
Abstract
Introduction
The problem of studying the quality of life and physical, social, and psychological adaptations of women after surgical treatment for breast cancer becomes more acute in the event that there is more chance of successful recovery in connection with the improvement of long-term results of breast cancer treatment.1,2
As a result of recent research, it was found that breast cancer survivors had a deterioration in the psycho-emotional status and a decrease in most criteria of quality of life, which were directly related to the severity of post-mastectomy edema, pain, and neurological disorders.3-6
Women with breast cancer have an increased risk of developing depression, anxiety, sexual dysfunction, sleep disturbances, cognitive problems, fatigue, and sexual problems. Assessment of life quality parameters has become a significant criterion of woman’s cancer rehabilitation.7-9
The credibility of a possible role of physical exercise in improving the quality of life, reducing the risk of relapse, and increasing the survival rate of cancer patients is increasing today. Physical activity can promote a favorable outlook for cancer biomarkers, normal energy balance, and a reduction in the risk of cardiovascular disease, which is one of the major causes of death for many people who survived cancer. 10
Many studies have been conducted to improve physical functioning and psychological well-being for breast cancer survivors, including water-based exercises,11-13 Pilates intervention, 14 yoga exercises,15-18 cognitive-behavioral therapy, 19 cognitively based compassion training, 20 and aerobic and resistance exercises 21 for problems associated with poor quality of life of patients. It has been suggested that research on benefits of different exercise interventions on various aspects of quality of life in cancer patients should be performed. 21
Taking into account research data showing that physical exercise is effective and safe for breast cancer patients, we decided to evaluate the effects of different exercise interventions on quality of life parameters in breast cancer patients during 1 year of outpatient rehabilitation.
Methods
The study was designed as a randomized, prospective, controlled trial. The study abided by the guidelines of the Declaration of Helsinki and was approved by the authors’ institutional Ethics Committee (Number 2017/12-11). Participants’ type of surgery treatment and cancer stage were determined using medical records. Eligible participants’ age ranged between 50 and 60 years, average time after breast cancer surgery ranged between 5 and 6 months, and women had to have completed adjuvant chemotherapy and radiotherapy. The focus was on women aged between 50 and 60 years, because the incidence of breast cancer was the highest in this age category. Women were randomized using sequentially numbered, opaque sealed envelopes. Randomization was done by an independent person via random numbers generated in Microsoft Excel. An independent person who was separate from the assessment and recruitment of the patients opened the envelope. Patients were recruited through direct referrals from oncologists at the Zaporizhzhya Regional Cancer Center.
Exclusion criteria consisted of women with bilateral mastectomy, metastases, stage III tumor, or any contraindications limiting activity. A total of 115 breast cancer patients met the eligibility criteria and completed the study. Participants were randomly allocated for the water exercise intervention (group A, n = 45), the Pilates exercise intervention (group B, n = 40), or the yoga exercise intervention (group C, n = 30). The 3 groups attended relevant programs for 1 year and received 144 rehabilitation sessions conducted by the same physiotherapist. Quality of life parameters were assessed using the Functional Assessment of Cancer Therapy questionnaire with a specific module for breast cancer patients (FACT-B).Quality of life data were recorded at baseline and after 6 and 12 months of exercise interventions. An independent researcher administered the FACT-B and was blinded to the group assignment of the participants. Administering of FACT-B was done at Zaporizhzhya Regional Cancer Center.
The fourth version of the FACT-B questionnaire has 4 primary quality of life domains: physical well-being, social/family well-being, emotional well-being, and functional well-being, and a special subscale for breast cancer patients. Physical, functional, and social/family well-being domains were rated by 28 points, emotional well-being domain was rated by 24 points, special subscale for breast cancer patients was rated by 36 points, and the arm subscale was rated by 20 points. 22
Data recorded (mean and standard error of the mean) were analyzed using Statistica for Windows (version 8.00). Before concluding analysis, data were evaluated for normality assumption, homogeneity, and occurrence of extreme scores. The distribution of the data recorded was tested using the Shapiro-Wilk test. This analysis was performed as preliminary measure before parametric calculations of the analysis of difference. Dependent samples t test was used to analyze life quality changes in one group between baseline and postintervention. Independent sample t tests were used to compare postintervention life quality parameters between the women of the 3 groups. Sample size was based on detection of meaningful differences in primary end points with 80% power and a 2-sided 5% significance level.
