
Abstract
The role of hyperthermia (HT) in cancer therapy and palliative care has been discussed for years in the literature. There are plenty of articles that show good feasibility of HT and its efficacy in terms of tumor response and survival improvements. Nevertheless, HT has never gained enough interest among oncologists to become a standard therapy in clinical practice. The main advantage of HT is the enhancement of chemotherapy (CHT), radiotherapy (RT), chemoradiotherapy (CRT), and immunotherapy benefits. This effect has been confirmed in several types of tumors: esophageal, gastrointestinal, pancreas, breast, cervix, head and neck, and bladder cancers, and soft tissue sarcoma. HT effects include oxygenation and perfusion changes, DNA repair inhibition and immune system activation as a consequence of new antigen exposure. The literature shows a wide variety of randomized, nonrandomized, and observational studies and both prospective and retrospective data to confirm the advantage of HT association to CHT and RT. There are still many ongoing trials on this subject. This article summarizes the available literature on HT in order to update the current knowledge on HT use in association with RT and/or CHT from 2010 up to 2019.
Keywords
Introduction
Regional hyperthermia (HT) is defined as an external, supraphysiological increase of tissue/body temperature using external electromagnetic fields with rapid field alternations. 1 HT is currently used for local/locoregional heat application alone or complementary to radiotherapy (RT) and/or chemotherapy (CHT), increasing their efficacy in terms of both tumor response and survival, while keeping toxicity at comparable levels to the single therapies. 1 Another advantage of HT association to RT increases its effects, and in cases of re-irradiation, where standard dose or dose escalation is not possible, HT can augment the radiation treatment. 1
Multimodal therapies involving HT are applied to several types of tumors: colorectal, pancreas, breast, and bladder cancers, and soft tissue sarcoma (STS) with significant clinical benefits.1,2
The complementary application of HT with CHT or RT is successful in several types of tumors such as pancreatic, brain, and breast cancers.3-5 The use of HT to increase the sensitivity of tumor cells to ionizing radiation or chemotherapeutic agents is reported in several clinical trials.3-6 HT influences perfusion and oxygenation of tumor tissues resulting in increased blood flow and oxygenation enhancing radiosensitivity of the tumor. HT induces apoptosis and inhibits DNA repair. HT enhances the effects of immunotherapy and induces immune stimulation.
The present article is a literature-based review, based on a search in the PubMed, MEDLINE, Embase, Cochrane, and ClinicalTrials.gov databases of the term “hyperthermia” in combination with CHT and RT in gastrointestinal, esophageal, pancreas, colorectal, breast, cervical, head and neck, and bladder cancers, and soft tissue sarcoma lesions. This review aims to update the current knowledge on HT use in association with RT and/or CHT from 2010 up to 2019.
Heating techniques are classified according to the size, penetration depth, and region of energy release. Local or regional HT is generally associated with RT or CHT. Whole-body HT can be performed alone or in combination with CHT in cases of metastatic cancer. Different methods are used for HT: capacitive, radiative, infrared-A, or ultrasound are among the most used techniques. 1
Capacitive local heating requires the positioning of 2 electrodes on both sites of the body with direct body contact using a water bolus, and the heat is obtained by the electric current flow between the 2 electrodes. 1 Radiative heating uses frequencies of 75 to 915 MHz and a water bolus for electromagnetic coupling. 1 This method allows obtaining a better temperature distribution leading to homogeneous target coverage by heat than capacitive coupling. Walter-filtered infrared-A-based HT is used for superficial tumors (15-20 mm depth), using a halogen lamp, passing through a water filter. 1
Modulated electro-hyperthermia (mEHT) is a type of HT that can be performed using the EHY-2000+ device (OncoTherm Ltd). It is a safe form of HT, resulting only in mild adverse events, such as skin burn or pain, and heat-related injuries are observed in 5% of cases. 6 mEHT has comparable benefits as those obtained with other types of HT, improving local control and survival rates in several types of tumors, such as cervical, brain, and pancreatic cancer. 6 mEHT targets the malignant cells selectively, heating and sensitizing them to subsequent oncological therapies (CHT and/or RT). A recent review of mEHT effects in different types of cancer shows promising results concerning both local disease control and survival. 6
Methods
The article search was performed using the following terms: regional hyperthermia, efficacy, toxicity, in PubMed, MEDLINE, Embase, Cochrane, and ClinicalTrials.gov databases. The search retrieved 1662 articles. A further selection was made to include only observational or experimental trial that were published from 2010 through December 2019 without language limitation. Review articles were discarded from tables and were used for the introduction and general considerations. This review included 42 articles that were divided according to tumor type. Efficacy and toxicity of HT were described for each tumor type separately.
Esophageal Cancer
Phase II trials report the feasibility of chemoradiotherapy (CRT) + HT as neoadjuvant treatment.7-10 A study on esophageal squamous cell carcinoma treated with CRT + HT shows 27% of complete response (CR) and 45% of stable disease (SD) with overall survival rates at 1, 2, and 5 years after CRT of 72.7%, 54.5%, and 9.1%, respectively (Table 1). 11 The data from a retrospective study on metastatic esophageal squamous cell carcinoma report that 3-year progression-free survival (PFS) rate and overall survival (OS) rate were 34.9% and 42.5%, respectively, after CRT + HT therapy, and HT-related pain (38.0%) and fatigue (40.0%) were of mild intensity, grade (G) 1 to 2 (Table 1). 11
Esophageal Cancer.

Abbreviations: HT, hyperthermia; ND, not reported; CRT, chemoradiotherapy; CR, complete response; SD, stable disease; PFS, progression-free survival; OS, overall survival; G, grade.
