
Abstract
Aim. The aim of the study was to compare the effects of aerobic exercise training and yoga on the functional capacity, peripheral muscle strength, quality of life (QOL), and fatigue in breast cancer survivors. Material and methods. A total of 52 patients with a diagnosis of breast cancer were included in the study. The patients were randomly assigned to 2 groups: aerobic exercise (n = 28) and yoga added to aerobic exercise (n = 24). Both groups participated in submaximal exercise 30 minutes/d, 3 d/wk for 6 weeks. The second group participated in a 1-hour yoga program in addition to aerobic exercise training. Functional capacity was assessed by the 6-Minute Walk Test (6MWT). Peripheral muscle strength was evaluated with a hand-held dynamometer. The fatigue severity level was assessed with the Fatigue Severity Scale (FSS). The QOL was determined by the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire. Results. There were statistically significant increases in peripheral muscle strength, the 6MWT distance, and the perception of QOL in both groups (P < .05). Additionally, the group with aerobic exercise and yoga showed marked improvement compared with the aerobic exercise group in fatigue perception (P < .05). Conclusion. According to the data from this study, aerobic exercise training and yoga improved the functional capacity and QOL of breast cancer patients. Aerobic exercise programs can be supported by body mind techniques, such as yoga, in the rehabilitation of cancer patients for improving functional recovery and psychosocial wellness.
Introduction
The most common type of cancer in women worldwide is breast cancer. The last report of the Health Ministry in Turkey demonstrated that the prevalence of breast cancer in women is 40.6/100 000 (age standardised rate [ASR]). 1 There is evidence of a strong relationship between the risk of breast cancer and physical activity levels because exercise training is an important physiotherapy and rehabilitation approach in breast cancer survivors. 2
Recent research on the benefits of exercise after the diagnosis of breast cancer is challenging. 3 According to randomized controlled trials on the outcomes of exercise regimens in women with breast cancer, there is improvement in the survival rates for women who exercise. Symptoms related to physical and psychological conditions, such as fatigue, pain, anxiety, depression, and reduced functional capacity, also diminish patients’ quality of life (QOL). 4 Notably, exercise interventions enhance immune function, musculoskeletal performance, cardiorespiratory fitness, body awareness, cognition, and psychological status in breast cancer during or following treatment. 5 Previous studies have shown that exercise programs have beneficial effects on the QOL in cancer patients during and after cancer treatment.6,7
The most accepted exercise regimen for breast cancer survivors is performing moderate- to vigorous-intensity aerobic exercise for approximately 150 minutes per week.8-11 However, only 30% to 47% of breast cancer survivors adhere to these exercise recommendations. 12 According to previous research and the study presented here, aerobic exercise, strengthening exercises, and body mind exercises have an important impact on the adverse effects of cancer survivors. 13
Aerobic and resistive exercises reduce particular physical and psychosocial problems associated with cancer and cancer treatment. 7 The breast cancer survivors can also participate in mindfulness, yoga, or body mind exercise classes to feel better and more relaxed. 14 Currently, yoga is used as a complementary therapy in many major cancer treatment centers worldwide.
Yoga is a mind-body exercise program that provides physiological effects that are similar to aerobic exercise, including physical poses, breathing, and meditation.15,16 Performing breathing exercises during physical activity is important for relaxation. 17 Yoga-related studies have reported improved cardiopulmonary, cognitive, perceptual, motor, spiritual, and physical outcomes in different patient groups. 14 The feeling of a positive mood, reduction in sleep disturbances, and prevention of fatigue are the main results of yoga sessions. 15 Yoga also increases the physical function of the patients as for aerobic exercise training.
