
Abstract
Introduction
Neuropathic pain related to chemotherapy (chemotherapy-induced peripheral neuropathy [CIPN]) is a troubling problem in cancer treatment; an estimated 30% to 40% of patients have been treated with at least one of the offending agents. 1 Some cytostatic groups are especially involved, such as bortezomib, platinum drugs, taxanes, vinca alkaloids, and thalidomide.2,3 Each of these drugs induces CIPN, although through different mechanisms; for example, taxanes are tubulin inhibitors that damage neuronal axons, while platinum analogs accumulate in the cell bodies of sensory nerves and damage DNA. 4
The clinical characteristics of CIPN include paresthesia (tingling, burning sensation), hyperalgesia (sensitive to noxious stimulation), allodynia (pain induced by a normally innocuous stimulation), and decreased physical activity. 5 Some patients also experience motor symptoms, such as dropping items, splaying fingers, and inability to complete normal daily activities. 6 Some patients may even withdraw from chemotherapy or receive reduced doses, which in turn decreases the treatment efficacy. Accordingly, multi-integrated therapies are used in these populations, such as fish oil, 7 vitamin B, 8 glutamines,9,10 and acupuncture,11,12 all of which have been reported to show some benefit in reducing CIPN. Acupuncture, which has drawn researchers’ attention in recent years, is widely accepted for its noninvasiveness and safety. In Chinese medicine theory, acupuncture works by regulating the imbalance of meridians, promoting the Qi (energy) over our body; in western medicine, acupuncture has been shown to work by adjusting neurophysiologic and neurohormonal activitiy.13,14 Although the interpretation of how acupuncture works varies by cultural context, researchers agree on its potential to alleviate some symptoms that are hard to control with conventional treatment.
In fact, many integrative oncologists have adopted acupuncture as a complementary or alternative medicine. Furthermore, evidence-based research increasingly shows that acupuncture can relieve many uncontrollable symptoms, including cancer pain15,16 (noted as evidence level I), chemotherapy-related side effects,1,17,18 hot flush or arthralgia related to hormone therapy,19,20 and xerostomia relevant to radiotherapy.21,22 With regard to neuropathy, acupuncture has been widely used in diabetes-related neuropathy23,24 and carpal tunnel syndrome,25,26 as well as CIPN.
There are no large-scale studies or systematic reviews of the effectiveness of acupuncture in alleviating CIPN. To clarify this point, we conducted a systematic review and meta-analysis, providing more objective data for applying acupuncture to chemotherapy-related neuropathy in the future.
Methods
Data Sources and Searches
The conduct of this systematic review complied with the PRISMA Statement27,28 to ensure transparent and complete reporting. Seven databases were searched for relevant randomized controlled trials (RCTs), from their inception dates to August 2019: MEDLINE (through the Ovid interface, including epub ahead of print, in-process, and other non-indexed citations), Embase, Cochrane CENTRAL, Scopus, and World Health Organization International Clinical Trials Registry Platform (ICTRP), CNKI (China National Knowledge Infrastructure), and Wanfang Med Online. The reference lists of eligible articles were reviewed to identify additional studies for possible inclusion. We also established e-mail alerts to identify newly released studies from the different databases, which fell within the scope of our review.
The key concepts used in the search (neuropathy, chemotherapy, and acupuncture) included their synonyms (116 English free-text terms plus truncation symbols when appropriate, and 16 Chinese free-text terms) and controlled vocabulary (25 MeSH [medical subject headings] terms and 21 Emtree terms). We adopted highly sensitive search syntaxes to identifying RCTs. Appendix 1 (available online) shows the search strategy.
Eligibility Criteria
All eligible studies examined patients afflicted with CIPN and measured the severity of neuropathy and quality of life. Only studies that used a true needle or electroacupuncture were included; those which adopted transcutaneous electrical nerve stimulation or other acupoint stimulation such as laser acupuncture were excluded. To improve consistency, only studies that measured the Brief Pain Inventory–Short Form worst pain score (BPI-SF), the Functional Assessment of Cancer Therapy/Neurotoxicity (FACT-NXT) score,29,30 and nerve conduction velocity (NCV) were subjected to meta-analysis.
