
Abstract
Background:
Integrative therapies reduce side effects from cancer treatment, though remain underutilized. There is a paucity of data on factors associated with familiarity, interest, and use of these therapies among breast cancer patients.
Methods:
A survey on familiarity, interest, and use of acupuncture, massage, meditation, music therapy, and yoga was conducted in patients enrolled in the Chicago Multiethnic Epidemiologic Breast Cancer Cohort. Familiarity and interest were assessed using a five-point Likert scale, and modeled using proportional odds regression. Use was per self-report, modeled using logistic regression. Adjusted odds ratios (aOR) and 95% confidence intervals (95% CI) were calculated.
Results:
Of 1300 study participants, 59.6% were familiar with massage, 47.2% acupuncture, 46.9% meditation, 46.5% yoga, and 34.5% music therapy; 63.3% were interested in massage, 50.2% yoga, 47.9% meditation, 44.2% acupuncture, and 41.4% music therapy. Only 41.3% had used massage, 25.8% acupuncture, 18.7% yoga, 18.5% meditation, and 7.4% music therapy. Older age and lower education level were associated with lower familiarity and interest. Black patients were more likely than White patients to be interested. Patients’ interest increased significantly when certain symptoms were treated. In the adjusted models, patients ages 40 to 65 were less likely than those ages <40 to have used massage (aOR 0.55, 95% CI: 0.31-0.98), yoga (aOR 0.52, 95% CI: 0.27-0.99), or meditation (aOR 0.47, 95% CI: 0.25-0.90). Patients with high school education were less likely than those with a graduate degree to have used acupuncture (aOR 0.42, 95% CI: 0.24-0.72), massage (aOR 0.39, 95% CI: 0.25-0.62), or meditation (aOR 0.26, 95% CI: 0.12-0.58). Having received chemotherapy was associated with increased interest in yoga (aOR 1.36, 95% CI: 1.07-1.73), massage (aOR 1.27, 95% CI: 1.01-1.59), or meditation (aOR 1.26, 95% CI: 1.01-1.57). Receipt of hormone therapy was not associated with interest or use.
Conclusion:
In this racially diverse cohort of patients, familiarity and interest of integrative therapies were high, while use was low. Older age and lower education level were associated with lack of interest and use. Chemotherapy was associated with interest, but hormone therapy was not. Strategies to promote the benefits and use of integrative therapies among breast cancer patients are needed.
Introduction
The treatment of breast cancer causes many common short- and long-term side effects and symptoms such as nausea, vomiting, hot flashes, chemotherapy-induced peripheral neuropathy, pain, depression, insomnia, and fatigue. 1 These side effects and symptoms can negatively affect breast cancer patients’ quality of life and adherence to cancer treatment. 2 Although pharmacologic interventions can help reduce side effects and improve symptoms, they often cause additional adverse effects. Integrative therapies, including acupuncture, therapeutic massage, meditation, music therapy, and yoga, have been shown to alleviate side effects and symptoms from cancer treatment modalities.3-5 In 2018, the American Society of Clinical Oncology (ASCO) endorsed Society for Integrative Oncology (SIO)’s clinical practice guidelines regarding the evidence-based use of integrative therapies for the management of side effects and symptoms during and after breast cancer treatment.3,6 In the guidelines, acupuncture is recommended for controlling hot flashes and nausea; meditation, therapeutic massage, and music therapy are recommended for treating anxiety and depressive symptoms; and meditation and yoga are recommended for improving the quality of life of breast cancer patients. 6
Integrative therapies are not unfamiliar to cancer patients and their caregivers, as Larbi et al reported that more than 50% were familiar or very familiar with acupuncture, yoga, or meditation. 7 Several studies also have indicated prevalent interest in and increasing demand for integrative medicine among patients with breast or gynecological cancers, but the study populations are limited to patients who are Caucasian.8-10 Cancer patients use integrative therapies during and beyond cancer treatment to reduce side effects, manage symptoms, and improve their quality of life, and are more likely than the general population to have used these therapies. 11 Although 45 National Cancer Institute-designated cancer centers in the United States (U.S.) offer various types of complementary and/or integrative therapies to their patients, 12 integrative therapies remain underutilized. A small survey study has documented that 25% and 22% of cancer survivors have used or are currently using meditation and massage, respectively, with the vast majority (96%) of survey participants being White. 13 Another study has also found that 19.1% of cancer patients are currently using meditation, followed by 17.9% massage, 13.5% yoga, and only 5.6% acupuncture. 14 Although 44% of the study participants were African American, there were only 165 patients in total. To summarize, there is a paucity of data on the demographic and clinical characteristics associated with familiarity, interest, and use of these therapies among breast cancer patients in the U.S.
