
Abstract
Introduction
Breast cancer (BC) patients commonly utilize different health behaviors (HBs) such as diet, exercise, and complementary and alternative medicine (CAM) for a variety of reasons including cancer prevention. 1 The overall prevalence ranges from 17% to over 70% depending on the population and the CAM therapies studied. Few studies have examined the use of CAM among women at high risk for BC (HR-BC). This HR-BC population includes women with a strong family history of BC and/or who have a genetic mutation that confers a high predisposition to developing breast and other cancers. This may also include women already diagnosed with BC or ductal carcinoma in situ at a young age with strong family history as the remaining breast would remain at high risk for developing BC in the future. One well-defined group is women with a BRCA1 or BRCA2 gene mutation, who have a cumulative risk of developing BC by age 70 years of 49% to 87%. 2 Because of this significantly elevated risk for developing BC, these women may seek prevention interventions such as CAM, diet, and exercise. Limited information exists regarding the use of different HBs in this population before and after being diagnosed with a HR-BC, which makes it of particular interest in our current study.
We hypothesized that among HR-BC women, individuals with increased emotional distress, anxiety, or depression would be more likely to incorporate different HBs such as CAM, diet, and exercise. The purpose of our study was to evaluate (1) the prevalence of HB, focusing on CAM, diet, and exercise, among HR-BC women; (2) explore decision and communication patterns regarding CAM use; and (3) determine whether correlations exist between CAM use and factors such as age, education, gender, race, cancer diagnosis, and psychological states (emotional distress, anxiety, and depression).
Methodology
Patients
Women at HR-BC enrolled in a prospective enhanced screening study were asked to complete a questionnaire about CAM use from 2007 to 2009. Details of this screening study have been published previously. 3 Participants were included if they had an identified genetic mutation in a BC predisposition gene (eg, BRCA1/2 or CDH1) or a ≥20% lifetime risk of developing BC using published probability models (eg, Gail, Claus, or BRCA-Pro).4,5 Patients with a history of BC needed to have completed treatment and be cancer free for 2 years. In addition to a yearly mammogram, enrolled subjects had 6-month evaluations that included a breast examination, ultrasound, and magnetic resonance imaging. A baseline questionnaire was given to the patients and included questions about age, ethnicity, income, education, and past medical history, including cancer diagnosis and treatment. The questionnaire was developed by the authors (RTL, AB, FO). This study was approved by the institutional review board of the University of Chicago (#12073B).
Health Behaviors
To identify use of CAM, diet, and exercise, we gave study subjects a self-administered survey instrument that asked about common HBs and all categories of CAM, as defined by the National Center for Complementary and Integrative Health. The questionnaire asked specifically about the use of biologically based therapies (coenzyme Q10, black cohosh, essiac, green tea supplement, Hoxsey Formula, maitake mushroom, mega-dose vitamins, mistletoe, selenium, shark cartilage, vitamin C, vitamin E, and other), dietary changes (low fat, increased soy, increased green tea, macrobiotic, and other), alternative medical systems (traditional Chinese medicine, naturopathic medicine, homeopathic medicine, and other), and nonbiologically based therapies (acupuncture, chiropractor, exercise, massage, meditation, prayer/spiritual healing, relaxation, psychotherapy, support group, yoga, and other). The timing (lifetime, before, and after diagnosis of HR-BC) and whether initiation of CAM use was cancer related were also documented. Other data collected via the questionnaire included communication patterns with health professionals, decision-making, and monthly out-of-pocket expenses related to CAM use.
Psychologic Measures
To evaluate depression in the subject cohort, we used the Beck Depression Inventory (BDI). A score of >9 at any time was considered abnormal. 6 We also used the State-Trait Anxiety Inventory (STAI) to evaluate the subjects for anxiety. 7 For the STAI-Trait score, the baseline average score was used to dichotomize patients with low versus elevated baseline anxiety trait levels. For the STAI-State score, subjects were divided into those with the elevated STAI-State score (as determined relative to the overall cohort average) at any time during the study and those with STAI-State scores that were never above average during the study. Finally, patients were asked about the general population risk for BC and whether they viewed their own risk as above, below, or the same as the general population risk for BC.
