
Abstract
Introduction:
Almost half of all patients with cancer use complementary medicine (CM) alongside conventional cancer treatment. Further integration of CM into clinical practice could enhance communication and ensure improved coordination between complementary medicine and conventional care. This study assessed the perspectives of healthcare professionals on the current status of integration of CM in oncology, as well as their attitudes and beliefs toward CM.
Methods:
A convenience, volunteer sample of healthcare providers and healthcare managers working in oncology in the Netherlands were surveyed, using a self-reporting, anonymous, online questionnaire. The perspectives on the current status of integration and barriers to implementing complementary medicine were characterized in part 1, while part 2 assessed respondents’ attitudes and beliefs regarding CM.
Results:
A total of 209 people completed part 1 of the survey and 159 people completed the entire questionnaire. Two-thirds (68.4%) of the respondents indicated that their organization has implemented complementary medicine in oncology, or envisions implementation, while 49.3% stated they were missing something to implement CM in oncology. About 86.8% of the respondents (completely) agreed that complementary medicine is an important supplement to oncological treatment. Female respondents were more likely to express positive attitudes, as well as respondents whose institutions have implemented CM.
Conclusion:
The findings of this study indicate that attention is being paid to the integration of CM into oncology. Overall, the attitudes of respondents toward CM were positive. The main barriers for implementing CM activities were missing knowledge, experience, financial support, and support from management. To improve the ability of healthcare providers to guide patients in their use of complementary medicine, these issues should be delved into in future research.
Introduction
In 2020, the estimated number of new cancer cases was around 19.3 million worldwide. 1 To improve their quality of life and to cope with treatment toxicities,2-4 almost half of all patients with cancer worldwide use complementary medicine (CM) alongside conventional cancer treatment.2-4 Corresponding with these global findings, around 65% of Dutch cancer patients with breast cancer 5 and 42% with hematological cancer indicated use of complementary medicine. 6 A questionnaire focusing on the use of both complementary and alternative medicine in pediatric oncology in the Netherlands showed that 42.4% of the children with cancer made use of such therapies. 7 Cancer patients are more likely to use CM during an advanced state of illness 8 and overall, the prevalence of use has been increasing over the years. 2 Complementary medicine consists of “supportive measures that help control symptoms, enhance well-being, and contribute to overall patient care,” 9 such as acupuncture, physiotherapy, mindfulness, nutritional supplements, and yoga.9,10 Although evidence exists that CM can be beneficial for patients with cancer,11-13 there is also a risk of harm when used in combination with conventional cancer treatment, in particular for supplements14-16 Therefore, effective communication between patients and their healthcare providers on the use of complementary medicine is pertinent. 17
However, a systematic review indicated that around 40% to 50% of cancer patients (range 20%-77%) do not discuss their use of CM with their healthcare provider. 18 In the Netherlands, patients with breast cancer, hematological cancer, and pediatric cancer indicated that 29%, 38%, and 66% respectively did not discuss their use of complementary medicine with their healthcare provider.5-7 Patients explained this lack of communication by stating that they either experienced barriers for discussing these options with their provider or that they did not consider it necessary.5-7,18 To gain a better understanding of how improvement in communication about CM can be facilitated, it is important to be aware of the attitudes and beliefs of healthcare providers on this topic and what underlying factors influence these. Previous self-report studies show that one of the biggest hurdles that oncologists experience is not having enough knowledge on the topic.4,19-22
Further integration of CM into clinical practice could enhance the communication between healthcare providers and patients on the topic of CM, as well as reduce the risk of harm by improving the coordination between complementary medicine and conventional care. 23 Within this paper, integration is broadly defined, from research and education on the topic of CM, to internally offering evidence-based CM services or having a referral network with qualified external CM providers. There is a growing interest in CM integration, due to greater awareness of the potential benefits, and an increase in demand for CM by patients with cancer.24-30 Key stakeholders of the integration of complementary medicine in conventional cancer care include healthcare providers and healthcare managers. 31 Research indicates that healthcare managers are less familiar with CM compared to other healthcare professionals and that familiarity is a large factor for positive attitudes. 32 From the healthcare providers’ side, the main reasons mentioned to explain why CM is not further integrated into oncological care were missing evidence, financial resources and qualifications.21,33,34
In the Netherlands, mostly positive attitudes toward complementary medicine were found for diverse healthcare providers, although the majority of respondents considered their knowledge on CM to be lacking.35-37 In a study surveying the opinions of (non)-clinical Dutch healthcare professionals active in various fields, 64% of the respondents believed that the use of complementary medicine is of importance for optimal healthcare and would consider integration in their institution. 32 To the best of our knowledge, no study has focused on the attitudes of Dutch healthcare providers and managers in oncology specifically. The purpose of this study is to assess the attitudes and beliefs of Dutch healthcare providers and managers on complementary medicine, as well as to gain a better understanding of the current status of integration of and communication about CM in oncology.
