
Abstract
Oxidative stress is a key component in carcinogenesis. Although radiation produces reactive oxygen species, some anticancer agents such as alkylating agents, platinum and antitumor antibiotics exert cytotoxicity by generating free radicals. Nonenzymatic exogenous antioxidants such as vitamins, minerals, and polyphenols can quench ROS activity. However, whether antioxidants alter antitumor effects during radiotherapy and some types of chemotherapy remains unclear. In the present study, we reviewed antioxidants as an adjuvant therapy for cancer patients during chemotherapy or radiotherapy. Electronic literature searches were performed to select all randomized controlled clinical trials (RCTs) in which antioxidants were administered to cancer patients along with chemotherapy or radiotherapy. Articles or abstracts written in English were included. In total, 399 reports received primary screening. Duplicated articles and those meeting the exclusion criteria (not RCT, not human, and no oral administration) were excluded. Finally, 49 reports matching the inclusion criteria were included. It was difficult to determine whether antioxidants affect treatment outcomes or whether antioxidants ameliorate adverse effects induced by chemotherapy and radiotherapy. It is desirable to use an evidence-based method to select supplements best suited to cancer patients. Although there are many opinions about risks or benefits of antioxidant supplementation, we could mostly conclude that the harm caused by antioxidant supplementation remains unclear for patients during cancer therapy, except for smokers undergoing radiotherapy.
Introduction
Cancer is the leading cause of death worldwide. Although outcomes of cancer therapy have improved, cancer becomes a systemic disease beyond a particular point. Because complete recovery of cancer patients following a single treatment is quite difficult, a multidisciplinary approach combined with surgery, chemotherapy, radiotherapy, and immunotherapy is usually utilized. 1
Other approaches using complementary and alternative medicine (CAM) modalities are an important choice among cancer patients. Hyodo et al 2 reported that 44.6% of cancer patients use CAM treatments in Japan. Patients undergoing chemotherapy tend to prefer CAM, particularly dietary supplements. However, it is not common for clinicians to use CAM as a general therapy in Japan because of the uncertainty regarding the safety and effects of CAM therapies.
Oxidative stress is a key component in the carcinogenesis process. 3 Stimulated by endogenous and exogenous factors, reactive oxygen species (ROS) induce cellular damage. 3 Although radiation certainly produces ROS, some anticancer agents such as alkylating agents and platinum and antitumor antibiotics exert cytotoxicity by generating free radicals. Some endogenous antioxidant defense mechanisms, such as superoxide dismutase, glutathione peroxidise, and catalase, can counterbalance oxidative microenvironments. Nonenzymatic exogenous antioxidants such as vitamins, minerals, and polyphenols also have the ability to quench ROS activity.3,4 Therefore, antioxidant therapies may alleviate the adverse effects of chemotherapy and/or radiotherapy but may antagonize antitumor effects by reducing oxidative damage. They prevent cellular damage of normal organs and tissues by reacting with oxidizing free radicals. 5 However, whether antioxidants can antagonize antitumor effects of radiotherapy and some types of chemotherapy remains controversial. It is necessary to clarify whether or not these supplements interact with cancer therapy using radiation and chemotherapy. 6 It is important to note that their effects on prognosis, such as survival rate and tumor progression, should be determined and the results disseminated widely. In this study, we reviewed antioxidants as an adjuvant therapy for cancer patients during chemotherapy or radiotherapy. As our end point, we aimed to provide information about their effectiveness and safety for survival, tumor development, and relief of adverse effects during chemotherapy or radiotherapy for patients with cancer.
Materials and Methods
Electronic literature searches were performed, and relevant articles from 1982 to July 1, 2014, were obtained. Published human clinical trials in English that used randomized controlled clinical trial (RCT) designs involving administration of antioxidant supplements to cancer patients during chemotherapy or radiotherapy were selected. Additional articles found in review articles that suited our inclusion criteria were added. The chosen results were evaluated by the authors independently according to the inclusion and exclusion criteria.
Studies that targeted cancer patients undergoing chemotherapy or radiotherapy were included. All cancer types and all chemotherapy or radiotherapy regimen types were included. Studies investigating chemopreventive effects using antioxidant supplements were excluded. Studies in which the antioxidant was administered by injection were excluded. Only oral supplements were included. Foods and Chinese medicine and herbs were excluded because it is unclear what their effective components might be. Names of antioxidants used in searches were researched and are listed in Supplementary Figure 1 (available at http://ict.sagepub.com/supplemental).7 -10
Results
In total, 399 reports received primary screening. Thereafter, duplicated articles and those that met the exclusion criteria were excluded. Finally, 49 reports that met our inclusion criteria were included: 22 vitamin reports (17 chemotherapy, 8 radiotherapy, including 3 duplicates), 12 reports on phytochemicals and related compounds (10 chemotherapy, 2 radiotherapy), 2 amino acid and related component reports (both chemotherapy), and 13 mineral reports (5 chemotherapy, 8 radiotherapy). Detailed descriptions of the search flow are shown in Figure 1. In Tables 1 to 4, for each category, antioxidant effects on mitigation or aggravation of the adverse effects of cancer therapy are indicated in the representative results. Similarly, antioxidant interference with or enhancement of survival rate and/or antitumor efficacy of cancer therapy are also indicated in the tables.

