
Abstract
Background. Methods currently available to prevent and manage xerostomia which caused by radiotherapy in patients with head and neck caner have limited efficacy. Some studies suggest that acupuncture may be beneficial. Objectives. The authors evaluated the preventive and therapeutic effect of acupuncture for radiation-induced xerostomia among patients with head and neck cancer. Methods. PUBMED, EMBASE, Cochrane Library, CBM, CAJD, Wan Fang database, and VIP Database for Chinese Technical Periodicals were electronically searched, in conjunction with further manual search for relevant articles. Studies that met the inclusion criteria were systematically evaluated. Results. Three randomized controlled trials (RCTs) investigating the therapeutic effect of acupuncture were included. One RCT on the preventive effect of acupuncture was found. Because of the considerable variation among included studies, meta-analysis was not possible. Two included RCTs used placebo controls, and both observed significant improvement in the salivary flow rates between acupuncture and control groups. However, no significant differences were found. Three included RCTs suggested that acupuncture for radiation-induced xerostomia can improve patients’ subjective symptoms. The only study evaluating the preventive effect of acupuncture for radiation-induced xerostomia showed positive changes in salivary flow rates (both unstimulated and stimulated) and dry mouth -related symptoms. Acupuncture treatment was well tolerated by all patients and no severe adverse effects were seen. Conclusions. Insufficient evidence is available to judge whether acupuncture is safe and whether it is effective in preventing or treating radiation-induced xerostomia. Significant research remains to be done before acupuncture can be recommended for routine use in radiation-induced xerostomia.
Introduction
Head and neck cancer (HNC) is one of the most common cancers worldwide. Radiotherapy is an integral part of the management of this disease, either as primary treatment or in conjunction with surgical resection. 1 Radiotherapy is typically associated with acute and chronic toxicities that can have a profound effect on patients’ quality of life. Xerostomia is one of the most common complaints. Salivary glands are highly radiosensitive, 2 and the destruction of salivary glands begins in the first few days of radiotherapy. In the first week, a 50% to 60% decrease in salivary flow occurs, and after 7 weeks of conventional radiotherapy, salivary flow diminishes to approximately 20%. 3 The severity of xerostomia depends largely on the dose of radiation administered and the irradiated gland volumes.4,5 The level of radiation necessary to destroy malignant cells ranges from 40 to 70 Gy, and dosages greater than 30 Gy are sufficient to change salivary function permanently. 6
Effective management is needed as xerostomia can reduce the quality of life as well as interfere with compliance or cause treatment delays, resulting in loss of tumor control. 7 Currently, available methods used to manage radiation-induced xerostomia include stringent oral hygiene with fluoride agents and antimicrobials to prevent dental caries and oral infection, saliva substitutes to relieve symptoms, and sialogogic agents to stimulate saliva production from remaining intact gland tissue.8-13 However, these treatments all have limited efficacy, and prevention is paramount. Several strategies have been developed to avoid radiation-induced salivary dysfunction, including cytoprotectants,14,15 salivary gland transfer,16,17 and salivary gland–sparing radiation techniques, such as 3-dimensional conformal or intensity-modulated radiotherapy.18-21 Nevertheless, not all patients can benefit from these preventive approaches. Salivary gland transfer is only practical in patients who plan to receive postoperative radiotherapy as the transfer is done during the surgical intervention. Intensity modulated radiotherapy can avoid some destruction of salivary glands; however, benefits vary based on technique, location of tumor, and status of lymph metastasis. 22 Radiation-induced xerostomia is still a critical problem to manage.
Acupuncture is a complementary, alternative medicine modality that is practiced in many parts of the world for a variety of ailments, such as pain, musculoskeletal disorders, and several neurologic diseases. 23 Acupuncture has been used to deal with xerostomia caused by various etiologies. It has been shown that acupuncture can increase salivary flow in healthy volunteers,24,25 patients with Sjogren’s syndrome, 26 and those with radiation-induced salivary gland damage.27-29 Acupuncture may be a useful therapy for the treatment of radiation-induced xerostomia. No reported trial has been large enough to accurately establish the efficacy of acupuncture for radiation-induced xerostomia with an acceptable degree of certainty. Before acupuncture can be recommended for routine use, we require compelling evidence. We aim to conduct a systematic review and meta-analysis to evaluate all the currently available studies of acupuncture as a treatment for radiation-induced xerostomia.