Study and Data Extraction
Searches of the 7 databases and additional sources led to the identification of 2405 potentially relevant articles, 2399 of which were ultimately excluded. The titles and abstracts that fulfilled the criteria of our study were independently read by 2 reviewers (Chien and Liu), and the full texts of articles that met these criteria were obtained. Final decisions on inclusion were made after examination of the full articles. In cases of duplicate publications, the most recent and complete versions were selected. Among the excluded records, 611 articles were excluded because of duplication, 1726 titles/abstracts were irrelevant, and 62 full texts were non-RCTs, non-English/Chinese, clinical trials in progress, reported a duplicate population, were conference abstracts or had no matched coverage or were clinical registers that did not provide enough information for analysis, or theses. We also contacted some authors to ensure that studies that had appeared only as abstracts at conferences could be included if completed data were available. The study selection flowchart is shown in Figure 1. Six RCTs were included: Molassiotis et al, 31 Greenlee et al, 32 Han et al, 33 Zhang et al, 34 Lu et al, 35 and Rostock et al 36 ; 5 of these were included in the meta-analysis. The characteristic and results of the included RCTs are presented in Table 1. We further gathered 4 additional pilot studies for reference: Hsieh et al, 37 Bao et al, 38 Garcia et al, 39 and Schroeder et al 40 (Table 2).

Studies selection flowchart, which is based on the PRISMA Statement. 28
The Characteristics of the Included RCTs.
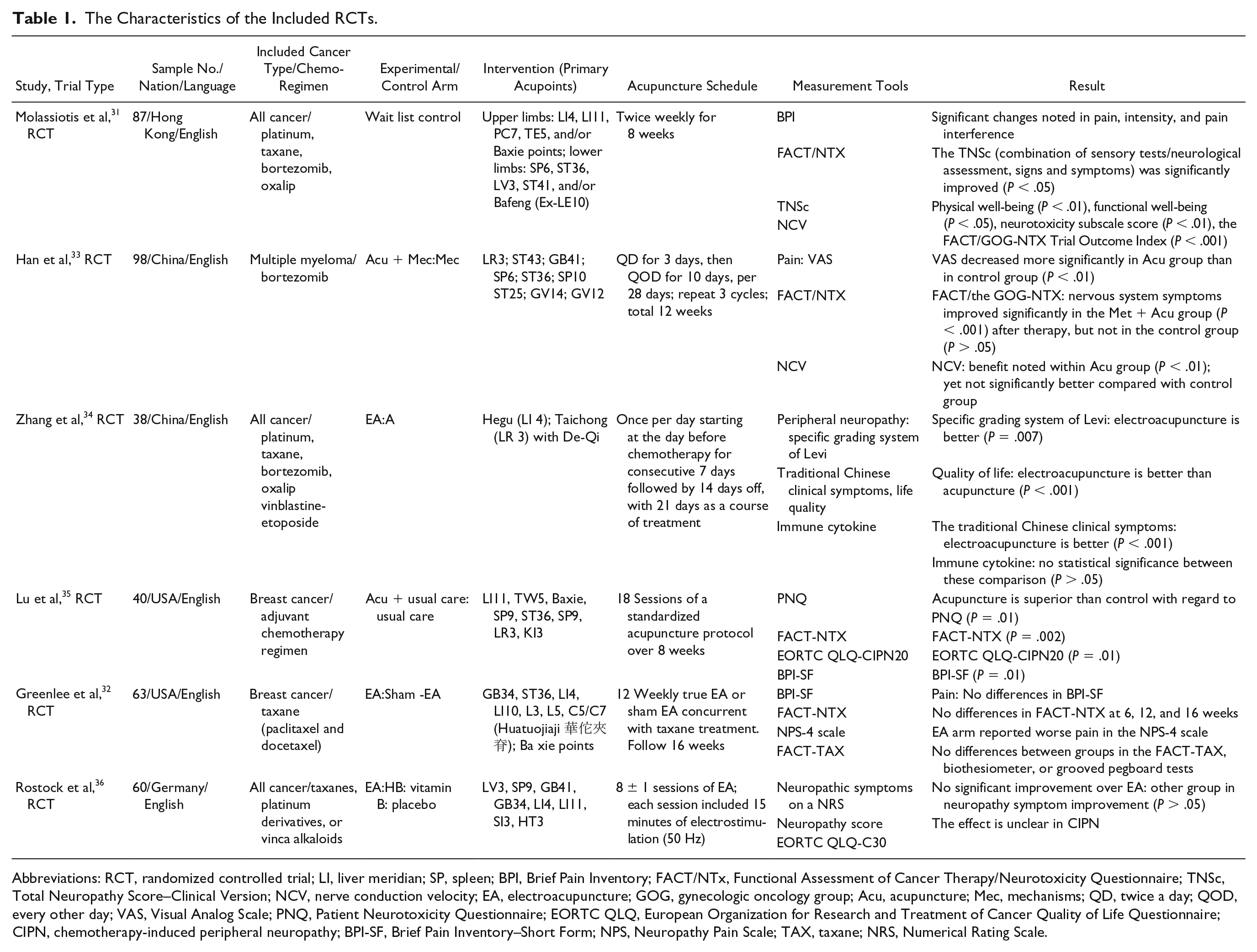
Abbreviations: RCT, randomized controlled trial; LI, liver meridian; SP, spleen; BPI, Brief Pain Inventory; FACT/NTx, Functional Assessment of Cancer Therapy/Neurotoxicity Questionnaire; TNSc, Total Neuropathy Score–Clinical Version; NCV, nerve conduction velocity; EA, electroacupuncture; GOG, gynecologic oncology group; Acu, acupuncture; Mec, mechanisms; QD, twice a day; QOD, every other day; VAS, Visual Analog Scale; PNQ, Patient Neurotoxicity Questionnaire; EORTC QLQ, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire; CIPN, chemotherapy-induced peripheral neuropathy; BPI-SF, Brief Pain Inventory–Short Form; NPS, Neuropathy Pain Scale; TAX, taxane; NRS, Numerical Rating Scale.
Pilot Study of Acupuncture in Chemotherapy Induced Neuropathy.