Methods
In this study, a self-reporting, anonymous, online questionnaire was administered among healthcare providers and healthcare managers working in an oncological setting in the Netherlands.
Respondents
A convenience, volunteer sample of healthcare providers and healthcare managers working in oncology was recruited. When opening the link to the questionnaire, respondents gave explicit consent for the use of their data.
Procedure
A comprehensive overview of general oncology centers and all oncology outpatient clinics of hospitals in the Netherlands was created, resulting in a list of 74 oncology departments. The secretaries of these departments were approached by phone or by e-mail with the request to distribute the link to the online questionnaire among healthcare providers and healthcare managers working at their department. Secretary contact details were derived from the websites of the hospitals. After a month, a reminder was sent to all departments. In order to reach more participants, the link to the online questionnaire was also placed on the websites of the Netherlands Comprehensive Cancer Organization (IKNL), the Oncological Collaboration Foundation (SONCOS) and the Professional Association of Nurses and Caretakers in Oncology (V&VN). Furthermore, an announcement was made in the online IKNL newsletter. The link to the online questionnaire remained open for 2 months (4 May-1 July 2021). Of the 74 oncology departments that were directly approached, we received (partly) completed questionnaires from 54 departments (73%). Besides, healthcare providers or managers from 20 additional institutes responded, such as radiotherapy clinics and specialized oncology centers (eg, breast cancer). The mean number of respondents per institute was 3.3 (SD = 4.6). Only respondents who completed at least the first part of the questionnaire were included in the analyses.
Questionnaire
The questionnaire was adapted from previous publications32,35,38 and piloted among 2 healthcare providers (1 oncologist, 1 oncology nurse) and 1 healthcare manager working in an oncology department at an academic hospital in the Netherlands. Completion time during the pilot appeared to be approximately 5 minutes. The pilot resulted in minor modifications to the formulation of the questions before the final version was disseminated.
The final questionnaire starts with an assessment of the demographic characteristics of respondents (sex, age category, organization, department, specialization). This was followed by a clear description of what complementary medicine entails, with examples provided, to ensure that the respondents had similar definitions of CM in mind. The survey that followed consisted of 2 parts, with 14 questions in total. The first part relates to the status of integration. First, a general assessment was made of the degree and area of implementation of complementary medicine in the respondent’s oncology department (areas: healthcare program, research, education, organization policy, department policy, personal policy, or other). Then, respondents were queried about barriers to implementation (knowledge, experience, scientific evidence, financial sources, support of management or colleagues, or other). The subsequent four questions were focused on specific details of the integration of complementary medicine in their institution related to communication: discussing, advising, referring or offering complementary medicine. The second part aims to gain more insight into the attitudes of healthcare professionals toward this integration. With this intent, 7 statements about the integration of complementary medicine in oncology care were presented to the respondents.