Methods
Search Strategy
All databases were searched up to September 30, 2011. We searched PUBMED, EMBASE, and Cochrane Library with the following medical subject headings (MESH): Xerostomias, Hyposalivation, Asialia, Mouth Dryness, Radiotherapy, Irradiation, Brachytherapy, External Beam, Acupuncture Therapy. There were no language restrictions. We also searched Chinese databases, including Chinese Biology Medicine (CBM), China Academic Journal Network Publishing Database (CAJD), Wanfang database, VIP Database for Chinese Technical Periodicals, using the key words Zhenjiu, Zhenci, Kougan, Kouqiangganzao, Tuoyequefa, Tuoyejianshao, Fangliao, and Fangshe. Electronic searches were supplemented with manual searches of reference lists of all retrieved review articles, primary studies, and abstracts from meetings to identify other studies not found in the electronic searches. Literature was searched by 2 authors (L-P Zhuang and Z-G Yang), and any inconsistencies were discussed with a third author (Z-Q Meng).
Selection Criteria
Two authors independently selected trials and discussed with each other when inconsistencies were found. Studies were included based on analysis of the following:
Participants: To evaluate the therapeutic effect of acupuncture, only studies that recruited patients with xerostomia and a history of radiotherapy for their HNC were included; to evaluate the preventive effect of acupuncture, we included studies that recruited patients with HNC who were undergoing radiotherapy. Interventions: To evaluate the therapeutic effect of acupuncture, only studies using invasive acupuncture were included, such as needling and needling with moxibustion. Variations in session, frequency, duration, and needling details were acceptable. The intervention and control groups could be placebo control or usual care. To evaluate the preventive effect of acupuncture, we included studies comparing radiotherapy combined with acupuncture versus radiotherapy only. We defined invasive acupuncture as acupuncture with needle penetration of skin. Noninvasive acupuncture refers to acupuncture without a needle, or in which the needle does not penetrate the skin, such as laser acupuncture or applying herbal medicine to the surface of acupoints. Co-interventions were allowed, such as Chinese herbal medicine, but they had to be balanced between the 2 groups. Outcome measures: Only studies using one or more of the following measurements were eligible: objective methods, such as salivary flow rates, salivary gland scintigraphy (SGS), or functional magnetic resonance imaging (fMRI) of salivary glands; or subjective measurements with observer-based toxicity grading or patient self-reported scoring, such as visual analogue scales, xerostomia inventory, or quality of life. Study types: Priority was given to randomized controlled trials (RCTs); if RCTs are unavailable, we would consider including non-RCTs.
The exclusion criteria were the following:
Full article not available Co-interventions not balanced between the 2 groups Studies used noninvasive acupuncture
Quality Assessment
The methodological quality of included RCTs was assessed according to the Cochrane Collaboration’s tool described in Handbook version 5.1.0. 30 Two authors (L-P Zhuang and X-T Zeng) assessed the quality independently, and inconsistency was discussed with a third review author (Z-Q Meng), who acted as arbiter.
Data Extraction
The included trials were reviewed using a list of predefined questions concerning patient characteristics, radiation modality, dosage, fields, acupuncture prescriptions (including acupuncture rationale, needling details, treatment regimen, co-intervention, practitioner background, control intervention), and interval between radiotherapy and acupuncture. Data extraction was done by 2 independent investigators (L-P Zhuang and Z-G Yang). Data sheets were compared and discussed with a third review author (Z-Q Meng). We contacted corresponding authors (if address was available) for missing data.
Outcome Variables
We evaluated the preventive and therapeutic effects of acupuncture on radiation-induced xerostomia using objective measures (salivary flow rates) and subjective measures (patient self-reported scores).
Data Analysis
Clinical heterogeneity was evaluated first. Without clinical heterogeneity, statistical heterogeneity among studies was then assessed with the Pearson χ 2 test and I 2 test. If statistical heterogeneity existed among studies, a random-effects model was used to incorporate the heterogeneity. If statistical heterogeneity was not found among studies, a fixed-effects model was used. Salivary flow rates and patient self-reported score were continuous outcomes, so the mean difference (MD) or the standardized mean difference (SMD) was used for meta-analysis. If there was considerable variation among studies, a brief qualitative analysis of evidence would be presented. Review Manage (v.5.1; Oxford, England) was used to for the data analysis.