Abbreviations: OSNS, Oxaliplatin-Specific Neurotoxicity Scale; PQAS, Pain Quality Assessment Scale; CINQ, Chemotherapy-Induced Neurotoxicity Questionnaire; FACT/NTX, Functional Assessment of Cancer Therapy/Neurotoxicity questionnaire; NPS, Neuropathy Pain Scale; BPI-SF, Brief Pain Inventory–Short Form; NCS, nerve conduction study; CIPN, chemotherapy-induced peripheral neuropathy.
The Risk of Bias and Quality Assessment
The quality of each enrolled study was assessed independently by 2 reviewers, adopting the criteria recommended in the Cochrane Handbook for Systematic Reviews of Interventions, version 5.1.0. 41 Six domains were assessed: (1) generation of randomization, (2) allocation concealment, (3) blinding of participants and personnel, (4) blinding of outcome assessment, (5) incomplete outcome data, and (6) selective outcome reporting. We assessed the quality of the included studies using the modified Jadad scale.42,43 The modified Jadad scale represents the quality of RCT, awarding a maximum of 5 points (1 point each for randomization, appropriate randomization method, describing dropouts, patient blinding, and assessor blinding). When data were missing or incomplete, we contacted authors to identify additional studies and asked them to provide methodological details.
Data Synthesis and Statistical Meta-Analysis
To analyze the effects of acupuncture on consistent outcomes (mean change in BPI-SF and FACT-NTX scores) and NCV after treatment compared with baseline, we estimated the weighted mean differences and 95% confidence intervals (CIs) from each study using the Cochrane Collaboration’s software, Review Manager (RevMan) Version 5.2 for Windows (The Nordic Cochrane Centre, Copenhagen, Denmark). For weighted mean differences, a point estimate of zero reflected “no effect,” and less than zero favored the acupuncture intervention. Statistical heterogeneity was assessed by using the χ2 test (P < .1). The I2 statistic was also calculated, and we considered I2 > 50% to indicate significant heterogeneity across studies. 44 A random-effects model was used if significant heterogeneity was shown in the included trials. Otherwise, results were obtained from a fixed-effects model. The results of other outcomes measures are shown in Table 1.
Results
Evaluation of Quality and Descriptions of the Included Trials
Table 3 shows the risk of bias in the 6 included studies. Most studies had a low risk for all domains, indicating a convincing quality of this systematic review. The quality of included studies was high, in that 3 studies had scores of 5, and 3 had scores of 4 on the modified Jadad scale.