Data Analysis
Descriptive statistics were used to summarize the demographic characteristics of respondents, the perspectives of healthcare providers on the integration of CM, and the respondents’ general attitudes and beliefs toward CM. A multivariable analysis was performed to gain a better understanding of the underlying influences for the attitudes and beliefs toward CM. Adopting the stepwise method conducted by Lee et al, 19 chi-squared tests were performed to explore the variables relating to the attitudes and beliefs of respondents toward CM. The variables that had a P-value ≤.20 in the chi-squared tests were included in the binomial logistic regression models. An exception was made for the variables “type of healthcare providers” and their sex, due to the high level of multicollinearity (chi-squared P-value <.000). Therefore, when both variables were significant in the univariable analyses, the variable with the lowest P-value was chosen to include in the multivariable analysis. The independent variables included in the analyses were “type of healthcare provider,” “age” and “sex of respondents,” as well as whether or not CM activities have been implemented in the institution. Due to the low response rate of managers, only healthcare providers (medical specialists and nurses) were included in the model. The univariable analyses can be found in the Appendix (Table A1). The nominal outcome variables included in the univariable analyses had to be transformed into dichotomous outcome variables for the multivariable logistic regression model. In line with for example, van Vliet et al., 35 positive attitudes and beliefs were captured by (completely) disagreeing with “healthcare providers should not engage in CM” and “my institution should not offer CM internally,” or (completely) agreeing with “CM is important as supplement to oncological treatment,” “healthcare providers should routinely inquire about patients CM use,” “healthcare providers should be able to advise on the effectiveness and safety of CM,” and “my institution should have a referral network of external CM providers.” All statistical analyses were performed using Stata/SE software (version 16.1).
Ethical Considerations
The research project “COMMON” was exempted from formal approval under the Dutch Medical Research Involving Human Subjects Act by the Arnhem-Nijmegen Medical Ethics Committee (case number 2020-6917).
Results
Characteristics of Respondents
Of the 260 people who started the survey, a total of 209 respondents (80.4%) provided complete information up to and including part 1; perspectives on the integration of CM (Figure 1). Of these, 159 healthcare professionals completed the entire survey, including the questions on attitudes and beliefs toward CM (61.2%). The majority of 209 respondents were women (85.9%) and 60.5% of the respondents were 50 years or younger (Table 1). Mostly nurses (76.1%) and medical specialists (20.1%) completed the survey. The 159 respondents that finished the entire survey are generally very similar in terms of demographic distribution to the 209 respondents that just filled in part 1.

Flowchart exclusion criteria survey responses.
Characteristics of Respondents.

Percentages may add to less than 100% due to rounding.
Of which 5 in (fellowship) training.
Perspectives on the Integration of Complementary Medicine
In Table 2, an overall impression of the perspectives on the integration of complementary medicine in oncology is depicted (n = 209). Two-thirds (68.4%) of the respondents indicated that their organization has implemented complementary medicine in oncology, or envisions implementation. Most of the implemented activities were implemented at department level. In the open question, activities mentioned were massages, tools for acupressure or colleagues specializing in counseling about complementary medicine.
Integration of Complementary Medicine.

Percentages may add to less or more than 100% due to rounding.
Of all 209 respondents, 49.3% stated they experienced 1 or more barriers to implement activities related to complementary medicine in oncology, of which knowledge was most commonly indicated to be lacking. This was followed by lack of experience, financial support and management support. Scientific evidence for the effectiveness of complementary medicine was least indicated, although it was still selected by 43.7% of respondents. In the category “other,” respondents added other lacking sources, such as time for implementation and execution, opportunities to learn from experienced colleagues, coordination with involved parties, and acceptance and commitment from colleagues.
A notable 71.1% of respondents said that in their institution, patients can discuss complementary medicine with their healthcare provider. However, less than half of respondents believed that healthcare providers in their institution are able to advise patients about complementary medicine (45.3%), although 18.1% indicated this is in preparation. Moreover, only 43.3% reported the ability to refer to external complementary medicine providers or to offer CM internally (42.1%). Many did not expect a change in referral to and internal offering of complementary medicine (47.8% and 43.3%, respectively).
