
Abstract
Integrative oncology aims to coordinate the delivery of conventional medicine and evidence-supported complementary and alternative medicine (CAM) to patients receiving cancer care. This field developed out of an increased interest in CAM usage among cancer patients. However, CAM use among medically underserved cancer patients remains to be well characterized. We evaluated CAM awareness as well as prevalence and characteristics of CAM use in 170 consecutive, medically underserved cancer patients presenting to a large, academic, inner-city cancer clinic, using a survey tool. Fifty-three participants declined participation and 17 survey results were incomplete. Therefore, 100 survey results were included in the final analysis. There were 65 males and 35 females in the survey with a mean age of 64.2 years. About 98% of the respondents were African American while 2% identified themselves as Hispanic. About 45% of patients had metastatic cancer, 24% had early-stage disease while 31% of patients were not aware of the stage of their cancer. About 55% patients had elementary school or lower level of education while only 16% had a college degree or higher. About 92% of respondents were unemployed. Some knowledge of CAM was reported by 22% of patients, while CAM use was reported in only 16% of patients. Female sex and college degree were significantly associated with CAM use. The most commonly used CAM modality was meditation (56%), followed by herbal remedies (31%), yoga (31%), and acupuncture (12%). Among CAM users, a majority used multiple CAM therapies. All users reported benefit from CAM use. Emotional wellbeing was the most common benefit followed by improvement in treatment related adverse effects, chemotherapy related symptoms, pain, and sleep. Even though the majority of our surveyed patients never used CAM, 90% of non-users were interested in gaining more information about the various CAM options and exploring its use and potential benefits. The majority (70%) wanted their primary oncologist to provide information about CAM options and discuss its safety and potential complementary benefit in management of their cancer and associated symptoms.
Introduction
Complementary and alternative medicine (CAM) describes medical products and practices, many of which are not yet largely accepted by contemporary Western medicine, that aim to help improve a patient’s health and wellbeing. The term “integrative medicine” is preferably used instead of “complementary and alternative medicine” to better reflect efforts to coordinate conventional and evidence-supported complementary treatments. There has been increasing demand for CAM among patients with cancer. To help meet these needs, the Journal of the National Cancer Institute (JNCI) has published a formal definition and description of integrative oncology. 1
According to the National Center for Complementary and Integrative Health (NCCIH) (formerly termed the “National Center for Complementary and Alternative Medicine” [NCCAM]), the most commonly used CAM techniques include dietary and herbal supplements, mind-body practices (yoga, chiropractic and osteopathic manipulation, meditation, prayers, massage, acupuncture, tai chi, qi-gong, hypnotherapy) and other complementary health approaches (Ayurveda, Chinese medicine, homeopathy, and naturopathy).2,3 Despite a lack of randomized clinical trials to prove CAM efficacy,4,5 the use of CAM continues to rise, especially among cancer patients.3-5 As evidence accumulates supporting the benefit of CAM as a component of holistic cancer care, efforts are being made to formulate and standardize evidence-based guidelines leading to the development of the field of integrative oncology. 6 Not surprisingly, National Cancer Institute (NCI) designated cancer centers have invested resources to provide information and CAM services to patients.6,7
Despite the increasing recognition of the role of CAM in supporting cancer care, the benefits of CAM have not been equally available to the entire spectrum of cancer patients. Knowledge and use of CAM have been noted to be higher in socioeconomically advantaged and Caucasian populations. 7 Patients receiving care at large academic centers are also better equipped with appropriate supervision of their CAM utilization. Significant disparities in knowledge and use of CAM among cancer patients who are members of medically underserved, ethnic minority, and lower socioeconomic status groups have been noted. 8 Additionally, use of these methods in medically underserved populations (MUPs), where often awareness is limited and economic constraints are prominent, may lead to CAM use without appropriate supervision. This raises significant concern with regards to the safety, cost, effectiveness, and interaction of CAM with conventional cancer therapies.9-11
Disparities in the appropriate and safe use of CAM among MUPs could contribute to poor symptom control and worse cancer treatment outcomes. Disparities of CAM use in non-oncology settings have been well studied; however, CAM awareness and use among medically underserved cancer patients remains to be well characterized. As such, it is imperative to evaluate the prevalence and characteristics of CAM awareness and use in the medically underserved cancer patient population, which in turn will enable oncology health professionals to understand and address safety gaps and barriers to CAM use in medically underserved cancer patients. To address this unmet area of needed information, we conducted a study utilizing a survey to assess knowledge and extent of CAM use in patients with active cancer. Patients were being treated at the Grady Memorial Hospital in Atlanta, Georgia, a large metropolitan inner-city safety net academic hospital which predominately serves a medically underserved African American population from the greater Atlanta area.