The available literature reports evidence of CRT + HT benefits in esophageal cancer therapy; nevertheless, further randomized clinical trials are required to compare CRT + HT versus CRT alone to confirm the above-mentioned data.
Colorectal Cancer
Surgery is the standard treatment for patients with colorectal cancer; however, the results are very poor for locally advanced cancer, in terms of both survival and recurrence. 13 The main aim of the treatments for locally advanced rectal cancer is the achievement of high resectability; for this reason, neoadjuvant CRT is often used to obtain high percentages of pathologic CR (pCR). 14
The introduction of CRT improves locoregional control for locally advanced colorectal cancer. This improvement is further achieved when CRT is associated to HT, resulting in long-term tumor control and survival in locally advanced nonmetastatic rectal cancer. 15 CRT + HT allows achievement of promising rates of pCR, ranging from 22.5% to 69% (Table 2). This association is safe, showing comparable toxicity with CRT alone and 6.5% of G >3 adverse events, such as skin reaction, diarrhea, stomatitis, and nausea/emesis, which were not increased with the additional use of HT; moreover, subcutaneous burns in 5.2% disappeared spontaneously within 2 weeks.16-21 Other HT-related adverse events were of G0 to G2 and included general or local discomfort in 15% of cases. 17 Concerning survival, CRT + HT allows longer OS with 5-year OS significantly higher than CRT alone (88% vs 76% P < .08). 16
Colorectal Cancer.
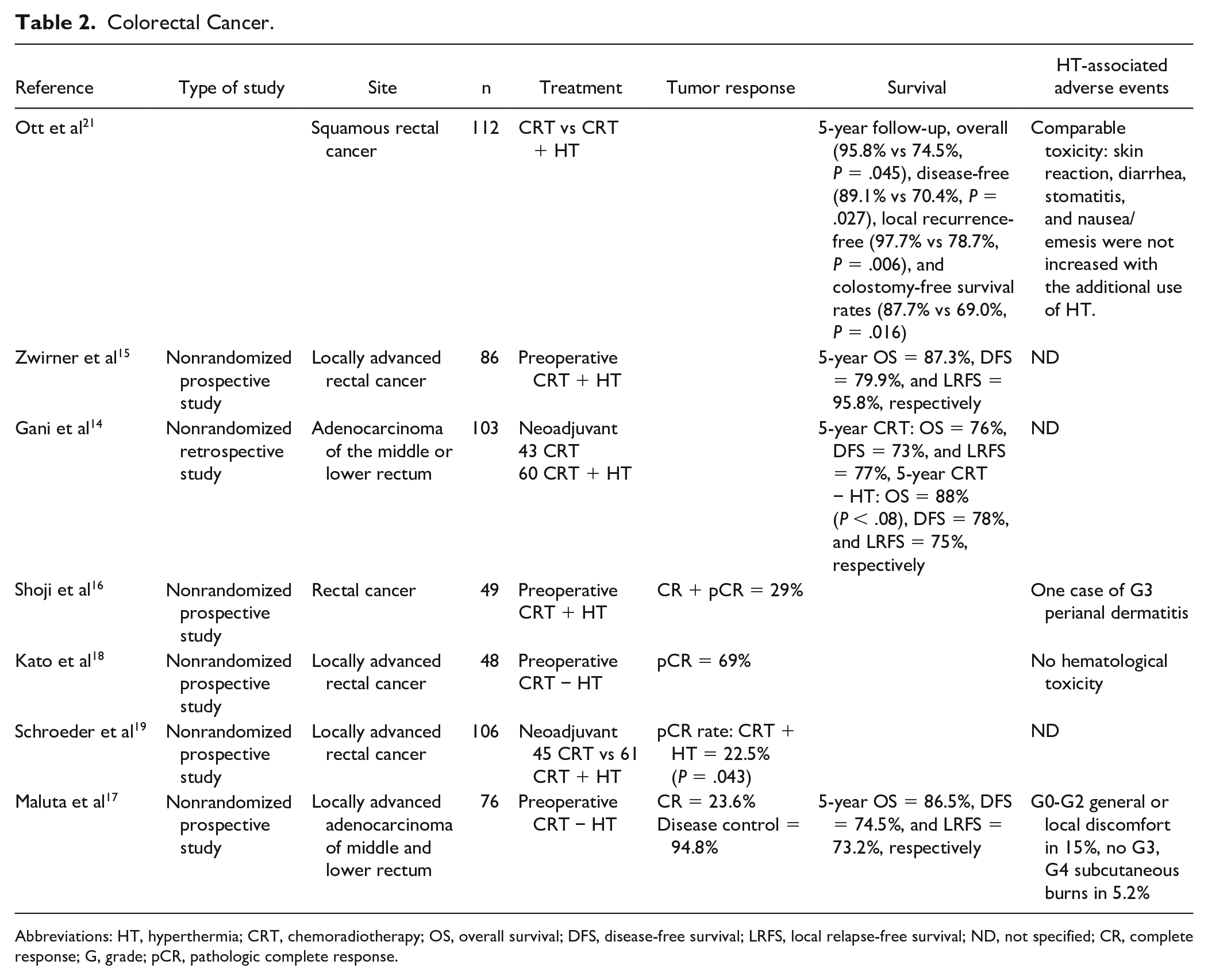
Abbreviations: HT, hyperthermia; CRT, chemoradiotherapy; OS, overall survival; DFS, disease-free survival; LRFS, local relapse-free survival; ND, not specified; CR, complete response; G, grade; pCR, pathologic complete response.