Risk of Bias in the Included Trials a .

Modified Jadad Scale: Jadad et al. 42
The 6 randomized clinical trials included 386 patients with CIPN (Table 1). Sample sizes ranged from 38 to 98. The control treatments varied from blank control to sham acupuncture, usual care, and vitamin B or methylcobalamin. Some RCTs had more than one control group. The heterogeneity and limited number of studies may contribute to some risk of bias. Table 3 shows the risk of bias in each of 6 domains, and Figure 2 demonstrates the risk of bias graph of included trials. Nevertheless, we included only studies with consistent outcomes for meta-analysis, in order to reach valid results.
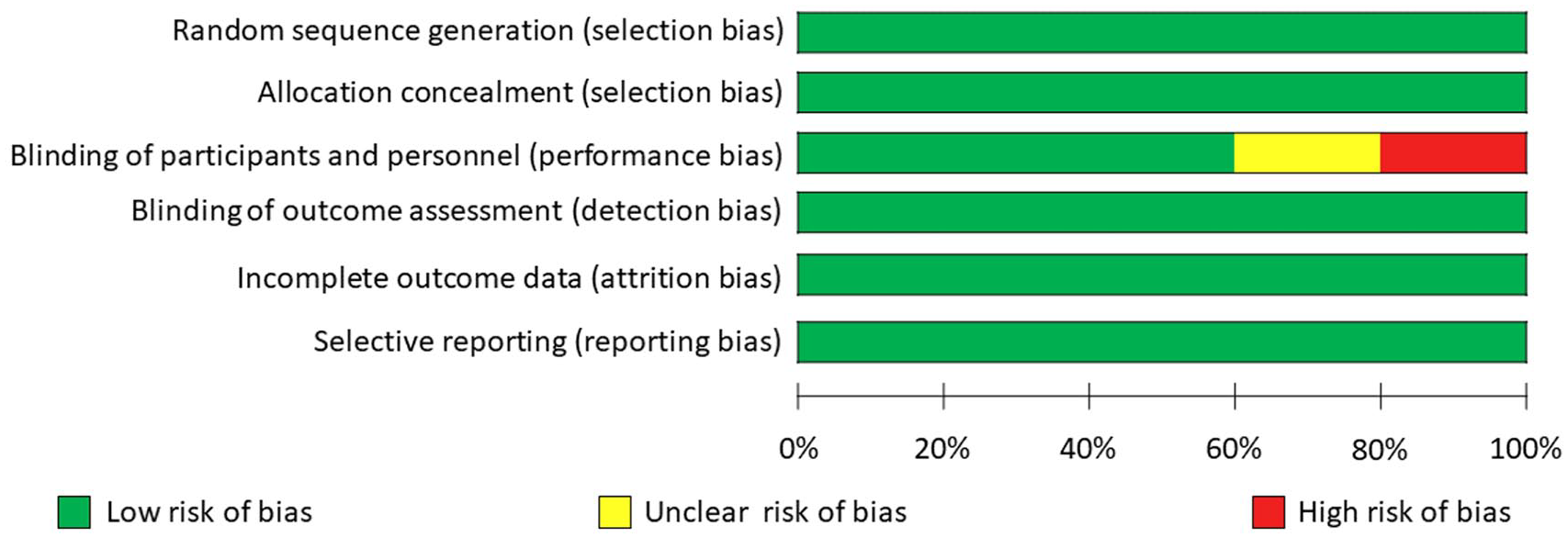
Risk of bias graph of included trials.
Effects of Acupuncture on CIPN Symptoms
Owing to the small number studies, we did not perform funnel plots and publication bias cannot be excluded. We observed significant between-study heterogeneity in the effects of acupuncture on neuropathy symptoms and quality of life (I2 = 89% and 36%, respectively). As for the 3 trials that reported pain scores, a significant reduction in the BPI-SF mean worst pain score was observed in subjects treated with acupuncture (−1.21, 95% CI = −1.61 to −0.82, P < .0001; Figure 3A) as compared with control subjects. For the 4 trials that reported Functional Assessment of Cancer Therapy/Gynaecologic Oncology Group/Neurotoxicity scores,29,30 subjects receiving acupuncture showed significant improvement in nervous system symptoms (−2.02, 95% CI = −2.21 to −1.84, P < .00001; Figure 3B) as compared with control subjects. However, for the 2 trials that reported sensory NCV of the sural nerve, no significant change in NCV was observed in subjects treated with acupuncture (1.58, 95% CI = −2.67 to 5.83, P = .47; Figure 3C) as compared with controls.