Results
Search Results
Figure 1 describes the procedure for selecting eligible trials. Our search yielded 482 citations. After review of the titles and abstracts, we excluded 427 studies, and 59 studies were full-text reviewed. Eventually, 4 studies31-34 were included.

Flowchart of the study selection process
Description of the Included Studies and Data Analysis
Three RCTs investigating the therapeutic effect of acupuncture were included. The total number of patients was 110, with 54 patients in the acupuncture group and 56 patients in the control group. Only 1 RCT investigating the preventive effect of acupuncture was found, 34 in which acupuncture was conducted before and during radiotherapy. This study included 40 patients in the acupuncture group and 46 patients in the control group. The 4 studies were conducted in Sweden, Korea, America, China. The specific subtypes of HNCs varied widely in each study. The study by Pfister 33 reported the subtypes of HNCs with pathological types. Histological types were divided into 4 categories: thyroid cancer, squamous cell carcinoma, melanoma, and others. Squamous cell carcinoma accounted for 57% of the acupuncture group patients and 70% of control group patients. The study by Meng et al 34 recruited patients with nasopharyngeal carcinoma only. The other 2 studies reported the subtypes of HNCs with the tumor sites. Each study recruited patients with various tumor sites. Overall, the 5 most common subtypes in these 2 studies were larynx cancer, oropharynx cancer, nasopharynx cancer, hypopharynx cancer, and tongue cancer.
Meta-analysis was considered inappropriate for this review, because of the obvious clinical heterogeneity and considerable variation in outcome measurements. For instance, there were variations among studies in disease-state characteristics of patients, variations in salivary flow rates before treatment, differences in salivary flow rate evaluation (different times using different stimulants after the treatment), and differences in questionnaires used for patient self-reporting. Thus, a brief qualitative analysis of the evidence is presented in narrative form (supplemented by Tables 1 and 2). The description of acupuncture intervention is based on the Standards for Reporting Interventions in Controlled Trials of Acupuncture (STRICTA). 35 The details covered 6 areas, including acupuncture rationale, needling details, treatment regimen, co-intervention, practitioner background, and control intervention.
Characteristics of Included Studies

Abbreviations: TD, total dose; RT, radiation therapy; RCT, randomized controlled trial.
Intervention Details of Acupuncture for Each Study
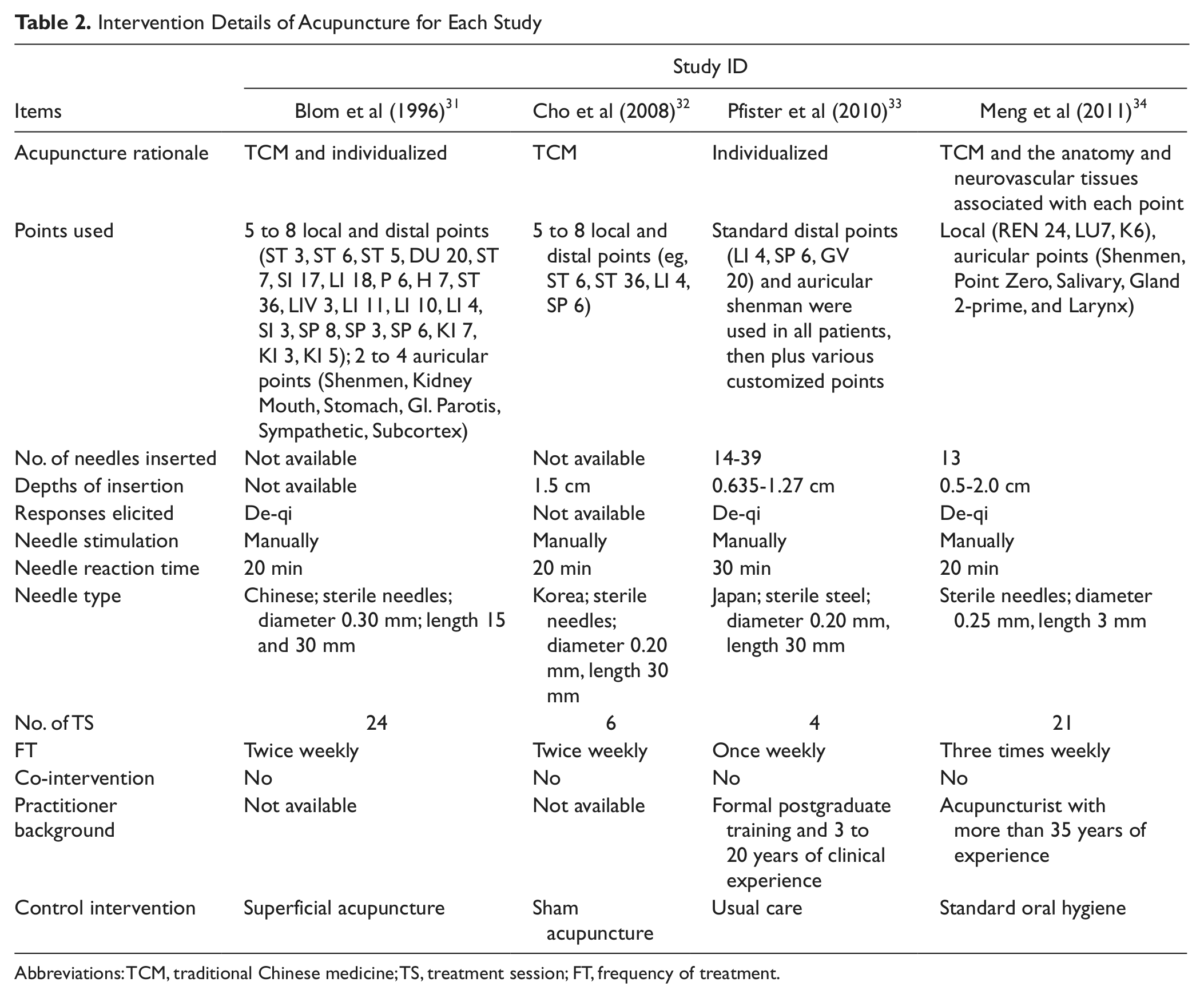
Abbreviations: TCM, traditional Chinese medicine; TS, treatment session; FT, frequency of treatment.
