
Abstract
Background:
Chemotherapy is associated with decreased quality of life (QOL), fatigue, depression, and weight gain in patients with breast cancer. Weight gain is associated with poorer prognosis. Yoga improves QOL, fatigue, and mood in women with breast cancer but its effect on treatment-related weight gain has not been studied. The aim of this trial was to determine the feasibility of personalized yoga therapy in women receiving treatment for early-stage or locally advanced breast cancer and assess its impact on weight gain.
Methods:
Thirty women were randomized 1:1 to receive yoga therapy by a certified yoga therapist during treatment or a control group. Participants in the yoga arm were asked to complete three 30 minute yoga sessions weekly (which included movement, breath work, mindfulness, and relaxation) throughout adjuvant or neoadjuvant chemotherapy (N = 29) or endocrine (N = 1); the control arm received breast cancer treatment without yoga. For comparability between participants randomized to yoga therapy, the single patient treated with endocrine therapy was excluded from the analysis. Primary outcomes were feasibility and weight change. Additional outcomes were mood, fatigue, QOL, serum tumor necrosis factor-alpha (TNF-alpha), and C-reactive protein (CRP) as immune mediator biomarkers.
Results:
Mean age was 51.6 years, 75.9% were white and 24.1% were people of color, reflecting the cancer center population. 80% had stage II-III disease. Enrollment was completed in 9 months. Compliance was lower than predicted; however, participants participated in on average 1.7 yoga sessions/week for a mean 15.6 weeks duration. There were no adverse events. Control arm participants gained on average 2.63% body weight during treatment while yoga participants lost 0.14% body weight (weight change = −0.36 in yoga arm vs. 2.89 in standard of care arm, Wilcoxon rank sum test P = .024). Control participants reported increased fatigue and decreased QOL, while yoga participants reported no change in QOL. No significant change in TNF-alpha or CRP was noted in either arm.
Conclusion:
This feasibility study suggests that personalized yoga therapy is beneficial for QOL and weight maintenance among women undergoing chemotherapy for early-stage or locally advanced breast cancer. Weight maintenance associated with yoga therapy may be of clinical significance in this population given the poorer prognosis associated with weight gain in breast cancer survivors.
Trial Registration:
NIH Clinicaltrials.gov #NCT03262831; August 25, 2017. https://clinicaltrials.gov/ct2/show/NCT03262831
Background
Breast cancer (BC) is the most common malignancy in women worldwide. It is the second leading cause of death in women in the United States (US) and leads to $26 billion in medical costs in the US each year. 1 Although there has been a significant reduction in BC mortality due to improved screening practices and more effective treatments, there is still a remarkable amount of morbidity associated with BC and its treatment. Survivors can experience short- and long-term weight gain, fatigue, anxiety, depression, and reduced quality of life (QOL).2-4 Weight gain is extremely common during and after BC treatment with nearly two-thirds of women who receive chemotherapy experiencing weight gain.5-7 Weight gain, likely mediated in part through decreased physical activity during and after BC treatment,8,9 has been associated with increased rates of recurrence and mortality, especially when weight gain occurs in the early years following diagnosis and treatment.10-12 The association between weight gain and BC prognosis is complex and may be in part mediated through alterations in immune mediators and inflammatory cytokines. C-reactive protein (CRP), tumor necrosis factor alpha (TNF-alpha), and other inflammatory cytokines have been shown to correlate with body mass index (BMI) in women with BC and to increase following chemotherapy.13-17 Weight loss programs among women with BC have been associated with decreases in CRP and may contribute to improved outcomes. 18 A large, international, randomized controlled trial of a weight loss intervention with the primary outcome of disease-free survival is currently being conducted and should shed light on the impact of weight loss after BC diagnosis on prognosis. 19
Physical activity, including yoga, has been shown to improve symptoms related to BC treatment and to improve QOL, including fatigue, anxiety, and depression.20-25 Unfortunately, physical activity during cancer therapy typically declines, with only about 20% of patients meeting national guidelines after BC treatment8,26 and less than 10% meeting guidelines throughout long-term follow up. 9 Yoga has been shown to be as effective as other types of physical activity, including aerobic exercise and strength training, at improving QOL among women with BC. 27 Many types of yoga programs have been studied for treating symptoms of BC, including hatha yoga, integrated yoga, iyengar yoga, yoga of awareness, and many others. 22 Hatha yoga is one of those most frequently studied, and although we are not aware of studies comparing the different yoga protocols, 28 hatha has been shown to have beneficial effects on QOL29,30 and fatigue.31,32 One study found that yoga added to standard care during chemotherapy reduced chemotherapy-related nausea and vomiting. 33 Yoga has also been shown to decrease pro-inflammatory and prognostic cytokines, including TNF-alpha, in women with BC. 34 Given the growing interest in the integrated therapies into the treatment of BC, yoga is an attractive and potentially effective intervention to reduce treatment- and fatigue- related weight gain and improve QOL. Despite yoga’s well-documented effects on QOL among women receiving BC treatment as well as BC survivors, 22 and despite a recent study demonstrating patients with BC perceive yoga and mindfulness as acceptable additions to interventions aimed at weight management, 35 few studies directly examined yoga’s effect on treatment-related weight gain. Several studies have examined yoga’s effect on weight change in BC survivors,29,31 whereas yoga’s effect on weight in women undergoing active BC treatment has not been reported.