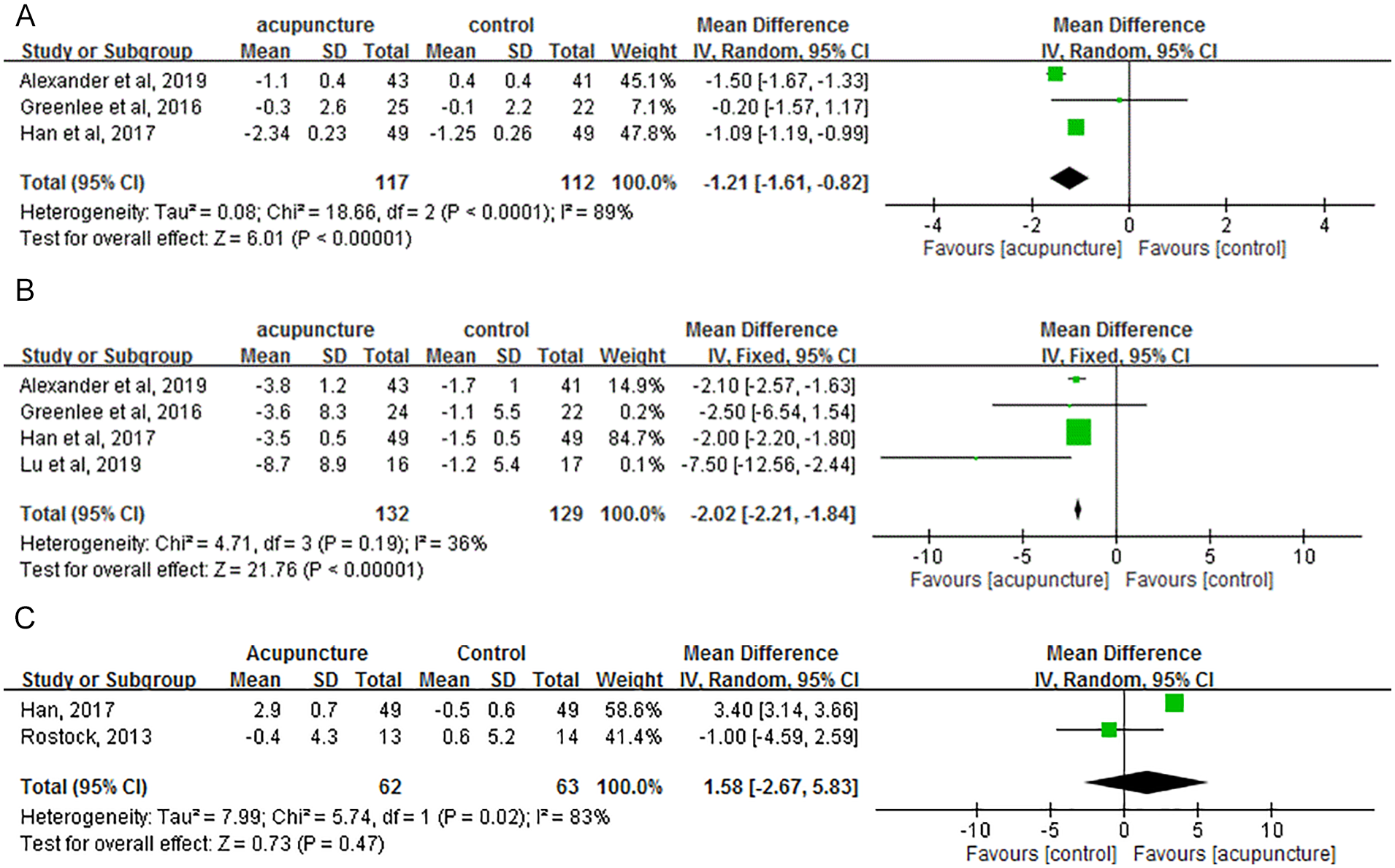
(A) Forest plot of the effect of acupuncture on the BPI-SF worst pain score of chemotherapy-induced peripheral neuropathy. (B) Forest plot of the effect of acupuncture on the FACT-NTX score of chemotherapy-induced peripheral neuropathy. (C) Forest plot of the effect of acupuncture on the sensory nerve conduction velocity of sural nerve for chemotherapy-induced peripheral neuropathy.
