
Abstract
Background:
Radiation-induced xerostomia is one of the most common symptoms experienced by cancer patients. The aim of our study is to evaluate the preventive and therapeutic effect of acupuncture for radiation-induced xerostomia in cancer patients.
Methods:
Eight databases were searched for all published randomized clinical trials (RCTs) on acupuncture for radiation-induced xerostomia in cancer patients up to December 31, 2019. Manual searching included other conference abstracts and reference lists. Meta-analysis was conducted using Revman V.5.3, and risks of bias for included studies was assessed following the Cochrane Handbook.
Results:
Eight clinical trials (725 participants) were analyzed, and 3 were included in a meta-analysis. All included trials had a high risk of bias, such as selection, performance, and detection bias. Analysis indicated favorable effects of acupuncture regarding the improvement of xerostomia symptoms (MD −3.05, P = 0.02, 95% CI −5.58 to −0.52), compared with sham acupuncture. There were no significant differences between real acupuncture and sham acupuncture regarding the stimulated salivary flow rate (MD 0.37, P = 0.08, 95% CI −0.05 to 0.79) and unstimulated salivary flow rate (MD 0.09, P = 0.12, 95% CI −0.02 to 0.21), which were whole salivary flow rate. Compared with no acupuncture (standard oral care, usual care, or no treatment), acupuncture produced a significant improvement in patient-reported xerostomia, without causing serious adverse effects. However, a Grading of Recommended Assessments analysis revealed that the quality of all acupuncture outcome measures was low.
Conclusion:
The present meta-analysis and systematic review suggests that acupuncture is effective at improving xerostomia symptoms in cancer patients but not at objective salivary flow measurements. The evidence is still limited due to the low quality of the published studies.
Introduction
Xerostomia is associated with reduced salivation that causes a subjective sensation of a dry mouth, and is one of the most common symptoms experienced by patients with cancer.1-4 Cancer treatments often adversely affect the quantity and quality of saliva. Patients may show clinical signs of dry mouth, such as hypofunction of the salivary glands (SGs) or hyposalivation, or symptoms of dry mouth (xerostomia). The decline in SG function is most severe after radiation therapy of the head and neck.5-10 Patients with cancer report varying degrees of dry mouth, reduced diet, and somnipathy, 11 and are at higher risk of developing dental complications, dysgeusia, dysphagia, odynophagia, difficulty sleeping and speaking, and oral ulcers, which may seriously decrease quality of life. 12 Xerostomia may also lead to decreased patient compliance and impact treatment, which can lead to inadequate tumor control 13 ; therefore, it is important to initiate effective xerostomia treatment. Several methods are available for the management of xerostomia, including stringent oral hygiene, fluoride agents, antimicrobials, saliva substitutes, and sialagogic agents that increase salivary secretion14-32; however, these treatments achieve limited effects23-32 and often induce adverse effects such as headache, dizziness, and sweating.19-21 Amifostine has been approved by the Food and Drug Administration to reduce the incidence and severity of radiation-induced xerostomia, but it requires parenteral administration, has potential adverse effects, and is not universally available. 33 There is also some low-level evidence that saliva substitutes and stimulants are beneficial for cancer-induced xerostomia. 34
Acupuncture comprises the needling of specific points of the body, and is one of the most widely used complementary therapies in many countries as a valid palliative intervention modality.35,36 In 2003, the World Health Organization published a report on the efficacy of acupuncture in the cure or relief of 64 different symptoms, including xerostomia. 37
There are several hypotheses regarding the mechanism by which acupuncture may increase saliva secretion. Acupuncture stimulates the parasympathetic and sympathetic nervous systems through neuronal activation,38-41 and causes the release of neuropeptides, such as vasoactive intestinal peptide and calcitonin gene-related peptide.40,41 These neuropeptides have anti-inflammatory properties and nutritional effects on the SGs, and increase the blood flow in the acini. Acupuncture also directly affects the local blood flow near the SGs, thereby increasing the secretion of saliva. 42 Finally, acupuncture therapy may tap into the neuronal circuit that activates the salivary nuclei in the pons and subsequently the SGs via the cranial nerves. 38
Some studies have explored the effect of acupuncture on xerostomia and showed that it can effectively treat or prevent dry mouth,43-56 and xerostomia is most common in cancer patients who were undergoing radiation therapy. However, high quality trials investigating efficacy and safety of acupuncture for radiation-induced xerostomia was limited. And 4 new trials have been published since the publication of previous systematic reviews of acupuncture for radiation-induced xerostomia in patients with head and neck cancer.57,58 Therefore, the present study aimed to update the evidence base by including the many clinical trials published during the past 10 years. A comprehensive review of acupuncture treatment of radiation-induced xerostomia in cancer patients might be beneficial to patients, practitioners, and healthcare policy-makers. The present systematic review and meta-analysis aimed to evaluate all of the currently available studies of acupuncture as a treatment or prevention for radiation-induced xerostomia in cancer patients.
