
Abstract
Objective:
Fatigue associated with malignant conditions and their treatments is a disabling condition. This trial assessed the anti-fatigue effects of melatonin coadministration during adjuvant treatment of patients with the breast cancer.
Material and Methods:
Patients with breast cancer were randomly assigned to receive melatonin or placebo during adjuvant chemotherapy and radiotherapy. Thirty-seven patients were randomly enrolled in each group. The mean ages of patients in the intervention and control groups were 50.47 ± 10.79 and 46.05 ± 10.55 years, respectively (P = .223). The intervention group received oral melatonin (18 mg/day) from 1 week before until 1 month after the adjuvant radiotherapy. The level of fatigue was assessed before and after intervention using Brief Fatigue Inventory (BFI) in both groups. To analyze data, the Student’s t-test and the Chi-square test were used at a significance level of P ≤ .05.
Results:
The BFI score was similar before the intervention in both groups, however, after the intervention, it was significantly lower in the melatonin group (P < .001). Moreover, the frequency of severe fatigue in the melatonin group was significantly lower than in the placebo group after intervention (42.1% vs 83.3%, P < .001).
Conclusion:
Coadministration of melatonin during adjuvant chemotherapy and radiotherapy of women with breast cancer decreased the levels of fatigue associated with the malignant condition and its treatments.
Introduction
Breast cancer is the most common malignancy and the leading cause of cancer-related deaths in women worldwide, including Iran, and is responsible for 24.6% of all cancers in Iranian women.1,2 Cancer-related fatigue (CRF) is one of the most common and debilitating side effects in breast cancer patients, especially in those who are receiving adjuvant therapies, specifically chemotherapy, radiation therapy, and hormone therapy.3,4
The underlying pathophysiology of CRF has not been elucidated clearly yet, however, tumor- directed or treatment-related factors along with preexistent medical or psychiatric disorders have been proposed.5,6 The hyperinflammation status resulting from tumor burden 7 and its treatments, 8 neuroendocrine alterations9,10 and autonomic nervous system dysregulation 6 are main postulated mechanisms.
Melatonin (MLT; N-acetyl-5-methoxytryptamine) is a pineal gland-originated hormone which induces its main function, that is, the chronobiotic action and regulation of the sleep–wake cycle, through acting on the circadian and seasonal patterns.11,12 Moreover, alteration of its level has been reported in depressive disorders. 13 Beside these clinical effects, melatonin has several effects on the molecular level including antioxidative, oncostatic, antiproliferative, and immunomodulatory ones.14-16 As a novel medication, several reports assessed the therapeutic use of melatonin in circadian rhythm-related metabolic disorders, and reviews and meta-analysis have been conducted in this regard showing promising results with a need for further evaluations.17-19
Cancer patients generally have lower levels of melatonin compared to the healthy population and it has been shown that melatonin supplementation helps patients to overcome sleep disorders and improves quality of their life, besides its potential anti-tumoral effects.20-23 In breast cancer, melatonin plays an important role in cancer development due to its potential effects on the inhibition of tumor cell proliferation and metastasis and its anti-angiogenic effects. Especially in hormone-positive breast cancer which is the most common subtype, melatonin can modulate estrogen-dependent pathways effectively. 24 In addition, studies showed that there is a strong relationship between low melatonin levels and poorer sleep quality and presence of mood disorders in patients with breast cancer that can subsequently lead to CRF. Zaki et al, in their study, showed a significant dysregulation of secretion of melatonin in patients with breast cancer, especially in the presence of tumor mass, that can be partially normalized by tumor resection. 25 Melatonin supplementation, however, may be needed in order to complete maintenance of melatonin levels.
There are limited data on the possible role of melatonin in the management of fatigue in patients with cancer and there is controversy about its efficacy especially in patients with advanced disease.22,26 This study aimed to assess the effects of coadministration of melatonin during adjuvant chemotherapy and radiotherapy of breast cancer on the fatigue associated with breast cancer and its adjuvant treatments.
Methods and Materials
Study Patients
In a double-blinded randomized placebo-controlled clinical trial, female patients with confirmed pathologic diagnosis of invasive breast carcinoma were enrolled. The study was conducted at Be’sat Hospital and Mahdieh Diagnostic and Treatment Center of Hamedan, Iran. Inclusion criteria consisted of stage I to III breast cancer (according to The American Joint Committee on Cancer (AJCC) staging system, 8th Edition) who were candidates to receive adjuvant chemotherapy and radiotherapy based on the National Comprehensive Cancer Network (NCCN) Guidelines for Patients with Invasive Breast Cancer. Also, there was no limitation regarding the type of surgery, hormone prescription, or type of systemic therapy. Exclusion criteria were prior history of malignancy and chemotherapy, presence of distant metastasis at presentation, and neoadjuvant chemotherapy schedule. Patients with uncontrolled hypercalcemia, lactation, and pregnancy were excluded. Also, patients who used warfarin, methylphenidate, and sleeping pills were excluded.