RT + HT is effective and well tolerated also in chemorefractory liver metastases from colorectal cancer, resulting in mild/moderate toxicity and the objective response of 30%. 20
In conclusion, preoperative CRT and HT association yields to acceptable toxicity, improved response rate, and survival; however, further studies are required to confirm the long-term benefit of CRT + HT in locally advanced colorectal cancer and liver metastases.
Pancreatic Cancer
The incidence of pancreatic cancer is constantly increasing, and pancreatic cancer reaches the fourth place among the most frequent causes of cancer deaths. 22 Advanced unresectable pancreatic cancer is diagnosed in >80% of patients, and standard first-line treatment is still missing for this population that develops recurrence in an average of 6 months with a very low OS of 1.9 months. Gemcitabine-based CHT is the most common treatment for unresectable pancreatic cancer, whereas FOLFIRINOX (leucovorin, fluorouracil, irinotecan, and oxaliplatin) is more indicated for fit patients because of the high toxicity. 23 mEHT is feasible for both palliative care and therapeutic purposes also in advanced pancreatic cancer,24-30 increasing OS and improving quality of life. These advantages of mEHT and HT are observed when it is used alone or in association with CRT for locally advanced pancreas carcinoma.24-30 Median OS increases from 10% to 11% of CRT alone to 15% to 18% of CRT + HT (Table 3). The disease control (DC) rate increases from 66% to 92% after mEHT. 24 Regional HT also shows encouraging DC rate (50%). As concerning the safety, no grade III to IV toxicity is observed, suggesting the good tolerability of HT in pancreatic cancer treatment.
Pancreas.

Abbreviations: HT, hyperthermia; mEHT, modulated electro-HT; RT, radiotherapy; CHT, chemotherapy; DC, disease control; OS, overall survival; PFS, progression-free survival; CRT, chemoradiotherapy.
Further studies that will investigate the effects of HT include the HEATPAC trial, a phase II randomized trial, in unresectable locally advanced pancreatic cancer that will explore the feasibility and efficacy of HT associated with CRT versus CRT alone, with pre- and postintervention FOLFIRINOX. 29
In conclusion, longer median OS and better tumor response can be obtained in correlation with HT treatment, suggesting a beneficial effect of HT in association with CHT and/or in locally advanced or metastatic pancreatic cancer with a low toxicity profile.
Breast Cancer
As concerning breast cancer therapy, surgery and CRT are very effective; however, there is a 30% local recurrence.1,2 HT is among the oldest methods of cancer therapy, and since 2013, it has been included in the National Comprehensive Cancer Network (NCCN) clinical practice guidelines for the treatment of recurrent breast cancer.31,32 HT increases the temperature of the tumor up to 42 °C to 45 °C using different methods, inducing tumor death. HT is often used in association with CHT or RT and immunotherapy, increasing their efficacy and prolonging their clinical benefits.5,33-35