In total, 399 reports were primarily screened. Thereafter, duplicated articles and those that met the exclusion criteria were excluded. Finally, 49 reports that met our inclusion criteria were included: 22 vitamin reports (17 chemotherapy, 8 radiotherapy, including 3 duplicates), 12 phytochemicals and related compounds reports (10 chemotherapy, 2 radiotherapy), 2 amino acid and related substances reports (both chemotherapy) and 13 mineral reports (5 chemotherapy, 8 radiotherapy).
List of Trials Using Antioxidant Vitamins. a
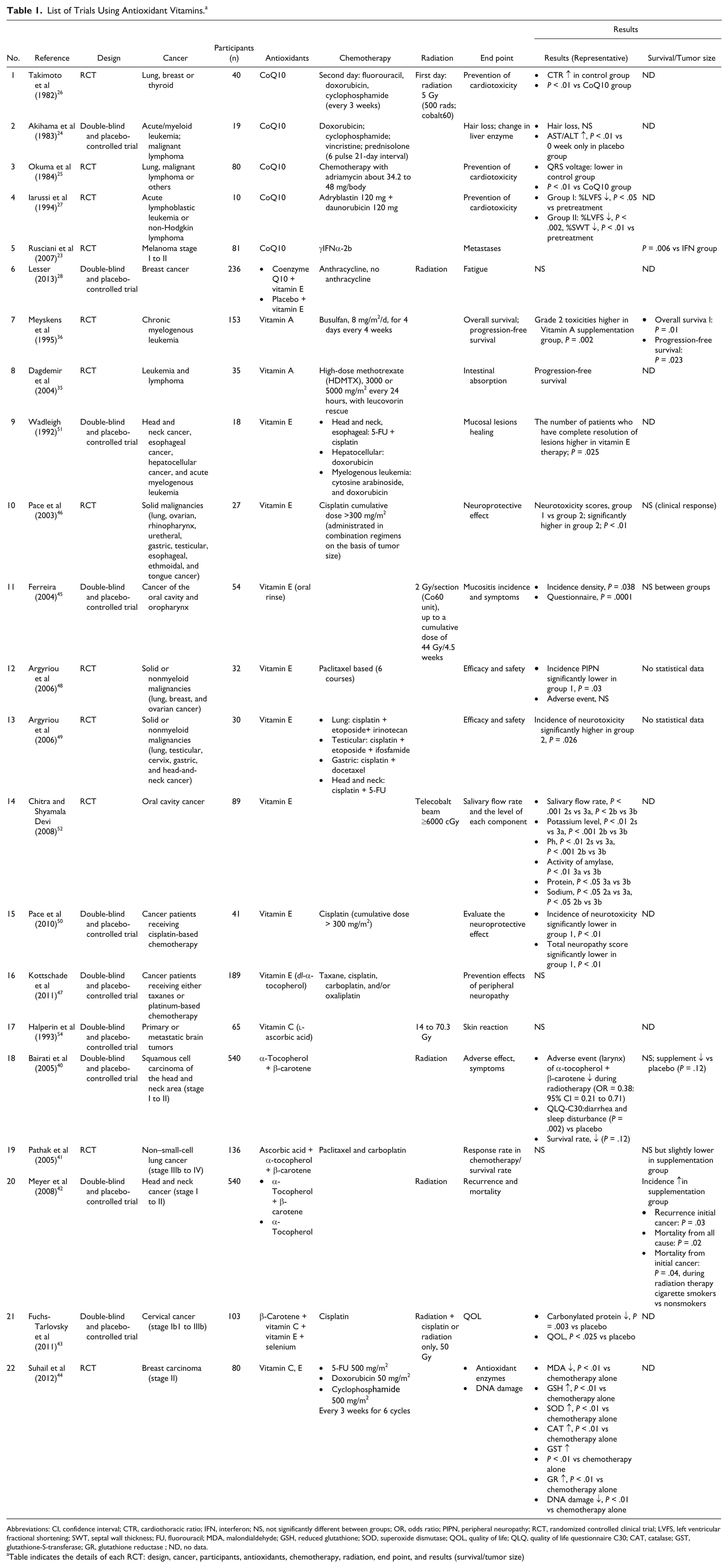
Abbreviations: CI, confidence interval; CTR, cardiothoracic ratio; IFN, interferon; NS, not significantly different between groups; OR, odds ratio; PIPN, peripheral neuropathy; RCT, randomized controlled clinical trial; LVFS, left ventricular fractional shortening; SWT, septal wall thickness; FU, fluorouracil; MDA, malondialdehyde; GSH, reduced glutathione; SOD, superoxide dismutase; QOL, quality of life; QLQ, quality of life questionnaire C30; CAT, catalase; GST, glutathione-S-transferase; GR, glutathione reductase ; ND, no data.