Interventions
The 3 groups performed relevant programs 3 times per week for 1 year and received 144 rehabilitation sessions. Each of the intervention sessions lasted 60 minutes. Attendance rate of the sessions in group A was 92%, in group B 90%, and in group C 94%. Intervention sessions were held at the Zaporizhzhya Regional Cancer Center. The Cancer Center has a convenient location in the city center, which made it possible for patients to attend classes regularly.
Group A received water exercise interventions that were implemented 3 times per week for 12 months. Distinctive features of proposed water exercises were rational combination of exercises in the horizontal and vertical positions of the body in deep and shallow water, which allowed to engage practically all muscles of the body. Water exercises consisted of a wide range of breathing exercises (static and dynamic) and physical (active, active-passive, special, combined developing, and sports-applied) exercises that helped solve current tasks. Water exercises were built on a rational combination of swimming, combined developing exercises, and exercises of local impact on different muscle groups using various initial positions: standing, half-squatting, sitting, and lying on noodles. Noodles, blades, and water dumbbells were used to increase the load. The intensity of physical activity depended on the motion state and varied from 45% to 60% of heart rate reserve. Heart rate was monitored using Polar.
Group B received Pilates exercises 3 times per week for 12 months. Pilates exercises were performed on the floor and included warmup, a main part using a resistance band, and cool-down. The total duration of the session was 60 minutes. Differentiation of Pilates exercises was performed taking into account the degree of patients’ lymphedema. Patients who had first and second degrees of lymphedema performed special exercises from different initial positions: standing, lying on the back, lying on the side, and sitting on the fitball. Women with third degree of lymphedema performed the majority of exercises from lying initial positions without special equipment. Exercise intensity was individualized for the patient and varied from 45% to 60% of heart rate reserve. Flexibility and resistance exercises were directed at the muscles of the scapular waist, lower limbs, back, and abdomen.
Group C received yoga exercises based on the Hatha yoga approach 3 sessions per week for 12 months. For group C, the yoga exercise session was performed as follows: warmup (10 minutes), followed by exercising (40 minutes), and ended by cooling down (10 minutes). The training of yoga physical exercises began with the study of the asana techniques, breathing exercises, and after successful assimilation, static and motor activity gradually proceeded to the implementation of integral dynamic asana complexes that were performed without pause. The breathing exercises were performed with an emphasis on a long exhalation, well coordinated with movements. The intensity of yoga exercise varied from low to moderate. Women constantly concentrated on their own feelings while doing the exercises.
Results
The CONSORT flow diagram is presented in Figure 1. The detailed characteristics of study participants are presented in Table 1. The study was conducted at the Zaporizhzhya Regional Cancer Center, Ukraine, between December 2017 and March 2019. There were no baseline differences between the studied groups by sociodemographic, treatment-related, or life quality characteristics. We screened 138 women for eligibility; 14 (10%) were excluded. The primary reasons for ineligibility were diagnosis with Stage 3 breast cancer (n = 4), less than 6 months, or more than 12 months posttreatment completion (n = 4); declined to participate (n = 6). One hundred and twenty-four breast cancer patients were randomly enrolled into 1 of the 3 groups. One hundred and fifteen women completed the study and were involved in the final analysis. Validated Functional Assessment of Cancer Therapy questionnaires were provided to women at baseline and at 6-month and 12-month intervals.

CONSORT flow diagram.
Sociodemographic and Treatment-Related Characteristics of Study Participants.

Results of life quality changes by the FACT-B+4 questionnaire in group A are presented in Table 2. Analysis of self-reported parameters of life quality after 6-month water exercise intervention indicated that physical well-being significantly improved by 3.89 points (P < .001), social/family well-being improved by 1.76 points (P < .001), emotional well-being improved by 2.65 points (P < .001), functional well-being improved by 2.96 points (P < .001), breast cancer subscale improved by 3.16 points (P < .001), and the arm subscale improved by 2.98 points (P < .001). After a 12-month course of study, the above indicators also achieved statistically significant changes. The results presented in Table 3 show that all indicators of life quality improved significantly after 6 months of Pilates training as compared with baseline. After the 6-month intervention physical well-being significantly improved by 3.32 points (P < .001), social/family well-being improved by 1.45 points (P < .01), emotional well-being improved by 2.45 points (P < .001), functional well-being improved by 3.02 points (P < .001), breast cancer subscale improved by 3.90 points (P < .001), and the arm subscale improved by 3.60 points (P < .001); after 12 months the above-mentioned indicators improved by 6.82 points (P < .001), 3.40 points (P < .001), 4.35 points (P < .001), 6.05 points (P < .001), 5.70 points (P < .001), and 5.92 points (P < .001), respectively.