Methods
Protocol and Registration
This systematic review was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. 59 The peer-reviewed protocol of this systematic review and meta-analysis was published in PROSPERO (registration no. CRD42019129069). 60
Search Method
Two authors independently performed a systematic literature search of the following databases: PubMed, MEDLINE, Cochrane Library, Embase, China National Knowledge Infrastructure, Chongqing VIP Chinese Science and Technology Periodical Database, Wanfang Database, and China Biology Medicine Disc. The search strategy consisted of 3 components: clinical condition (cancer, tumor/tumour, carcinoma, neoplasm AND xerostomia), intervention (manual acupuncture, electroacupuncture, body or auricular acupuncture), and study type (randomized clinical trial). The databases were searched from inception to December 31, 2019. The Pubmed search strategy is shown in Table 1; this strategy was modified appropriately for other databases. The authors also searched the Index to Scientific & Technical Proceedings (Web of Science) and the reference lists of relevant primary and review articles to identify cited articles not detected in electronic searches.
Search Strategy for the PubMed Database.

Abbreviations: ti, ab, title/abstract; pt, article type.
There is no limit to the number of matches.
Study Selection
The abstracts of all identified articles were carefully and independently reviewed for eligibility by 2 investigators. The inclusion criteria were: (1) randomized controlled trials (RCTs) (parallel and/or crossover studies); (2) studies of cancer patients with symptoms of dry mouth caused by radiotherapy or studies that recruited patients with cancer who will be going radiotherapy; (3) studies with adult patients (≥18 years of age); (4) studies using invasive acupuncture as an experimental intervention, such as body acupuncture, manual acupuncture, and electroacupuncture; (5) studies with a control group that included patients treated with control interventions such as placebo acupuncture, sham acupuncture (SA), Chinese herbs, Western medicine, no treatment (waiting list control), routine care, or conventional therapy; (6) studies using one or more of the following measurements: (a) objective methods, such as stimulated salivary flow rate (SSFR), unstimulated salivary flow rate (USSFR), saliva collection, whole saliva production, or scintigraphy or functional magnetic resonance imaging of the SGs; (b) subjective measurements comprising observer-based toxicity grading or patient self-reported scoring, such as the visual analogue scale, the Xerostomia Questionnaire (XQ), or quality of life scoring 61 ; (7) studies published in English or Chinese. The exclusion criteria were: (1) non-RCTs, quasi-RCTs, case series, review articles, meta-analyses; (2) animal studies; (3) mixed interventions (eg, acupuncture in combination with other therapies) when manual acupuncture or electroacupuncture was not considered the main intervention. If the 2 investigators disagreed about the eligibility of an article, the disagreement was resolved by consensus with a third reviewer.