The parotid gland is the most important gland for salivation. Studies have revealed that there is a direct association between saliva flow reduction and the mean radiation dose administered to the parotid. 36 So we extracted data on the volume of radiation delivered to the parotid. Only 1 study 32 described in detail the principles used in choosing acupuncture points—for this study, points that support salivary flow or water-like elements of the body were chosen. The points most frequently used were ST 36, LI 4, auricular of Shenmen, and the corresponding points in the ear (such as parotis, larynx, and mouth)
Results of Methodological Quality Assessment
All the studies were described as randomized. However, only in 2 studies33,34 was random assignment implemented via a secure computerized database, ensuring full concealment of allocation. Double blinding was described in 1 trial, 31 and neither the examiner nor the patients knew whether acupuncture or placebo acupuncture had been given in this study. One trial 32 used a single-blind setting, and the placebo setting was considered as appropriate. The study by Pfister et al 33 had 6 patients lost to follow-up, but the missing outcome data were balanced between the 2 groups. In the study by Meng et al, 34 at 7-week follow-up, missing outcome data were balanced between intervention groups, with similar reasons for missing data. However, at 11-week and 6-month follow-up, missing outcome data were not balanced between groups. No patient was lost to follow-up in the other 2 studies, and intent-to-treat principle was used in these 4 RCTs. They were considered as low risk for incomplete outcome data, whereas the study by Meng et al 34 was considered high risk. Selective reporting was found in the study by Pfister et al, 33 because it failed to include results that would be expected to have been reported for such a study, for example, the salivary flow rates. In the study by Cho et al, 32 subjects were not evenly divided based on disease-state characteristics, which we considered as a potential source of bias (see Figures 2 and 3 for overview).

Risk of bias graph: review authors’ judgments about each risk of bias item presented as percentages across all included studies

Risk of bias summary: review authors’ judgments about each risk of bias item for each included study
Efficacy and Safety of Acupuncture for Radiation-Induced Xerostomia
Therapeutic effect of acupuncture for radiation-induced xerostomia
Two included RCTs used salivary flow rates as objective outcome measures. Blom et al 31 reported that in the acupuncture group 68% and in the control group 50% of the patients had increased salivary flow rates at the end of the 1-year observation period. Significant differences of salivary flow rates between pretreatment and posttreatment could be observed within each group, but there were no statistically significant differences between acupuncture and control groups. Cho et al 32 reported that real acupuncture significantly improved unstimulated saliva secretion at 6 weeks, compared with before acupuncture treatment (0.030 ± 0.013 vs 0.071 ± 0.071, P < .05), and difference between acupuncture and control groups was not significant at any time point.