Dynamics of Life Quality Indicators in Group A by FACT-B+4 Questionnaire (Scores).

Abbreviation: FACT-B, Functional Assessment of Cancer Therapy questionnaire with a specific module for breast cancer.
P < .001 compared with the baseline data; •••P < .001 compared with the baseline data.
Dynamics of Life Quality Indicators in Group B by FACT-B+4 Questionnaire (Scores).

Abbreviation: FACT-B, Functional Assessment of Cancer Therapy questionnaire with a specific module for breast cancer.
P < .01; *** P < .001 compared with the baseline data; •••P < .001 compared with the baseline data.
The results presented in Table 4 show that after the 6-month yoga intervention physical well-being significantly improved by 4.20 points (P < .001), social/family well-being improved by 2.43 points (P < .001), emotional well-being improved by 2.66 points (P < .001), functional well-being improved by 3.63 points (P < .001), breast cancer subscale improved by 3.40 points (P < .001), and the arm subscale improved by 4.10 points (P < .001); after 12 months the above-mentioned indicators improved by 8.13 points (P < .001), 4.77 points (P < .001), 4.63 points (P < .001), 5.03 points (P < .001), 7.30 points (P < .001), 6.70 points (P < .001), respectively.
Dynamics of Life Quality Indicators in Group C by FACT-B+4 Questionnaire (Scores).
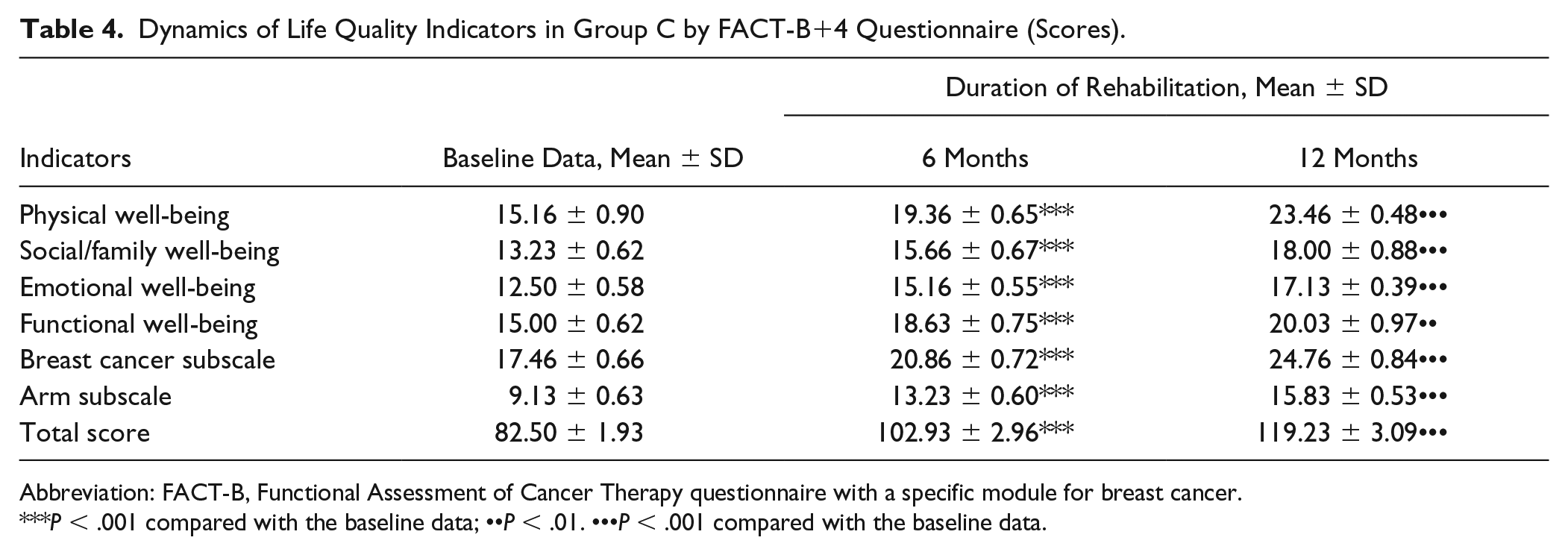
Abbreviation: FACT-B, Functional Assessment of Cancer Therapy questionnaire with a specific module for breast cancer.