General Attitudes and Beliefs Towards Complementary Medicine
In Table 3, the general attitudes and beliefs of respondents toward complementary medicine are summarized (n = 159). In total, 86.8% (completely) agreed that complementary medicine is an important supplement to oncological treatment. Over three-quarters (76.7%) felt that healthcare providers should engage in complementary medicine for patients, but fewer people (69.1%) believed that healthcare providers should routinely inquire about the use of complementary medicine by patients. The majority (82.3%) of respondents believed that healthcare providers must be able to advise patients on the effectiveness and safety of complementary medicine, although 72.3% indicated that they would need support to discuss this topic with patients. Moreover, 19.5% thought that their institution should not offer CM internally, while 62.3% believed that their organization should have a referral network of external complementary healthcare providers.
Attitudes and Beliefs toward Complementary Medicine.
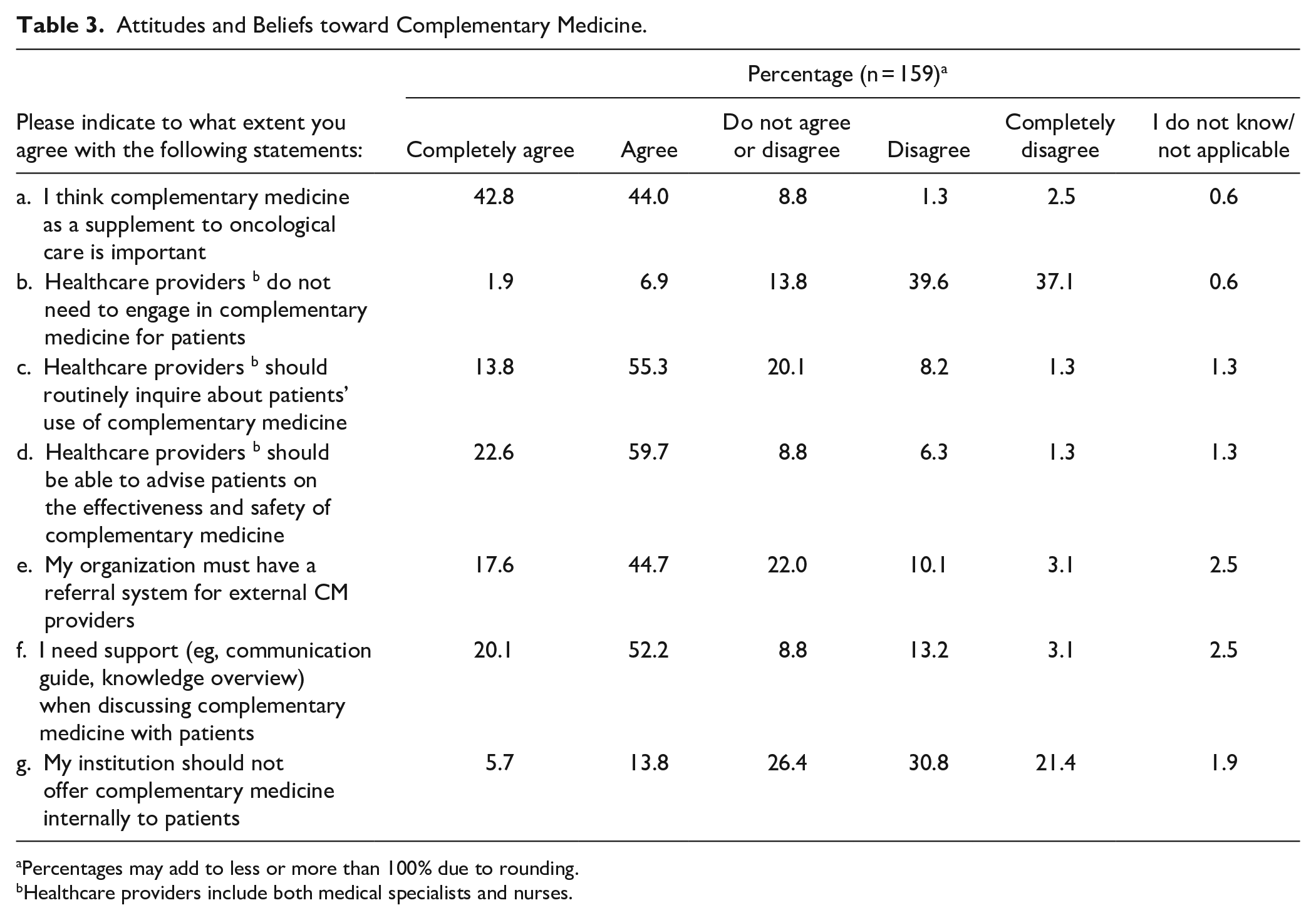
Percentages may add to less or more than 100% due to rounding.