The Short Form 36 (SF-36) was used to collect information on the quality of life of subjects and provides a score in 8 domains: general health, mental health, physical function, social role function, emotional role function, physical role function, vitality, and body pain.8,9 Scores were converted to a scale of 0 to 100 with 50 being the general population norm and participants with scores <50 having poorer quality of life. Mental health and emotional role function subscales were used to evaluate for emotional distress with scores < 50 considered to represent emotional distress.
Statistical Analysis
To explore predictors of HBs and CAM therapies, we performed univariate analysis using the different HBs survey categories: (1) any HB (including CAM, diet, exercise, support group, and psychotherapy), (2) CAM (herbs and supplements [HS], acupuncture, massage, and so on, but excludes diet, exercise, support group, and psychotherapy), (3) HS, (4) other CAM therapies (such as diet, exercise, support group, and psychotherapy) excluding HS, (5) diet programs, and (6) exercise. These categories were examined separately for time points before and after a diagnosis of cancer (or risk of cancer). For the purposes of this study, diagnosis of BC or diagnosis of elevated BC risk were considered equivalent. If subjects were pursuing a HB, they were asked if the reason was related to cancer (both risk of BC and/or diagnosis of BC) or not. Demographic variables, which have been previously reported to be correlated with CAM use (age, income, education, and race), along with variables of interest (perceived risk of cancer, breast and/or ovarian cancer history, and psychological measures), were analyzed using univariate logistic regression to test for associations between the different categories of HBs.10-12 All associations with HBs are presented as odds ratios (ORs) and P values. Variables with a P value of <.10 in the univariate analysis were sequentially included in the multivariate logistic regression model. All statistical analyses were performed using STATA 11.0 (StataCorp LP, College Station, TX).
Results
Patients