This beneficial effect is due to heat-induced improvement of CHT delivery, increase of blood flow, and oxygen radical production, while inhibiting hypoxia, angiogenesis, and DNA repair, resulting in enhanced apoptosis of tumor cells.5,33,34
The analysis of the literature shows 9 clinical trials (Table 4) on advanced or recurrent breast cancer treatment with HT combined therapy from 2010 up to 2019.36-44 The association of HT to RT resulted in CR in a range of 52.7% to 76% with local control rates of 53% to 76% at 1 year, 25% to 78% at 3 years, and 39% to 65% at 5 years.36-44
Breast Cancer.
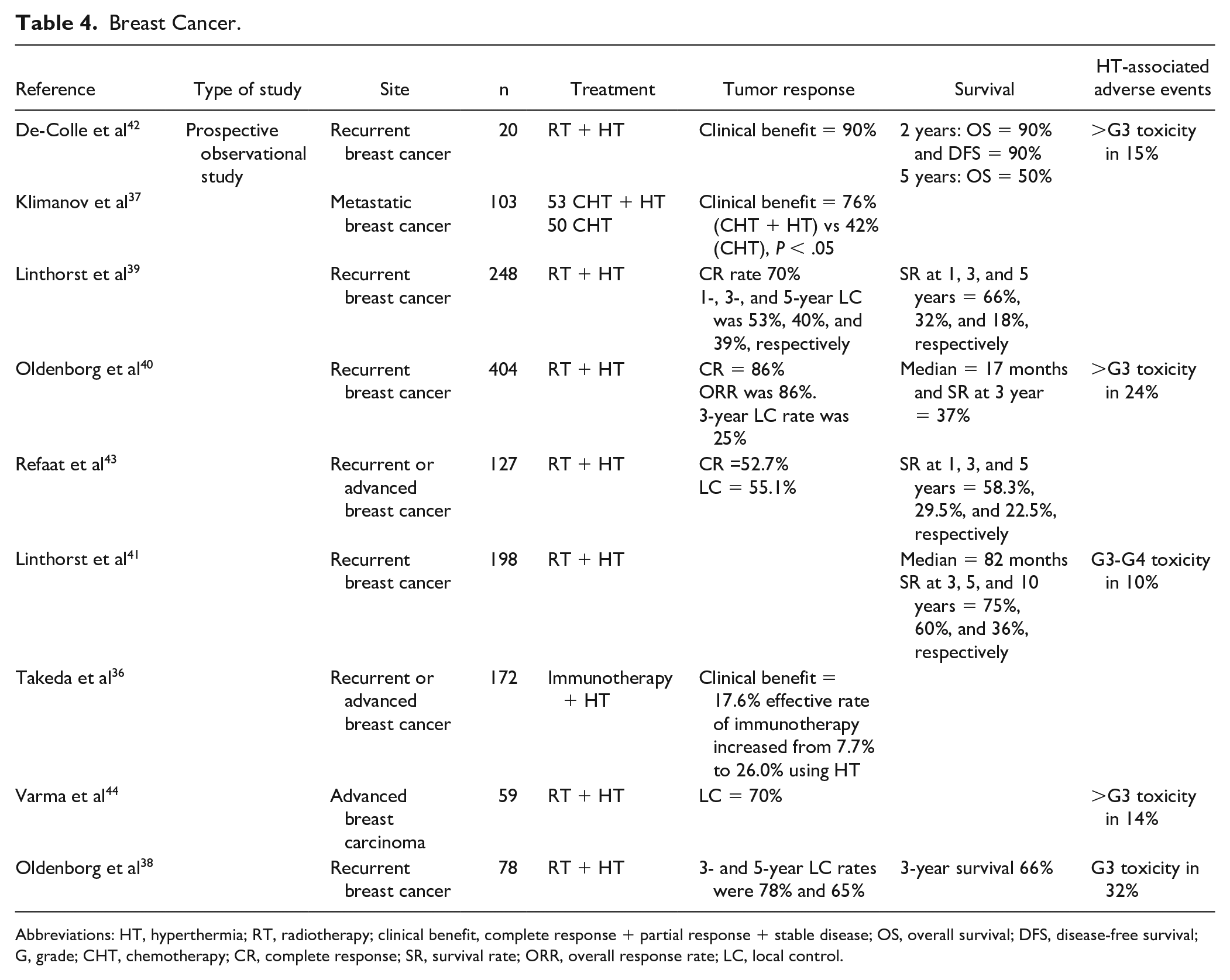
Abbreviations: HT, hyperthermia; RT, radiotherapy; clinical benefit, complete response + partial response + stable disease; OS, overall survival; DFS, disease-free survival; G, grade; CHT, chemotherapy; CR, complete response; SR, survival rate; ORR, overall response rate; LC, local control.
Five studies report the results of survival analysis and show survival rates of 58.3% to 75% at 1 year, 29.5% to 66% at 3 years, 18% to 36% at 5 years, and one study showed also a 10% survival at 10 years. 41
As concerning the toxicity, adverse events (>G3 intensity, according to CTCAE [Common Terminology Criteria for Adverse Events] criteria) are observed in a small portion of patients (10% to 31%) and include thermal burns, ulceration, and osteoradionecrosis.36-41
The combination of re-irradiation and HT results in high tumor response and local control rates that are maintained for up to 10 years in advanced or recurrent breast cancer. This combination, moreover, offers long survival and is well tolerated. For this reason, this combined treatment should be suggested to all patients with advanced or recurrent or at high risk of local recurrence.
The HT in association with CHT is compared with CHT treatment alone in one study. 37 This combination improves the therapeutic efficacy in patients with metastatic breast cancer, resulting in a clinical benefit of 76% versus 42% of CHT alone (P < .05). 37
These data confirm the safety and efficacy of the combination therapy HT/CHT and RT for advanced or recurrent breast cancer in both tumor response and survival; these trials, however, are nonrandomized.36-44
Cervical Cancer
Concomitant cisplatin-based CHT and RT (CRT) improve OS of locally advanced cervical cancer more than RT alone as reported by a review 45 and clinical trials,46-48 even if the prognosis is still poor. 48 HT improves tumor response of CHT-RT in locally advanced cervical cancer.47-52 Several randomized reports HT benefit for locally advanced cervical cancer suggest, including survival improvement and good tolerability (Table 5).47-52
Cervical Cancer.
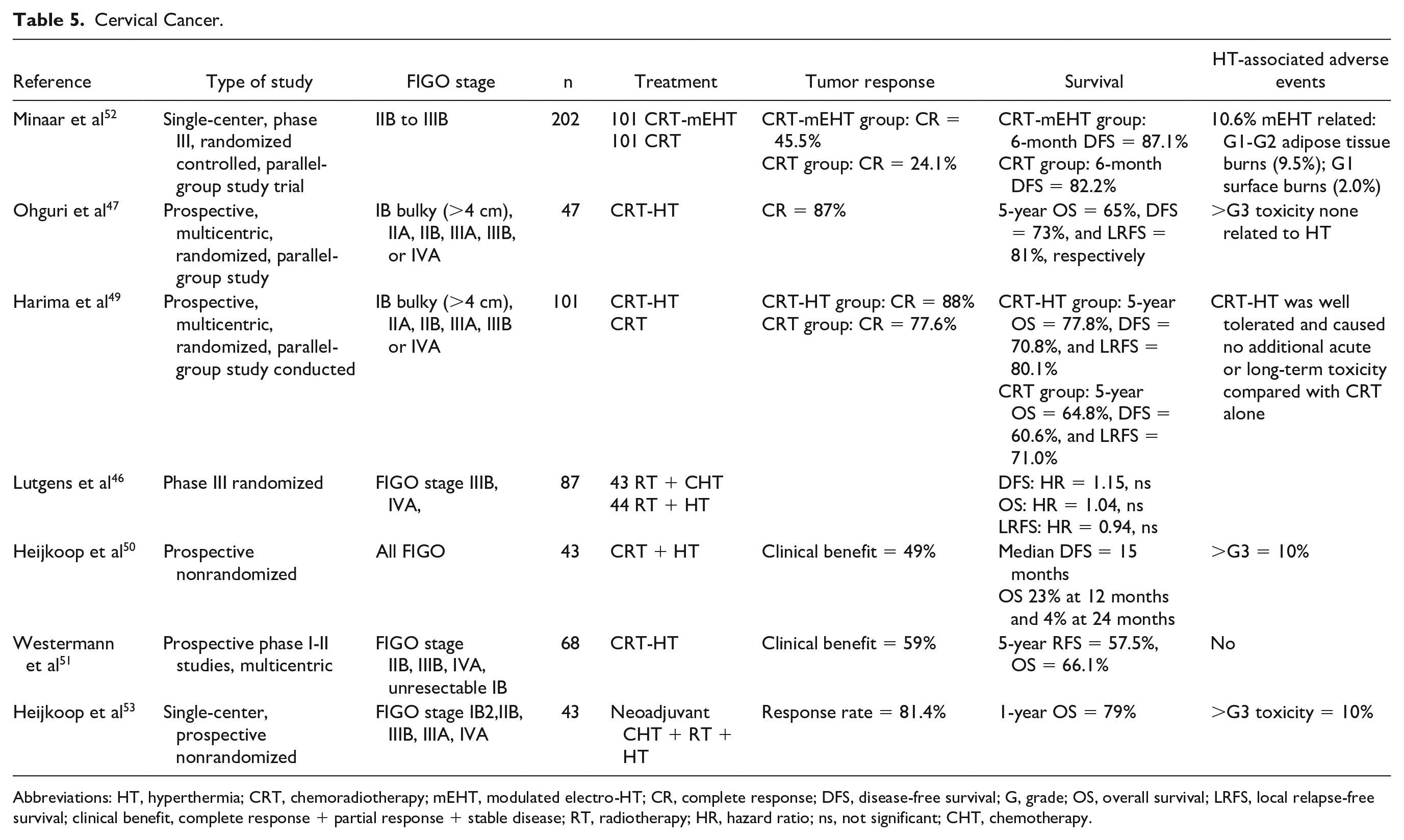
Abbreviations: HT, hyperthermia; CRT, chemoradiotherapy; mEHT, modulated electro-HT; CR, complete response; DFS, disease-free survival; G, grade; OS, overall survival; LRFS, local relapse-free survival; clinical benefit, complete response + partial response + stable disease; RT, radiotherapy; HR, hazard ratio; ns, not significant; CHT, chemotherapy.