Healthcare providers include both medical specialists and nurses.
Multivariable Analysis of Attitudes and Beliefs Towards Complementary Medicine
As can be seen in Table 4, being female makes it significantly more likely to (completely) agree with the belief that CM is an important supplement (OR, 5.10; 95% CI, 1.58-16.41) and to (completely) disagree with the statement that healthcare providers should not engage in CM (OR, 3.31; 95% CI, 1.17-9.37). Institutional implementation of CM also made it more likely for respondents to (completely) agree with the statement that healthcare providers should routinely inquire about patients’ CM use (OR, 2.25; 95% CI, 1.07-4.74) and to (completely) disagree with the statement that their organization should not offer CM internally (OR, 2.26; 95% CI, 1.09-4.69). Lastly, nurses were more likely than medical specialists to agree that there should be an external referral system (OR, 2.17; 95% CI, 1.02-4.60) and that CM should be offered internally (OR, 2.28; 95% CI, 1.01-5.13). The age of respondents was never significantly associated with the attitudes and beliefs of respondents.
Multivariable Analysis of Attitudes and Beliefs Toward Complementary Medicine (CM).

Odds Ratio.
Confidence interval.
P < .10; **P < .05; ***P < .01 by multivariable logistic regression.
Discussion
This survey examined the attitudes and beliefs toward CM among a sample of Dutch healthcare professionals in oncology, as well as their perspectives on the current status of integration of CM in oncology. Over half of the respondents indicated that their institution has implemented CM in their oncology department, while 10% stated that implementation is envisioned. A direct comparison of the extent of integration to that of other countries is not possible, as such studies used different conceptualizations, methods and definitions. However, some findings are highlighted for the purpose of context. A European study stated that 47.5% of European oncology centers provided integrative oncological treatments,4,39 while an Australian study found that 25.8% of their organizations offered integrative oncology. In the United States, 60% of National Cancer Institutes listed information on integrative therapies on their websites. 28
Around half of the respondents reported they lack something for CM implementation in oncology. Congruent with previous findings, barriers to implementing CM activities indicated by the study sample were mainly a lack of knowledge4,19-22 and experience,32,35 but also lacking financial support,28,40,41 support from management,25,34,40 and scientific evidence.4,40,42 The majority of respondents indicated a need for support in discussing CM use, despite the results showing that in most hospitals, patients are provided with the opportunity to discuss CM use with their healthcare providers. A survey conducted in Germany also indicated low confidence among healthcare providers in discussing CM. 43 These limitations can hinder a healthcare providers’ ability to adequately advise their patients and to provide support, which may lead to patients making decisions on CM use that could potentially be harmful.14-16 Providing education and training on CM for healthcare professionals could be part of the answer.44,45 Moreover, the responses show that less than half of the institutions in this sample refer to external CM providers or offer CM internally to patients, which also seem to be less envisioned compared to discussing and advising patients on CM use. Lack of financial support and support from management and colleagues can potentially explain this finding. Change can be driven by professionals working in the field; however, healthcare managers are key stakeholders needed to facilitate the integration of complementary medicine in conventional care. Therefore, their attitudes, beliefs and perspectives on this topic are relevant, 31 particularly since some of the crucial key points mentioned for effective integration are having a strong strategic plan, supportive leadership and a viable operating budget.25,41 Little research has been done on investigating the managers’ perspectives on CM31,46 and thus, further research into this topic is warranted. As this group of interest is relatively small, a more direct approach might be more suitable than convenience sampling. Given the limited number of responses, unfortunately, no conclusions can be drawn on the opinions of managers included in this survey.