To fill this gap, we conducted a randomized feasibility study of a personalized mindfulness-based yoga therapy compared to control in women undergoing chemotherapy or endocrine therapy for early-stage or locally advanced BC. The primary objective of the current study was to evaluate the feasibility of implementing a randomized controlled trial evaluating yoga therapy among women undergoing chemotherapy or endocrine therapy for early-stage or locally advanced BC. Secondary outcomes were to evaluate the effect of the yoga therapy on (a) weight change, (b) inflammatory markers including CRP and TNF-alpha, (c) overall QOL including cancer related symptoms and concerns, satisfaction with QOL during cancer treatment, and cancer-related fatigue,
Methods
Participants
Thirty patients with early-stage or locally advanced (stage I-III) BC were enrolled in the study. Participants were recruited prior to the start of endocrine or chemotherapy treatment, and were eligible if they were (a) scheduled to undergo neoadjuvant chemotherapy (after recruitment was started, the protocol was amended to allow adjuvant chemotherapy to improve generalizability), or endocrine therapy, (b) older than age 18, (c) female, (d) not currently practicing yoga (patients were excluded from the study if they were current practitioners of yoga, which was defined as participating in yoga at least once per month.), (e) able to read and understand English, and (f) able to understand and sign informed consent.
Procedures
Participants were randomized either to the intervention arm, which consisted of yoga therapy along with BC treatment determined by the treating physician, or to the control arm, which consisted of BC treatment alone, in a 1:1 ratio. The randomization scheme was generated using the SAS program PROC PLAN with a block size of 4 patients. After enrollment and confirmation of eligibility status, randomization occurred online through REDCap, an online software for clinical trial databases, so that the randomization scheme was concealed until assignment. Thirty patients were accrued; 15 were randomized to each arm. This study adheres to consolidated standards of reporting trials 2010 (CONSORT) guidelines. 36
Approval was obtained from the Washington University Institutional Review Board (9/19/2017 IRB ID #: 201708076). All procedures performed were in accordance with the 1964 Helsinki declaration and its later amendments. All participants signed informed consent. Participants were recruited between February 2018 and March 2019 from Washington University School of Medicine Siteman Cancer Center in Saint Louis, Missouri. Participants were identified using clinic schedules and approached for participation during routine clinic visits by a member of the study team.
Intervention
The yoga therapy was developed based on gentle hatha and restorative yoga protocols found to decrease fatigue and weight gain in people with BC.29,31,32,37,38 Yoga therapy as defined by the International Association of Yoga Therapists “Scope of Practice for Yoga Therapy” is the professional application of the principles and practices of yoga to promote health and well-being within a therapeutic relationship that includes personalized assessment, goal setting, lifestyle management, and yoga practices for individuals or small groups. The yoga therapy in this protocol included mindful breathing, mindful movement, and mindful moments. Prior to the start of their first chemotherapy or endocrine therapy session, a trained certified yoga therapist met in the clinic with each participant and developed a personalized treatment plan from the general training manual and determined how many sessions the participant would have with the therapist. Each of the yoga therapists have at least 600 hours of yoga teaching training, while 2 were certified yoga therapists (C-IAYT) with at least 1000 hours of yoga teaching and therapy training. The 3 yoga therapists all have advanced professional training in a medical field, and 1 is an oncology nurse. The yoga therapy was personalized for each participant and included options for gentle and supported poses using props that would be available to the participant at home, such as blankets, books, and pillows, to make poses more accessible to participants with limited mobility and to account for fluctuations of daily energy level and other BC treatment-related side effects. Participants in the yoga therapy arm were met in person and given a thick yoga mat, a blanket, the training manual, which included a journal for recording data on participation, mood, fatigue and QOL, and a carrying case. Meditation and breath work were included as part of the protocol. Each individualized protocol was created from the training manual and consisted of 5 to 10 minutes of centering/breathing poses, 15 to 20 minutes of seated and standing gentle poses and ended with 5 to 10 minutes of guided relaxation (see Supplemental Appendix 1). Participants were asked to practice at home 3 times per week for 30 minutes per session, even if it meant just sitting/lying and being aware of one’s breath. Participants were asked to continue this practice for the duration of their adjuvant or neoadjuvant treatment, which was 12 to 20 weeks depending on treatment regimen. Each participant was asked to record the time and duration of practice at home in patient logs. Each participant in the yoga therapy arm was contacted weekly by one of the yoga therapists by phone, email or text to provide support and/or answer any questions about their practice.