Table indicates the details of each RCT: design, cancer, participants, antioxidants, chemotherapy, radiation, end point, and results (survival/tumor size)
List of Trials Using Antioxidant Phytochemicals and Related Compounds. a

Abbreviations: 5-MTT, 5-methoxytryptamine; CPT-11, irinotecan; NS, not significant; NSCLC, non–small-cell lung cancer; RCT, randomized controlled clinical trial; RTOG, Radiation Therapy Oncology Group; 5-FU, 5-fluorouracil; ADL activities of daily living; ND, no data.
Table indicates the details of each RCT: design, cancer, participants, antioxidants, chemotherapy, radiation, end point, and results (survival/tumor size).
List of Trials Using Antioxidant Amino Acids and Related Compounds. a

Abbreviations: CTC, common toxicity criteria; NCI, National Cancer Institute; RCT, randomized controlled clinical trial.
Table indicates the details of each RCT: design, cancer, participants, antioxidants, chemotherapy, radiation, end point, and results (survival/tumor size).
List of Trials Using Antioxidant Minerals. a

Abbreviations: CTC, common toxicity criteria system version 2a; PTV, planning target volume; RCT, randomized controlled clinical trial; NAG N-acetyl-β-D-glucosaminidase; γGT, γ-glutamyl transpeptidase; AAP, alanine aminopeptidase; SOD, superoxide dismutase.
Table indicates the details of each RCT: design, cancer, participants, antioxidants, chemotherapy, radiation, end point, and results (survival/tumor size).
Vitamins
The antioxidant effect of vitamins suggests that an adequate intake of these micronutrients would contribute to a lower risk of neoplastic diseases. 11 Vitamins have also been used for reducing oxidative stress during chemotherapy and radiotherapy. The vitamins with antioxidant capacity researched in this study were ubiquinone, carotenoids, retinol, tocopherol, ascorbic acid, and folate.12,13 Multivitamins and combinations of multiple vitamins were also included. The results and details of clinical studies are summarized in Table 1 and Supplementary Table 1 (available at http://ict.sagepub.com/supplemental).
Ubiquinone (Vitamin Q)
Ubiquinone, also known as coenzyme Q10 (CoQ10), is a fat-soluble quinone. It has properties similar to those of other vitamins and is essential for the synthesis of adenosine 5-triphosphate (ATP). It plays an important role in the electron transport chain, 14 functions as an antioxidant, and prevents lipid peroxidation.15,16 It is involved in optimal energy production for cell growth and maintenance within human cells. 17 Adverse effects of CoQ10 may include insomnia, elevated liver enzymes, rash, nausea, epigastric pain, dizziness, photophobia, irritability, headache, and heartburn. 18 Coenzyme Q10 is a lipid-soluble antioxidant that may protect against mitochondrial ROS, 19 is an essential component of the electron transport system, and as a potent intracellular antioxidant, appears to prevent damage to the mitochondria of the heart. 20 CoQ10 deficiency is significantly higher in cancer patients than in healthy populations. 21 CoQ10 is widely promoted for enhancing or modulating the immune system. 22
We found 5 clinical trials using CoQ10 alone23 -27 and 1 trial 28 using a combination of CoQ10 and other vitamins. These results indicated some effectiveness of CoQ10 as an adjuvant therapy in cancer treatment. Among 6 trials, 2 reported tumor development and survival rates. Rusciani et al 23 indicated that the administration of γ interferon α-2b (γIFNα-2b) in combination with CoQ10 for 3 years significantly decreased melanoma metastases rates in patients who were followed up for 5 years compared with those in their control group. 23 Although the mechanism by which coenzyme Q10 affected metastasis is not clear, it is unlikely that antioxidant effects interfered with IFN treatments because IFN appears to work through an immunological rather than a free-radical mechanism. CoQ10 also has an effect on the production of ATP required to compensate for the energy loss during chemotherapy. Chemotherapeutic agents could have deleterious effects on mitochondrial respiratory chains by interfering with CoQ10 and leading to calcium overload, causing myocardial cell necrosis. 29 However, CoQ10 supplementation may be effective in protecting myocardial function from chemotherapeutic cardiotoxicity.25 -27,30 Takimoto et al, 26 Okuma et al, 25 and Iarussi et al 27 investigated whether CoQ10 supplementation prevents cardiotoxicity during chemotherapy with anthracycline antibiotics. In all 3 studies, it was reported that supplementation was effective in preventing cardiotoxicity caused by anthracycline antibiotics. However, there is some doubt about the evidence quality of these older studies, which have small sample sizes 27 and other study design issues.25,26
These results indicate that CoQ10 may provide some protection against toxicity and deterioration associated with chemotherapy or radiotherapy. No adverse effects caused by CoQ10 supplementation were reported in any trial.
Retinol (Vitamin A)
Retinoids are reported to inhibit tumor growth on both exocrine and endocrine human pancreatic cell lines. 31 Retinoids and IFNs act synergistically in inhibiting the growth of several cell lines. 32 Furthermore, it is reported that retinol has a protective effect on the mucosa of the gastrointestinal system. 33 However, very few RCTs were performed that combined cancer therapy and retinol supplementation. Regarding tumor development and survival rate, a report on retinol supplementation during cancer therapy was found. However, we excluded this study because it did not meet our inclusion criteria (article in French). 34
Dagdemir et al 35 reported that high-dose retinol supplementation with methotrexate reduces adverse effects of intestinal malabsorption during chemotherapy in children with leukemia and lymphoma. Although methotrexate is classified as an antimetabolite, it is not reported to increase oxidative stress. On the other hand, Meyskens et al 36 reported that the control group in a vitamin A supplementation study had a significantly increased risk of disease progression and death, although toxicities greater than grade 2 were higher in the vitamin A supplementation group.