Data Extraction
Two investigators independently extracted data from the included studies and entered this information into a unified data statistics table. The extracted data included the reference ID, first author’s name, publication year, type of cancer, patient age, type of acupuncture intervention, type of control intervention, sample size of each intervention group, intervention duration, randomization, allocation concealment and blinding methods, outcome measures, primary outcomes and adverse events, duration of follow-up, type and source of financial support, and adherence to the Standards for Reporting Interventions in Controlled Trials of Acupuncture. 62 Any disagreements were solved by consensus. A third investigator made the final judgment when consensus on data extraction could not be obtained through negotiation. Data tables were compared and discussed with a third review author. If a study was missing information, the corresponding author was contacted (if the contact details were available). The methodological quality of included RCTs was assessed in accordance with the Cochrane Collaboration’s tool described in the Cochrane Handbook version 5.1.0. 63 If more than 10 trials were included in the meta-analysis, a funnel plot was used to assess the reporting biases. Begg and Egger tests were used to evaluate the asymmetry of the funnel plots, and values of P < .05 were considered to represent significant publication bias. 64
Statistical Analysis
Data analysis was performed using RevMan software (version 5.3). The effect size was calculated for each study and combined to generate an overall effect size. For categorical variables, the risk ratio or odds ratio and 95% confidence interval (95% CI) were used. For continuous variables, the weighted mean difference (MD) or standard MD and 95% CI were used. A random-effects or fixed-effects model was used for the meta-analysis. In accordance with the Cochrane Handbook for Systematic Reviews of Interventions, heterogeneity was assessed by a visual check of the forest plot, a heterogeneity χ2 test, and the Higgins’ I2 statistic. 65 If the P value was >.10 and the I2 value was <50%, a fixed-effects model was used to pool the data; otherwise, a random-effects model was used. If there was significant heterogeneity between a set of studies, causes of heterogeneity such as patient characteristics and degree of variation in interventions were explored. Sensitivity analysis or subgroup analysis was used to evaluate heterogeneity if applicable. The Grading of Recommendations Assessment (GRADE) approach was used to describe the quality of the evidence for the results obtained. 66
Results
Study Selection
The initial database searches identified 94 potentially relevant articles. A total of 26 duplicates were excluded, and a further 52 articles were removed based on the title and abstract screening process. The full-text versions of the remaining 16 studies were reviewed, and 8 more studies were excluded in accordance with the eligibility criteria (Figure 1). Eventually, 8 studies49,67-73 were included in the qualitative synthesis, while 3 studies67,68,73 were included in the meta-analysis.

Flow diagram of the trial selection process.
Study Characteristics
The study characteristics of the included RCTs are summarized in Table 2. The selection criteria were met by 8 RCTs with 725 participants in total, comprising 304 patients in the acupuncture group and 421 patients in the control group. Three of the included RCTs were conducted in China,71-73 2 was conducted in the United States,69,73 and 1 was conducted in each of Sweden, 67 South Korea, 68 Brazil, 49 and England. 70 Seven studies were 2-armed, while 1 was 3-armed. 73 Seven trials used parallel group designs, while 1 was a cross-over study. 70 Three articles aimed to explore the preventive effect,49,71,72 the rest to explore the therapeutic effect of acupuncture on radiation-induced xerostomia in cancer patients.67-70,73
Study Characteristics.

Abbreviations: RCT, randomized clinical trials; TG, treatment group; CG, control group; SSFR, stimulated salivary flow rate; USSFR, unstimulated salivary flow rate; XQ, Xerostomia Questionnaire; XI, Xerostomia Inventory; RSFR, resting salivary flow rate.
Condition characteristics
All 8 trials included patients diagnosed with tumors in the head and neck region with a history of radiotherapy. None of the included RCTs specifically identified the types of cancer; therefore, there were no specific diagnostic criteria.
Patient characteristics
The average age of patients was 54.15 years (median 55.12; interquartile range (IQR) 46.53-59.4). The proportion of females ranged from 4.76% to 34.48% (median 26.95; IQR 16.67-31.58).
Intervention characteristics
The treatment groups in 7 trials received body acupuncture plus ear acupuncture, while 1 trial used body acupuncture alone. 68 The number of treatment sessions ranged from 4 to 24 (median 18; IQR 8-20); the frequency of treatment ranged from 1 to 3 times per week (median 2; IQR 1-3). The treatment period ranged from 4 to 14 weeks (median 7; IQR 6-8). The duration of each acupuncture session ranged from 20 to 30 minutes (median 20; IQR 20-20). The duration of the follow-up period ranged from 4 to 52 weeks in 6 studies, while 2 RCTs did not perform any follow-up.49,68 The number of needle insertions ranged from 4 to 24 (median 19.5; IQR 8-24). The number of acupoints ranged from 2 to 15 (median 3.5; IQR 3-5).