Control Arm
Participants who were randomized to the control arm received BC treatment (neoadjuvant endocrine or chemotherapy, or adjuvant chemotherapy), but without yoga therapy. Participants in both arms received verbal recommendations regarding the importance of avoiding weight gain during treatment from their treating provider, as is standard in our medical oncology practices. For both arms, BC treatment (endocrine therapy or chemotherapy) and duration was determined by the treating physician.
Primary Outcome
Feasibility
Feasibility was defined as 80% of participants completing the intervention. A completion rate of 80% was selected based on the completion rate seen in previous yoga studies.23,31,39 A participant was considered to have completed the intervention if she practiced yoga 3 or more sessions per week for 30 minutes or more per session for the duration of chemotherapy or endocrine therapy (12-20 weeks depending on treatment regimen).
Secondary Outcomes
Weight change
Weight was collected in clinic at baseline and at the end of treatment. All participants were weighed on digital scales (Doran DS5100) at the time of vital sign collection by certified medical assistants prior to seeing their oncology provider. Baseline weight was taken prior to the start of adjuvant or neoadjuvant treatment; end of treatment weight was taken within 4 weeks of the patient’s last treatment for those receiving adjuvant treatment and at the last physician visit before surgery for those receiving neoadjuvant treatment.
Quality of life measures
Quality of life was measured at baseline and at the end of treatment using the Functional Assessment of Cancer Therapy-General (FACT-G7), a validated rapid version of the FACT-G designed to assess cancer-related symptoms most important to patients. 40 Higher scores on this survey indicate greater QOL. Each item scores on a 0 to 4 Likert scale with the total score ranging possibly from 0 to 28. The total FACT-G7 score as well as sub-scores for fatigue and QOL were examined. In addition to the FACT-G7, participants in the yoga therapy arm were asked to keep a yoga journal following each yoga therapy session, in which they recorded the duration of their session and rated their fatigue and mood following that session. Fatigue was scored on a 0 to 4 Likert scale, with 0 as “not at all” fatigued, and 4 as “very much” fatigued. Mood was scored on a 0 to 4 Likert scale, with 0 as mood being “not good” and 4 as mood being “good.”
Inflammatory markers
Blood samples were collected from participants at baseline (after enrollment in the trial but before the start of adjuvant or neoadjuvant treatment) and following completion of treatment for the assessment of inflammatory markers CRP and TNF-alpha. End of treatment collection was completed within 4 weeks of the patient’s last treatment for those receiving adjuvant treatment or on the day of the patient’s last physician visit prior to surgery for those receiving neoadjuvant treatment. Participants were not instructed to give fasting samples. Whole blood samples were centrifuged following collection. Human TNF-alpha and Human C-reactive Protein Quantikine ELISA Kits (R&D, Cat# DTA00D and D6050) were used to assess serum cytokine levels according to the manufacturer’s protocol. Optical density (OD) was calculated using a Tecan Infinite 200 Pro microplate reader.
Clinical characteristics
The medical record was reviewed for age, race, smoking status, and tumor characteristics including hormone receptor status, stage, and pathologic response.
Sample size
The sample size of 15 per arm was primarily determined based on clinical feasibility and targeted to providing reasonable precision for estimating preliminary efficacy data. 41 For detecting pre-post weight change within an arm, 15 patients per arm provide 80% power to detect an effect size of 0.78 for pre-post weight difference using a 2-sided paired t-test at a 5% significance level; for comparing pre-post weight change between the 2 arms, 15 patients per arm achieve 80% power to detect a minimal effect size of 1.06 based on 2-sample t test at a 2-sided significance level of 5%.
Statistical analysis
Descriptive analyses were used to examine feasibility, patient characteristics, and tumor characteristics. Feasibility was defined as at least 80% completion of the intervention. Wilcoxon signed rank test was used for comparison of paired pre-post data within group while Wilcoxon rank sum test was used to compare between group differences. Chi-squared test was used for categorical data. R (Version 3.6.1) was used to conduct statistical analyses and to generate all figures.
Results
Participant Baseline Characteristics
Thirty women were enrolled between April 2018 and January 2019; follow up continued through June 2019 (Figure 1).

Enrollment, Randomization and Outcomes.