Previous studies have already demonstrated the effects of aerobic exercise and yoga on the functional capacity and QOL of breast cancer survivors. Moreover, combining aerobic exercise and yoga programs may provide more information on the effects on functional capacity, muscle strength, fatigue, and QOL than either modality alone. However, no previous studies have investigated the effects of the 2 exercise programs together. The main purpose of the study presented here is to compare the effects of aerobic exercise training and aerobic exercise training with the effects of the addition of yoga on functional capacity as a primary outcome and on the peripheral muscle strength, fatigue, and QOL as secondary outcomes in breast cancer survivors.
Materials and Methods
Participants
This study was carried out in the Cardiopulmonary Rehabilitation Unit of Physiotherapy and Rehabilitation Department and Hope Lodge. Hope Lodge is the first residence in our country, founded by the support of International Union Against Cancer, in which the patients receive medical, psychological, and social support. As a part of Hope Lodge, a Hope Support program has been developed. The Hope Support Program provides emotional support to people affected by cancer, including those who care for them, from the time of cancer diagnosis, through treatment and afterward, to enhance coping skills. Yoga was a part of the Hope Support Program.
A total of 52 volunteer patients, between 20 and 60 years of age with a diagnosis of unilateral breast cancer, who were mentally intact and whose cancer treatment was completed at least 3 years prior participated in the study. A cardiologist performed the cardiological examinations. The randomization procedures were performed by an independent person who selected a random envelope from a box with sealed envelopes. 18 Among the participants, 28 were randomly allocated to the aerobic exercise group; 24 patients were randomly allocated to the aerobic exercise combined with yoga group. Patient demographic data (age, sex, height, weight, and disease duration) were recorded. All patients were inactive before participating in the study. The exclusion criteria for the study included chronic systemic disease and metastasis, relative and absolute contraindications for exercise training, drug therapy with a risk for exercise, types I and II diabetes mellitus, uncontrolled hypertension, and cardiac disease.
The study was accepted by the Ethical Committee of University Medical Faculty. The patients signed informed consent forms after the authors explained the purpose of the study.
Functional Capacity Assessment
The 6-Minute Walk Test (6MWT) is a standardized measure of functional capacity. It has been widely used for measuring the response to therapeutic interventions for pulmonary and cardiac disease. 19 The participants were instructed to walk as far as possible in 6 minutes in an enclosed 30-m long corridor. During the walk, the patients’ heart rate, systolic and diastolic blood pressure, dyspnea, and fatigue perception were recorded using the modified Borg Scale, before and after the 6MWT. 20
Peripheral Muscle Strength Assessment
Peripheral muscle strength (knee extensors, shoulder abductors, and hand grip strength) was measured using a hand-held digital dynamometer (JTECH, Medical Commander Powertrack II, USA). For each area, muscle strength testing was repeated 3 times, and the mean value was recorded in Newtons. The extremity side that underwent surgery is not assessed for muscle strength. The unaffected side was then used in the statistical analysis.21,22
Quality-of-Life Assessment
To assess QOL, the European Organisation for Research and Treatment of Cancer Quality of Life C30 (EORTC QOL-C30) questionnaire was utilized. The questionnaire consists of 30 items, including 5 functional scales (physical, role, cognitive, emotional, and social functioning), 3 symptom scales (fatigue, pain, nausea, and vomiting), and symptoms reported by cancer patients (dyspnea, loss of appetite, insomnia, constipation, diarrhea, and financial difficulties). A score between 0 and 100 was given to each parameter of the EORTC QOL-C30. High scores for functional and global health scales show a good QOL, whereas high scores in the symptom scale indicate higher insufficiency.23,24
Fatigue Perception Assessment
Fatigue perception was evaluated with the Fatigue Severity Scale (FSS). This is a 9-item self-report scale. Scores can range between 9 (no fatigue) and 63 (maximum fatigue). Patients were asked to rate their fatigue level in every statement between 1 and 7 (1, strong disagreement; 7, strong agreement). A score higher than 36 indicates the presence of significant fatigue.25,26
Interventions
Both groups performed aerobic exercise training on a treadmill for 6 weeks, 3 days a week, for 30 minutes each day at the exercise level of 60% to 70% of the predicted maximum heart rate. The heart rate, arterial blood pressure, and fatigue perception were recorded before, during, and after the treatment sessions. The fatigue perception level was examined using the Modified Borg Scale. The aerobic exercise program consisted of a warm-up period, main exercise period, and cool-down period. The warm-up period consisted of 5 minutes of low-intensity exercise. The main exercise phase was performed for 20 minutes at a submaximal heart rate appropriate to the target intensity. The cool-down period was approximately 5 to 10 minutes, with slow reduction in the exercise intensity. The patients were monitored for 5 minutes in the recovery period.