Methods
This cross-sectional survey-based study was approved by the Morehouse School of Medicine Institutional Review Board (Protocol #1289641-6). An anonymous survey questionnaire was prepared by the research team and conducted in person via paper-based survey, while patients were waiting for physician evaluation in clinic. The survey was conducted at the Cancer Center clinic at Grady Memorial Hospital in Atlanta, Georgia, a general oncology clinic that provides treatment for both solid and hematological malignancies. Inclusion criteria included patients ≥21 years old, with active malignancy receiving care at the Cancer Center clinic, proficient in English and able to understand and provide verbal consent. Exclusion criteria were patients who were acutely sick or unable to consent. Patients were identified consecutively and were presented a printed copy of the questionnaire, upon agreeing to participate in the survey.
Survey
The survey questionnaire (provided in the Supplemental Material) was anonymous and did not collect identifying information that could be traced back to a respondent. It consisted of 33 multiple choice questions, several of which had the option of selecting multiple responses. Respondents were asked to provide information about their awareness of various CAM therapies, types of CAM therapies they had used, reason for use, benefits or harmful effects (if any), and if they had foregone recommended treatment to pursue CAM. Respondents were queried regarding their sources of advice on CAM use and experiences discussing CAM use with oncology providers. CAM modalities discussed in the questionnaire included dietary supplements, herbs, traditional Chinese medicine, Ayurveda, fasting, caloric restriction, homeopathy, and mind body techniques including meditation, Tai chi, Reiki, Yoga, and acupuncture. In addition to questions regarding CAM, the questionnaire collected demographic characteristics of respondents including race/ethnicity, educational background, socioeconomic status, and health insurance status.