Discussion
The application of acupuncture to CIPN is important, since the condition currently has no definitive treatment. According to the studies we reviewed, acupuncture has the potential to improve quality of life in terms of pain score and FACT-NTX assessment, yet no difference in NCV or relevant serum cytokines has been reported.
Among the 6 RCTs collected in our systematic review, 4 found a positive effect of acupuncture on CIPN. The negative studies raise questions about different effects across acupuncture modalities, utility, and timing.
Since the outcome measurements were not consistent across studies, only BPI-SF, FACT-NTX, and NCV could be used for meta-analysis. In the qualified enrolled studies, we found positive effects of acupuncture in these variables. Individually, Molassiotis et al 31 and Han et al 33 concluded that acupuncture can improve quality of life and neuropathy, while Greenlee et al 32 noted an inferior effect of acupuncture compared with sham control, and Rostock et al, 36 who used a 4-arm study, deemed the efficacy of acupuncture unclear. Zhang et al 34 found electroacupuncture superior to acupuncture in terms of symptom relief and quality of life improvement in treating bortezomib-related neuropathy. Others found a positive effect for bortezomib-induced neuropathy33,38,39 but a negative effect for taxane used for breast cancer. 32 Despite these findings, the limited number of studies prevents drawing any definite conclusions about the efficacy of acupuncture. We further reviewed the relevant pilot studies of acupuncture on chemotherapy-induced nausea and vomiting, some designed to target bortezomib-related neuropathy but others not restricted by type of chemo-regimen. However, only Zhang et al 34 used objective measures such as proinflammatory cytokines, and they showed no difference after acupuncture.
The cause and progression of CIPN involves multiple mechanisms according to drug type. For taxanes, the cause is attributed to disruption of the microtubule structure, which leads to impairment of axoplasmic transport and dying-back neuropathy.45,46 Bortezomib damages the dorsal root ganglia neuronal cell bodies, leading to peripheral nerve degeneration. 47 The mechanism of neuropathy related to thalidomide or lenalidomide is uncertain, although most complaints are sensory impairment, with some autonomic neuropathy also being noted. 48 Platinum derivatives, the most commonly used regimen, have been noted to be retained in the dorsal root ganglion cells with reduction in nuclear size. 49 Other chemo-regimens that lead to neuropathy include ixabepilone and vinca-alkaloids. These regimens interfere with axonal transport 50 or produce a loss of axonal microtubules and alterations in their length, arrangement, and orientation. 51 In most cases, the neurotoxicity is related to the accumulating dose and use period, yet none of the studies addressed the accumulated dose of the chemo-regimen.
Previous research does not indicate whether acupuncture can accelerate neuron recovery. One study found that the efficacy of acupuncture in oxaliplatin-induced neuropathy works through activation of the serotonergic system, especially spinal 5-HT3 receptors. 52 Another study claimed that acupuncture can alter sensory perception, reducing the pain evoked by blunt pressure or the perception of noxious heat or cold. 53 In short, acupuncture can reduce CIPN to some extent via improving symptoms, but the mechanism is not clear. Finally, many studies have noted that polymorphisms of genes play an important role in CIPN, which might affect the drug metabolism 54 or the relevant repair mechanisms and inflammation. 55 In short, our current understanding of CIPN is in its infancy. Nevertheless, our study showed that acupuncture is safe and has great potential in relieving symptoms, although large-scale studies remain to be conducted.