Tocopherol (Vitamin E)
The main constituent of vitamin E is α-tocopherol, a lipid-soluble vitamin. It is the most important natural antioxidant, scavenging ROS and boosting cellular antioxidative capacity to reduce oxidative damage. 37 Radiation-induced oxygen free radicals have been implicated as mediators of radiation-induced mucosal cell injury.38,39
We found 3 clinical trials using α-tocopherol or vitamin E alone and another 6 trials using a combination of β-carotene, ascorbic acid, selenium, and CoQ10.16,28 Among these, 6 trials28,40 -44 used α-tocopherol in combination with other vitamins. These were included in the “multiple combination with vitamins” category.
Regarding tumor development and survival rates, Ferreira et al 45 conducted a double-blind and placebo-controlled RCT and concluded that mouthwashes (used to thoroughly rinse the oral cavity for 5 minutes and then swallowed immediately) containing vitamin E did not affect the survival rate of patients with cancer of the oral cavity and oropharynx. In addition, they reported that the supplementation reduced the incidence of mucosal adverse effects during radiotherapy. They reported no adverse effects caused by vitamin E supplementation. Two groups, Pace et al 46 and Kottschade et al 47 performed clinical trials using vitamin E for cancer patients treated with taxane or platinum. They reported that no significant difference in peripheral neuropathy was observed between the supplementation group and control group. Argyriou et al48,49 and Pace et al 50 reported that vitamin E supplementation significantly protects against chemotherapy (cisplatin/paclitaxel)-induced neurotoxicity. Similarly, Wadleigh et al 51 reported that application of vitamin E oil to the oral lesions may be effective for chemotherapy-induced mucositis. Chitra and Shyamala Devi 52 performed a clinical trial for patients with oral cavity cancer. They concluded that α-tocopherol supplementation improves the salivary flow rate, thereby maintaining salivary parameters such as pH, activity of amylase, protein, and sodium during radiotherapy. These results suggest that α-tocopherol supplementation may have a preventive effect against radiation-induced oxygen free-radical toxicity.
Ascorbic Acid (Vitamin C)
Ascorbic acid, vitamin C, is a water-soluble antioxidant. It is thought to counteract free radicals and prevents organ and tissue damage caused by adverse effects of chemotherapy and radiotherapy. 53 In this review, there were no reports found on tumor development and survival rates using ascorbic acid during cancer therapy.
Regarding radiotoxicity, Halperin et al 54 investigated protective effects of a vitamin C solution on the skin. It was applied to the radiation site before radiotherapy in patients with brain tumors. However, the skin radiotoxicity score and diagnosis results indicated no significant effect. They reported a rusty discoloration on the skin caused by the application of ascorbic acid solution.
Carotenoid and Multiple Vitamin Combinations
More than 40 carotenoids have been identified in human blood samples; of these, α-carotene, β-carotene, lutein, β-cryptoxanthin, lycopene, and zeaxanthin are found at higher levels. 55 It appears that carotenoids have various chemopreventive actions. 56 Because of its cancer prevention and regression effects, lycopene has been adopted for use in various cancers types. It is also the most potent quencher of free radicals and is an immunomodulator.57,58
We found 4 trials using carotenoids in combination with other antioxidants. Among them, 3 trials investigated survival rates and reported both positive and negative data. Bairati et al 40 indicated that β-carotene treatment in combination with α-tocopherol has the potential to decrease the occurrence and severity of adverse effects of radiations in patients with squamous cell carcinoma of the head and neck. In contrast, antioxidant vitamins may interfere with treatment efficacy, although this negative aspect was not found to be significant (P = .12). Although there was no statistical significance, the survival rate of the supplementation group was slightly lower than that of the placebo group. Although the studies of Bairati et al 40 and Meyer et al 42 were the same trial, we have included both of them because outcome variables presented in each article were different. Meyer et al 42 performed a subgroup analysis that verified that α-tocopherol and β-carotene supplementation had a significant negative effect on cigarette smokers undergoing radiotherapy, particularly with respect to recurrence (P = .03), all-cause mortality (P = .02), and initial cancer (P = .04) of head and neck cancer (HNC). For patients who smoked during radiation therapy compared with those who did not smoke during radiation (not shown in Table 1), they reported high adjusted hazard ratios (HRs) for recurrence (HR = 2.41, smokers; HR = 1.07, nonsmokers), all-cause death (HR = 2.26, smokers; HR = 1.14, nonsmokers), and death from the initial cancer (HR = 3.38, smokers; HR = 1.06, nonsmokers). Furthermore, increased HRs were reported in patients who smoked even prior to and after radiation therapy. On the other hand, Pathak et al 41 conducted an RCT for non–small-cell lung cancer (NSCLC) patients and researched the chemotherapy response and survival rate with and without supplementation using multiple antioxidants. They concluded that the data indicated a slightly higher response and survival rate in the supplementation group, but there was no significant difference between groups.