Previous studies are descriptive in nature due to limited sample sizes and include patients with different cancer types or mostly White. Thus, the findings may not be generalizable specifically to the breast cancer patient population. To address this gap in the literature, using data obtained from a large, multiethnic cohort of patients with breast cancer, we sought to estimate the prevalence of familiarity, of interest, and of use of 5 integrative therapy modalities (i.e., acupuncture, therapeutic massage, meditation, music therapy, and yoga); explored facilitating factors for interest in and barriers to using these therapies; and examined the demographic and clinical characteristics that were associated with familiarity, interest, and use of these therapies.
Materials and Methods
Study Design and Population
This was a cross-sectional study conducted in breast cancer patients who were enrolled in the Chicago Multiethnic Epidemiologic Breast Cancer Cohort (ChiMEC). ChiMEC is a hospital-based study that has a total enrollment of more than 5000 patients who were diagnosed with breast cancer since 1993. Details on ChiMEC have been described elsewhere. 15 During July and September 2021, a total of 2788 questionnaires were sent to ChiMEC participants who consented to follow-up surveys via Research Electronic Data Capture at the University of Chicago.16,17 All patients provided written informed consent. Approval of the study was granted by the Institutional Review Board at the University of Chicago.
Measures
Patients with breast cancer responded to the questionnaire regarding their familiarity, interest, and past use of 5 integrative therapies: acupuncture, therapeutic massage, meditation, music therapy, and yoga. Familiarity was assessed by asking how familiar participants were with these therapies, using a five-point Likert scale (i.e., not familiar at all, not very familiar, neutral, familiar, and very familiar). Interest was assessed by asking how interested participants would be in these therapies if offered at the University of Chicago Medicine, using a five-point Likert scale (i.e., not interested at all, not very interested, neutral, interested, and very interested). Use was assessed by asking whether or not participants had received these therapies in the past, and was self-reported as either yes or no.
To explore symptoms as facilitating factors for interest in any therapy use, we asked participants how interested they would be if an integrative therapy modality specifically treated hot flashes, chemotherapy-induced neuropathy, nausea, joint, back or other pain, depression, fatigue, or anxiety, using the same five-point Likert scale aforementioned. Other facilitating factors were also assessed, including recommendations from your doctor or nurse, cost not being a barrier, being covered by health insurance, and price willing to pay out-of-pocket for a session. Additionally, barriers such as cost, lack of access to services, lack of transportation to service-providing facilities, lack of time, lack of interest, unaware of the benefits of these services, low confidence about the benefits, and lack of trusted information were assessed by asking participants what generally prevents them from using any of these therapies.
Demographic and clinical characteristics were collected from the baseline questionnaire or ascertained via patients’ electronic health records, including age, race/ethnicity (Asian, Black, Hispanic, and White), highest level of education (High school/GED or less, post high school, trade/technical school, or some college, associate’s degree, bachelor’s degree, and graduate or professional degree), marital status, annual household income (<$50 000, $50 000-$74 999, $75 000-$99 999, $100 000-$149 999, $150 000-$199 999, and ≥$200 000), type of health insurance (Medicaid, Medicare, private, and other), history of tobacco use, history of alcohol consumption, duration from diagnosis to survey, Charlson comorbidity index, 18 molecular subtype (hormone receptors-positive/human epidermal growth factor receptor 2-negative [HR+/HER2-], HER2+, and triple negative breast cancer [TNBC]), American Joint Committee on Cancer’s stage group, receipt of chemotherapy, receipt of radiation therapy, and receipt of hormone therapy. Age was measured at the time of survey, categorized into 3 age groups: <40 years, 40 to 65 years, and >65 years. Marital status was documented at the time of cancer diagnosis. Duration from diagnosis to survey was defined as the duration from cancer diagnosis to survey administration, dichotomized as ≤6 years and >6 years based on the distribution of the sample.