Statistical Analysis
Descriptive analysis was used to evaluate correlations between demographic, socioeconomic, and clinical data with knowledge and use of CAM. Fisher’s exact test was used to identify statistically significant associations between patient characteristics and knowledge and use of CAM at a significance level of P < .05.
Results
During the study, 170 consecutive patients presenting to the Cancer Center clinic at Grady Memorial Hospital were approached regarding participation in the survey. Fifty-three participants declined participation and 17 survey results were grossly incomplete with missing information and could not be included in the final analyses. Therefore, 100 questionnaires were included in the final analysis.
Patient Demographics
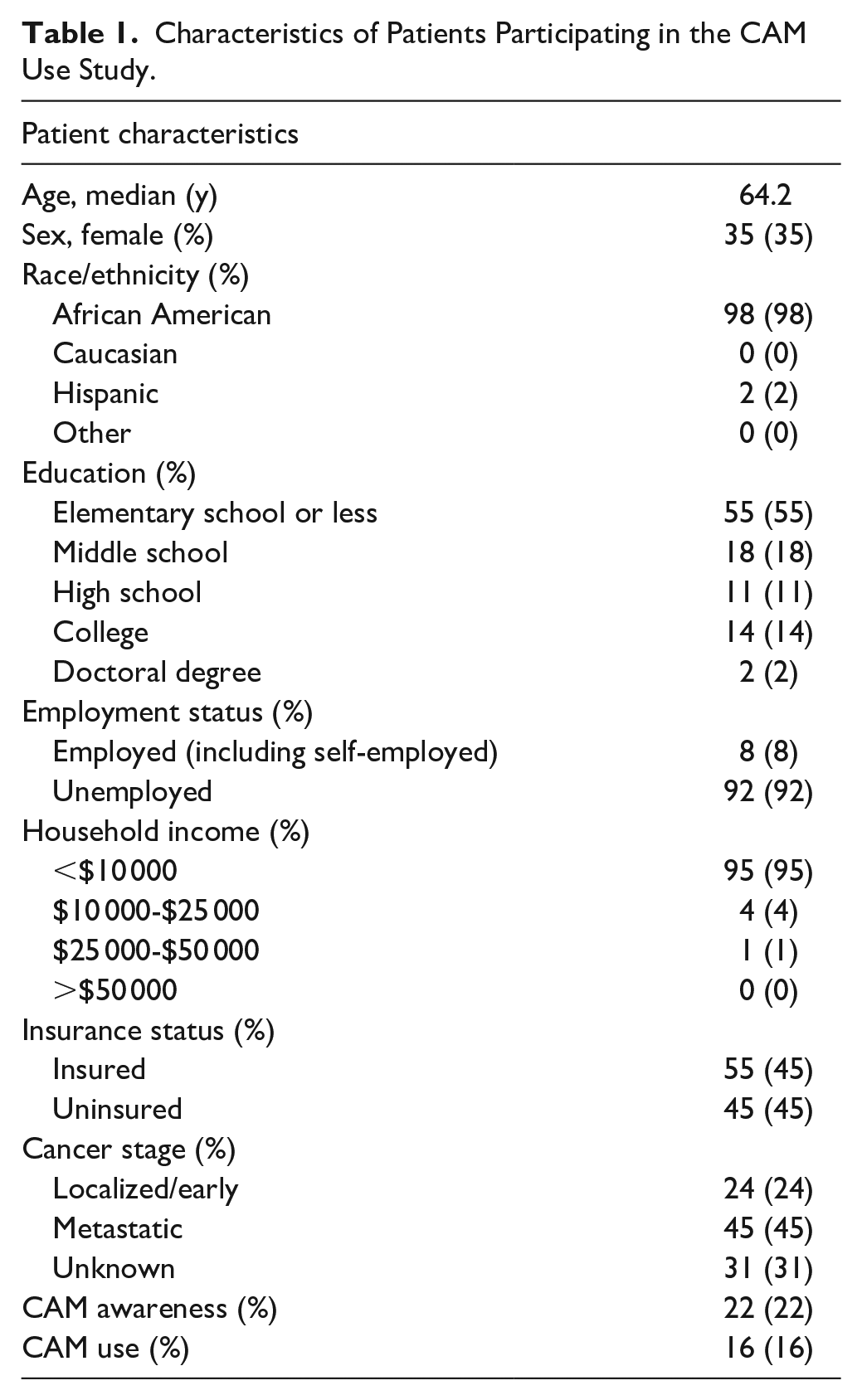
Of the 100 included surveys, respondents were 65% male with mean age of 64.2 years. Most respondents identified as African American (98%) with 2% identifying as Hispanic. About 45% of patients had metastatic cancer, 24% had early-stage cancer, and 31% were not aware of their cancer stage. A majority of patients had an educational attainment level of elementary school or less (55%) while only 16% had a college degree or higher. About 92% of respondents were unemployed, which also included retired participants, and 8% of patients had active employment. Annual income was less than $10 000 for 95% of respondents. About 55% of patients had health insurance coverage, which was primarily Medicaid, and the remaining 45% had no active insurance (Table 1).
Characteristics of Patients Participating in the CAM Use Study.