Regarding antioxidant effects of supplementation, a trial with antioxidant supplementation for patients with cervical cancer was performed by Fuchs-Tarlovsky et al.43,59 They indicated that β-carotene, vitamin C, vitamin E, and selenium supplementation lowered the level of carbonylated proteins and maintained higher QOL scores in global and cognitive ability (using quality of life 30(QOL-30) and quality of life questionnaire CX24 (QLQ-CX24)) compared with placebo, which may have decreased active oxygen induced by chemotherapy with cisplatin and/or radiotherapy. In addition, using combinations of vitamins, Suhail et al 44 performed an RCT for healthy individuals and for breast cancer patients during chemotherapy. They concluded that using vitamin C and E therapy significantly prevented chemotherapy-induced DNA damage assessed in the peripheral lymphocytes. They did not indicate the survival rate and tumor response.
Phytochemicals and Related Compounds
In addition to minerals, amino acids, and vitamins, certain phytochemicals and related compounds have an antioxidant capacity. Here, the phytochemicals and related compounds with antioxidant efficacy that we studied included polyphenols, allicin, melatonin, α-lipoic acid, uric acid, urobilinogen, ferulic acid, melanoidin, phytic acid, and saponin. The results of the research and the details of the clinical trials are shown in Table 2 and Supplementary Table 1.
Melatonin
Melatonin (5-methoxytryptamine) is a neurohormone secreted from the pineal body. Myeloprotective and immunoenhancing effects of melatonin have been demonstrated in in vitro and in vivo experimental models.60,61 Melatonin, a potent antioxidant, plays various roles in regulating circadian rhythms, sleep, tumor growth, and ageing. For many years, it has been known that it plays an important anticancer role. 62 As an antioxidant agent, melatonin enhances the prevention of free-radical production and potentially protects against chemotherapy-induced toxicity. 63
In this study, all the included articles used melatonin combined with chemotherapy. Many of them reported positive data regarding tumor development and survival rates63 -66 when melatonin was combined with chemotherapy. The survival rate of patients with NSCLC and other cancers was significantly higher with melatonin supplementation when combined with chemotherapy using, for example, cisplatin and etoposide. Similarly, tumor regression rates were significantly higher with melatonin supplementation. 66 The study of Cerea et al 67 and many other studies63 -66,68,69 reported positive results regarding toxicity reduction and clinical response. However, Ghielmini et al 61 performed a double-blind and placebo RCT for NSCLC patients whose chemotherapy regimen included cisplatin and etoposide. They reported that there was no significant difference in regard to hematological toxicity in their trial.
In almost all the trials, melatonin supplements were administered in the evening. This was based on the idea that the synthesis of melatonin is strictly controlled by lighting conditions and shows a clear circadian rhythm, with lower levels during the daytime and significantly higher levels at night. 70 There were no severe adverse effects of melatonin supplementation.
α-Lipoic Acid
The administration of α-lipoic acid has been shown to be effective in the treatment of diabetic distal sensorimotor neuropathy. 71 Similarly, the effect of α-lipoic acid on chemotherapy-induced peripheral neuropathy has been investigated. 72 The neuroprotective mechanism of α-lipoic acid is related to the reduction of oxidative stress from free-radical formation. It also has a protective effect during chemotherapy via the regulation of proinflammatory cytokines. 73
Guo et al 72 conducted a double-blind, placebo-controlled trial for patients undergoing platinum-based chemotherapy. Although only 28% of patients in the supplementation group and 30% in the placebo group completed this trial, they reported no significant effects in regard to the tumor reduction rate, activities of daily living, or chemotherapy-induced toxicity such as neurotoxicity and pain. No severe adverse effects caused by supplementation were found. This was the only RCT using α-lipoic acid; therefore, further RCTs using α-lipoic acid are required.
Polyphenols
Polyphenol 74 compounds have been widely studied for their antioxidant properties. They are found in many foods such as chocolate, tea, red wine, and pomegranate juice, which are an integral part of the human diet. 75 The polyphenols researched in this study were ellagic acid, coumarin, curcumin, catechin, resveratrol, anthocyanidin, tannin, rutin, isoflavone, quercetin, chlorogenic acid, and lignan.
Ellagic acid
Ellagic acid is an antioxidant substance that can be found in certain plants.76,77 It is an effective antimutagen and anticarcinogen phytotherapeutic agent that prevents carcinogens from binding to DNA. It may keep cancer cells from spreading and inhibits cancer onset and tumor proliferation during radiotherapy and chemotherapy in laboratory studies. 78
Falsaperla et al 79 conducted RCT using ellagic acid during chemotherapy for patients with hormone-refractory prostate cancer. They investigated clinical responses and survival rates. They indicated that the administration of alkaloid antitumor agents in combination with ellagic acid did not significantly affect the survival rate. However, ellagic acid supplementation significantly reduced chemotherapeutic neutropenia. A trend in serum prostate specific antigen reduction (>75%) was observed in the supplementation group, but there was no significant difference between each group. No significant adverse effects caused by ellagic acid supplementation were found. It is possible that ellagic acid reduces the effect of chemotherapy-induced toxicities; however, further studies are required.