Statistical Analysis
Descriptive statistics were used to summarize the characteristics of the sample. Specifically, means (standard deviations [SD]) were calculated for continuous data, and frequencies (percentages [%]) were tabulated for categorical data. Bivariate analyses were conducted using Student’s t tests or ANOVA for continuous variables and Pearson’s Chi-square or Fisher’s exact tests for categorical variables. Familiarity and interest, considered ordinal outcomes, were modeled using multivariable proportional odds models. The proportional odds assumption was evaluated for each model based on the score test statistic, and no violations were observed for all models. Past use, as a binary outcome, was modeled using multivariable binary logistic regression. Variables with a P-value < .05 in bivariate analyses were selected for multivariable regression models. Further, only significant covariates, as per the global null hypothesis testing, were included in the final models. To address multiple hypothesis testing, we implemented the Bonferroni correction and considered P-values of <0.002 (0.05/25) as statistical significance after multiple testing correction and P-values of <0.05 as nominal significance. Adjusted odds ratios (aOR) and 95% confidence intervals (95% CI) were calculated to elucidate the association of demographic and clinical characteristics with familiarity, interest, and use of integrative therapies. All analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC).
Results
Demographic and Clinical Characteristics
A total of 1300 patients with breast cancer responded to the survey. Of these, 99.6% were female, the mean age was 61.2 (SD 11.7) years, 71.4% were White and 21.9% were Black, 39.3% had obtained a graduate or professional degree, 69.6% were married, 20.0% had an annual household income of less than $50 000, 74.8% had private insurance and 18.5% were on Medicare, 56.5% reported as being a current alcohol drinker, 65.8% had a molecular subtype of HR+/HER2-, 45.3% had AJCC stage I tumor, 44.9% received chemotherapy, and 67.8% received hormone therapy (Table 1).
Demographic, Behavioral, and Clinical Characteristics of Patients With Breast Cancer (N = 1300).

Abbreviations: SD, standard deviation; GED, general educational development; HR, hormone receptors; HER2, human epidermal growth factor receptor 2; TNBC, triple-negative breast cancer.
Age was measured at the time of survey.
Marital status was documented at the time of cancer diagnosis.
Other included 1 uninsured/self-pay, 17 insurance not otherwise specified, 1 TRICARE, and 1 Military.
Tobacco products assessed included cigarette, cigar, pipe, snuff, chew, smokeless, or mixed use with more than one type.
Duration from diagnosis to survey was defined as the duration from the time of cancer diagnosis to the time of survey.
Stage group was defined based on the American Joint Committee on Cancer’s cancer staging.
Familiarity
Overall, 59.6% of the patients were familiar or very familiar with therapeutic massage, followed by acupuncture (47.2%), meditation (46.9%), yoga (46.5%), and music therapy (34.5%) (Table 2). In bivariate analyses, significant differences in familiarity with any of these therapies were observed for age group, race/ethnicity, highest level of education, annual household income, and type of health insurance (Supplemental Table 1). In the adjusted proportional odds models (Supplemental Table 2), characteristics associated with lower odds of being familiar with these therapies were older age, lower level of education, marital status as widowed, and duration from diagnosis to survey ≤6 years. It is worth noting that Black (aOR 0.68, 95% CI: 0.51-0.91) or Hispanic (aOR 0.44, 95% CI: 0.23-0.82) patients were less likely than their White counterparts to be familiar with acupuncture. Compared with patients who had stage 0 disease, those who had stage I (aOR 0.70, 95% CI: 0.52-0.93) or stage II (aOR 0.65, 95% CI: 0.47-0.89) were less likely to be familiar with meditation. (Supplemental Table 2).
Familiarity, Interest, and Use of Integrative Therapies Among Patients With Breast Cancer (N = 1300).

Abbreviations: SD, standard deviation.
Familiarity was assessed by asking participants how familiar they were with these integrative therapies.
Interest was assessed by asking participants how interested they would be in these integrative therapies if offered at the center.
Participants were asked about these integrative therapies they have used in the past.