Fifteen were randomized to the yoga therapy arm and 15 to the standard of care arm. One participant in the standard of care arm was found to be ineligible following randomization due to metastatic disease and was excluded; 29 participants were included in the analysis of baseline characteristics. Four patients dropped out of the study, thus 25 patients had pre and post intervention data. The mean age was 51.6 years for all participants (Table 1).
Patient Characteristics.

The majority of the participants were Caucasian (75.9%) and never-smokers (69.0%). Six participants had stage I disease (20.7%), 17 had stage II disease (58.6%), and 6 had stage III disease (20.7%). Eighteen participants (62.1%) had estrogen receptor positive (ER+) tumors, 14 (48.3%) had progesterone receptor positive (PR+) tumors, 10 (34.5%) had human epidermal growth factor receptor 2 (HER2) positive tumors, and 7 (24.1%) had triple negative tumors. There was no significant difference in baseline characteristics between the yoga therapy and control arms.
Participants were treated with adjuvant or neoadjuvant endocrine therapy or chemotherapy for a duration of 12 to 20 weeks, as determined by the treating physician. Twenty-eight participants were treated with chemotherapy; 1 participant was treated with endocrine therapy (anastrozole). For comparability between participants randomized to yoga therapy, the single patient treated with endocrine therapy was excluded from the analysis given the different treatment-related toxicities. Of the 28 participants treated with chemotherapy, 6 received docetaxel, carboplatin, and trastuzumab with or without pertuzumab (TCH +/- pertuzumab), 5 received dose-dense doxorubicin plus cyclophosphamide followed by paclitaxel (ddAC + taxol), 4 received paclitaxel plus trastuzumab, 3 received docetaxel plus cyclophosphamide (TC), 3 received docetaxel plus carboplatin, 2 received paclitaxel, and 5 received other chemotherapy regimens. Sixteen participants received neoadjuvant therapy and 13 received adjuvant therapy. 6/16 participants (37.5%) receiving neoadjuvant therapy had a complete pathologic response, 8/16 participants (50%) had a partial pathologic response, and 2/16 participants (12.5%) had no pathologic response documented (Table 1). The study was not powered to detect a statistically significant difference in pathologic response between the 2 arms.
Feasibility Measures
Of the 32 participants who consented, 93.8% were successfully enrolled within a 9 months time frame. Of the 30 women enrolled in the trial, 1 participant was found to be ineligible following randomization due to metastatic disease, 3 participants withdrew from the study, 2 from the yoga therapy arm and 1 from the control arm. One participant in the yoga therapy arm cited lack of time and flexibility in her schedule as the reason for withdrawal. None of the participants randomized to the yoga therapy arm were able to complete three 30 minute yoga sessions per week, which was defined per protocol as successful completion of the yoga therapy.
Twenty-five of the 29 (86%) participants who initiated on protocol continued either their yoga therapy (N = 13) or their control arm follow up (N = 12) throughout the duration of the study. Participants received a mean of 15.6 weeks of yoga therapy, ranging from 11 to 20 weeks. Contact with the patients by the yoga therapists was by phone, text or email, with text response being the most successful communication method noted by the yoga therapists. Patients participated in an average of 1.7 (standard deviation = 1.3, interquartile range = 0.75-2), yoga therapy sessions per week with cycle-averaged weekly yoga minutes of 28.1 (inter-quartile range = 13.67-40.89) minutes among the 13 participants and averaged 17.7 minutes per session. Participants practiced on average a total of 26 yoga therapy sessions, ranging from 0 to 59 sessions, and a total of 432.2 minutes of yoga therapy practice, ranging from 0 to 1015 minutes of practice, over the course of the study (Table 2).
Yoga Practice.