All recent studies on CRT and CRT-HT reported possible advantages of HT and mEHT association to CRT.46,47,49-52,53 Two of them show better 5-year OS, disease-free survival (DFS), and local relapse-free survival (LRFS) in the CRT-HT group than those in the CRT group47,49; however, the difference is not statistically significant. CR is significantly higher in the CRT-HT group than that in the CRT group. As concerning safety, the addition of HT is well tolerated, and no additional acute or long-term toxicity is observed than CRT alone.47,49
One of the above-mentioned studies measures the intrarectal temperature with a 4-point micro-thermocouple sensor during regional whole-pelvis HT of locally advanced cervical cancer patients associated to CRT. 47 It shows that higher thermal dose parameter of HT significantly increases LRFS in both univariate (P = .024) and multivariate (P = .0097) analyses. 47 The same result is observed for DFS (P = .071) and tumor response (P = .056). DFS, LRFS, and CR are significantly improved after CRT-HT at higher temperature than CRT alone (P = .036, P = .036, and P = .048). 47 These data suggest a dose-effect correlation between thermal dose parameters and clinical outcomes in locally advanced cervical cancer patients. 47 This correlation is confirmed also in another previous study on 420 patients. 54
The latter study on CRT-HT differentiates the analysis according to nationality and reports 5-year RFS rates of 65.8% for the Dutch patients, 57.4% for Norwegian, and 38.5% for US patients. However, the difference in RFS is significant only between the Netherlands and the United States (P < .01, hazard ratio [HR] = 3.096, 95% confidence interval [CI] = 1.2495-7.671). 51 This may suggest a correlation of HT response to patient characteristics of different countries.
A further study reports the results of CRT associated with mEHT compared with CRT alone for the treatment of FIGO stages IIB to IIIB locally advanced cervical cancer. 52 It reports a higher tumor response for the CRT- mEHT group, CR = 45.5% versus 24.1% of the CRT-alone group (Pearson’s χ2: P = .003) and an improvement in quality of life, in particular as concerning the social functioning (P = .049) and emotional functioning (P = .017) seen in the mEHT group. 52 This difference was observed in both HIV-positive and HIV-negative women. 52 The HT is not associated with an increased toxicity or RT delays and shows reduced posttreatment fatigue and pain at 3 months after therapy. 49
Bladder Cancer
The beneficial effects of HT associated with CHT or RT have been shown also for bladder cancer (Table 6).53,55-57 The induction of regional HT in bladder cancer can be attained with 3 different techniques: 70 to 120 MHz antennas, intracavitary radiofrequency HT using a 916 MHz antenna, and intravesical conductive therapy using a heated perfusate. 56 The use of 70 MHz had higher recurrence-free survival rate than the use of heated perfusate (78% vs 33%). 56
Bladder.

