improvements in many aspects of each questionnaire, a larger sample size may yield the same clinically meaningful changes alongside statistical significance. Since we will be evaluating multiple sessions, intervention fidelity will be an important consideration for future discussions around the program’s generalizability.
Conclusions
The six-week group program for people with lung cancer was feasible to run and evaluate. Qualitative feedback was overwhelmingly positive, and in particular participants valued the group support. Preliminary data indicates that clinically relevant changes in QoL and patient-specific concerns are possible; a larger study is needed to evaluate and confirm the efficacy of the program. Findings from this pilot study will inform changes to future sessions of Inspire Now, and analysis of multiple sessions powered to determine efficacy is planned. If successful, this model of care can be replicated to meet unmet psychosocial needs of people with lung cancer, for which there is currently inadequate support.
Supplemental Material
sj-docx-1-ict-10.1177_1534735420983472 – Supplemental material for A Prospective Outcomes Pilot Evaluation of Inspire Now: A Program for People with Lung Cancer
Supplemental material, sj-docx-1-ict-10.1177_1534735420983472 for A Prospective Outcomes Pilot Evaluation of Inspire Now: A Program for People with Lung Cancer by Ellen Conte, Mark Legacy, Athanasios Psihogios, Anne Pitman, Andrea Redway, Jill Hamer-Wilson and Dugald Seely in Integrative Cancer Therapies
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ottawa Integrative Cancer Centre Foundation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.