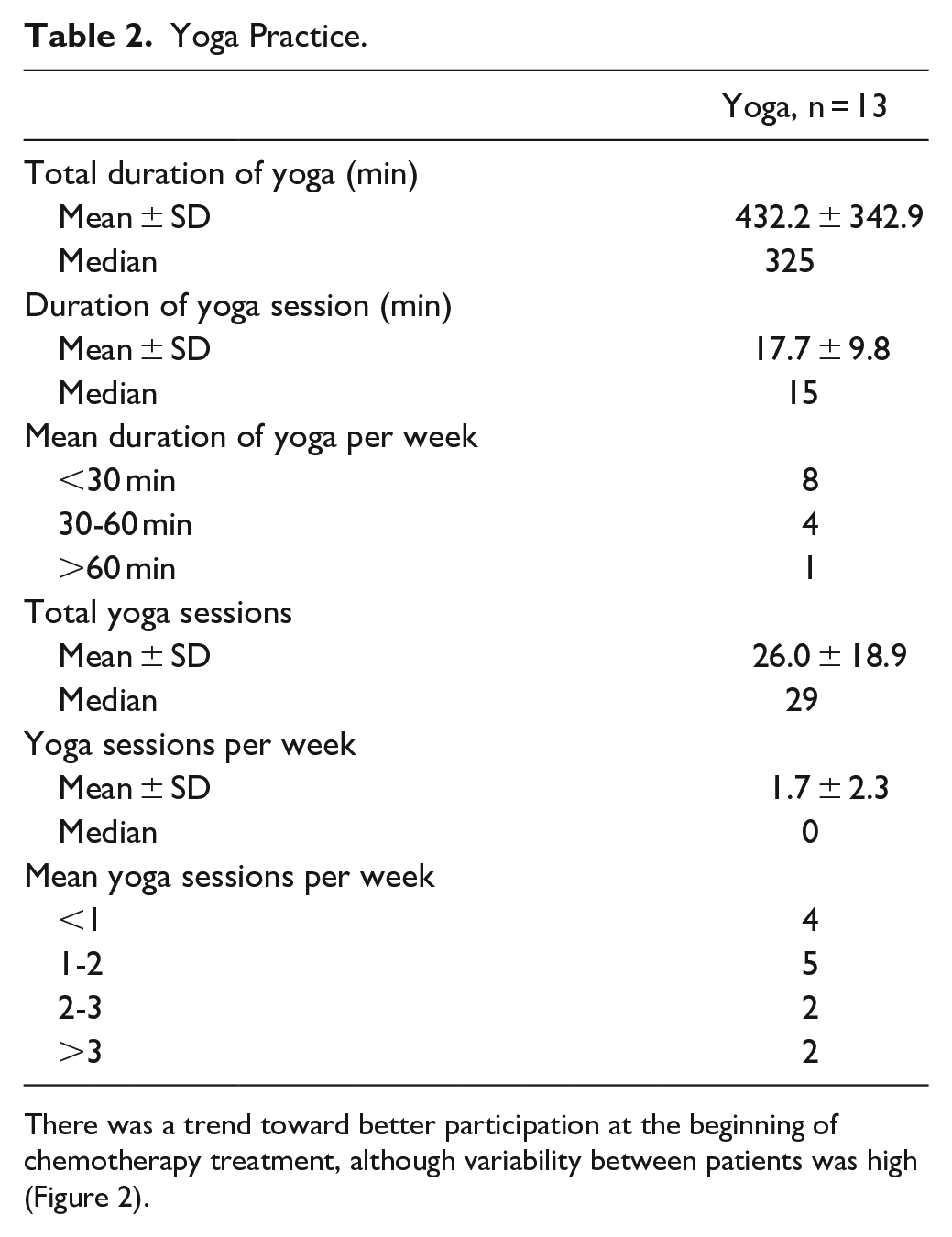
There was a trend toward better participation at the beginning of chemotherapy treatment, although variability between patients was high (Figure 2).
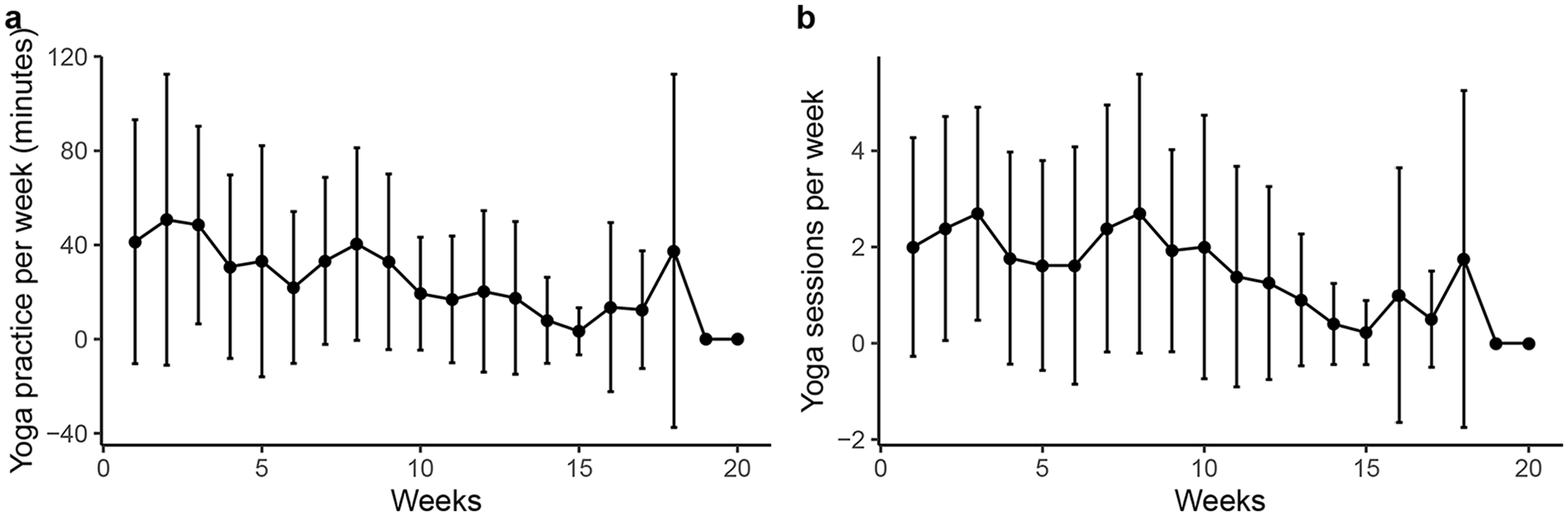
Amount of yoga (in minutes) practiced per week was variable.
