
Abstract
Introduction:
Breast cancer is the most commonly diagnosed cancer worldwide, and most patients experience fatigue. However, there are no effective treatments for cancer-related fatigue (CRF). Several randomized controlled trials (RCTs) have suggested that moxibustion improves CRF. We conducted a systematic review and meta-analysis to compare the differences in fatigue scale scores, quality of life, and clinical efficacy in patients with breast cancer who developed CRF and did versus did not receive moxibustion.
Methods:
RCTs were searched in 7 databases using a standardized search method from database inception to March 2023, and RCTs that met the inclusion criteria were selected.
Results:
Among 1337 initially identified RCTs, 10 RCTs involving 744 participants were selected for this study. The meta-analysis involved assessment of the revised Piper Fatigue Scale scores, Cancer Fatigue Scale scores, Karnofsky Performance Scale scores, Athens Insomnia Scale scores, clinical efficacy, and Qi deficiency syndrome scale scores. Compared with the control, moxibustion was associated with significantly better Piper Fatigue Scale scores (P < 0.0001), quality of life [Karnofsky Performance Scale scores (P < 0.0001)], clinical efficacy (P = 0.0007), and Qi deficiency syndrome scale scores (P = 0.02).
Conclusions:
Moxibustion improves CRF in patients with breast cancer. The efficacy of moxibustion should be further examined by high-quality studies in various countries with patients subdivided by their breast cancer treatment status.
Registration:
PROSPERO ID: CRD42023451292
Introduction
Breast cancer is the most commonly diagnosed cancer worldwide, and 2.3 million women were newly diagnosed with breast cancer globally in 2020. 1 Cancer-related fatigue (CRF) is defined as persistent subjective tiredness linked to both cancer and its treatment, impeding regular functioning. 2 Fatigue is reportedly one of the most important and stressful problems for patients with cancer. 3 The occurrence and intensity of CRF differ based on the patient’s subjective condition and the screening method used, but 50% to 90% of all patients with cancer experience fatigue.4 -7 Unlike fatigue in healthy people, CRF is not associated with overwork and is not resolved by rest or sleep. 8 CRF occurs mainly during cancer treatment, such as cytotoxic chemotherapy, immunotherapy, or radiation therapy; however, due to the sustained impact or late effect of cancer treatment, CRF can last months or years after the malignancy is cured.9 -11 CRF causes physical limitations and psychological, social, and emotional deterioration, all of which adversely impact the quality of life and functional well-being of affected individuals.10,12
A specific review focusing on CRF in patients with breast cancer is necessary because fatigue in breast cancer survivors may have distinct features. 13 Fatigue is a frequently observed symptom in individuals diagnosed with breast cancer. Studies indicate that fatigue is experienced by as many as 99% of individuals undergoing treatment for breast cancer at some stage. 14 Studies have indicated that CRF occurs more frequently in women than in men15,16 and may be more prevalent among survivors of breast cancer than among survivors of other types of cancer,17 -19 including female cancer survivors. 20 Breast cancer has one of the highest survival rates among all cancers, 21 and the quality of life of breast cancer survivors is important. Many women have reported facing challenging symptoms, such as fatigue, persisting for months or even years after completing treatment. 13
Because the cause and mechanism of CRF have not been clearly identified, 22 effective treatment strategies are lacking. Both pharmacological and non-pharmacological treatments are employed to alleviate CRF, but research has shown that these interventions provide only limited advantages at best. 23 Moxibustion, which stimulates certain parts of the human body with heat generated by burning herbal medicines, is a traditional treatment of various diseases in East Asian countries. 24
Like acupuncture, moxibustion is used to improve fatigue in patients with cancer. 25 A meta-analysis conducted in Korea in 2014 demonstrated the efficacy of moxibustion in alleviating fatigue in patients with cancer. 26
Many studies have examined the effectiveness of acupuncture and moxibustion in improving fatigue in patients with cancer, but no comprehensive studies have focused on moxibustion for CRF in patients with breast cancer.
This systematic review and meta-analysis was conducted to synthesize data on the efficacy of moxibustion with respect to fatigue scale scores, insomnia scale scores, quality of life, and safety in patients with breast cancer who have developed CRF.
Methods
This review was prepared according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The review protocol was registered at PROSPERO (NO: CRD42023451292).