Abbreviations: HT, hyperthermia; RT, radiotherapy; OS, overall survival; DFS, disease-free survival; LRFS, local relapse-free survival; G, grade; CR, complete response; PR, partial response,
Intravesical mitomycin C associated with HT (70 MHz) at mean temperatures of 40.6 °C to 41.6 °C was reported in 2 studies that treated intermediate-/high-risk nonmuscle invasive bladder cancer. The first study showed a CR in 23% and partial response in 15%, and 2-year recurrence-free survival rate was 78%. 58 As concerning the toxicity, adverse event intensity was G1 in 43% of cases and G2 in 14%. 58 The second study showed a 3-year recurrence-free survival rate of 33%. 59 These data suggested that the treatment with mitomycin C and HT in patients with intermediate-/high-risk nonmuscle invasive bladder cancer was effective and safe.58,59
Soft Tissue Sarcoma
Soft tissue sarcoma includes a wide and heterogeneous group of tumors that are derived from connective tissues. Most patients (>80%) present a high-grade histologic type at diagnosis. 55 STS treatment involves a combination of CHT, RT, and resection. 60 In this scenario, regional HT is used to improve CHT and RT efficacy, in terms of PFS, DFS, and tumor response (Table 7). 61 CHT-HT significantly improves local PFS (56% vs 45%, P = .044) and DFS (56% vs 45%, P = 0.044) at 5 years with regard to CHT alone, whereas OS and toxicity do not change significantly between groups. 61 These results suggest an important role of HT in association with CHT for the treatment of abdominal and retroperitoneal high-risk sarcomas after radical surgery. 61
Soft Tissue Sarcoma.
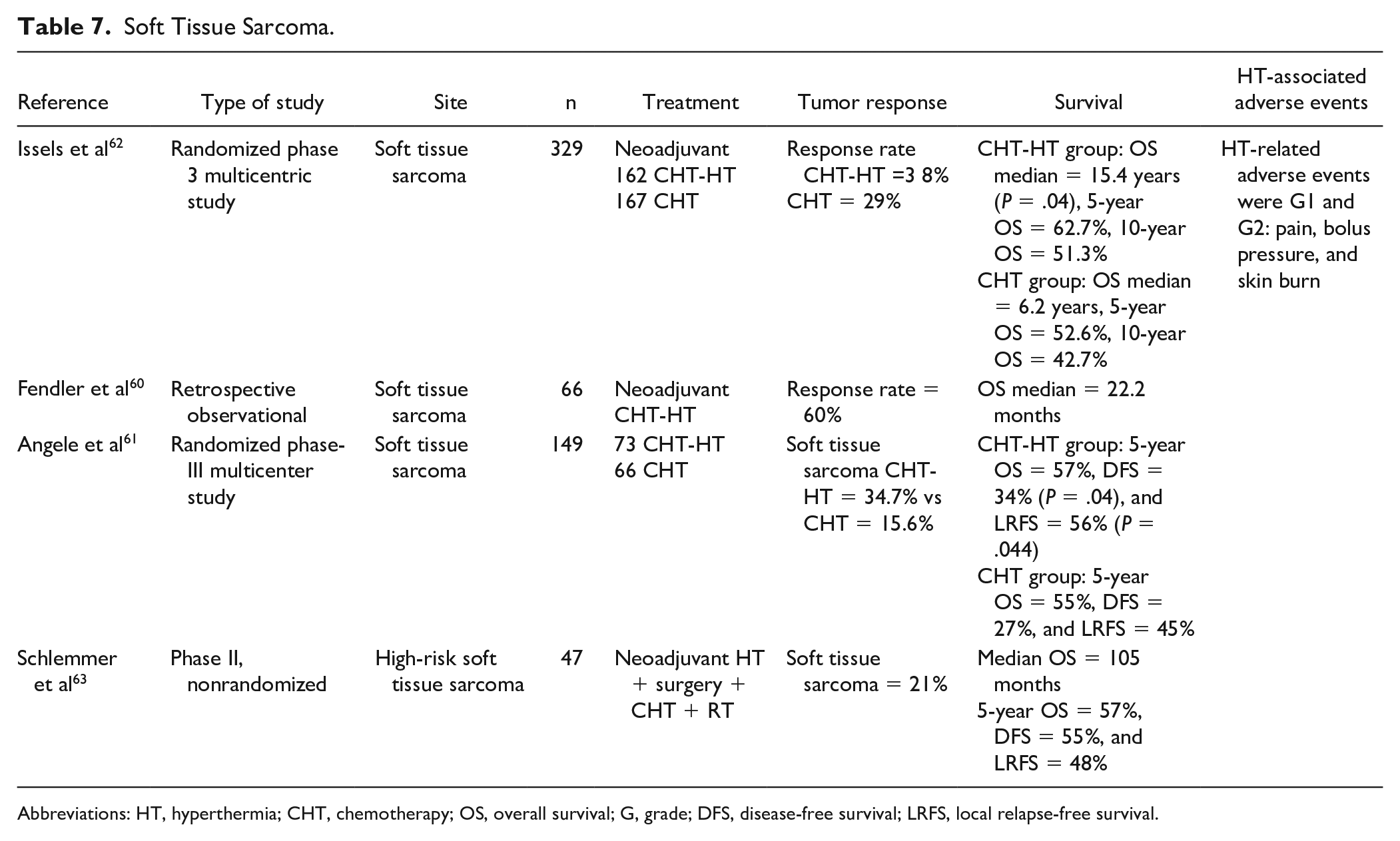
Abbreviations: HT, hyperthermia; CHT, chemotherapy; OS, overall survival; G, grade; DFS, disease-free survival; LRFS, local relapse-free survival.