Interest and Symptoms as Facilitators
Overall, 63.3% of the breast cancer patients were interested or very interested in therapeutic massage, followed by 50.2% yoga, 47.9% meditation, 44.2% acupuncture, and 41.4% music therapy (Table 2). As shown in Figure 1, higher percentages of the patients reported being interested or very interested in any therapy use if it specifically treated joint pain (67.6%), back or other pain (67.6%), fatigue (64.0%), anxiety (63.3%), depression (52.2%), hot flashes (45.5%), chemotherapy-induced neuropathy (39.2%), and nausea (30.3%). More than half of the patients were interested or very interested in any of these therapies if their doctors or nurses recommended it, if cost was not a barrier, or if being covered by health insurance (Table 3). Prices willing to pay out-of-pocket for a session reported most were between $0-$39 (Table 3). In bivariate analyses, significant differences in interest across the 5 therapies were observed for age group, marital status, type of health insurance, and receipt of chemotherapy; when comparing levels of education, there were significant differences in interest in these therapies, except for music therapy; racial/ethnic differences in interest were also observed for all therapies except for acupuncture (Supplemental Table 3).

Symptoms as facilitators for interest in the use of any integrative therapy among patients with breast cancer (N = 1300).
Facilitators for Interest in Use of Integrative Therapies Among Patients With Breast Cancer (N = 1300).
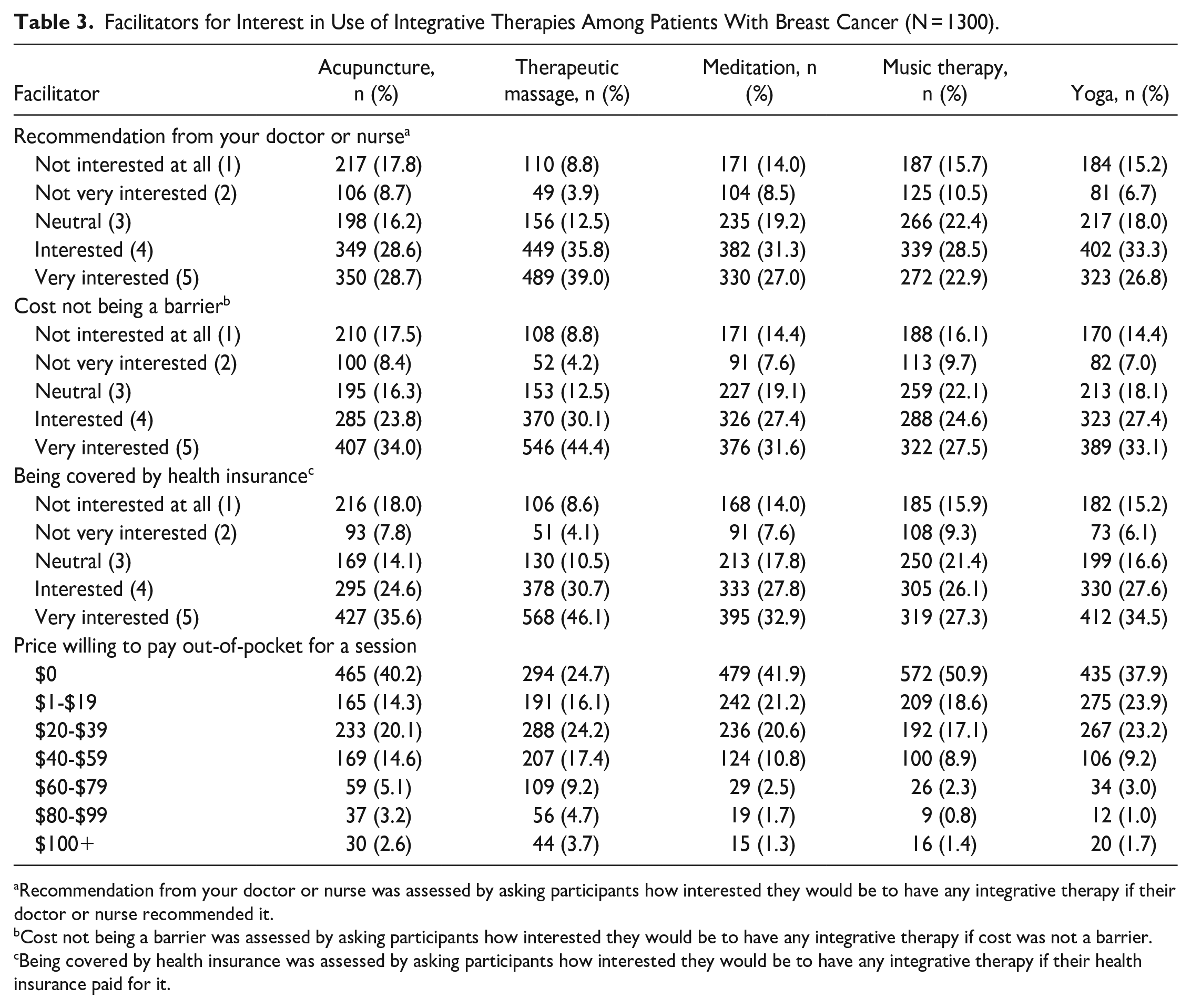
Recommendation from your doctor or nurse was assessed by asking participants how interested they would be to have any integrative therapy if their doctor or nurse recommended it.