Databases and Search Strategy
PubMed, EMBASE, the Cochrane Library, 2 Korean medical databases (Research Information Service System and Korean Studies Information Service System), one Chinese medical database (China National Knowledge Infrastructure), and one Japanese medical database (Japan Science Technology Information Aggregator, Electronic [J-STAGE]) were searched from inception to March 2023. We used the MeSH terms “breast neoplasms,” “fatigue,” and “moxibustion.” The search strategy was as follows: (“breast neoplasms [Title/Abstract]” OR “breast cancer [Title/Abstract]” OR “breast carcinoma [Title/Abstract]” OR “breast tumor [Title/Abstract]”) AND “fatigue [Title/Abstract]” AND (“moxibustion [Title/Abstract]” OR “moxa [Title/Abstract]” OR “mugwort [Title/Abstract]”) in English, Chinese, Korean, or Japanese. The reference list of each study was also reviewed to identify additional studies. No language limitation was used.
Selection Criteria
Two reviewers independently selected the studies for inclusion. They first screened the abstracts of all identified studies and then retrieved and reviewed the full texts of all potentially relevant articles for assessment against the inclusion criteria.
Types of studies
Only randomized controlled trials (RCTs) that used moxibustion to treat CRF in patients with breast cancer were included. Guidelines and conference abstracts were excluded.
Types of participants
Patients with a diagnosis of breast cancer and breast cancer survivors who reported fatigue were included, regardless of their clinical status.
Types of interventions
Any type of moxibustion (including direct, indirect, and infrared laser moxibustion) used as an intervention for fatigue in patients with breast cancer was included. We included studies comparing moxibustion with sham (placebo) moxibustion, routine care (eg, psychosocial interventions, education, and conventional medications), and no treatment.
Outcome measures
We included studies that assessed CRF using validated fatigue scales as a main outcome. Performance status, quality of life, effects on sleep, clinical efficacy, traditional Chinese medicine (TCM) syndrome score, and adverse events were assessed as secondary outcomes.
Data Extraction and Review Process
The data were independently extracted by 2 reviewers. All study characteristics and outcome data were independently extracted according to predefined criteria. Any disagreement was resolved by discussion or consensus with the corresponding author. Duplicate publications, missing data, changes in data, and the median and standard deviation values were assessed by methods described in the Cochrane Handbook. 27
Selection bias (random sequence generation and allocation concealment), performance bias (blinding of participants and personnel), detection bias (blinding of outcome assessment), attrition bias (incomplete outcome data), reporting bias (selective reporting), and other biases were evaluated according to the criteria described in the Cochrane Risk of Bias Tool version 5.4.1. 28 Three potential bias judgments (low risk, high risk, and unclear risk) were determined for each trial.
The Cochrane Collaboration software Review Manager 5.4.1 was used to perform the statistical analysis. 28 Dichotomous data are expressed as the relative risk with the 95% confidence interval (CI). The weighted mean difference (WMD) with 95% CI was calculated for continuous data, and standardized mean differences were calculated for data measured in different manners in each trial. The I2 test was used to assess the heterogeneity of the data. If heterogeneity was present (I2 ≥ 50%), a random-effects model was applied. Otherwise, a fixed-effects model was applied. A statistically significant difference was defined as P < 0.05.
Results
Search Results and Study
In total, 1337 articles were retrieved by searching the databases and other sources. After screening the titles and abstracts to exclude articles that did not meet the inclusion criteria, 10 studies were identified. One trial was published in English, 29 and nine were published in Chinese.30 -32 A flow diagram of the study selection process is presented in Figure 1. All 10 studies were RCTs.

Flow chart of the study selection process for the meta-analysis.
The sample sizes of the trials ranged from 60 to 168. Among the total 744 patients enrolled in the studies, 372 received moxibustion treatment. One trial enrolled male patients, 31 2 trials enrolled patients undergoing postoperative chemotherapy,30,32,33 one trial enrolled patients who had completed postoperative chemotherapy, 34 one trial enrolled patients who had completed postoperative chemotherapy or radiotherapy, 35 one trial enrolled patients who had finished primary cancer treatments (surgery, chemotherapy, or radiotherapy), 29 and six trials reported the breast cancer stage.29,30,32,33,36,37 The duration of moxibustion administration ranged from 2 to 8 weeks. Patients with Yang deficiency were selected as participants in the studies conducted by Bao 36 and Chen et al 31 Participants with Qi deficiency were chosen for inclusion in the studies conducted by Geng et al, 34 Wang et al, 35 and Lu et al. 38 The syndrome differentiation criteria for patients included in the RCTs were determined by the TCM practitioner’s judgment or in accordance with 'The Guiding Principles for Clinical Research of New TCM Drugs’. 39
The baseline characteristics of the studies are shown in Table 1. The main characteristics of each trial included in the meta-analysis are shown in Table 2.