Patients were recruited at the oncology departments of Be’sat Hospital affiliated to Hamedan University of Medical Sciences and Mahdieh Diagnostic and Treatment Center of Hamedan during spring and summer of 2019 by simple random sampling method. The study protocol was approved by the Research Ethics Committee of the Medical School of Hamedan University of Medical Sciences (IR.UMSHA.REC.1397.5). Also, the study was registered on the Iranian Registry of Clinical Trials (IRCT20180426039421N1). Undersigned informed consent was obtained from all patients prior to the enrolment.
Trial Design and Definition of Primary Endpoints
The study was designed as a double-armed randomized prospective trial. A random number table which was generated by www.randomization.com was used to assign patients randomly in each group. A person who was out of the research team put the numbers that were dedicated to each group in sealed envelopes to be opened at the time of assignment.
The primary endpoint was defined as level of fatigue which was assessed by the Brief Fatigue Inventory (BFI) questionnaire. The Persian version of the BFI validated and described by Karimi et al previously was used. 27 Briefly, the scores in BFI are as follows: No fatigue = 0, mild fatigue = 0-3, average fatigue = 4-6, severe fatigue = 7-9, and very severe fatigue = 10. The CRF was assessed before and 4 weeks after intervention.
The study was designed double-blinded and placebo-controlled, and the physicians, nurses, outcome assessor, and patients were not aware of the study group assignment.
The occurrence of any significant chemotherapy related side-effects, that is, febrile neutropenia or other grade ≥2 toxicities based on the Common Terminology Criteria for Adverse Events (CTC-AE) v 5.0 resulted in exclusion of patients from the study.
Treatment Schedule
The adjuvant treatment consisted of chemotherapy initially and then radiotherapy and was initiated in all patients in both groups within 4 weeks from the surgery (breast conserving surgery (BCS) or modified radical mastectomy (MRM)). The intervention group received 18 mg oral melatonin daily (18 mg once a day) from 1 week prior to adjuvant chemotherapy until 1 month after completion of adjuvant radiotherapy every night approximately 1 hour before bedtime. The placebo group received a similar cellulose-made drug with similar instructions and duration. Melatonin tablets were provided by RAZAK Laboratory, Tehran, Iran, and similar tablets were produced at the School of Pharmacy, Hamedan University of Medical Sciences, Hamedan, Iran.
All patients received the dose-dense AC-T chemotherapy regimen [including doxorubicin (A), cyclophosphamide (C), and paclitaxel (T)] every 2-weeks with granulocyte colony-stimulating factor (G-CSF) for 8 cycles [AC ×4 and T ×4].
In Her2/neu positive patients, Trastuzumab was added within and after the prescription of paclitaxel, however, the study was caried out just until 1 month after completion of adjuvant radiotherapy.
The radiotherapy treatment schedule in both groups was conventional radiotherapy of chest wall/whole breast with regional node irradiation if clinically indicated.
Data Registration, Quality Assurance and Follow-Up
Patients were visited weekly during radiation and before each session of chemotherapy. Another patient visit was 1 month after completion of adjuvant chemotherapy and radiation treatments. All visits were done in the corresponding oncology clinics. In each visit, patients were asked about the use of melatonin/placebo drug to assess their adherences to the treatment. In total, the study lasted 25 weeks (one week before the start of adjuvant treatment, 16 weeks for during chemotherapy, 5 weeks for radiotherapy, 4 weeks for follow-up). The BFI was assessed in 2 visits including 1 week before the start of adjuvant treatment and at 4 weeks after its completion by one of investigators (Z.K.A.) who were blinded to the groups.
Statistical Methods
Sample size was calculated based on results of our pilot study using
Results
Of 78 eligible patients, 41 patients were enrolled in the intervention group (oral melatonin) and 37 were enrolled in control group (oral placebo). In the intervention group, 3 patients were excluded due to severe nausea and vomiting. And in the control group, 1 patient was excluded due to failure to follow up (Figure 1).

Screening, randomization, and analysis.
Mean age of patients in intervention and control group was 50.47 ± 10.79 and 46.05 ± 10.55 years, respectively (P = .232). All patients in both groups had Eastern Cooperative Oncology Group (ECOG) performance score of 0-1. Characteristics of the patients at baseline are shown in Table 1.
Characteristics of the Patients at Baseline.

Abbreviations: BCS, breast conserving surgery; DM, diabetes mellitus; DOX, doxorubicin; ER, estrogen receptor; Her2, human epidermal growth factor receptor 2; HTN, Hypertension; MRM, modified radical mastectomy; PR, progesterone receptor.