Three included RCTs used different patient self-reported scores as subjective outcome measures. Blom et al 31 reported the alleviation of symptoms, leading to a better quality of life, but without quantitative data. The questionnaire used by Cho et al 32 consisted of 4 questions addressing problems in communicating, eating, sleeping, and daily functions. They found that real acupuncture markedly improved scores for dry mouth according to the xerostomia questionnaire, to 2.33 points versus 0.33 in the controls. Pfister et al 33 reported that acupuncture produced greater improvement in reported xerostomia (adjusted difference in Xerostomia Inventory= −5.8; 95% confidence interval = −0.9 to −10.7; P < .02). The Xerostomia Inventory used included 11 questions. Although the aforementioned studies showed improvement in the acupuncture groups, because of potential bias and variation among the included studies, we are unable to positively identify the therapeutic effect of acupuncture for radiation-induced xerostomia.
Preventive effect of acupuncture for radiation-induced xerostomia
The study by Meng et al 34 reported that significant differences between groups in saliva flow were found as early as 3 weeks into treatment (unestimated whole salivary flow rate [UWSFR], P = .0004), with greater saliva flow in the acupuncture group at week 7 (UWSFR, P < .0001; stimulated salivary flow rate [SSFR], P = .002), week 11 (UWSFR, P < .02; SSFR, P < .03), and at 6 months (SSFR, P < .003). Both Xerostomia Questionnaire scores and the MD Anderson Symptom Inventory–Head and Neck scores were statistically significantly lower for the acupuncture group than for controls, from week 3 through 6 months (P = .003 at week 3, all other Ps < .0001).
Side effects of acupuncture for radiation-induced xerostomia
One included study provided no information on the side effects of acupuncture, whereas the other 3 studies showed that acupuncture treatment was well tolerated by all patients. The most frequent side effect was tiny hemorrhage at puncture site, and no severe adverse effects were seen. However, based on the small number of patients included in this review, there was no sufficient evidence to determine the safety of acupuncture treatment.
Discussion
Because of the considerable variation among the included studies, meta-analysis was not possible. There was no sufficient evidence to recommend acupuncture for routine use. However, there are several issues that merit discussion.
The Optimal Candidates
To apply acupuncture therapy to a specific patient population, we need to choose the optimal candidates. However, patients with various subtypes of HNC were recruited into our review, and the total number of each subtype was too small to define optimal candidates for each one. In our own opinion, no matter where the primary tumor site is, the degree of injury to the salivary glands has the greatest impact on acupuncture efficacy. We assume that a study comparing the effects of acupuncture for different degrees of injury to the salivary glands is necessary, especially for the parotid gland.
Prevalence of Acupuncture
Acupuncture has been extensively used in the treatment of radiation-induced xerostomia, but has not yet been accepted as a standard treatment. Many of the published studies had a small number of participants; therefore, a high-quality meta-analysis is necessary to increase sample size. Furthermore, acupuncture prescriptions in published studies have varied widely, including points used, number of needles inserted, depth of insertion, needle stimulation, needle reaction time, practitioner background, treatment sessions, and frequency of treatment. Finally, acupuncture treatment and control group interventions in trials of acupuncture are not always precisely reported. Rigorous trial design, more robust conclusions, and better data are needed to determine future policy and practice. The recommendations of the STRICTA should be put into practice. Adding to the lack of clarity is acupuncture’s unclear mechanism of action. A recent fMRI study showed central nervous system imaging changes (activation of the insula and adjacent operculi) during acupuncture for xerostomia. 25 These results are consistent with the suggestion that autonomic changes induced by needle manipulation inducing specific de-qi sensations might be mediated through the central nervous system, especially through the forebrain as shown in EEG changes. 37 Release of neuropeptides that stimulate the salivary glands and increase blood flow are other possible explanations for the effect of acupuncture for xerostomia. Studies by Dawidson et al have shown that the increased release of calcitonin gene-related peptide and vasoactive intestinal polypeptide may positively affect the salivary flow rates of xerostomic patients treated with acupuncture.38,39 Further studies of the mechanism of acupuncture are needed.