Weight Change Due to Yoga Therapy
To identify if the yoga therapy could prevent weight gain during treatment, the patient’s weight was collected prior to the start of and after completion of treatment. Twenty-five patients were analyzed for weight change. Participants in the control arm gained, on average, 2.63% (SD = 4.10%, 95% CI 0.03%-5.24%) compared to their baseline weight, while participants in the yoga therapy arm, on average, lost 0.14% (SD = 5.51%, 95% CI −3.47%-3.19%) relative to their baseline weight (Figure 3A). The weight change was significantly different between the 2 arms (weight change = −0.36 in yoga therapy arm vs 2.89 in standard of care arm, Wilcoxon rank sum test P = .024). Women in the control arm gained an average of 2.17 kg over the timeframe of this study, although this within patient change was not statistically significant. Weight among women in the yoga therapy arm did not change from pre- to post-treatment (Figure 3B), indicating their ability to maintain their weight, as opposed to the weight gain seen in the control arm.

Weight of participants pre and post yoga therapy; yoga participants maintain their weight during treatment.
Differences in Inflammatory Markers Due to Yoga Therapy
To further understand if there were any biomolecular benefits of implementing yoga therapy alongside the standard of care treatment, levels of CRP and TNF-alpha were measured on 25 participants due to sample availability. Neither CRP (Figure 4A) nor TNF-alpha (Figure 4B) serum levels at completion of treatment changed significantly from baseline in either participants in the yoga therapy or the standard of care groups, although there was a nonsignificant trend toward improvement in the yoga therapy arm.

Inflammatory markers do not change following yoga therapy.
Quality of Life Measures
Patients completed the FACT-G7 at baseline and at the end of treatment (between 1 and 4 week following the last treatment cycle) to assess QOL; 28 participants completed all or part of the surveys and were included in the analysis. While patients in the control arm reported an increase in their fatigue score and a decrease in their overall QOL score, patients in the yoga therapy arm did not report any change in these parameters (Table 3).
FACT-G7.

CI, confidence interval
Fatigue
Quality of life scores are subsets of the FACT-G7.
Mean change includes data for which there are paired pre-treatment and post-treatment samples
Among participants in the yoga therapy arm, total score remained stable, with an average increase of 0.33 points (95% CI −3.1-3.8). The mean total score fell among the control arm, with an average decrease of 4.2 point (95% CI −6.8-−1.6). The sub-scores for fatigue and satisfaction with QOL showed a similar trend. Participants were asked to complete a yoga journal rating their fatigue and mood each time they practiced yoga therapy. Most participants reported low to moderate levels of fatigue and good mood (Table 4).
Yoga Journal Fatigue and Mood Score Summary.

Adverse events.
Fatigue: 0 to 4, 0 = no fatigue, 4 = very fatigued.
Mood: 0 to 4, 0 = not good mood, 4 = good mood.
There were no reported yoga therapy related adverse events or unintended effects.
Discussion
This study to determine the feasibility of administering a yoga therapy consisting of mindful breathing, gentle yoga poses, and relaxation was conducted in women with early stage and locally advanced BC. Unlike many studies of yoga therapy in BC which are conducted after active BC therapy is complete, all women in our study were receiving curative intent chemotherapy. The results suggest that this mindfulness-based yoga therapy may have a positive impact on weight management during BC treatment. Additionally, to our knowledge, no study prior to ours has evaluated the impact of yoga therapy on weight during chemotherapy. Given that the majority of women who receive these treatments gain weight,5-7 and that weight gain is associated with poorer cancer outcomes including increased risk of recurrence, BC death, and overall mortality,10-12 this study opens the door for larger trials of the impact of yoga therapy on not just QOL but also cancer outcomes, in this population. The study accrued quickly indicating strong interest in the intervention among the study population, which is consistent with recently published qualitative data showing patients with BC have significant interest in yoga as an adjunct to weight management strategies. 36 Twenty-five of 29 patients who initiated on protocol continuing follow up throughout the entire intervention period. Additionally, while compliance with the yoga therapy was less than expected, there was a significant difference in weight change between the yoga therapy arm (maintained weight) and control arm (gained weight), indicating there may be an effect of the mindful focus through the breath and meditative/relaxation practices in addition to the physical yoga poses. Given that physical activity generally declines during active BC treatment,8,9 a less physically demanding activity such as yoga therapy may fill a much-needed gap in lifestyle modifications during BC treatment to combat weight gain seen during treatment.