The training intensity was increased with respect to the individual tolerability, with a peak heart rate that corresponded to 90% of the heart rate reached in the 6MWT and a 4 to 6 rating on the modified Borg scale.
The yoga program consisted of 6-week group sessions in Hope Lodge. Yoga classes were approximately 60 minutes and 3 sessions per week on the same day as aerobic exercise training. The yoga program, performed as yogasana, included a set of asanas (physical postures that are adapted to the abilities of cancer patients), pranayama (breathing exercises), awareness meditation, and relaxation techniques with imagery. The postures began with stretching techniques for warm-up followed by standing, supine, and side-lying and sitting postures. The applied asanas were the following: side lateral bending (ardhakati chakrasana), ardhachakrasana, side bending triangle posture (trikonasana), forward bending (padahastasana), bhujangasana, salabhasana, dandasana, janusirşasana, makarasana, matsyasana, naukasana, side angle pose (parshvakonâsana), paschimatanasna, pavanamuktasana, şavasana, ushtasana, vajrasana, vakrasana, veerabhadrasana, tree pose supported by wall (vrikshâsana), and veerasana. 27 Each pose was held for 10 to 30 s, with resting periods between poses lasting for 30 s to 1 minute. Asanas were followed by breathing techniques. Then, meditation was performed in the supine posture with closed eyes and relaxation of every part of the body. The yoga program was supervised by a physiotherapist with a yoga certification.
Statistical Analysis
Data were analyzed using the statistical software package SPSS version 16.0 (SPSS Inc, Chicago, IL) and tested with the Kolmogorov-Smirnov test for normality. The statistical tests were 2 sided, and P < .05 was statistically significant. The results were presented as means and standard deviations and percentage. χ2 Analysis was used to examine the differences in the frequencies for categorical variables. Differences in continuous variables within and between the groups were determined using Student’s t test. Baseline and posttraining data were compared with the paired t test in each group. Vital signs measured in every session were compared with ANOVA analysis.
In the power analysis, the primary outcome was accepted as differences in the 6MWT at the end of the training of 24.26 m in both groups. Finally, the power of our study was 85%, with a confidence interval of 95% and a risk for a type 1 error of 5%. The methodology used for the statistical analysis was a per-protocol approach.
Results
A total of 176 breast cancer patients, screened for eligibility, were admitted to the oncology hospital. Among them 124 patients did not meet the inclusion criteria or refused to participate and were excluded from the study; 52 patients who fulfilled the inclusion criteria and agreed to participate in the study were randomly assigned to yoga combined with aerobic exercise (n = 24) or aerobic exercise training (n = 28). Three patients from the yoga and exercise training group did not receive the treatment because of uncontrolled cardiac disease and hypertension. Two patients in the same group stopped treatment without providing any reasons. In the aerobic exercise training group, 3 patients did not undergo the intervention because of cardiac diseases; also, 3 patients did not attend the program because of transportation difficulties. Therefore, statistical analyses were performed for 19 patients in the aerobic exercise and yoga training group and 21 patients in the aerobic exercise group (Figure 1).