Characteristics of the Included Studies.

Abbreviations: CT, chemotherapy; RTx, radiotherapy.
Details of the Included Studies.

The study reported the changes in BFI scores before and after treatment.
Abbreviations: BFI, Brief Fatigue Inventory; CFS, Cancer Fatigue Scale; CRF, Cancer-related Fatigue; KPS, Karnofsky Performance Scale; Min, minute(s); NR, Not Reported; PFS-R, Revised Piper Fatigue Scale; TCM, traditional Chinese medicine; TEC regimen, Paclitaxel-epirubicin-cyclophosphamide; UC, usual care; Wk, week(s).
Quality Assessment
Nine RCTs described the randomization method. Only one study reported that the randomization sequence generation was completed before participant recruitment. 29 Two RCTs implemented blinding of the participants and personnel,29,37 and one of them was a placebo-controlled trial. 29 One RCT reported that the outcome assessors and statisticians were blinded. 29 There were no missing findings in 8 RCTs,21,23 -29, one RCT clearly described the number of patients who dropped out and their reasons for doing so (Figures 2 and 3).
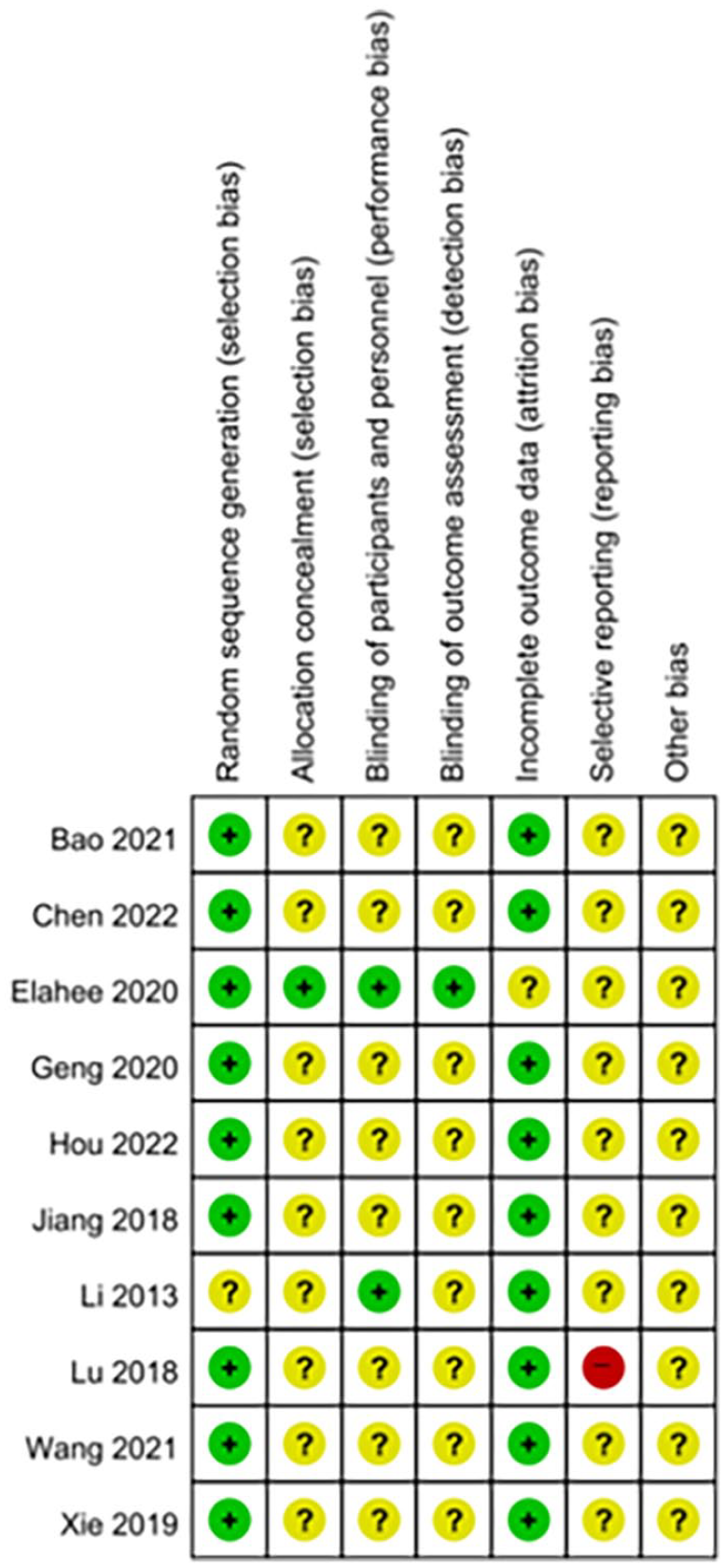
Risk of bias summary.