Hyperthermia has a potential role also in association with neoadjuvant CHT for STS, increasing survival, tumor response, and local PFS.60,62-64 A phase III randomized study shows a 27% OS improvement as a consequence of neoadjuvant CHT + HT versus neoadjuvant CHT alone. 64 Neoadjuvant CHT + HT, in particular, results in a statistically significant improvement of 11.4% and 9.9% in the 5-year and 10-year survival rate, respectively (62.7% vs 51.3% and 52.6% vs 42.7%). 64
Brain Tumors
Glioblastoma multiforme (GBM) is an aggressive brain tumor, representing 45% to 54% of gliomas.65,66 GBM prognosis is still poor, notwithstanding the advances in brain tumor treatment, and median OS ranges between 15 and 18 months. 66 Actually, a standard therapy for recurrent GBM is not yet available; however, emerging results show an advantage of mEHT as an integrative therapy for treatment and not only palliative care of recurrent GBM and astrocytomas (AST; Table 8).67-73
Brain Tumors.
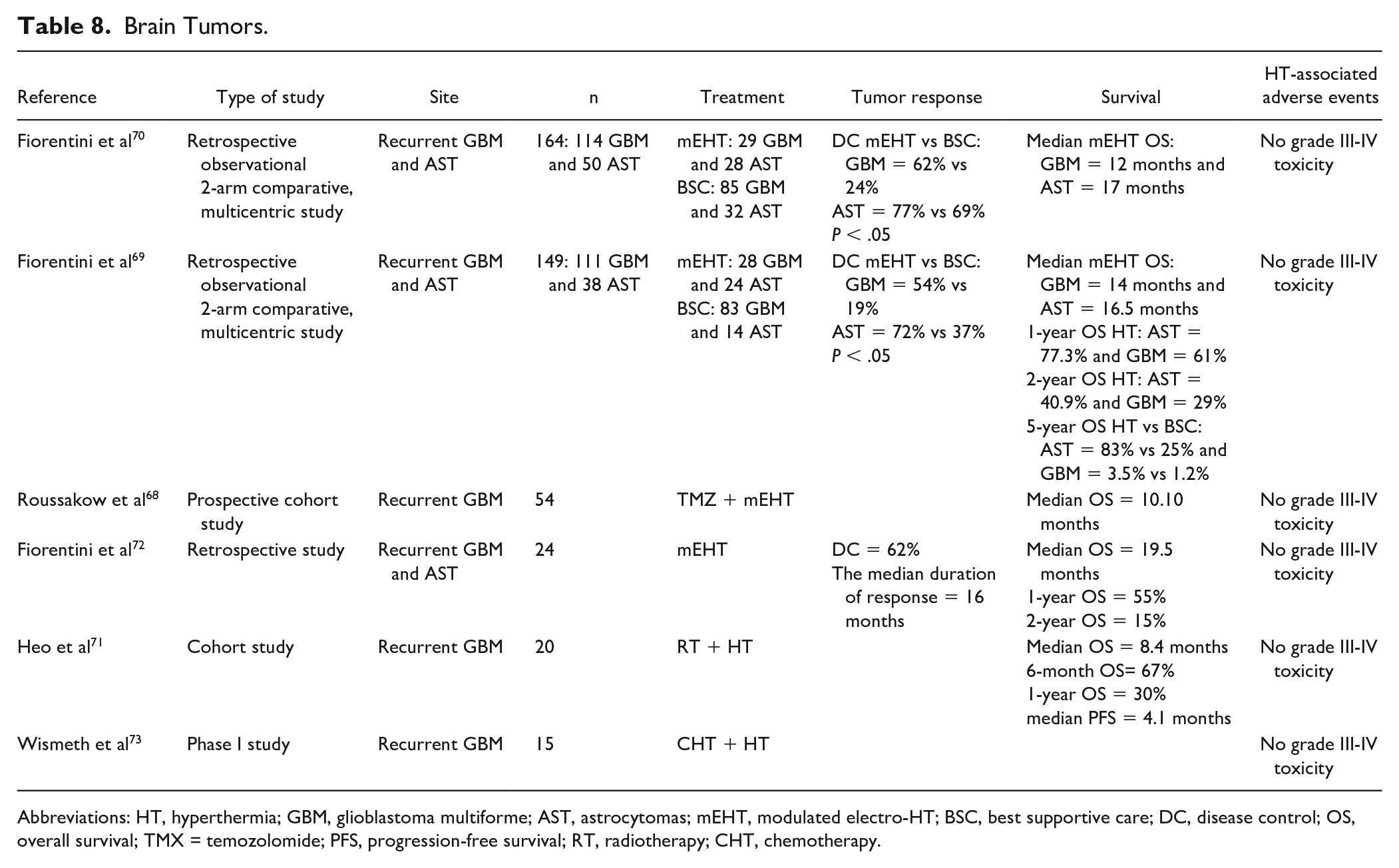
Abbreviations: HT, hyperthermia; GBM, glioblastoma multiforme; AST, astrocytomas; mEHT, modulated electro-HT; BSC, best supportive care; DC, disease control; OS, overall survival; TMX = temozolomide; PFS, progression-free survival; RT, radiotherapy; CHT, chemotherapy.
Available data report a tumor response rate of 24% to 29% for GBM and 43% to 48% for AST 3 months after mEHT, whereas it is 4% for GBM and 10% to 37% for AST in control group.69,70 HT also improves the survival of GBM and AST with a median OS of 12 months (range = 5-108) for GBM, and 17 months for AST. Five-year OS is 83% for AST after mEHT versus 25% after best supportive care and 3.5% for GBM after HT versus 1.2% after best supportive care for GBM. 68 HT also has a low toxicity profile, resulting in no G3 and G4 adverse events.
In conclusion, mEHT may have a beneficial effect on both the treatment and palliation of relapsed GBM and AST in integrative cancer therapy.