Control characteristics
The most commonly used control intervention was SA comprising either needle puncture at sham locations (eg, sham points, pseudo points, inactive points) or sham insertions (eg, superficial insertion, pseudo insertion, or electroacupuncture without electric stimulation). 74 The control intervention was SA in 4 trials,67,68,72,73 standard oral care in 3 trials,70,71,73 usual care (entailing no specific treatment, physical therapy, analgesia, and/or anti-inflammatory drugs) in 1 trial, 69 and no treatment in 1 trial. 49
Outcomes
Most studies used the XQ as a subjective outcome to assess the effect of acupuncture,49,68,71-73 while the objective outcomes included the SSFR and USSFR.49,67-69,71,72 Other outcomes included the Modified Constant-Murley score and Xerostomia Inventory in 1 trial, 69 the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire in 1 trial, 70 and the incidence of clinically significant xerostomia (score >30), salivary flow, quality of life, and salivary constituents in 1 trial. 73
Risk of Bias
Figure 2 shows the risk of bias in each of the 6 domains for all included studies. Most included studies were classified as having a high risk of bias. Most studies explicitly reported the randomization method, while 2 study failed to provide a detailed description of the randomization process.49,67 Only 1 trial provided information about allocation concealment via the use of sealed envelopes or by computer. 69 Due to the special nature of acupuncture, there was no blinding of the acupuncturists in all trials. There was no blinding of the participants in 5 trials,49,67,69-71 while the other 3 were single-blind.68,72,73 In 6 studies,49,67,68,70-72 the outcome assessors were not blinded, suggesting a risk of measurement bias. In addition, only 1 RCT reported the number of dropouts, 71 but did not mention the reasons. All studies had comparable baseline characteristic data. A summary of the risk of bias in each of the included trials is presented in Figure 3.

Risk of bias graph: review authors’ judgments about each risk of bias item presented as percentages across all included studies.

Risk of bias summary: review authors’ judgments about each risk of bias item for each included. +, low risk of bias; ?, high risk of bias; −, unclear risk of bias.
Results of Individual Studies
Acupuncture Versus Sham Acupuncture
Four RCTs used SA as a control treatment; 2 used superficial needling at nonacupoints,67,68 1 used nonpenetrating needling at nonacupoints, 72 and 1 used a mixture of real needling at a real acupoint not indicated for xerostomia, real needling at sham points, and placebo needling at sham points. 73 Three RCTs reported significantly increased salivary flow rates after treatment in all groups, although the changes in the SA group were smaller and appeared after a longer latency phase compared with the real acupuncture (RA) group, 67 and RA improved the XQ score for dry mouth.68,72 However, one study found no differences between the RA and SA groups in the USSFR and SSFR. 72 One study reported that the XQ scores of the RA group were marginally lower but not significantly different from those of the SA group, and that the incidence of clinically significant xerostomia at 1 year after radiation therapy ended was significantly different in the RA group versus the SA group only at one of the participating research centers. 73
Acupuncture versus no acupuncture
Three studies used standard oral care as a control intervention.70,71,73 One study showed that compared with oral care, acupuncture produced significant reductions in patient-reported severe dry mouth, while there were no significant changes in the SSFR and USSFR over time. 70 Two studies reported that the XQ scores of the acupuncture group were significantly lower than those of the control group,71,73 and found a significant difference between the acupuncture and standard oral care groups in the incidence of clinically significant xerostomia at 1 year after radiation therapy ended. 73 One trial reported that acupuncture produced greater improvement in patient-reported xerostomia compared with usual care (entailing no specific treatment, physical therapy, analgesia, and/or anti-inflammatory drugs). 69 One study showed that acupuncture treatment significantly minimized the severity of radiation-induced xerostomia compared with no treatment. 49
Safety
Six of the included RCTs assessed the adverse effects, while 2 did not.68,71 No serious adverse events were attributed to acupuncture, although somnolence, tiredness, tiny hemorrhages, and minor bruising or bleeding at the puncture site were reported. One trial reported that 2 patients were treated for coronary syndrome during the 8-week acupuncture treatment period 70 ; however, both of these patients had multiple risk factors for cardiac disease, and therefore the events were unlikely to be related to the acupuncture treatment. During the oral care intervention period, 1 patient suffered a traumatic hip fracture, while another was hospitalized for aspiration pneumonia. 70 One RCT reported no adverse event. 72
Meta-Analysis
Acupuncture Versus Sham Acupuncture
Xerostomia Questionnaire
Three studies used the XQ as an outcome to measure the effect of acupuncture on radiation-induced xerostomia in cancer patients, but only 2 of these studies contained adequate data for inclusion in the present meta-analysis.68,73 Meta-analysis showed no heterogeneity between these 2 trials (I2 = 0%, P = .34), and so a fixed-effects model was used (Figure 4). RA had favorable effects on the improvement of xerostomia symptoms compared with SA (n = 254, MD = −3.05, P = .02, 95% CI −5.58 to −0.52).