P < .001 compared with the baseline data; ••P < .01. •••P < .001 compared with the baseline data.
Comparing the results of life quality parameters of between groups in 12 months, some significant differences were found (Table 5). Based on the results obtained, patients of group A scored significantly more points for emotional well-being compared with group B and group C by 1.40 points (P < .05) and 1.69 points (P < .01), respectively, as well as by breast cancer subscale by 2.15 points (P < .05) compared with group B. At the same time, the indicator of social/family well-being was significantly higher in patients of group C compared with group A by 2.80 points (P < .01). Patients of group A showed middle and large effect sizes by emotional well-being compared with group B and C, respectively. In addition, participants of group A showed middle effect size by breast cancer subscale compared with group B.
Comparison of Life Quality Indicators by FACT-B+4 Questionnaire (Scores) Between Studied Groups After 12 Months of Interventions a .
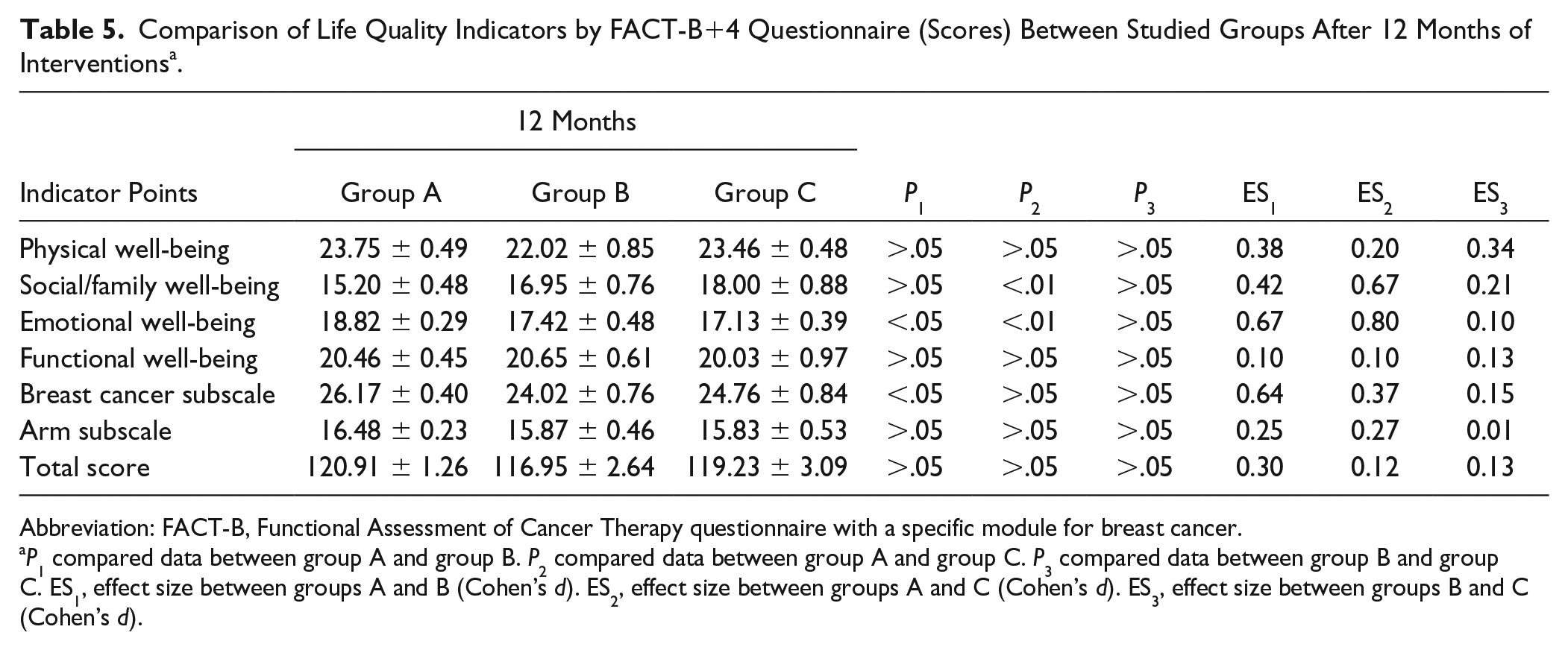
Abbreviation: FACT-B, Functional Assessment of Cancer Therapy questionnaire with a specific module for breast cancer.