Appropriate Control Setting for Trials of Acupuncture
Placebo-controlled trials are a crucial tool to investigate the clinical effects of an intervention. To accurately identify the effect of acupuncture for radiation-induced xerostomia, an optimal control setting is necessary. To provide an effective and credible placebo, the control must be convincing and should mimic the real active treatment in all respects apart from a physiological effect. 40 The use of controlled needling in clinical trials of acupuncture has varied widely, that is, needling at nonacupuncture points, superficial needling, needling without manual or electrostimulation, 41 and sham acupuncture device42,43 (blunt tipped needle that retracts into a handle when “inserted into the skin,” though participants see and feel the needle penetration). No consensus has been reached on the standard placebo control setting in acupuncture research. Two of the trials included in this study used nonacupoint needling as a placebo control. The results showed no significant differences between the groups. This result calls into question whether nonacupoint needling is an effective and credible placebo. Though nonacupoint needling has been used extensively, many studies have argued that this control option is physiologically active and may not be an appropriate placebo. 44 The effect produced by acupuncture is usually attributed to 3 components: a nonspecific placebo effect, which is related to patients’ expectation and the interaction between patients and acupuncturists; physiological effect due to needles being inserted into the skin; and specific effect due to needling manipulation at specific acupoints. 45 Compared with nonacupoint needling, we believe that the sham acupuncture device designed by Streitberger and Kleinhenz 42 is most credible for use as a control in acupuncture research, because it is feasible to keep patients blind in the study of acupuncture by eliminating the effect caused by needle penetration through the skin, and the stimulation on the acupoints. Deng et al used this sham acupuncture device in their study. 25 In the study, unilateral manual acupuncture stimulation at Erjian (LI-2), a point commonly used in clinical practice to treat xerostomia, was associated with bilateral activation of the insula and adjacent operculum, and sham acupuncture at an adjacent site induced neither activation nor deactivation. The results demonstrated that true acupuncture induced more saliva production than sham acupuncture.
Suggestions for Treatment Protocol
According to syndrome differentiation based on theories of traditional Chinese medicine, xerostomia is caused by a lack of yin, 46 especially yin of stomach and kidney. Acupoints on stomach and kidney meridians are frequently used. Furthermore, radiation is described as a type of pathogenic factor known as toxic heat in the traditional Chinese medical theory. When dealing with this condition, we choose acupoints with an aim to clear away heat and toxic materials. We recommend the following acupoints. Local points: ST 4, ST 6, ST 7, CV23, CV24; distal points: LI 2, LI 4, LI 11, PC 6, LU 7, ST 36, KI 3, KI 5, KI 6,SP 6, LR 3; auricular points: Shenmen, Point zero, Salivary gland. The manipulation details of each acupoint vary with the function of the points, as does the manipulation method chosen (reinforcing method or draining method). We stress that the above suggestions represent the authors’ personal views. Although acupuncture has been used extensively to treat radiation-induced xerostomia, it by no means represents the standard of practice.
Issues Remaining
First, standardized measurements are necessary to compare the efficacy of preventive or curative interventions. For example, salivary flow rate is the most commonly applied objective measure of salivary gland function. However, results are not always comparable between studies because of variations in the nature of stimulants, duration of collection, and other factors that may affect salivary output. The method of evaluation of salivary flow rate should be defined in detail. Magnetic resonance sialography is also a potential measurement. In a word, an applicative questionnaire should be recommended.
Second, the optimal acupuncture treatment protocol needs further research, including the best combination of acupoints, the number of treatment session, and the manipulation details. Absolute consistency of the acupuncture treatment protocol is almost impossible, but we need to identify the critical factors that most influence the effect and then pay more attention to them during practice.
Third, how to choose the optimal patient population. Fourth, the mechanism of action of acupuncture for xerostomia, such as how long the increased salivary flow rates stimulated by acupuncture last. This evidence would help us design a better treatment regimen. Finally, studies with long-term follow-up are required, to more accurately identify the long-term and short-term effects of acupuncture.
Conclusion
Insufficient evidence is available to judge whether acupuncture is effective in preventing or treating radiation-induced xerostomia in patients with head and neck cancer. Significant research remains to be done in order to recommend acupuncture for routine use in radiation-induced xerostomia.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.