Forest plot of the Xerostomia Questionnaire scores for real acupuncture versus sham acupuncture.
Stimulated salivary flow rate
Three studies evaluated the SSFR to measure the effect of acupuncture on radiation-induced xerostomia in cancer patients. Two of these studies contained adequate data for inclusion in the present meta-analysis.67,68 There was significant heterogeneity between the 2 studies (I2 = 60%, P = .11), and so a random-effects model was used (Figure 5). The SSFR did not significantly differ between the RA and SA groups (n = 50, MD = 0.37, P = .08, 95% CI −0.05 to 0.79).

Forest plot of the stimulated salivary flow rate results for real acupuncture versus sham acupuncture.
Unstimulated salivary flow rate
Three studies used the USSFR to assess the effectiveness of acupuncture in treating radiation-induced xerostomia in cancer patients. As the original data were not available for one of these studies, only the data from the other 2 studies were included in the present meta-analysis.67,68 There was significant heterogeneity between the 2 trials (I 2 = 64%, P = .10), and so a random-effects model was used. The USSFR was not improved in the RA group compared with the SA group (n = 50, MD = 0.09, P = .12, 95% CI −0.02 to 0.21) (Figure 6).

Forest plot of the unstimulated salivary flow rate results for real acupuncture versus sham acupuncture.
Discussion
Summary of the Main Results
The present systematic review included 8 studies involving 725 patients. Sample sizes ranged from 12 to 339 patients. The main findings were that there was no significant difference between RA and SA for treating radiation-induced xerostomia in cancer patients in terms of the salivary flow rate, but RA showed better results in resolving the symptoms of dry mouth. Compared with no acupuncture (standard oral care, usual care, or no treatment), acupuncture produced a significant improvement in patient-reported xerostomia. There were no serious acupuncture-related adverse reactions in all groups, except for some normal phenomena such as bleeding or slight pain due to needling. However, the present meta-analysis findings were insufficient to support a clinical recommendation due to the generally low methodological quality of the included studies.
Possible Explanations for the Present Findings
Similar to previous reviews, the present review found limited evidence to suggest that acupuncture was beneficial for radiation-induced xerostomia in cancer patients, especially compared with SA. Three factors might explain these findings. First, SA might have direct physiological effects on the mechanisms associated with dry mouth symptoms. Second, a placebo effect may occur in the SA group due to patient expectations, conditioning, anxiety reduction, and social support.75,76 Third, acupuncture itself might be a particularly effective placebo.
Quality of Evidence
The Cochrane Collaboration Network GRADE approach was used to perform a systematic review of the results (Figure 7). The systematic analysis comprised 3 outcomes in the acupuncture group and the SA group. Relief of the symptom of dry mouth was the key outcome, while the SSFR and USSFR were important secondary outcomes. The GRADE profile indicated that the quality of evidence was low for all outcomes, mainly due to methodological limitations, unexplained inconsistencies, and variations in sample sizes.