Risk of bias graph.
Main Results
Revised Piper Fatigue Scale
Three RCTs utilized the revised Piper Fatigue Scale (PFS-R). The results indicated a statistically significant difference between the moxibustion groups and control groups (3 studies involving 190 patients; WMD = −1.20; 95% CI −1.79 to −0.60; P < 0.0001) using a random-effects model (chi2 = 5.68, P = 0.06, I2 = 65%) (Figure 4).

Comparison of revised Piper Fatigue Scale between the moxibustion group and control group.
Cancer Fatigue Scale
The Cancer Fatigue Scale was evaluated in 2 RCTs. A meta-analysis of these studies revealed no statistically significant differences between the moxibustion groups and control groups (2 studies involving 130 patients; WMD = −2.56; 95% CI −5.25 to 0.14; P =0.06) using a random-effects model (chi2 = 57.30, P <0.0001, I2 = 98%) (Figure 5).

Comparison of Cancer Fatigue Scale between the moxibustion group and control group.
Karnofsky Performance Scale
In 4 RCTs that examined the effects of moxibustion therapy using the Karnofsky Performance Scale (KPS), the results demonstrated a significant difference between the moxibustion groups and control groups (4 studies involving 348 patients; WMD = 12.16; 95% CI 9.50-14.82; P < 0.0001) using a random-effects model (chi2 = 19.26; P = 0.0002; I2 = 84%) (Figure 6).

Comparison of Karnofsky Performance Scale between the moxibustion group and control group.
Athens Insomnia Scale
Two RCTs utilized the Athens Insomnia Scale. A meta-analysis showed that the difference between the moxibustion groups and control groups was not statistically significant (2 studies involving 114 patients; WMD = −13.70; 95% CI −36.41 to 9.02; P = 0.24) using a random-effects model (chi2 = 154.83; P < 0.0001; I2 = 99%) (Figure 7).

Comparison of Athens Insomnia Scale score between the moxibustion group and control group.
Clinical efficacy
Five studies reported the clinical efficacy. Clinical efficacy was judged using the following formula: (pretreatment TCM syndrome score − post-treatment TCM syndrome score) / pretreatment TCM syndrome score × 100. A significant effect was defined as a therapeutic effect index of ≥70%, improvement as a therapeutic effect index of 30% to <70%, and an invalid result as a therapeutic effect index of <30%. The percentage of patients exhibiting a significant effect and improvement corresponded to the clinical efficacy.
The meta-analysis demonstrated a statistically significant difference between the moxibustion groups and control groups (5 studies involving 294 patients; RR = 2.66; 95% CI 1.51-4.68; P = 0.0007) using a random-effects model (chi2 = 22.96; P = 0.0001; I2 = 83%) (Figure 8).

Comparison of clinical efficacy between the moxibustion group and control group.
Qi deficiency syndrome scale
Three RCTs utilized the Qi deficiency syndrome scale, but one study did not provide accurate Qi deficiency syndrome scale scores. 38 The assessment criteria for Qi deficiency syndrome were divided into 4 stages based on the severity of symptoms such as shortness of breath, fatigue, weakness, cold sweat, and sluggish speech, and each stage was assigned 0 to 3 points. Higher scores indicated more severe Qi deficiency symptoms.