Cost not being a barrier was assessed by asking participants how interested they would be to have any integrative therapy if cost was not a barrier.
Being covered by health insurance was assessed by asking participants how interested they would be to have any integrative therapy if their health insurance paid for it.
In multivariable proportional odds models (Table 4), we observed that overall, patients with older ages were less interested in the 5 integrative therapy modalities. In particular, patients aged >65 years were less likely than those aged <40 years to be more interested in meditation (aOR 0.34, 95% CI: 0.19-0.60), acupuncture (aOR 0.29, 95% CI: 0.16-0.51), or therapeutic massage (aOR 0.22, 95% CI: 0.12-0.40). Compared with White patients, Black patients had higher odds of being more interested in music therapy (aOR 2.47, 95% CI: 1.89-3.22), meditation (aOR 2.16, 95% CI: 1.64-2.85), yoga (aOR 1.98, 95% CI: 1.47-2.68), or therapeutic massage (aOR 1.86, 95% CI: 1.41-2.46). Patients with high school/GED or less education were less likely than those with a graduate or professional degree to be interested in meditation (aOR 0.57, 95% CI: 0.39-0.84). Patients who received chemotherapy were more likely to be more interested in yoga (aOR 1.36, 95% CI: 1.07-1.73), therapeutic massage (aOR 1.27, 95% CI: 1.01-1.59), or meditation (aOR 1.26, 95% CI: 1.01-1.57) than those who did not receive chemotherapy (Table 4). However, there was no association between receipt of hormone therapy and interest in using integrative therapies.
Multivariable Proportional Odds Models of Characteristics and Interest in Use of Integrative Therapies Among Patients With Breast Cancer (N = 1300).

Abbreviations: aOR, adjusted odds ratio; CI, confidence interval; GED, general educational development.
Bold font indicates statistically significant results.
Adjusted for age, highest level of education, history of alcohol consumption, and chemotherapy.
Adjusted for age, race/ethnicity, highest level of education, and chemotherapy.
Adjusted for age, race/ethnicity, highest level of education, and chemotherapy.
Adjusted for age, race/ethnicity, and highest level of education.
Adjusted for age, race/ethnicity, highest level of education, history of alcohol consumption, and chemotherapy.
P < .05. **P < .01. †P<.002. ‡P<.0001.
Past Use and Barriers
Overall, 41.3% had used therapeutic massage, 25.8% had used acupuncture, 18.7% had used yoga, 18.5% had used meditation, and only 7.4% had used music therapy, in the past (Table 2). As illustrated in Supplemental Figure 1, high percentages of patients reported that cost (37.5%), lack of time (30.4%), unaware of benefits of these services (27.2%), and lack of access to services (19.9%) were barriers to using integrative therapies. In bivariate analyses, significant differences in past use of these 5 therapies were observed for level of education. There were significant differences in past use of all therapies, except for meditation, when comparing levels of annual household income. Significant differences in past use of any therapy were also observed for age group, race/ethnicity, and type of health insurance (Supplemental Table 4).