A total of 134 of the 198 women (67%) enrolled in the screening study completed the survey. Participants had a mean age 45 years (±10.4 years) and generally Caucasian (92%), well educated, and affluent (Table 1). Nearly one third (30%) of the patients surveyed reported a history of breast and/or ovarian cancer. BC risk models predicted that the subjects had a 13.7% to 32.5% overall average risk of being a carrier of a BC susceptibility gene. Approximately half of the subjects (51%) had a known susceptibility gene for BC. Most patients had normal psychological scores on BDI (86%), SF-36 Mental Health Subscale (94%), and the SF-36 Emotional Role Subscale (88%; Table 2). Approximately half of subjects (52%) perceived a much high risk of developing cancer in the future as compared with the general population.
Demographic.

Psychological Characteristics.
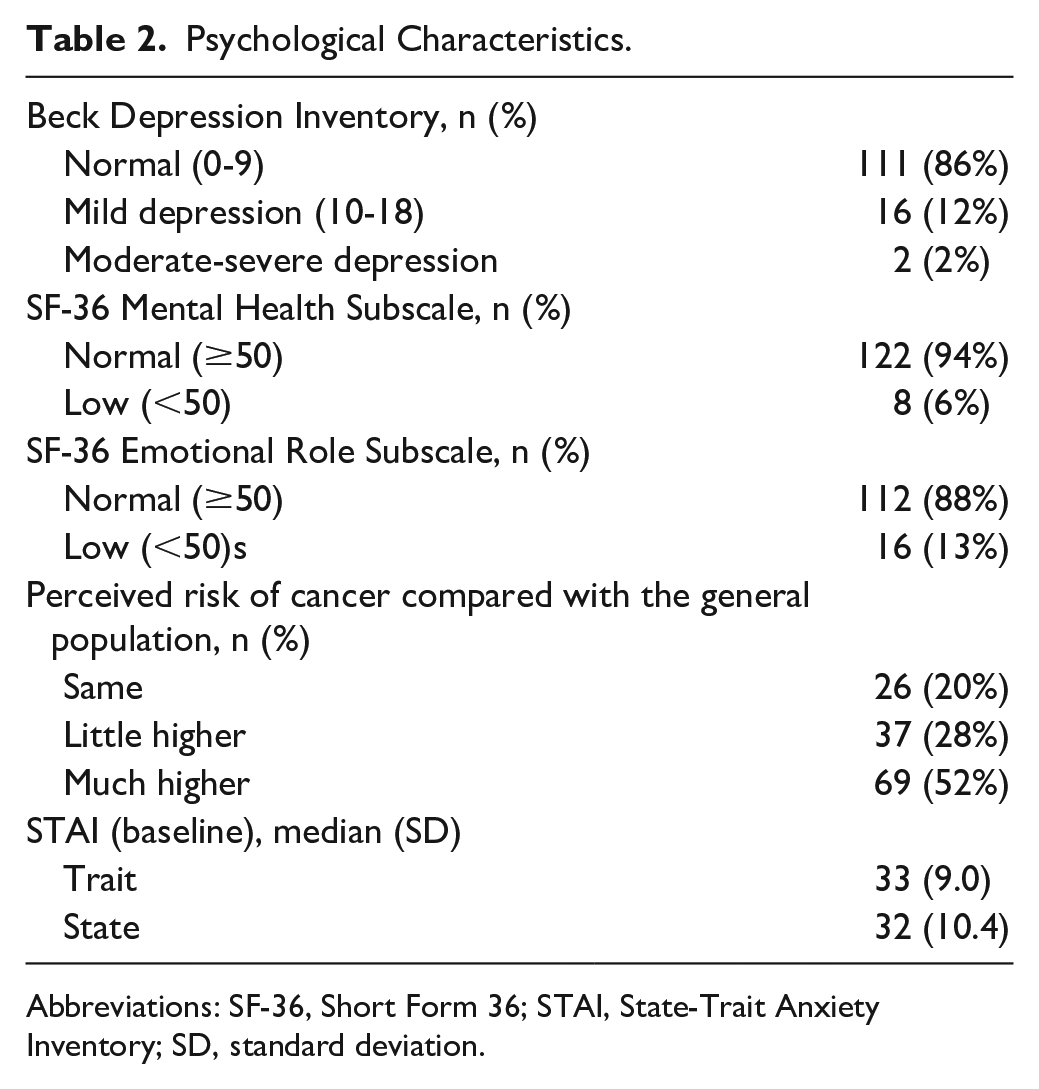
Abbreviations: SF-36, Short Form 36; STAI, State-Trait Anxiety Inventory; SD, standard deviation.
Health Behaviors and CAM Use
Nearly all subjects (97%) reported utilizing HBs at some point in their lives; most commonly use of a CAM therapy (91%). This utilization of any HB dropped from 87% before a diagnosis of HR-BC to 68% after diagnosis. CAM therapies (excluding diet, exercise, psychotherapy, and support group) similarly dropped from 81% to 51% after diagnosis of HR-BC. Subjects were also less likely to incorporate diet and exercise behaviors after diagnosis of HR-BC, 48% versus 32% and 64% vs 34%, respectively. The use of CAM therapies was more likely to be cancer related (31%) than were diet (21%) and exercise (16%; Table 3).
Prevalence of Health Behaviors and CAM by Category a .

Abbreviations: CAM, complementary and alternative medicine; BC, breast cancer; HS, herbs and supplements.
Data shown provides the number of subjects and percent of the entire cohort for each column. For the column “cancer-related reason,” the percentage is of those subjects who reported utilizing the specific health behavior.
Excludes diet, exercise, prayer, support group, and psychotherapy.
Excludes diet, exercise, prayer, support group, psychotherapy, and HS.