The findings demonstrated a statistically significant difference between the moxibustion groups and control groups (2 studies involving 214 patients; WMD = 12.97; 95% CI 7.33-18.60; P < 0.0001) using a random-effects model (chi2 = 106.87; P < 0.0001; I2 = 98%) (Figure 9).

Comparison of Qi deficiency syndrome scale between the moxibustion group and control group.
Adverse events
The moxibustion treatments were well tolerated, and no serious adverse events were reported. Of the 10 RCTs, 2 provided detailed descriptions of adverse events,29,35 4 reported no serious adverse events,30,31,33,34, 4 did not mention any adverse events.32,36 -38
Discussion
Several recent meta-analytic studies have explored the use of moxibustion in treating cancer-related fatigue (CRF). Deng et al published a systematic review and meta-analysis protocol examining the therapeutic effects and safety of moxibustion for cancer-related fatigue. 40 Wang et al conducted meta-analysis involving 24 RCTs with 1894 participants. The aggregated standardized mean difference (SMD) indicated a statistically significant association between moxibustion and alleviation of cancer-related fatigue. 41 Our study incorporates additional RCTs not covered in their research, and we have specifically narrowed inclusion criteria to focus on breast cancer patients. Additionally, unlike the aforementioned studies, we utilized databases from Korea and Japan, in addition to English and Chinese databases.
This meta-analysis of 10 RCTs showed that the moxibustion groups had lower PFS-R scores, lower Qi deficiency syndrome scale scores, greater clinical efficacy, and higher KPS scores than those of the control groups. These results suggest that moxibustion is effective in improving fatigue and quality of life in patients with breast cancer.
While KPS and the insomnia scale are not direct measures of cancer-related fatigue, we included them in our analysis as they are often associated with fatigue and can serve as relevant indicators of the overall well-being and sleep quality of breast cancer patients. The KPS served as an observer-rated assessment of functional capacity, and it has been widely employed in research focused on cancer patients.42,43 Higher scores on the fatigue measures were correlated with lower KPS. 44 Studies suggest a reciprocal and close association between fatigue and insomnia.45 -47 In cancer patients, insomnia emerges as a significant predictor of intense fatigue, thereby escalating the likelihood of persistent fatigue. Simultaneously, fatigue amplifies disruptions in sleep and contributes to psychological distress among patients with insomnia.48 -54
Breast cancer not only ranks as the most frequently diagnosed cancer in women but also stands as the primary cause of cancer-related fatalities among them. 55 Breast cancer treatment commonly includes various combinations of surgery, radiation therapy, chemotherapy, and hormone therapy. 56 As used in the study conducted by Hou et al, 32 paclitaxel is commonly employed as the initial treatment medication for breast cancer. 57 Paclitaxel, belonging to the taxanes class, is an antineoplastic medication known for its ability to stabilize microtubules. 58 The suggested protocol involves administering paclitaxel injection intravenously at a dosage of 175 mg/m² over a period of 3 hours every 3 weeks. 59 It has been noted that TAC chemotherapy, comprising paclitaxel/docetaxel, cyclophosphamide, and doxorubicin, is associated with potential enhancements in the overall survival of breast cancer patients. However, this regimen is also linked to an elevated toxicity profile. 60 The TEC chemotherapy regimen, as utilized in the study conducted by Jiang and Xiao 33 employing cyclophosphamide, paclitaxel/docetaxel, and epirubicin, could potentially yield therapeutic effects similar to those of the TAC regimen. Moreover, it offers the advantage of potentially lower toxicity levels compared to TAC chemotherapy. 61 The TEC chemotherapy regimen is typically administered to breast cancer patients at the following dosages and intervals. TEC regimen: epirubicin 60 to 75 mg/m2 d1, cyclophosphamide 500 mg/m2 d1, docetaxel 75 mg/m2 d1, every 3 weeks.62,63
CRF is reportedly associated with the production of cytokines or inflammatory mediators secondary to cancer and/or cancer treatment. 64 In addition to inflammation,65,66 various factors have been implicated in CRF, including oxidative stress, 67 dysregulation of the hypothalamic–pituitary–adrenal axis, autonomic nervous system disorders (eg, central vagal stimulation), serotonin dysregulation,65,66 and alterations in muscle 66 and adenosine triphosphate metabolism.65,66 Despite these findings, however, the exact mechanism underlying CRF remains incompletely understood. 68