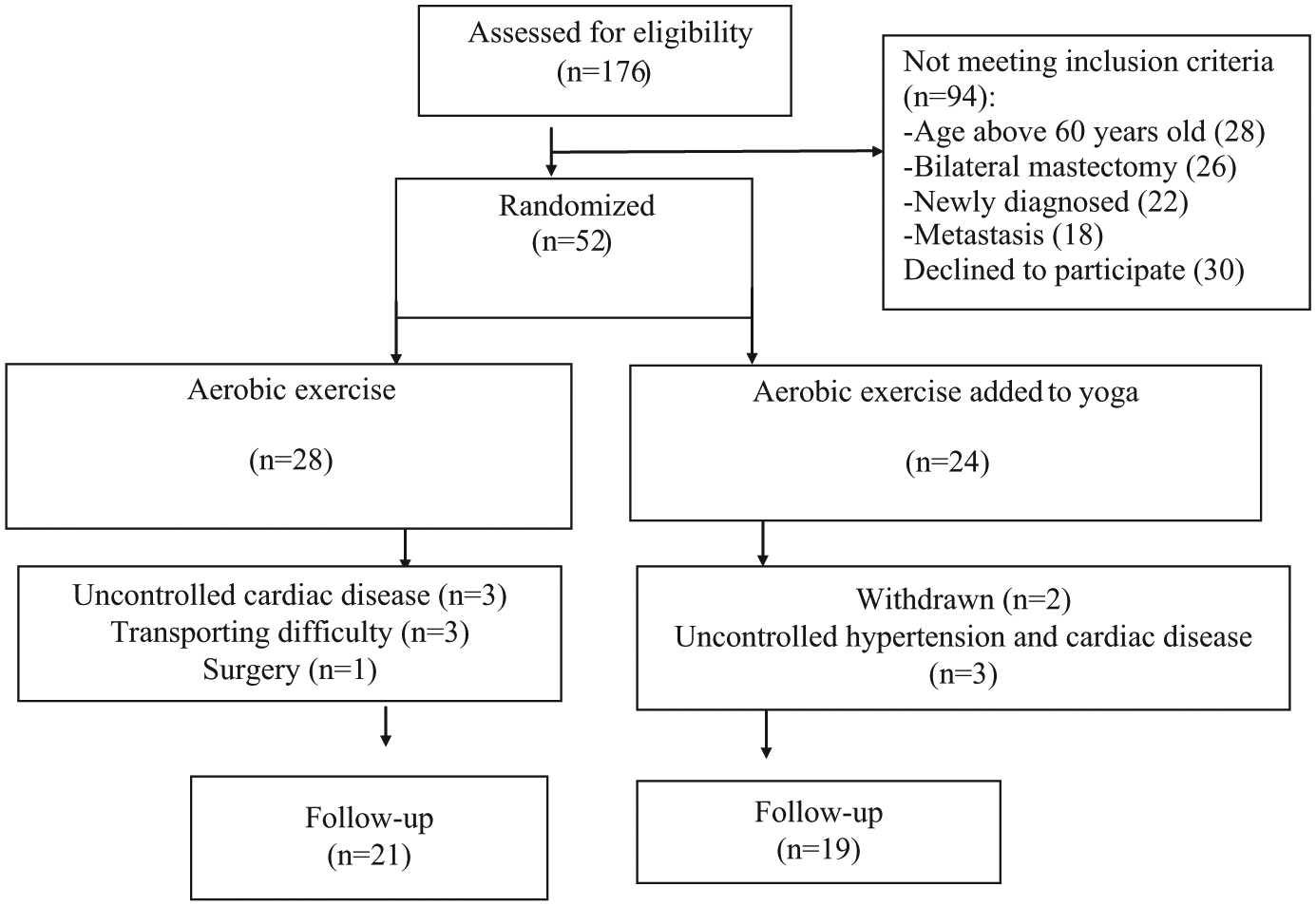
Flow diagram of the participants in the study.
The demographic characteristics (age and body mass index), disease duration, cancer stage, and medical therapy of patients are presented in Table 1. The baseline characteristics of the study groups were similar (Table 1).