CAM Awareness and Its Use
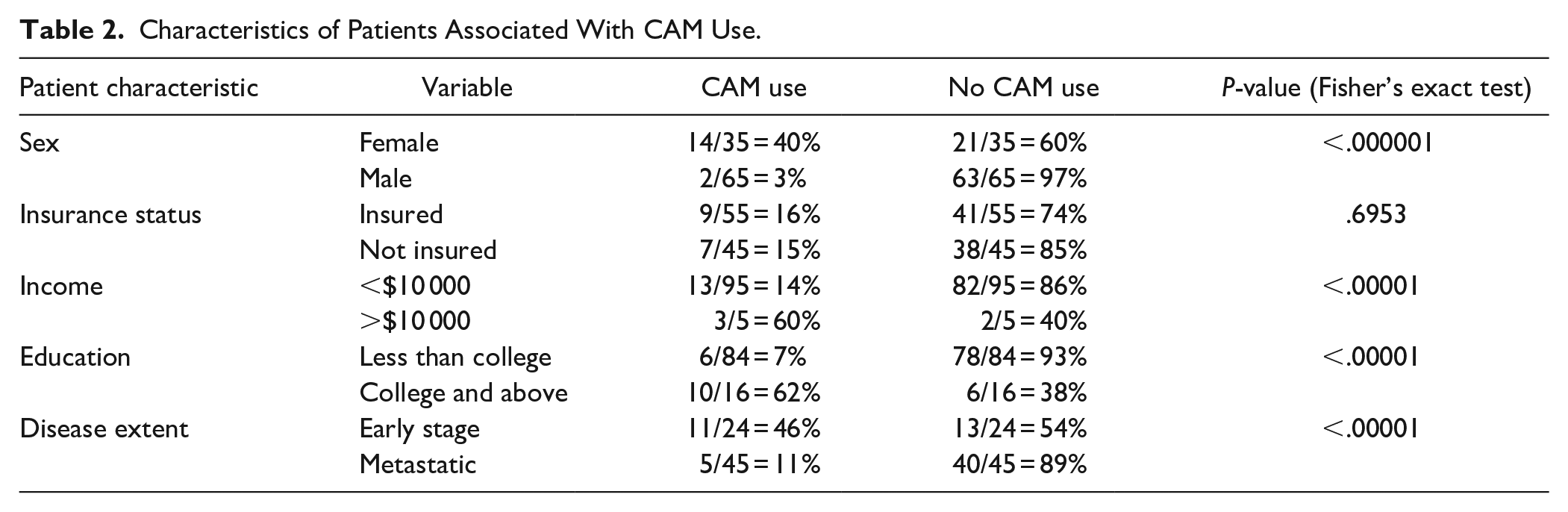
Some knowledge or awareness of CAM was reported by 22% of patients, while CAM use was reported in only 16% of patients. Among patients who reported CAM use, 87.5% (14/16) were females. Of these 14 female CAM users, 10 had breast cancer (62.5% of all CAM users). The use of CAM was strongly related to patients’ education level with 62.5% (10/16) of CAM users having a college or higher level of education. Patients with localized disease, and females were more likely to use CAM (P < .0001) (Table 2).
Characteristics of Patients Associated With CAM Use.
Among CAM users, meditation was the most used modality (56.3%), followed by herbal remedies (31.3%), yoga (31.3%), and acupuncture (12.5%) (Table 3). A majority of CAM users reported utilization of multiple CAM therapies with meditation and yoga frequently combined together.
Type of CAM Used.

All users reported benefit from CAM use. Emotional wellbeing was the most common benefit seen in 75.0% of CAM users, followed by improvement in treatment related adverse effects in 37.5%, pain control in 25.0%, and improved sleep in 18.8% (Table 4). Although the majority of respondents had never used CAM, 89.2% of non-users were interested in getting more information about the various CAM options and exploring its use and potential benefits in improving physical and emotional symptoms of cancer and treatment. A majority (70%) wanted their primary oncologist to provide information about CAM options and discuss its safety and potential complementary benefit in management of their cancer and associated symptoms.
Perceived Benefit of CAM.

Discussion
This study is one of few investigations of CAM use, in a medically underserved and uninsured population, which faces numerous healthcare disparities. Most large studies investigating CAM usage have involved predominantly non-minority patients. Such studies have shown high CAM utilization, with up to 85% of respondents using some form of CAM, with dietary and herbal supplements (73%) being the most common method used. 12 There is a relative paucity of studies investigating CAM utilization in cancer patients from MUPs. Jones et al 13 surveyed 165 cancer patients from a MUP in the greater Houston area in Texas, and found a high utilization, up to 85%, of non-physician guided CAM. This initially appears to contrast our study, which found only 16% of surveyed cancer patients from a MUP utilizing CAM. However, this discrepancy is likely due to differing definitions of CAM. The highest CAM therapies utilized in the study by Jones et al included prayer (85%) and relaxation (54%), 2 methodologies that we did not specifically inquire about in our survey. Usage of acupuncture, aromatherapy, herb, massage, meditation, and yoga in this population were each less than 20%. In our study, among CAM users, meditation was the most common method cited, which is consistent with results from other studies among MUPs.11-13 Similar to our study, Jones et al 13 identified a significant interest among the surveyed population for information on CAM and reported lack of knowledge and cost as barriers to use.