Specifically, the most prevalent lifetime HBs reported were exercise (83%), massage (68%), vitamin C use (57%), low-fat diet (49%), yoga (44%), and vitamin E (41%). These same behaviors were reported as the most common prior to diagnosis of HR-BC. After this diagnosis, the same 6 behaviors were the most common, but the prevalence dropped significantly (Table 4). For example, the use of massage went from 54% before diagnosis of HR-BC to 25% after diagnosis. The most common HBs used for “cancer-related reasons” differed significantly from the prevalence above and included low-fat diet (68%, among those using this diet), exercise (31%), support group (100%), meditation (68%), prayer (48%), and drinking green tea (59%). Adoption of new HBs was most prevalent for HS (36% among those using HS) followed by diet (21%) and exercise (21%). Only 2 of the most common HBs were reported as increasing in utilization after diagnosis of HR-BC: green tea (9% vs 13%) and support groups (6% vs 10%). Patients reported spending an average of $106 ($0-$800) per month on out-of-pocket expenses for these HBs.
Most Common Specific Health Behaviors a .

Abbreviation: BC, breast cancer.
Data shown provides the number of subjects and percent of the entire cohort for each column. For the column “cancer-related reason,” the percentage is of those subjects who reported utilizing the specific health behaviors.
Communication and Decision Practices Related to Health Behaviors
Subjects reported learning about HBs from family and/or friends (50%), print media (44%), physicians (37%), and the Internet (25%). This cohort reported that they most often considered diet (18%), acupuncture (17%), green tea (16%), meditation (16%), yoga (14%), and relaxation therapy (11%) but did not make these types of changes primarily because they were unsure of the benefit (31%), lack of interest (26%), lack of information (22%), and cost (12%). When deciding about HBs and CAM, 68% reported that they made the decision entirely on their own. The most commonly reported reasons for pursuing these interventions were to improve overall health (82%), to employ a holistic approach to health care (44%), to minimize side effects from intervention (42%), to do everything possible to treat (or prevent) cancer (38%), and to have a sense of control over health care (35%). Almost half of the subjects (48%) reported that they did not discuss these HBs or CAM therapies with a physician.
Univariate and Multivariate Analyses
Similar to previous studies, younger age, race, higher income, more education, history of breast and/or ovarian cancer, and higher perceived risk for future BC were found to have correlations to use of different HB categories on univariate analysis. We also found that several psychological measures were correlated with different HBs: STAI-Trait, STAI-State, SF-36 Emotional Role Subscale, SF-36 Mental Health Subscale, and BDI. An above average STAI-State at any time during the study had the strongest correlation with the use of different HBs, specifically use of any HB after diagnosis of HR-BC (P = .058), use of an exercise program at any time (P = .021) and before diagnosis (P = .058), and CAM use after diagnosis (P = .087). The STAI-State variable was used as the psychological dependent variable in multivariate analysis along with younger age, race, income, education, and history of cancer. Before a diagnosis of HR-BC, an elevated perceived risk of developing BC was associated with the utilization of any HB (OR = 5.0, P = .01), CAM (OR = 3.2, P = .02), non-HS CAM (OR = 3.9, P = .004), and exercise program (OR = 4.0, P = .003). Having a history of breast and/or ovarian cancer as well as an elevated STAI-State anxiety score were associated with utilization of an exercise program—OR 3.1 (P = .03) and OR 2.5 (P = .04), respectively. In contrast, after a diagnosis of HR-BC, having a history of breast and/or ovarian cancer was the strongest predictor of different HBs: any HB (OR = 6.6, P = .003), CAM (OR = 5.9, P = .001), HS (OR = 4.3, P = .001), non-HS CAM (OR = 5.0, P = .001), and dietary change (OR = 4.4, P = .002). A high perceived risk of developing BC remained associated with CAM (OR = 2.6, P = .04) and non-HS CAM (OR = 2.6, P = .04) after diagnosis. A household income of more than $70 000 a year was associated with incorporating an exercise program after diagnosis (OR = 4.8, P = .007).
Discussion
Our findings indicated that a high prevalence of HBs including CAM, diet, and exercise was reported among women at HR-BC. Although most participants endorsed using these HBs at some point in their lives, all activities were less prevalent after diagnosis of a HR-BC and even fewer HBs were used for cancer-related reasons. The reasons for these findings were not explored in this study. With over 80% of subjects reporting improved overall health as a reason to pursue HBs, it was surprising that only a fraction of respondents reported that exercise and diet changes were pursued for cancer-related reasons.