Head and Neck Tumors
Radiotherapy + HT is also used in the treatment of head and neck carcinomas, resulting in better CR than RT alone (62.5% vs 39.6%) with comparable toxicity also (Table 9). 74 As concerning nasopharyngeal carcinomas, 3 studies report improved CR, PFS, DFS, and OS for CRT + HT treatment.75-77 This response is temperature-dependent; indeed, patients treated with higher temperatures have a better outcome. 75 In these studies, no difference in toxicity is observed; moreover, patients receiving HT reported a better quality of life after the treatment. 77 Also, re-irradiations combined with HT result in promising tumor response (CR = 46%). 78 These data suggest that the association of HT to CRT is a safe and effective choice of therapy for head and neck tumors. For this reason, HT may be suggested for the treatment of elderly or poorly fit patients to spare the toxicity of more aggressive therapies.
Head and Neck.

Abbreviations: HT, hyperthermia; CRT, chemoradiotherapy; OS, overall survival; PFS, progression-free survival; DFS, disease-free survival; ns, not significant.
Discussion
The available literature includes both retrospective and prospective studies on the benefits of HT association to RT or CRT in several types of tumors, resulting in confirmation of efficacy for the majority of them. 1 These data, however, do not bring the HT to the level of the standard care in many countries. This may be due to different issues, such as reimbursement, technical difficulties and poor proofs of homogenous heating, difficulties in temperature measurements, and a low number of centers performing HT around the world.
There is a need for standardized protocols to be applied in a single tumor type to avoid the current heterogeneity of HT treatments that creates difficulties in comparing the results of different studies. The frequency of HT treatments reviewed varied from once a week to daily and the mean temperature obtained in each treatment varied widely in the range 39 °C to 43 °C. The use of HT at higher temperatures or applied frequencies is correlated with better outcome,47,54 further underlying the need to establish standardized protocols for HT treatments and larger randomized studies on HT variables.
Modulated electro-HT is a modification of conventional HT that targets tumor cell membranes to increase the temperature inside cancer tissue and sensitize it to cancer therapies: RT, CHT, and immunotherapy. 6 Combination therapies of mEHT and CHT or RT are reported by preclinical and clinical studies.6,24,52,68-70 mEHT induces moderate rises in tissue temperatures, improving tumor perfusion, increasing drug absorption and sensitivity to radiation therapy. mEHT is safely used in several types of cancers, such as cervical, brain, and pancreatic tumors, improving local control and survival rates and seems to induce an abscopal (systemic) response to ionizing radiation.24,52,68-70
Applying of HT alone or complementary to other treatments (CHT and/or RT) is assessed in terms of efficacy and tolerability for several types of tumors: esophageal, colorectal, pancreatic, breast, cervix, bladder, and brain tumors, and STS. The data presented confirm the benefits of HT, such as increased tumor response rates, local and distant control rates, and survival in each type of cancer examined. HT was also well tolerated, resulting in a low number and intensity (G1-G2 mainly) adverse events. No cardiac toxicity is reported in any observed study.
CRT + HT, when compared with CRT alone, improves both OS and DC in esophageal cancer with low toxicity.10-12 HT is often used in association with preoperative and neoadjuvant CRT also in locally advanced both nonmetastatic and metastatic colorectal cancer, improving OS and long-term tumor control, resulting in mild toxicity, comparable to that or CRT alone.14,15,20 The same advantages are observed for advanced pancreatic cancer. HT alone or complementary to CRT is, indeed, feasible for both palliative care and therapeutic purposes, increasing OS and improving quality of life for locally advanced pancreas carcinoma.70-73
This HTA reports the available literature to show that there is wide evidence that HT associated with CHT, RT, and immunotherapy for advanced or recurrent breast cancer brings about improvements in both tumor response and OS that are maintained for a long time (up to 10 years).36-44
Successful use of HT is also shown for cervical cancer, improving tumor response rates and quality of life in both social and emotional functioning. 52 It is observed, moreover, that there is a dose-effect correlation between thermal dose parameters and clinical outcomes and that HT response may be modified by patient characteristics in different countries.47,51,54
Fewer studies are available on the use of HT for bladder cancer treatment. Their data, nevertheless, confirm the positive effects of HT associated with intravesical mitomycin C in terms of CR and PFS in bladder cancer.57-59
As concerning STS, the association of HT with RT or CHT improves local PFS and DFS after radical surgery. 61 The same benefits are observed when HT is used in the neoadjuvant setting, resulting also in higher response rates.60,62-65
Available literature shows that HT may have a beneficial effect for both treatment and palliation of relapsed GBM and AST and is a valid option for integrative cancer therapy.68-73 Improvements of CR, PFS, DFS, and OS are observed also for head and neck tumor treatment for HT associated with CRT and re-irradiation.75-77 In these studies, no difference in toxicity is observed and patients receiving HT reported a better quality of life, suggesting that the association of HT to CRT is a safe and effective choice of therapy for head and neck tumors.
Constant improvement of HT includes heat delivery, treatment planning, and monitoring of efficacy and toxicity. HT associated with new targeted therapies, immunotherapy, nanomedicine, or particle therapy may represent new fields of future research and clinical application.
The main limitation of this review is that the quality of the articles was not assessed as it would be in systematic review or meta-analysis.
Conclusion
There are numerous clinical studies that show good feasibility and efficacy of HT and mEHT in terms of tumor response and survival improvements in several tumor types, such as gastrointestinal and other malignancies. HT and mEHT can be successfully applied in association with CHT, RT, and CRT for the treatment of recurrent disease.
In conclusion, HT in combination with other therapeutic modalities results in better outcomes concerning both tumor response and survival and is associated with low-grade toxicity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.