Baseline Participant Characteristics.

Abbreviation: BMI, body mass index.
Significance level at P < .05; mean ± standard deviation.
Functional Capacity Assessment
Participants in the yoga and aerobic exercise group had an increase in the distance of the 6-minute walking test (Table 2, P < .05) by 94 m—from 509.2 (40.9) m to 603 (48.8) m—whereas it was 69 m for those in the aerobic exercise group—from 512 (48.6) m to 581.6 (52.2) m.
Comparison of the Peripheral Muscle Strength and Functional Capacity in Both Groups.

Abbreviation: 6MWT, 6-Minute Walk Test.
Significant difference before and after treatment in each group.
Significant difference between the groups.
After exercise training, dyspnea, fatigue, and leg fatigue perception were significantly decreased in both groups, and the improvement was similar in the 2 groups (Table 2, P < .05).
Peripheral Muscle Strength Assessment
Quadriceps, shoulder abductors, and hand grip muscle strength increased significantly in both groups after training (Table 2, P < .05). The improvement in the shoulder abductors and hand grip muscle strength were consistently higher in the yoga and aerobic exercise group (Table 2, P < .05).
Quality of Life Assessment
QOL was assessed with EORTC QOL-C30. Comparison with the EORTC QOL-C30 QOL subscale of the general well-being and functional scores, overall well-being, physical function, role function, emotional, cognitive, and social functioning was obviously improved in the yoga and aerobic exercise group after training (Table 3, P < .05). Differences in the overall well-being, role function, emotional, and social functioning were statistically significant compared with the aerobic exercise group (Table 3, P < .05).
Comparison of the Differences in the Psychosocial Parameters and QOL in the Groups.

Abbreviations: EORTC QOL-C30, The European Organisation for Research and Treatment of Cancer Quality of Life C30; FSS, Fatigue Severity Scale.
Significant difference before and after the treatment in each group.
Significant difference between the groups.
When comparing the EORTC QOL-C30 QOL subscales with the symptom scores, significant improvements were found in the fatigue, pain, dyspnea, insomnia, and constipation scores (Table 3, P < .05). Sleep and constipation scores were significantly improved in the yoga and aerobic exercise group (Table 3, P < .05).
Fatigue Perception Assessment
A statistically significant decrease was found in the FSS score in the yoga and aerobic exercise groups compared with the group that underwent aerobic exercise alone (Table 3, P < .05).
Discussion
This randomized controlled trial demonstrates that yoga combined with aerobic exercise training is more beneficial than aerobic exercise intervention alone in patients with breast cancer. Although both groups showed improvement in the functional exercise capacity, peripheral muscle strength, QOL, and fatigue perception, the yoga and aerobic exercise group had significantly greater improvement in the functional exercise capacity, peripheral muscle strength, QOL, and fatigue perception. All participants stated that they were less tired in their daily activities and during work in addition to their increased capacity in performing various household chores.
When planning exercise programs, exercise tests applied in accordance with the person’s functional capacity are especially important for prescribing individual programs.28,29 In our study, 6MWT was used as a functional capacity assessment that is commonly chosen in clinical trials. 30 Although both groups had marked improvement in the 6MWT after training, the effect of yoga and aerobic exercise (93.85 ± 29.55 m) was higher than the effect of aerobic exercise alone (69.59 ± 17.22 m). Studies investigating the effects of aerobic exercise training and yoga together for improving functional capacity in breast cancer are lacking. Campbell et al 31 observed an increase in the average 60 m in 12 MWT after 12 weekly group exercise programs. Additionally, a study investigating the 7-week Hatha yoga program showed an improvement in the walk distance and reduced resting heart rate. 32 To conclude, yoga may be an effective intervention for increasing the functional capacity, especially when performed together with aerobic exercise programs.