In adjusted logistic regression analyses (Table 5), younger age was significantly associated with past use of 4 integrative therapy modalities: therapeutic massage, yoga, meditation, and music therapy. Black patients were less likely than their White counterparts to have used acupuncture (aOR 0.51, 95% CI: 0.35-0.73). Level of education was positively associated with the use of 4 integrative therapy modalities. Compared with patients with a graduate or professional degree, those with high school/GED or less education were less likely to have used therapeutic massage (aOR 0.39, 95% CI: 0.25-0.62), meditation (aOR 0.26, 95% CI: 0.12-0.58), or yoga (aOR 0.18, 95% CI: 0.07-0.46). An association between receipt of chemotherapy or hormone therapy and use of these therapies was not observed.
Multivariable Binary Logistic Regression Models of Characteristics and Use of Integrative Therapies Among Patients With Breast Cancer (N = 1300).

Abbreviations: aOR, adjusted odds ratio; CI, confidence interval; GED, general educational development.
Bold font indicates statistically significant results.
Adjusted for race/ethnicity and highest level of education.
Adjusted for age and highest level of education.
Adjusted for age, highest level of education, and history of alcohol consumption.
Adjusted for age and annual household income.
Adjusted for age, race/ethnicity, and highest level of education.
P < .05. **P < .01. †P<.002. ‡P<.0001.
Discussion
In this study of a racially diverse sample of patients with breast cancer, high proportions of the patients were familiar with and interested in integrative therapies, but the use of these therapies was low. Demographic characteristics associated with lower interest or use of these therapies were older age groups and lower levels of education, which are consistent with existing literature.7,10,13,19 This finding can be supported in part by our findings that older breast cancer patients were less familiar with meditation and yoga, and patients with high school/GED or less education were less familiar with all 5 modalities. Although familiarity with integrative therapies was prevalent overall, 47.0% were still not familiar with music therapy, followed by 40.2% acupuncture, 36.8% yoga, 36.6% meditation, and 29.0% therapeutic massage. When patients were asked to report their interest in use of any integrative therapy modality if they were treated for a specific symptom, the proportions of being interested significantly increased. One published study has demonstrated that the use of acupuncture and massage markedly increases when patients experience back, joint, neck, or other pain. 20 This study interviewed patients with chronic diseases including cancer, not breast cancer patients in particular. We did not assess the relationships between these symptoms and integrative therapy use, which is worth doing in future research. Patients’ interest in these therapies also increased if their doctors or nurses recommended it, if cost was not a barrier, and if being covered by their health insurance. Most patients reported their willingness to pay $0-$39 out-of-pocket for a therapy session. One in 3 patients reported cost as a major barrier, while 1 in 4 patients reported being unaware of the benefits of integrative therapies as a barrier, suggesting that comprehensive cancer centers should provide patient education on integrative therapies and associated benefits among breast cancer patients, and these services should be covered as part of standard cancer care.
We found that Black breast cancer patients were less familiar with acupuncture than their White counterparts. Similarly, Hispanic patients were also less likely than White patients to be familiar with acupuncture. Black patients were twice as likely as White patients to be more interested in the use of therapeutic massage, meditation, music therapy, or yoga; however, they were less likely to have used acupuncture and yoga. Asian patients also were 2 times more likely than their White counterparts to be more interested in Yoga. A recent study of familiarity and interest of integrative therapies among cancer patients and their caregivers found that non-White patients were less likely than White patients to be familiar with therapeutic massage, with no significant differences in familiarity with other therapy modalities and in interest, possibly due to its small sample size. 7 Moreover, we found that 1 in 5 patients reported lack of access to these services, while 1 in 10 patients reported lack of transportation to service-providing facilities. Our results indicate unmet needs for integrative therapies among patients with breast cancer, especially among racial and ethnic minorities, and underscore the importance of equitable service access for all patients. It is worth exploring factors that contribute to racial and ethnic disparities in the use of these therapies in future research.