Coumarin
Coumarins are benzopyrones that have antioxidant and anti-inflammatory effects. 80 It is suggested that antioxidants exert their protective effect against cancer by inhibiting the formation of carcinogenic metabolites. 81 However, some studies have reported that coumarin supplements cause liver toxicity.82,83 In this study, we found 1 RCT using coumarin supplementation, which did not present results about the survival rate or clinical response.
Grotz et al 84 performed a double-blind and placebo RCT and reported that the combination of coumarin and troxerutin supplementation reduced the toxicity of radiation in patients with HNC. They reported no severe adverse effects caused by coumarin supplementation. However, there was only a single RCT using coumarin, and further RCTs are required to determine its safety and efficacy as a supplement.
Curcumin
Curcumin, a polyphenol contained in turmeric, has potent antioxidant, anticancer, 85 and anti-inflammatory effects.86,87 Some clinical trials have revealed that curcumin lowered the toxicity of pancreatic cancer treatment, although diarrhea was an adverse effect in some. 88
In this study, we found 1 RCT using curcumin supplementation, with no results concerning the survival rate or clinical response. Ryan et al 87 performed a double-blind and placebo-controlled RCT for breast cancer patients. They reported that curcumin relieved radiation skin toxicities, without causing any severe adverse effects. Other trials88 -90 were not categorized as RCTs.
Amino Acids and Related Substances
Recently, the antioxidant efficacy of certain amino acids and related substances—namely glutathione, N-acetylcysteine, methionine, albumin, lactoferrin, and arginine—has attracted attention. The results of the research and trial details are shown in Table 3 and Supplementary Table 1.
N-Acetylcysteine
N-Acetylcysteine supplementation can increase whole blood concentrations of glutathione, 91 which is a tripeptide associated with reduced chemotherapy-induced neurotoxicity. 92 N-acetylcysteine has not been as well studied as other amino acids. Lin et al 92 performed a placebo-controlled RCT for colorectal cancer patients. They did not indicate the results of survival rates or clinical response. They investigated the efficacy of reducing chemotherapy-induced toxicity. Their results showed that N-acetylcysteine significantly reduced chemotherapy-induced neurotoxicity. They reported no severe adverse effects caused by N-acetylcysteine supplementation. However, there was only 1 RCT using N-acetylcysteine, and further RCTs are required to determine its safety and efficacy as a supplement.
L-Arginine
Heys et al
95
conducted a double-blind, placebo-controlled RCT for patients with primary breast cancer. They indicated that
Minerals
Some minerals chelate substances, thereby exerting an antioxidant effect. These minerals were reported to be susceptible to oxidation-reduction reactions.7 -10,96 -100 In this study, chromium, transferrin (ferritin), selenium, manganese, molybdenum, and zinc met our inclusion criteria. The results of the research and trial details are shown in Table 4 and Supplementary Table 1.
Selenium
Selenium has been shown to possess cancer-preventive and cytoprotective qualities. 100 It affects a wide range of biological processes, including energy metabolism and membrane integrity (by acting as an antioxidant), as well as protecting against DNA damage, exerting anti-inflammatory effects, and regulating the production of active thyroid hormone.100,101
Based on these capabilities, some clinical trials were performed with cancer patients during chemotherapy or radiotherapy. We found 6 results (4 chemotherapy, 2 radiotherapy) for selenium use during cancer therapy. No significant adverse effects of selenium supplementation were found. None of the selected trials reported survival rates or clinical response data, but a follow-up study assessed survival 6 years after 1 trial.101,102 The study reported that there was no significant difference in 6-year survival between groups. 102
Buntzel et al 103 and Muecke et al 101 performed RCTs for patients undergoing radiotherapy for HNC, and cervical and endometrial cancer. They concluded that selenium supplements reduced the number of episodes and the severity of radiotoxicities, such as dysphagia and diarrhea.
Hu et al 104 and Sieja and Talerczyk 105 performed RCTs using placebo controls for patients with many cancer types undergoing chemotherapy using cisplatin. They concluded that selenium supplements reduced the nephrotoxicity and neurotoxicity of cisplatin. Elsendoorn et al 106 and Weijl et al 107 conducted a double-blind and placebo RCT for patients with many cancer types undergoing chemotherapy with cisplatin. They used a combined supplement of selenium, vitamin C, and vitamin E. In contrast to the result of Hu et al 104 and Sieja and Talerczyk, 105 they found no significant difference between trial groups regarding chemotherapy-induced organ toxicity.
Zinc
Zinc, a major dietary antioxidant, protects the airway epithelium against oxyradicals and other noxious substances. Zinc, therefore, has important implications for asthma and other inflammatory diseases, where the physical barrier is vulnerable and compromised. 108 Some studies used zinc supplements to study its effect on maintaining and priming the immune system and tissue repair. There were 7 RCTs in this study, none of which provided data regarding survival rates or clinical responses. Most of them reported no severe adverse effects caused by zinc supplementation.
Sangthawan et al 109 and Ripamonti et al 110 performed RCTs using placebo controls for patients undergoing radiotherapy for HNC. They concluded that compared with placebo controls, zinc supplementation was not significantly effective in relieving radiotoxicities such as taste alterations, weight loss, nausea, and vomiting.