Feasibility
Feasibility was defined as 80% of participants completing the intervention. Completion of the intervention was defined as practicing yoga therapy at least 3 sessions per week for at least 30 minutes per session while the participant received chemotherapy or endocrine therapy. Although no participants were able to complete all planned 30 minute sessions per week, 86% percent of participants consistently practiced yoga throughout the duration study. Our attrition rate of 10% was within range of other studies, which have ranged from close to zero up to greater than 20%.29,39,42 Participants were on average able to complete 17.7 minutes (ranging from <30to >60 minutes), 1.7 times per week. Although compliance with the assigned yoga therapy was lower than expected, it is similar to the frequency of practice seen in other studies that have included home-based practice.29,39 Regarding additional feasibility aspects of the study, vital information was gained on administration of the program and barriers to compliance. First, the yoga therapists felt that in planning the individualized protocols, the influence of stress on the patient due to the initial diagnosis and planning for chemotherapy was underestimated. Second, difficulties arose in setting up the initial in-person session due to the variability of patients’ schedules for clinic visits, procedures, imaging tests, and treatment. Third, settings for in-person teaching of the individualized yoga therapy varied due to space availability in clinics. Fourth, multiple methods for contacting the patient for follow-up were allowed. Methods included phone calls, emails, and texting which led at times to inconsistent communication. This variability was due to patients’ internet access, convenience, preference, general well-being, etc. Fifth, originally the yoga therapy was designed for patients receiving neoadjuvant chemotherapy, however, the protocol was amended to include patients receiving adjuvant chemotherapy, and thus the protocol was altered to accommodate patients who were status post BC surgery. Finally, the wide range of treatment-related side effects made yoga therapy more difficult for some patients.
Weight Change, Inflammatory Markers, Fatigue, and Quality of Life
As mentioned, participants in the control arm gained weight, while participants in the yoga therapy arm, on average, lost weight, although this did not meet statistical significance (Figure 3A). The weight change was however significantly different between the 2 arms. Weight stability during the first several years following diagnosis has also been associated with improved mortality rates. 11 Weight loss may lead to improved prognosis, but this has yet to be demonstrated. A randomized controlled trial to evaluate this is being conducted, however. 19 At a minimum, avoiding weight gain should be a primary goal of BC survivors, and yoga therapy may be one method to do so. The clinical significance of the weight change observed in our study (−0.14%, 95% CI −3.47%-3.19% in the yoga therapy arm; 2.63%, 95% CI 0.03%-5.24% in the control group) is unclear, but may be of clinical significance, as weight maintenance has been associated with improved survival. 10 Two randomized controlled trials in post-treatment BC patients found no difference in weight change between yoga therapy and control groups.29,31 Of note, these trials only included patients who had finished treatment for BC. Studies of yoga among patients undergoing active medical treatment for BC, have been limited to assessing fatigue and other QOL measures.22,43 Further studies are needed to determine if yoga therapy in patients undergoing active treatment can impact long-term weight change.
In this study, there was a trend toward decreased CRP and TNF-alpha following yoga therapy, while these inflammatory makers remained stable in the standard of care arm. Although we cannot conclude a significant difference given our small sample size, this suggests that yoga therapy may ameliorate some of the systemic inflammation associated with BC and BC treatment. Previous studies of yoga in BC patients have found similar decreases in TNF-alpha 34 and other inflammatory markers. 31 This is of interest as reducing associated chronic inflammation improves prognosis (recurrence and mortality) among women with BC. 44
Interestingly, even with the relatively small sample size of our study, participants in the yoga therapy arm reported better QOL compared to participants in the control arm. Control patients had a decline both in overall QOL and in fatigue scores, while yoga patients’ QOL and fatigue scores remained stable. A subscale score change of 2 to 3 likely represents a meaningful important difference in the FACT-G7 assessment, 45 so the changes in QOL measures seen in our study may be of significance. Given the wide confidence intervals, larger studies with higher power may be warranted to detect whether the QOL differences observed here fall into a clinically significant range. These data suggest that yoga therapy may be beneficial in terms of maintaining QOL during treatment. This is in line with the findings of previous studies, which have consistently shown that yoga improves QOL and fatigue among BC patients.29,31,32
Limitations
As a pilot study, this study had several obvious limitations. The sample size was small and not powered to detect difference in outcomes of interest beyond feasibility; a larger, longer study with sufficient power will be needed to detect differences in long term weight change and inflammatory markers. In addition, a larger study will include body composition measures to ensure patients are losing fat mass, as opposed to muscle mass, given these patients are at risk for losing muscle mass with their cancer treatments. 46 Additionally, the participants in our study were predominantly white and from a single cancer center. However, nearly 25% of our participants were minorities, which is higher than the minority rate of the community that the cancer center serves. Future studies should aim to include multiple centers and continue to recruit minority participants to mirror the diversity of the general BC population. A patient satisfaction measure was not included in this trial, and although satisfaction tends to be high with yoga-based interventions, 47 future studies should include a patient satisfaction measure.