Overall, the attitudes of the respondents toward CM were positive. Most respondents agreed that CM is an important supplement to conventional cancer treatment and that healthcare providers need to engage and should have knowledge on the topic. Previous surveys in European countries also report a predominantly positive attitude among oncology professionals toward CM,20,43,47 although healthcare provider’ attitude is not measured in a consistent manner across studies. Respondents seemed more neutral when it comes to the routine inquiry of CM use, external referral systems or internally offering CM. Already having implemented CM in the institution meant that respondents were significantly more likely to believe that healthcare providers should routinely inquire about CM use and that their institution should offer CM internally. This suggests that healthcare providers are more uncertain how CM should be integrated into standard care when it has not been implemented yet. Examinations of different types of implementation show a preference for a more integrative form of oncology care, where patients receive guidance and have access to all information and care at a single location.4,48 Compared to medical specialists, nurses were more likely to show a positive attitude toward referral to external CM providers and offering CM internally. This could be due to nursing being generally a more holistic and supportive role toward the patient than the more technical role of a medical specialist. 35 Lastly, in line with previous research,19,42,47,49 the results show that female healthcare providers are significantly more positive toward complementary medicine as part of cancer treatment compared to male healthcare providers. This could reflect a greater open-mindedness of females toward CM in general as some suggest,42,47 backed up by studies showing that female patients are also more interested in CM than men.50-52 However, the high response rate of nurses (who are mainly female, see Table 1) might have influenced these results as well, given the high multicollinearity between the type of healthcare professionals and their sex.
Some other limitations of this study are important to note when interpreting the findings. The method chosen is a convenience, volunteer sample, which is a poorer reflection of the population compared to random sampling. 53 Due to this chosen method, the sample size is relatively low with limited statistical power to detect small differences. 54 The survey was split into 2 parts and designed to be simple to encourage response. About 80.4% of the respondents completed only the first half of the survey and 61.2% filled it in completely, limiting the generalizability of the findings. This might reflect self-selection bias, as it can be assumed that respondents who fully completed the survey were generally more interested in and/or positive toward the topic of CM, thus influencing the results of attitudes and beliefs. Moreover, all data were self-reported, which can thus be subject to recall bias for the questions about integration, in addition to the possibility that the respondents may not be fully aware of what their institution provides. Lastly, the concept of implementation is open to many interpretations, and it is therefore not entirely certain how the respondents perceived the questions on the integration of CM. The answers should thus merely be interpreted as a signal that complementary medicine has been receiving more consideration.
Conclusion
The findings of this study indicate that in a sample of Dutch healthcare providers, consisting mainly of nurses, attention is being paid to the integration of CM into oncology. Overall, the attitudes of respondents toward CM were positive. The main barriers for implementing CM activities were missing knowledge, experience, financial support, and support from management. To improve the ability of healthcare providers to guide patients in their use of complementary medicine, these issues should be delved into in future research.
Footnotes
Appendix
Univariable Analysis of Attitudes and Beliefs.