Similarly, Lyckholm et al 111 found that zinc supplementation did not significantly improve chemotoxicity in terms of altered taste and smell. In addition, Ertekin et al112 -114 and Halyard et al 115 conducted an RCT for patients undergoing radiotherapy for HNC. They reported that zinc supplementation was effective in preventing opportunistic bacterial infections and radiotherapy-induced oropharyngeal mucositis and promoting antioxidant enzyme activities. Although the 3 articles of Ertekin et al112 -114 reported on the same trial, we included all of them because the outcome variables presented in each article were different.
Discussion
Survival/Clinical Response
In 17 articles23,36,40
-42,45,46,63
-69,79,95,107 of 49 (approximately 35%) included in this study, effects on patient survival or clinical response during chemotherapy and/or radiotherapy were described. In 7 of 17 RCTs using melatonin supplementation, 4 reported a significantly increased survival rate and 4 reported a significantly increased the tumor regression rate. In addition, 1 trial each using vitamin A
36
and multiple vitamins
42
reported a significantly increased survival rate. On the other hand, 2 trials using multiple vitamins40,41 reported that there were no significant differences between supplementation and control groups, although the survival rates of the supplementation groups were slightly lower than those of the control groups. Two trials using vitamin E45,46 reported that there was no significant difference in clinical response between groups. Also, the RCT using ellagic acid reported that there were no significant differences between groups in survival rate and clinical response.
79
Similarly, a trial using
We list anticancer agents by class and whether they produce ROS in Supplementary Table 2 (available at http://ict.sagepub.com/supplemental). 116 From the results of this review, there might be a possibility that potent antioxidant supplementation could reduce therapeutic effects of radiotherapy or chemotherapy using alkylating agents, platinum compounds, or anthracycline. These agents exert a therapeutic effect by generating active oxygen. Compared with regular doses (6-8 mg/d) as sleep aid, high-dose melatonin supplementation (20-40 mg/d dose) was administered in all trials in this review. In the case of melatonin and also for vitamin C, higher dose or stronger antioxidants might protect not only normal cells from ROS-generating therapies, but might also protect cancer cells themselves by helping them proliferate. On the other hand, it is also known that a higher dose of antioxidant can function as a pro-oxidant in cancer cells,99,117 suggesting that high-dose antioxidants might augment effects of ROS-generating therapies. Lower-dose antioxidant supplementation may protect normal cells and reduce the toxicity of radiation and chemotherapy. 42 However, it is difficult to demonstrate either positive or negative effects of antioxidant supplementation on patient survival and growth inhibition of cancer cells in the studies reviewed in this article.
However, a negative effect was demonstrated by Meyer et al, 42 studying HNC patients who were undergoing radiotherapy and who also smoked. Their data indicated that α-tocopherol and β-carotene supplementation with radiotherapy significantly increased recurrence and mortality in patients who smoked during radiation therapy, although not in nonsmoking patients. In evaluating the negative results of that study, 2 factors were suggested to interact with each other. The first was that antioxidant supplementation scavenged free radicals and reduced the damage caused by ionizing radiations. The second was that the carbon monoxide in cigarette smoke increased the blood carboxyhemoglobin, 118 and oxygen transport abilities were adversely affected. This might have led to the proliferation of cancer cells that were resistant to hypoxia. It is known that carbon monoxide has 200 to 300 times higher affinity for hemoglobin than oxygen. It is difficult to generate ROS in a state of oxygen deficiency. Furthermore, cancer cells can adapt to hypoxia, 119 which results in invasion, metastasis, and angiogenesis. 120 Cancer cells stop growing during hypoxic cell cycle arrest, making any treatment less effective. It is, therefore, suggested that a combination of smoking with the consumption of a strong antioxidant during radiotherapy may create a favorable condition for cancer growth, resulting in lower survival rates.
Reduction of Adverse Effects: Chemotherapy
Among the 49 studies, 46 examined the reduction of adverse effects by antioxidant supplementation. In 34 trials, possible reductions in chemotoxicities or radiotoxicities using antioxidant supplementation were reported. On the other hand, only 1 RCT, using vitamin A, reported that supplementation possibly increased chemoinduced toxicities. The remaining 11 studies displayed no difference in toxicities between control and supplementation groups.