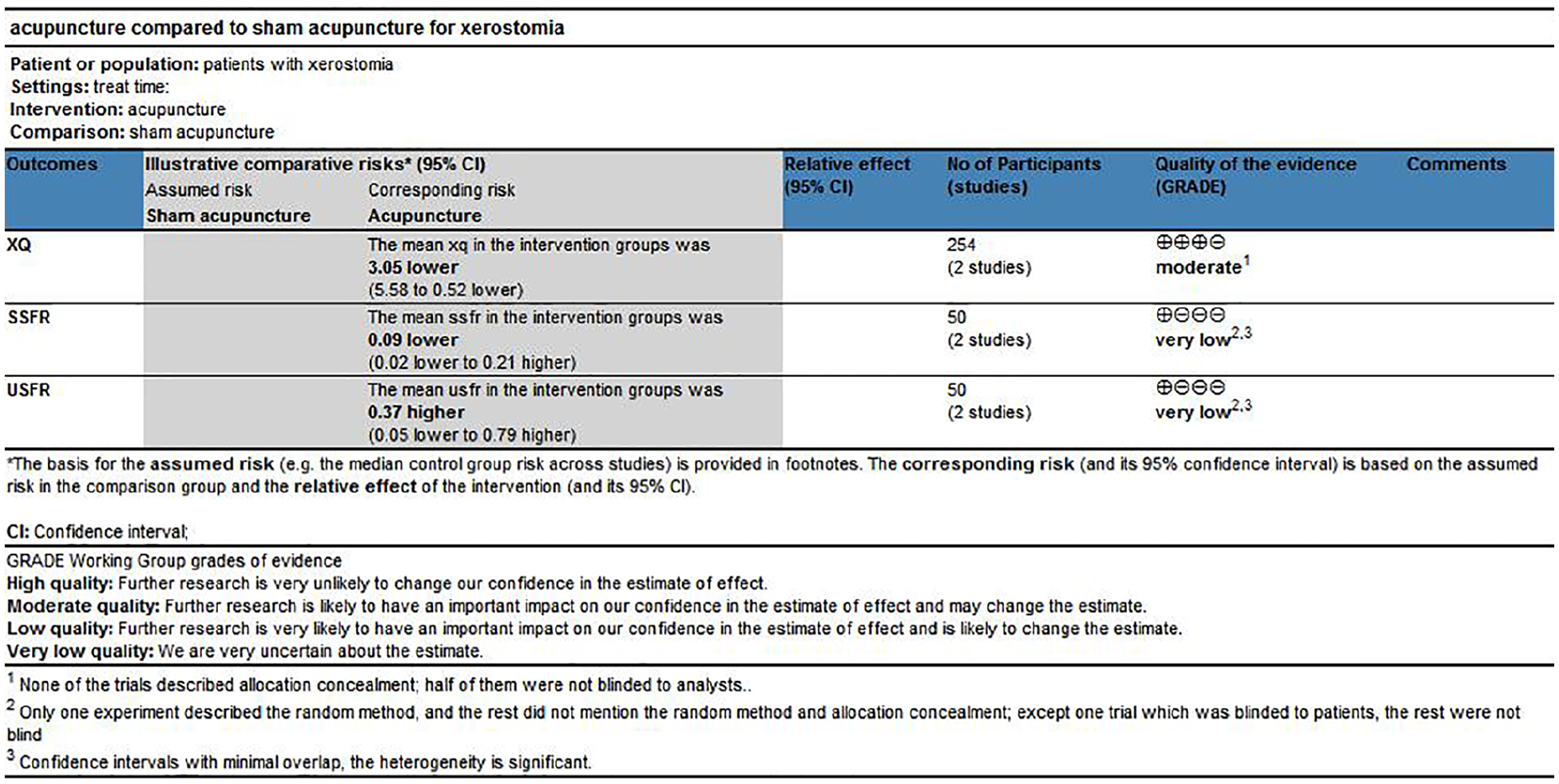
Grading of recommendations assessment of evidence regarding the effects of acupuncture for cancer-induced xerostomia.
Limitations of Included Studies
Methodological quality
The methodological quality of the included trials was low, especially regarding allocation concealment and blinding. Of the 8 included RCTs, 2 did not describe the randomization process in detail.49,67 In addition, only 1 RCT provided information about allocation concealment. 69 Patients were blinded to treatment allocation in only 3 RCTs,68,72,73 and were blinded to the outcome assessment in 2 RCTs.69,73 In addition, no descriptions could be used to determine whether the included studies had selective reporting bias. These different types of bias may have led to false positive results. Furthermore, only 2 RCTs reported the methods used to calculate the sample sizes,71,73 and so the included RCTs might have extremely low statistical analysis power.
Inconsistent interventions
The 8 included RCTs used different experimental groups, such as RA versus SA, and acupuncture versus standard oral care control, usual care, and no treatment. The included RCTs also differed regarding the frequency, number of sessions, and duration of acupuncture, the selection and number of acupoints, needling depth, acupuncture process, and needle retention time; all of which might have caused bias. There is often a lack of standardization and transparency in complementary and alternative medicine research. This problem is difficult to solve because there is no “gold standard” for acupuncture in treating dry mouth. In fact, as traditional Chinese acupuncture and complementary and alternative medicine does not advocate the use of a standardized, 1-size-fits-all acupuncture regimen, 77 personalized treatment for each person is considered an important part of care. Skilled practitioners may therefore consider the use of any single “gold standard” acupuncture regimen to be restrictive and counterproductive.