There is growing evidence that diet and exercise have the ability to improve survival rates among women with BC.13,14 In addition, psychological interventions that reduce stress and anxiety (eg meditation, yoga, and support groups) may also improve outcomes such as quality of life and survival.15,16 Women at particularly HR-BC should be counseled on lifestyle management as a key component of their prevention strategy, which clearly has strong implications for also improving their overall health and wellbeing. A common reason that women did not report pursuing lifestyle interventions was lack of information. By providing information about the benefits of diet and exercise, physicians can help reduce the barriers to these simple yet important interventions for women at high risk for cancer.
Our results differ somewhat from those of other studies about women at HR-BC. DiGianni et al found a general increase in CAM use, from 54% to 62%, 1 year after baseline assessments among a cohort of women at HR-BC.17,18 Those results differ from our results, in which respondents reported a general decline in use of CAM therapies over time, except for mega-dose vitamins and dietary green tea. Our current study also reported correlations between CAM use and self-reported depression among cancer survivors. Mueller et al also found a high prevalence of CAM use among BRCA1/2 carriers history of cancer, higher education, younger age, breast self-examinations, and anxiety associated with ovarian cancer. 19 In contrast, a study by Field et al found that worry associated with BC but not ovarian cancer was associated with CAM use. 20 This study also reported correlations among those with increased general anxiety but not a cancer-specific anxiety. Mueller et al’s study of patients at HR-BC assessed depression using a validated instrument, and no associations were found with CAM use. 19 Differences in findings may be related to methodology as our study was a single cross-sectional survey and was not repeated over time. In addition, the population included in these studies were different in the proportion of women with a known mutation and cancer diagnosis.
The current study, as well as others, still leaves several questions unanswered about what accounts for the differences in our study findings from previous studies, how to best examine HBs (including CAM), as well as how to measure psychological factors such as anxiety and depression. Future studies may benefit from examining a broad range of HBs such as diet, exercise, and breast self-examination to have a better understanding of all related activities pursued by patients at HR-BC. Understanding why most women decrease their use of HB after a diagnosis of HR-BC should be explored further in order to develop interventions that would help increase their use. Studies of HBs and CAM should attempt to use more uniform categories to allow for easier comparisons between studies. Additionally, it remains unclear whether general or cancer-specific measures of psychological factors such as anxiety are important factors when patients decide to pursue specific HBs such as CAM.
Our current study focuses on a specific population of women at HR-BC, which limits the generalizability of our data. Our methodology relied on self-reported, retrospective questionnaires, which likely underestimated the actual prevalence of HBs and CAM use. A longitudinal study design would provide additional information on the long-term use of these types of interventions. Future studies would also investigate CAM use in other racial and ethnic groups that are underrepresented in the literature. Validated measures for both cancer-specific and general measures of anxiety could provide additional information to help clinicians identify patients who are most likely to pursue CAM therapies.
Summary
Patients at high risk for breast reported that they commonly use CAM and lifestyle interventions. Most of the women surveyed reported that these practices were done to improve their overall health and were not related to their cancer or their risk of cancer. Nearly half of the patients reported that they did not discuss any of these interventions with their doctors. Our results indicate that this population of women at HR-BC appears favorably inclined toward the use of these interventions; however, the use of diet, exercise, and CAM decreased after the diagnosis of HR-BC. Education for patients and clinicians about the potential benefits of a healthy lifestyle, including a healthy diet and physical activity, may help prevent this decline. Patients and physicians should be encouraged to discuss the risks and benefits of CAM use in conjunction with other therapies or risk modifying activities.
Footnotes
Acknowledgements
The authors thank Farr Curlin, MD for his help with this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: American Society of Clinical Oncology Cancer Foundation Young Investigator Award (RTL). Grant No. T32 CA009566 from the National Cancer Institute.