Inflammation seems to play a key role in the fatigue that develops before, during, and after cancer treatment. 65 Tumors and their treatments can activate the inflammatory cytokine network, causing fatigue symptoms through signaling in the central nervous system.69,70 Research on breast cancer patients prior to undergoing radiotherapy or chemotherapy has shown a correlation between fatigue and an elevated level of C-reactive protein (CRP).71,72 Both radiotherapy and chemotherapy increase the prevalence of fatigue and levels of proinflammatory cytokines such as interleukin (IL)-6, IL-10, and soluble tumor necrosis factor (TNF) receptors.73 -77 In a study involving patients undergoing radiotherapy for early-stage breast or prostate cancer, higher levels of CRP and IL-1 receptor antagonist were associated with increased fatigue. 77 Another study of breast cancer survivors experiencing persistent post-treatment fatigue revealed elevated levels of IL-1 receptor antagonist, soluble TNF receptor, neopterin, soluble IL-6 receptor,78,79 and lipopolysaccharide-stimulated cytokine production.79,80 Additionally, 200 breast cancer survivors who developed CRF between 3 and 48 months after cancer treatment exhibited elevated levels of CRP. 81
According to TCM theory, disease progression can result in a Yin and Yang imbalance, subsequently leading to a decline in Essence qi. 82 Yang-Qi deficiency refers to an inadequacy of the qi, presenting with symptoms such as easy fatigue, low energy, reduced appetite, poor circulation, and, in some cases, cold symptoms. 83 Both Qi-deficiency and Yang-deficiency are separately linked to an elevated risk of experiencing moderate-to-severe CRF in cancer patients. 84 The presence of Yang-Qi deficiency plays a role in the onset of fatigue among patients with breast cancer.85,86 The connection between fatigue and Yang-Qi deficiency in cancer patients may be associated with disturbances in mitochondrial metabolic activity. 87
Recent studies have demonstrated the effectiveness of moxibustion in relieving chronic fatigue.88 -90 The mechanism underlying this therapeutic effect has been related to several factors, including improved inflammation, 91 activation of the vagus nerve, 89 and reduced oxidative damage.88,89,92
Moxibustion can attenuate the inflammatory impairment in patients with exercise-induced fatigue, which might be mediated by inhibition of the proinflammatory cytokine IL-6 in the hippocampus, as shown in a rat model. 93 Moxibustion has been clearly shown to modulate immune function in various types of illnesses.94 -97 Moxibustion can regulate the serum TNF-α level 95 and Th1/Th2 cytokine imbalance 96 ; it can also reduce the serum levels of IL-1β and interferon-γ and the interferon-γ/IL-4 ratio. 97
This study has some limitations. First, all RCTs were conducted in China. Despite conducting the search without any geographical limitations, only RCTs conducted in one country were included. Because all the trials were conducted in China, it may be difficult to generalize the results to other populations. Second, there was an insufficient number of RCTs, and all of the studies had relatively small sample sizes. The meta-analysis results indicate significant heterogeneity, as evidenced by a substantial I2 value. Third, most of the trials included in this review were considered to have significant methodological flaws and a high risk of bias; none of the trials had a low risk of bias in every domain. Only 1 of the 10 RCTs was placebo-controlled. 29 Consequently, the findings of this study should be interpreted with caution because these limitations have the potential to impact the reliability of the evidence.
Conclusions
This study showed that moxibustion improved CRF and quality of life in patients with breast cancer. The meta-analysis of 10 RCTs demonstrated that moxibustion decreased the PFS-R score, decreased the Qi deficiency syndrome scale score, improved the clinical efficacy, and increased the KPS score. No serious adverse events were reported in any of the RCTs. Moxibustion can be considered as a treatment option for CRF in patients with breast cancer. The efficacy of moxibustion in patients with breast cancer who develop CRF should be thoroughly examined via well-designed studies that include patients from different countries.
Footnotes
Data Availability
The data used to support the findings of this study are included in the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the National Research Foundation of Korea (NRF) (No. RS-2023-00246351).
Ethical Statement
No ethical approval was required.