Limited outcomes
The subjective outcome measures used in most of the included trials were not uniform, and studies that used the same indicators also used different individualized scales. In addition, a meta-analysis using a subjective outcome measure such as the XQ yielded positive results for treatment, while a meta-analysis using an objective outcome measure such as the salivary flow rate yielded no significant difference between treatment and control interventions. Thus, future studies should consider using more objective outcome indicators to evaluate the effect of acupuncture on dry mouth.
Lack of economic data
No economic data or relative economic analysis has been reported.
Limitations of the Current Study
Although a considerable amount of effort was spent in retrieving RCTs and evaluating data quality, and the GRADE framework was applied to assess the quality of evidence for certain outcomes, the current study still had several limitations. (1) The literature search was limited to articles published in Chinese or English, which excluded studies published in other languages (such as Japanese, Korean, and German). This language limitation may have induced biased outcomes. (2) The risk of assessment bias varied between studies based on the study authors’ subjective views and diligence. (3) The total sample size was small (n = 725), as few RCTs have investigated the effect of acupuncture on radiation-induced xerostomia in cancer patients. (4) A Funnel plot was not generated for the outcomes due to the limited number of included RCTs. Therefore, publication bias might exist. (5) The quality of the evidence was poor due to the limited number of included trials and the imperfect study design.
Comparison With Other Reviews
Two systematic reviews that included a small number of studies have evaluated the effects of acupuncture for radiation-induced xerostomia in patients with head and neck cancer.57,58 They concluded that there was not enough evidence to judge whether acupuncture was safe and whether it was effective in preventing or treating radiation-induced xerostomia. We identified 4 new RCTs and updated the evidence. Although the evidence for the effectiveness of acupuncture for radiation-induced xerostomia in cancer patients was still limited, the present meta-analysis of relevant outcome indicators concluded that acupuncture alleviates patient-reported subjective symptoms of dry mouth. The present review used the GRADE framework to assess the quality of evidence for certain outcomes.
Suggestions for Trials
As the quality and quantity of literature concerning the efficacy of acupuncture for cancer-induced xerostomia are limited, a potentially beneficial effect might exist, and future rigorous RCTs with appropriate controls should be conducted. Clinical trials should be registered in the World Health Organization International Clinical Registry Platform or Clinical Trials.gov, and reported in detail in accordance with the Consolidated Standards for Reporting of Trials 78 or Standards for Reporting Interventions in Controlled Trials of Acupuncture 62 guidelines. Randomization, allocation concealment, and blinding should be designed and rigorously conducted, and the duration of follow-up should be based on the research objectives. Furthermore, in addition to patient-reported subjective symptom relief, future clinical trials should introduce more objective outcome indicators. Finally, more attention should be paid to the reporting of adverse events.
Conclusion
There was a lack of evidence for objective salivary flow of acupuncture on xerostomia according the present meta-analysis. Although acupuncture improves the symptoms of cancer-induced xerostomia, this intervention cannot be recommended due to the limited number of included RCTs and the low quality of evidence. Acupuncture cannot yet be recommended for radiation-induced xerostomia in cancer patients until more solid evidence is produced.
Footnotes
Acknowledgements
Thanks to all the participants and clinical researchers involved in the publications cited in this review. Thanks to all the peer reviewers who contributed to the continuous improvement of this article.
Author Contributions
XXN conceived and designed the article. XXN and TT searched the databases and screened the articles. XXN and DC extract information and analyzed the data. XXN and TT assess the quality of included literature. XL and FML made figures and tables. XXN analyzed the data. All the authors contributed to the composition of the manuscript. LZ and FRL monitor each procedure of the review and are responsible for the quality control. All authors read and approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The review is financially supported by the National Natural Science Foundation of China (Grant No. 81722050, 81973962) and Project of Science and Technology Department of Sichuan Province (Grant No. 20ZDYF1199). Funders and sponsors have no role in the design of this review.