After training, a similar decrease was observed in dyspnea, fatigue, and leg fatigue perception in both groups. Possibly, this decrease was based on the effects of aerobic training. Future studies are required to study the effects of yoga intervention alone.
According to the peripheral muscle strength test, quadriceps, shoulder abductor, muscle strength, and hand grip strength were significantly increased after the treatment in both groups. Shoulder abductor and hand grip muscle strength were higher in the yoga combined with aerobic exercise intervention. This result most likely originates from the yoga program, including upper-extremity activities as well as aerobic exercise training. In the recent studies on breast cancer, hand grip strength assessments were also performed.21,33 Harrington et al 21 demonstrated that upper-limb function was impaired after breast cancer–related surgery and reported that the normal shoulder joint movement and function should also be assessed. Aerobic exercise training causes an increase in the muscle myoglobin content, volume, and size of mitochondria34,35; therefore, skeletal muscle strength and endurance can be increased. 25 To the best of our knowledge, this is the first study that shows the effects of yoga and aerobic exercise training on peripheral muscle strengthening.
Many studies on breast cancer patients have investigated the effects of exercise training on QOL.36,37 In our study, we used the cancer-specific EORTC QOL-C30. The EORTC QOL-C30 QOL subscale for general well-being and functional scores on general well-being, physical function, and emotional and social functioning were significantly improved in both groups. A total of 729 early-stage breast cancer survivors were recommended to perform physical activity to improve QOL in the energy levels, social functioning, emotional role, and overall well-being. 38 There was greater improvement in general well-being, role, and social and emotional function in the yoga combined with aerobic exercise intervention. Yoga has positive effects on the emotional state by providing social sharing and contributing to the spiritual development. Studies have reported that yoga programs for breast cancer patients are associated with better coping skills, overall well-being, and spiritual development after chemotherapy, radiotherapy, and systemic treatment.39-41
The EORTC QOL-C30 QOL symptom subscale scores showed significant decreases in the fatigue, pain, sleep disturbance, dyspnea, and constipation parameters in both groups. Sleep disorders and constipation scores were significantly better in the yoga and aerobic exercise group.
In our study, the fatigue levels of patients were evaluated using the FSS. The baseline FSS scores of all participants were greater than 36 in our study, showing that our patients have severe fatigue. The FSS scores were reduced an average of 15 points in the yoga and aerobic exercise group, whereas the aerobic exercise group decreased an average of 7 points. The reduction in the fatigue perception may be a result of the improvement in the emotional state and heightened sense of confidence and increased motivation in the yoga group.
There are several limitations in the present study. We did not include a group that practiced yoga alone, and we could thus not report the effects of yoga alone. The exercise training period was 6 weeks. Longer exercise intervention is needed to determine the effects on other outcomes. The power analysis was performed post hoc according to the primary outcome (6MWT) but revealed that the study had sufficient power (85%) to support our conclusions. Areas for future research include appropriate levels of intensity for exercise training and the application of the program during cancer treatment and with patients undergoing bilateral mastectomy.
Conclusion
According to the data in the study, aerobic exercise training and yoga improved the functional capacity and QOL of breast cancer patients. Aerobic exercise programs can be supported by body-mind techniques, such as yoga, in the rehabilitation of cancer patients to improve their functional recovery and psychosocial wellness. These findings are important in oncological rehabilitation to create awareness within the interdisciplinary team. The outcome of this study could also be very important from the point of view of functional capacity improvement, which can be effectively utilized in cancer prevention.
The results of this study indicate that participation in physical activity with interventions such as aerobic exercise training and yoga in breast cancer patients is an effective method for sustaining functional capacity and QOL. Finally, mind-body approaches should also be considered in addition to aerobic training in physiotherapy and the rehabilitation of the patients who survive breast cancer.
Footnotes
Acknowledgements
The authors thank all participants of the study and staff of Hope Lodge for their patience and kindness during the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by University Research Center (PhD Thesis Grant No: 5129).