Suggestions for Future Mindful Yoga Therapy Design
First, it would be beneficial for the patient, in addition to the gentle yoga practice, to emphasize the practices of yoga breath work, mindfulness and relaxation in reducing stress. Second, there is a significant need to meet with patients in a designated area for initial yoga training. In other studies, this has been done with a formal yoga class.21,23,24,29,32 Third, the yoga therapy would benefit from being separated into individual modules that patients can use: relaxation and meditation; gentle seated movement; standing poses. This would allow patients to choose a module depending on their needs for a particular day. This was done successfully by one Japanese study that reported high levels of compliance and acceptability. 42 Additionally, completing shorter more frequent sessions may be necessary and more realistic for patients receiving chemotherapy. Finally, it is critical to develop and communicate a rigorous follow-up regime so that patients’ individual needs can be met.
Conclusions
Yoga has been found by many over the years to be considered most effective when practiced for an extended period of time, with consistency and a positive attitude toward outcome. 48 This study suggests that yoga therapy may improve QOL, as has been shown in previous studies, but importantly, is the first study to show that yoga therapy may ameliorate weight gain which is so commonly associated with BC treatment. The patients randomized to the yoga therapy arm did not gain weight during chemotherapy, even with lower than expected compliance to the physical yoga poses, suggesting that impact of yoga therapy, incorporating mindfulness, may lead to improvements in outcomes over physical yoga asanas alone. Larger randomized controlled studies conducted during breast cancer treatment are needed to determine the impact of yoga therapy on short- and long-term weight change.
Supplemental Material
sj-docx-1-ict-10.1177_15347354221137285 – Supplemental material for Yoga Therapy During Chemotherapy for Early-Stage and Locally Advanced Breast Cancer
Supplemental material, sj-docx-1-ict-10.1177_15347354221137285 for Yoga Therapy During Chemotherapy for Early-Stage and Locally Advanced Breast Cancer by Samantha K. Greaney, Neha Amin, Bethany C. Prudner, Maggie Compernolle, Linda J. Sandell, Susan C. Tebb, Katherine N. Weilbaecher, Peri Abeln, Jingqin Luo, Yu Tao, Angela C. Hirbe and Lindsay L. Peterson in Integrative Cancer Therapies
Supplemental Material
sj-pdf-2-ict-10.1177_15347354221137285 – Supplemental material for Yoga Therapy During Chemotherapy for Early-Stage and Locally Advanced Breast Cancer
Supplemental material, sj-pdf-2-ict-10.1177_15347354221137285 for Yoga Therapy During Chemotherapy for Early-Stage and Locally Advanced Breast Cancer by Samantha K. Greaney, Neha Amin, Bethany C. Prudner, Maggie Compernolle, Linda J. Sandell, Susan C. Tebb, Katherine N. Weilbaecher, Peri Abeln, Jingqin Luo, Yu Tao, Angela C. Hirbe and Lindsay L. Peterson in Integrative Cancer Therapies
Footnotes
Acknowledgements
Not applicable
Author Contributions
Designed Study: ACH, LP, KNW, LS, ST, JL, YT
Implemented Study: PA, LS, ST, MC
Performed experiments: NA, BCP
Analyzed data: NA, SG, BCP, JL, YT
Writing of manuscript: SG, ACH, LS, ST, MC, LP, KNW, BCP
All authors read and approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially funded by a grant awarded to ACH from the Barnes Jewish Hospital Foundation. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Ethics approval and consent to participate
Approval was obtained from the Washington University Institutional Review Board prior to the start of the trial. All procedures performed were in accordance with the 1964 Helsinki declaration and its later amendments. All participants signed informed consent prior to their participation in the study.
Consent for publication
Not applicable
Availability of data and materials
The datasets used and/or analyzed during the current study and full trial protocol are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.