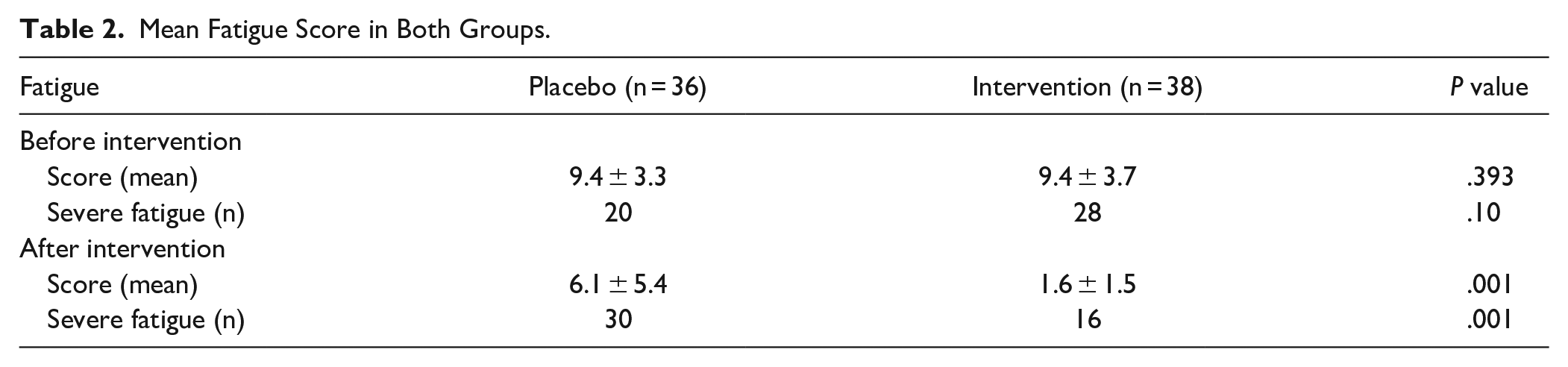
There was no statistically significant difference between severity and mean score of fatigue in the patients before the intervention. However, after intervention, the mean fatigue score and severity of fatigue were significantly lower in the intervention group (P < .05; Table 2).
Mean Fatigue Score in Both Groups.
Discussion
In the present study, the level of fatigue decreased significantly after coadministration of melatonin during adjuvant chemotherapy and radiotherapy of patients with breast cancer. There are controversies regarding the role of melatonin in the management of fatigue in patients with breast cancer. Consistent with results of present study, in a study by Palmer et al the results showed that prescription of melatonin during adjuvant chemotherapy patients with breast cancer resulted in significant reduction of fatigue. 22 In their randomized, double-blinded, placebo-controlled trial, patients with breast cancer received 20 mg of oral melatonin daily before and after the first cycle of adjuvant chemotherapy. Although they did not assess fatigue as an independent variable, they used the European Organization for Cancer Research and Treatment (EORTC QLQ-C30) questionnaires which is a validated instrument to evaluate different side-effects in patients with cancer, including fatigue. They showed that the EORTC QLQ-C30 decreased significantly after intervention compared to the placebo group who showed no significant changes. 22 In another study by Semiglazova, results showed that melatonin coadministration during neoadjuvant chemotherapy of patients with breast cancer is associated with decreased level of fatigue as assessed by EORTC QLQ-C30. 28 In opposition to the findings of the present study, Lund Rasmussen et al showed no benefits for using oral melatonin on fatigue in patients with cancer. 26 In their trial, patients with various metastatic cancers who were on palliative treatments were enrolled to receive melatonin at a dose of 20 mg or placebo. They showed that there was no significant change in the score of fatigue in both groups. 26 Recruitment of patients from the Department of Palliative Medicine who had histories of treatment with several lines of chemotherapy or radiotherapy and the chronic nature of metastatic disease may be the reason for this negative results.
There are some limitations in the current study. Not assessing the pretreatment level of melatonin in the serum of patients, not addressing the potential side effects of adjuvant treatments and their relationship with CRF, and using a single inventory to assess CRF considering the various methods available 29 are among of them. Also, the multifactorial nature of fatigue which can be affected by social and economic status of patient that are beyond ability of researchers to control them is another limitation.
Conclusion
Oral administration of melatonin in women with breast cancer undergoing radiation therapy and chemotherapy in adjuvant setting significantly reduced associated fatigue.
Footnotes
Acknowledgements
We thank all staffs of Besat Medical Center of Hamadan University of Medical Sciences and Mahdieh Diagnostic and Charitable Center of Hamedan. We also grateful for sincere participation of all patients with breast cancer in the current study.
Author Contribution
Study concept and design: A.S.P., K.M., and S.A.; acquisition of data: E.A.H, M.H.G., and A.M.; analysis and interpretation of data: S.A.J. and Z.K.A.; drafting of the manuscript: S.A.J. and Z.K.A.; critical revision of the manuscript for important intellectual content: A.S.P., K.M., and S.A.; statistical analysis: consultant epidemiologist.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Hamadan University of Medical Sciences.
Data Sharing Statement
All data generated and analyzed during this study can be accessible through direct communication with corresponding author and agreement of all research team members.
Ethical Considerations
The protocol of study was approved by Ethics Committee of Hamadan University of Medical Sciences (IR.UMSHA.REC.1397.5). Written informed consent from was obtained before the enrolment.
Clinical Trial Registration
The protocol of study was approved by Iranian Registry of Clinical Trials (IRCT) (IRCT20180426039421N1).