| Predictor | Complementary medicine is an important supplement to oncological treatment |
Healthcare providers should not engage in complementary medicine |
||||||
|---|---|---|---|---|---|---|---|---|
| Total a (n = 159) | (Completely) agree | Do not (completely) agree | P (χ2-test) | Total a (n = 159) | (Completely) disagree | Do not (completely) disagree | P (χ2-test) | |
| Type of healthcare provider | 0.017 | 0.986 | ||||||
| Medical specialist | 40 | 30 | 10 | 39 | 30 | 9 | ||
| Nurse | 112 | 101 | 11 | 112 | 86 | 26 | ||
| Age | 0.932 | 0.799 | ||||||
| <20 | 1 | 1 | 0 | 1 | 1 | 0 | ||
| 20-30 | 15 | 12 | 3 | 15 | 11 | 4 | ||
| 31-40 | 37 | 33 | 4 | 37 | 29 | 8 | ||
| 41-50 | 39 | 33 | 6 | 38 | 29 | 9 | ||
| 51-60 | 52 | 45 | 7 | 52 | 38 | 14 | ||
| >60 | 12 | 11 | 1 | 12 | 11 | 1 | ||
| Sex | 0.010 | 0.034 | ||||||
| Male | 23 | 16 | 7 | 22 | 13 | 9 | ||
| Female | 133 | 119 | 14 | 133 | 106 | 27 | ||
| CM implementation | 0.185 | 0.138 | ||||||
| Yes | 98 | 89 | 9 | 98 | 80 | 18 | ||
| No | 48 | 40 | 8 | 48 | 34 | 14 | ||
| Predictor | Healthcare providers should routinely inquire about patients’ use of complementary medicine | Healthcare providers should be able to advise patients on the effectiveness and safety of complementary medicine | ||||||
| Total a (n = 159) | (Completely) agree | Do not (completely) agree | P (χ2-test) | Total a (n = 159) | (Completely) agree | Do not (completely) agree | P (χ2-test) | |
| Type of healthcare provider | 0.711 | 0.542 | ||||||
| Medical specialist | 38 | 28 | 10 | 39 | 31 | 8 | ||
| Nurse | 112 | 79 | 33 | 111 | 93 | 18 | ||
| Age | 0.714 | 0.093 | ||||||
| <20 | 1 | 1 | 0 | 1 | 1 | 0 | ||
| 20-30 | 15 | 9 | 6 | 15 | 13 | 2 | ||
| 31-40 | 37 | 26 | 11 | 36 | 25 | 11 | ||
| 41-50 | 38 | 24 | 14 | 38 | 36 | 2 | ||
| 51-60 | 52 | 38 | 14 | 52 | 44 | 8 | ||
| >60 | 11 | 9 | 2 | 12 | 9 | 3 | ||
| Sex | 0.175 | 0.661 | ||||||
| Male | 22 | 18 | 4 | 22 | 19 | 3 | ||
| Female | 132 | 89 | 43 | 132 | 109 | 23 | ||
| CM implementation | 0.026 | 0.174 | ||||||
| Yes | 97 | 74 | 23 | 98 | 84 | 14 | ||
| No | 48 | 28 | 20 | 47 | 36 | 11 | ||
| Predictor | My institution should have a referral network of external complementary medicine providers | My organization should not offer complementary medicine to patients | ||||||
| Total a (n = 159) | (Completely) agree | Do not (completely) agree | P (χ2-test) | Total a (n = 159) | (Completely) disagree | Do not (completely) disagree | P (χ2-test) | |
| Type of healthcare provider | 0.041 | 0.015 | ||||||
| Medical specialist | 38 | 19 | 19 | 39 | 15 | 24 | ||
| Nurse | 111 | 76 | 35 | 110 | 67 | 43 | ||
| Age | 0.839 | 0.809 | ||||||
| <20 | 1 | 1 | 0 | 1 | 1 | 0 | ||
| 20-30 | 15 | 10 | 5 | 15 | 9 | 6 | ||
| 31-40 | 36 | 22 | 14 | 37 | 20 | 17 | ||
| 41-50 | 36 | 22 | 14 | 38 | 22 | 16 | ||
| 51-60 | 52 | 35 | 17 | 51 | 24 | 27 | ||
| >60 | 12 | 6 | 6 | 11 | 6 | 5 | ||
| Sex | 0.960 | 0.197 | ||||||
| Male | 22 | 14 | 8 | 22 | 9 | 13 | ||
| Female | 130 | 82 | 48 | 131 | 73 | 58 | ||
| CM implementation | 0.274 | 0.044 | ||||||
| Yes | 97 | 66 | 31 | 96 | 59 | 37 | ||
| No | 46 | 27 | 19 | 48 | 21 | 27 | ||
Numbers may not add up to the total because of missing values.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Dutch Cancer Society [grant number 12566].