Another important finding is that breast cancer patients who received chemotherapy were more interested in using integrative therapies, specifically therapeutic massage, meditation, and yoga, which aligns with previous research.8,10 Hack et al reported that 1 in 2 breast cancer patients had used integrative medicine in the past. However, their analysis was limited to only post-menopausal HR + breast cancer patients who received neo-adjuvant chemotherapy, 10 whereas we included patients with all molecular subtypes and having received neo-adjuvant or adjuvant chemotherapy. We did not observe an association between receipt of chemotherapy and use of any integrative therapy. Interestingly, receipt of hormone therapy was not associated with either interest or use of these therapies in our study. Notably, integrative therapies have demonstrated benefits in managing hormone therapy-associated side effects and symptoms such as hot flashes, depression, fatigue, sleep disturbances, and nausea. Our findings suggest the lack of awareness to use integrative therapies to alleviate side effects and symptoms associated with chemotherapy and hormone therapy. Therefore, patients who receive either cancer treatment should be counseled on the benefits of integrative therapies with the goal of helping them reduce side effects and manage symptoms. In addition, raising awareness could lead to improved adherence to breast cancer treatment and an enhancement in quality of life post-treatment. However, we did not assess whether the patients had used these integrative therapies before, during, or after their cancer treatments, and thus, future research should investigate whether there are differences in usage between these time points and how such differences would affect cancer treatment adherence and quality of life.
There are several limitations to this study. First, the survey data were self-reported, which is prone to recall error or social desirability bias. However, such bias is probably minimal given the limited patient-staff interaction that would influence their survey responses. Second, we did not assess whether patients had used these integrative therapies prior to their cancer diagnoses or during or after their cancer treatments. Furthermore, the data only included breast cancer patients who were willing to participate in the study, with an approximately 47% response rate. Therefore, our prevalence estimates may have been overestimated or underestimated. Third, we were not able to assess unmeasured factors (e.g., cultural background/influence, employment status) that could potentially affect or better explain the associations we observed in this analysis. Lastly, ChiMEC participants may not be representative of all patients with breast cancer in the U.S. and thus limiting the generalizability of our findings. Despite the aforementioned limitations, this study has 2 major strengths. One pertains to its large, racially diverse sample of patients with breast cancer patients. Another strength of the study is the inclusion of many key clinical characteristics and treatments related to breast cancer.
Conclusions
In this multiethnic cohort of patients with breast cancer, we showed that familiarity and interest of integrative therapies were high, however, self-reported past use of these therapies was low. Many patients expressed their interest in integrative therapy use when certain symptoms were specified to be addressed. Older age and lower level of education were associated with lack of interest and actual use of these integrative therapy modalities. Receipt of chemotherapy was associated with increased interest in integrative therapies, while receipt of hormone therapy was not associated with either interest or use. Strategies to promote the benefits and use of integrative therapies among breast cancer patients, particularly among those who are older, have a lower level of education, and receive chemotherapy or hormone therapy alone, in health care and services settings are needed.
Supplemental Material
sj-docx-1-ict-10.1177_15347354231185122 – Supplemental material for Demographic and Clinical Characteristics Associated With Familiarity, Interest, and Use of Integrative Therapies Among Patients With Breast Cancer
Supplemental material, sj-docx-1-ict-10.1177_15347354231185122 for Demographic and Clinical Characteristics Associated With Familiarity, Interest, and Use of Integrative Therapies Among Patients With Breast Cancer by Jincong Q. Freeman, Jori Sheade, Fangyuan Zhao, Olufunmilayo I. Olopade, Rita Nanda and Dezheng Huo in Integrative Cancer Therapies
Footnotes
Acknowledgements
We are grateful to the participants enrolled in the Chicago Multiethnic Epidemiologic Breast Cancer Cohort and the staff in our research team. We thank the Iannessa family for their generous donation to support this study and our acupuncture program at the University of Chicago Medicine.
Author Contributions
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jincong Q. Freeman, Jori Sheade, Fangyuan Zhao, and Dezheng Huo declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Rita Nanda declared advisory board involvement with and research funding from Arvinas, AstraZeneca, BeyondSpring, Celgene, FujiFilm, Genentech/Roche, Gilead, Infinity, iTeos, Merck, OBI Pharma, OncoSec, Pfizer, Relay Therapeutics, SeaGen, Sun Pharma, and Taiho. Olufunmilayo Olopade declared financial relationships with CancerIQ, 54gnene, HealthWell Solutions, Tempus; research funding from Ayala Pharmaceuticals, Cepheid, Color Genomics, Novartis, and Roche/Genentech.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by a donation from the Iannessa family, the National Cancer Institute (P20CA233307), and the Breast Cancer Research Foundation (BCRF-22-071).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.