P1 compared data between group A and group B. P2 compared data between group A and group C. P3 compared data between group B and group C. ES1, effect size between groups A and B (Cohen’s d). ES2, effect size between groups A and C (Cohen’s d). ES3, effect size between groups B and C (Cohen’s d).
Discussion
Results from this research indicate that implementation of different exercise interventions had a substantial influence on life quality in women after breast cancer surgery.
Based on the results of the 12-month monitoring, it was found that using water exercise intervention is more effective for improving emotional well-being and decreasing negative symptoms associated with breast cancer treatment compared with Pilates and yoga interventions. The yoga intervention was more effective than the water and Pilates exercise in improving social/family well-being.
The results agree with considerable body of research that recommend regular physical exercises as effective tools for reducing fatigue, stress, and depression, and improving physical fitness and life quality in breast cancer patients.23-26
Previous studies have observed10-13 that water exercises were effective tools for reducing pain and lymphedema, but various intervention methods, duration, and intensity of exercises create some difficulties in comparing the results obtained in the context of current research. The proposed water exercise intervention exhibited a significant improvement in quality of life. The combination of various modes of training, particularly resistance and endurance training, had a great impact on all domains of quality of life.
Some previous investigations14,24 have been devoted to the analysis of Pilates exercises as useful practices for women experiencing lymphedema, fatigue, and sleep disturbance. Previous studies applied these interventions frequencies of 2 to 3 sessions per week, durations from 4 to 8 weeks with different combination of intensity for breast cancer patients. The proposed Pilates exercise intervention with a rational combination of breathing, strength, and stretching exercises has been claimed to be beneficial in improving quality of life among breast cancer survivors.
The findings obtained in recent studies15-18,27,28 indicate positive effects of yoga exercises for reducing depression, fatigue, and sleep disturbances, and improving overall quality of life in a breast cancer survivor. Results from this research indicate that using special yoga exercise is safe and effective for increasing shoulder range of motion, balance, and stretching, contributing to improving physical, functional, social/family, emotional well-being domains, and the arm subscale in breast cancer survivors as well as resistance and flexibility training.
The benefits of a water intervention can be explained by the fact that a rational combination of breathing exercises, special exercises in horizontal and vertical body positions in deep and shallow water, made it possible to use almost all the muscles of the body and improve emotional well-being. The strengths of our current research provide a long intervention period compared with most studies that lasted only 1 to 2 months. A positive friendly atmosphere during training sessions and getting positive effect from the exercises were the motivating factors for patients to attend systematic interventions throughout the year. Any harms or unintended effects were not observed in studied groups.
Limitation
The weak side of our study is that physical well-being, social/family well-being, emotional well-being, functional well-being, and special subscale for breast cancer patients were evaluated using a questionnaire and patients’ lifestyle differences could have an impact on the obtained results. Moreover, the sample involved in our research study included predominantly female participants from Ukraine, thus limiting the possibility to generalize to other populations. Another limitation of the study is that only one quality of life measurement was used. The other possible limitations in this study might be psychological and potential cultural issues.
Conclusions
It was found that using water exercise intervention is more effective for improving emotional well-being and decreasing negative symptoms associated with breast cancer treatment compared with Pilates and yoga interventions. Patients of group A scored significantly more points by emotional well-being compared with group B and group C by 1.40 points (P < .05) and 1.69 points (P < .01), respectively, as well as by breast cancer subscale by 2.15 points (P < .05) compared with group B. It was observed that the yoga intervention resulted in better social/family well-being than the water exercise intervention by 2.80 points (P < .01). Further research on water interventions for different population is warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was conducted in accordance to the guidelines of the Declaration of Helsinki.