Chemotherapy and radiotherapy cause various adverse effects, which may in part be caused by free radicals and ROS. 121 ROS generation causes various tissue or organ injuries 122 : doxorubicin and other anthracycline antibiotics are known to lead to cardiotoxicity 123 ; cisplatin and other platinums lead to nephrotoxicity, ototoxicity, and peripheral neuropathy124,125; bleomycin leads to lung injury 126 ; and alkylating agents cause DNA damage of drug-treated cells.8,127 Carcinogenesis may also occur as the result of tissue or organ injuries. 122
In 18 RCTs in which platinum was used as the therapeutic agent, the effects of melatonin,61,63 -65,67 -69 selenium,104 -107 and vitamin41,43,46,47,49 -51 supplementation on chemotoxicities were reported. Among 7 trials using melatonin, 6 reported that melatonin supplementation significantly improved myelosuppression, weight loss, and neurotoxicity. Selenium supplementation was used in 4 trials. In 2 trials selenium supplementation was reported to be significantly effective for nephrotoxicity and QOL. Vitamins were used in 7 RCTs, showing a significant improvement of QOL in 1 trial and a significant decrease of various chemoinduced toxicities in 5 trials. Similarly, we found 7 RCTs studying the effects of melatonin63 -66,68,69 or vitamin E 48 on relieving toxicity of plant alkaloid–based chemotherapy, although these regimens were not considered to exert cytotoxicity by generating free radicals. All of them reported that melatonin or vitamin E supplementation was significantly effective in reducing toxicities. Furthermore, we found 5 studies26,36,69,105 that researched the interaction between antioxidants and alkylating chemotherapy (cyclophosphamide). In 3 trials26,69,105 out of 5 using cyclophosphamide regimens, there was a significant effect of antioxidants on chemoinduced toxicity. One trial 36 using busulfan reported improvement in chemoinduced toxicities for more patients in the vitamin A supplementation group than in controls.
As described above, a significant relief in chemotherapy-induced toxicities was reported in many trials using various antioxidant supplements. However, among trials in which the same combination of chemotherapeutic agent and antioxidant was used, some reported effective outcomes, whereas others did not. This could be considered to be dependent on the dosage and/or patient’s background rather than on a scale difference of the trials.
Reduction of Adverse Effects: Radiation
In total, 19 radiotoxicity prevention trials were investigated, which specifically aimed to reduce toxicities affecting the mucosa, skin, salivary glands, and taste. Four of 19 trials reported no significant differences in toxicity between groups. Antioxidant supplements such as vitamin E,45,52 multivitamin combination,40,42,43 polyphenol,84,87 and zinc109 -115 were effective in preventing radiation-induced toxicities in the skin, mucosa, and salivary glands.
Clinical Use of Antioxidant Supplements
Regarding the conflicting issues related to antioxidant use in cancer chemotherapy or radiotherapy, although a large, well-designed review of the relationship between mitigating effects of antioxidants and oxidative stress caused by anticancer agents is warranted, various aspects of the relationship between cancer and antioxidants have already been investigated. Using animal and in vitro experiments, Chandel and Tuveson 128 demonstrated that antioxidants do not prevent cancer and may accelerate tumor development by targeting ROS in the cell. They caution that antioxidant supplementation should be carefully utilized in cancer patients undergoing concurrent cancer therapy. It may be highly arguable whether cancer patients during cancer therapy should freely use antioxidants.
Finally, the efficacy of each combination of anticancer agent with antioxidant supplement requires adequate verification. In the present research, there were no investigations in which the study drug proliferated the growth of cancer and increased mortality. However, if we want to use antioxidant supplements as CAM for cancer patients, further investigations are required for each and every combination of cancer, dietary supplement, and therapy. Unsupervised use of supplements should be avoided. 129
One limitation of our review is that we included some trials with low Jadad scores. In most systematic reviews, trials scoring more than 3 are included. In our selected 49 studies, there were 23 trials that scored more than 3. However, we felt that Jadad scores themselves had limitations in describing study quality. Some studies met our inclusion criteria even though they had low Jadad scores. We have, therefore, included all studies but described them in detail in Tables 1 to 4 to allow the reader to judge study quality. With regard to statistical data integration, it is difficult to perform a meta-analysis with this set of studies because of variability of the data available for each antioxidant. Thus, data were compiled without statistical analysis.
To examine the viability and safety of antioxidants in pathological conditions and cancer therapy, trials should be performed with a single regimen, single type of cancer, and single antioxidant. Only such investigations would adequately describe the safety and effectiveness of antioxidant use by cancer patients during therapy. However, in our research, only 2 trials that met those conditions reported survival rate or tumor development. Similarly, only 5 trials that met those conditions reported effects on chemotoxicities or radiotoxicities. Therefore, we are unable to judge the effectiveness and safety of antioxidants definitively.
In conclusion, it was difficult to determine whether antioxidants may have an impact on treatment outcomes or whether they may ameliorate adverse effects of chemotherapy and radiotherapy. Discussion of antioxidant use has sometimes distinguished palliative versus curative regimens. For curative regimens, it is important not to inhibit therapy in any way, and patients are usually in better overall condition to tolerate side effects. In palliative or recurrent settings, however, patients are less able to tolerate side effects, and cytotoxic efficacy may be less of a concern than maintaining the patient in treatment. Basically, stable disease is acceptable in this situation if side effects can be managed. Thus, it is important that clinicians make an integrated decision, taking into account the following: (1) the antioxidant dosage and types, (2) the background and state of the patient, and (3) type of cancer and antitumor therapy. 130 It is desirable to use an evidence-based method to select supplements best suited to cancer patients. Although there are many opinions about the risks or benefits of antioxidant supplementation, the only supportable conclusions based on the present research are that it is difficult to demonstrate definitively that antioxidants ameliorate therapeutic toxicities and that there is no evidence of antioxidant supplementation causing harm alongside cancer therapy, except for smokers undergoing radiotherapy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.