As for the choice of acupoints, different trials adopted diverse acupoints complex without consistency. This issue had been noted for a period time since in different topics about acupuncture-related meta-analysis, choice of acupoints always varied in included RCTs. However, we noted in this topic that some common acupoints are categorized to spleen (SP6, SP10) and liver (LI4, LI11) meridians. We supposed that the spleen and liver meridians circulate to breast area, whereas another important acupoint, ST36 (ZuSanLi), is famous in boosting overall immunity and vitality, the so called Qi (氣). 56 Anyway, it is hard to have a definite and consistent prescription in acupoints selection in clinical trials in certain diseases, yet some articles also discuss whether De-Qi is no less important than acupoints selection. 57
To our knowledge, this is the first systematic review of the effect of acupuncture in chemotherapy-related neuropathy. Clinical trials have demonstrated that there is no unequivocal gold standard for the prevention and treatment of CIPN. 58 Several neuroprotective agents including thiols, neurotrophic factors, anticonvulsants, and antioxidants have been tested in preclinical models and RCTs for their ability to prevent or treat symptoms of CIPN. 59 Although agents like vitamin E, glutamine, glutathione, N-acetylcysteine, oxcarbazepine, and xaliproden have shown promise, convincing evidence for their efficacy is still lacking. 60 In this context, we assume that acupuncture is a feasible and promising method for its safety and noninvasive approach, which in turn means patients can avoid taking more drugs and risking further drug interaction. However, research relevant to this issue is limited and the control arms are varied; furthermore, more quantitative tools, such as NCV examinations, 61 verified cytokines targeted to a specified regimen31,62 and image studies63,64 such as functioning magnetic resonance imaging could provide more objective evidence and warrant scholars’ consideration in the future. 65
Last, from the perspective of Chinese medicine, acupuncture promotes the flow of Qi (氣), which reconciles the Yin-Yang and thus improves both symptoms and pain; this theory, though, is difficult to prove. A critical drawback to clinical trials of acupuncture is that researchers have reached no consensus on what constitutes a consistent acupuncture schedule, including acupoint selection, treatment course, and frequency. Given the need for individualized treatment, a basic consistency in schedule will further the crosstalk between acupuncture and modern medicine. We observed that an acupuncture protocol for peripheral neuropathy was published in 2017, which implies some progress in this area. 66
Limitations
One limitation of this systematic review is the limited number of trials, despite the timeliness of the topic. The variety in control arms may also have led to some bias in explaining the results. The outcome measurements were not consistent, complicating the analysis. Additionally, the result will be more convincing with a larger number of cases; nevertheless, acupuncture shows promise in its ability to deal with CIPN due to its safety and previous evidence-based efficacy in pain relief and neuromodulation. In terms of its use in CIPN, further large-scale, regimen-targeted design, randomized studies are warranted. From an objective perspective, if more medical centers can join together to conduct a similar study in one country or even in different countries, that will promote the traditional Chinese medicine–related research and lead to more convincing results.
Conclusion
This meta-analysis of the efficacy of acupuncture in CIPN reveals that acupuncture can reduce pain and improve quality of life (FACT-NTX score). However, we cannot yet recommend a definite acupuncture protocol from the limited number of studies reviewed here. Future study design will need to include more quantitative end points, such as completed NCV, quantitative sensory testing or proinflammatory cytokines, and neurotrophic factors. Considering the safety and lack of serious adverse effects associated with acupuncture and the lack of a definite treatment for CIPN, acupuncture could be considered for treating CIPN.
Supplemental Material
S1_Appendix._Search_Strategy_20190919 – Supplemental material for The Efficacy of Acupuncture in Chemotherapy-Induced Peripheral Neuropathy: Systematic Review and Meta-Analysis
Supplemental material, S1_Appendix._Search_Strategy_20190919 for The Efficacy of Acupuncture in Chemotherapy-Induced Peripheral Neuropathy: Systematic Review and Meta-Analysis by Tsai-Ju Chien, Chia-Yu Liu, Ching-Ju Fang and Chun-Yu Kuo in Integrative Cancer Therapies
Supplemental Material
S2_Appendix._PRISMA_2009_Checklist – Supplemental material for The Efficacy of Acupuncture in Chemotherapy-Induced Peripheral Neuropathy: Systematic Review and Meta-Analysis
Supplemental material, S2_Appendix._PRISMA_2009_Checklist for The Efficacy of Acupuncture in Chemotherapy-Induced Peripheral Neuropathy: Systematic Review and Meta-Analysis by Tsai-Ju Chien, Chia-Yu Liu, Ching-Ju Fang and Chun-Yu Kuo in Integrative Cancer Therapies
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from Ministry of Science and Technology, 108-2320-B-532-001-MY3.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.