Taken together, our study and prior data suggest that cancer patients from MUPs are interested in CAM but face significant barriers in accessing CAM modalities that are not easily self-directed and free such as prayer and meditation. This is not surprising given that underserved and uninsured populations face significant healthcare disparities with studies showing that up to 19% of non-elderly adults are unable to afford even their prescriptions. 14 Accordingly, CAM options which would require out of pocket expenses like herbal and other supplements, were used in only 31.3% of our surveyed patients, while the use among patients from non-MUPs has been reported to be around 73%.12,15 Given the significant cost-barriers cancer patients from MUPs face in accessing CAM, programs aiming to educate these patients on how to effectively utilize free CAM methodologies such as meditation and yoga would likely be cost-effective and impactful. Additionally, these patients would greatly benefit from social worker or community assistance in accessing low-cost or charitable CAM opportunities.
Within MUPs, further demographic and disease factors affect utilization of CAM. Our study affirms higher use of CAM in women, particularly those with breast cancer, which has been an established trend in previous studies. 15 It is not clear why females or those with breast cancer are more likely to utilize CAM; possible contributing factors include increased acceptance among these populations and more prevalent social network and charitable opportunities available to those with breast cancer. Ultimately, reasons for these associations were not elucidated by this study but are likely multifactorial and important areas for future investigation to guide efforts to increase CAM utilization in other populations. Additionally, CAM usage was associated with a higher income level and college education, likely due in part to improved access with higher income and an increased ability to research and understand CAM options with higher levels of education. CAM use in patients with localized disease was higher compared to among those with metastatic disease. Patients with advanced disease often face increased pain, decreased functional status, and increased despair and depression all of which negatively impact their quality of life and ability to actively participate in their care. 16 Targeted delivery of CAM to those with advanced disease could be highly impactful in palliation of both physical and emotional symptoms when conventional therapeutic options are limited or exhausted.
One of the most critical findings in our study was the perceived success of the CAM methods used by the patients. All patients felt very optimistic about the benefit of CAM and none of them reported experiencing any side effects. Benefits were seen in both physical and emotional health with reported improvements in treatment-related adverse effects, emotional wellbeing, pain, and sleep. These results suggest that patients who use CAM have a favorable impression regarding potential impact of CAM on their perceived overall wellbeing. This reinforces the importance of increasing the accessibility of CAM in MUPs.
Interest in exploring CAM as an adjunct to cancer care was high among our surveyed MUP. However, most patients wanted their oncologists to provide information on CAM. Prior studies have found that initiation of CAM therapy is positively associated with discussions of CAM with oncology providers. 12 Identified barriers to patient-initiation of discussions regarding CAM include a fear of negative provider response.17,18 This fear is plausibly compounded in members of MUPs by lower levels of educational attainment, evidenced in our study as a majority of respondents with elementary school level or below educational backgrounds, and the ensuing power dynamic between highly-educated expert provider and patient. Among cancer survivors, physician-initiated, patient-centered communication has been shown to facilitate discussion of CAM use between patient and provider. 19 This has far reaching implications for the physicians taking care of cancer patients.
Rising interest in CAM across all patient groups calls for a shift in our cancer treatment paradigm. Current and future oncologists must continue to deliver the most current and effective cancer-directed therapies to their patients. However, they should also know various CAM options and their potential benefits and interactions with cancer-directed therapies. They should be able to initiate and hold patient-centered discussions on CAM treatments and facilitate integration of such adjunctive therapies into their treatment plans based on patient needs and desires. In MUPs, patient-centered discussion and delivery of CAM must consider patient medical literacy level, availability and accessibility of both conventional and complementary medicine, and expense concerns. Efforts to improve discussion and delivery of CAM in MUPs would benefit not only from oncologist education, but also education of multidisciplinary teams. For example, inclusion of pharmacists would allow for improved recognition of interactions between CAM techniques and pharmacotherapy and the inclusion of social workers would allow for increased knowledge of financially feasible CAM opportunities. This multidisciplinary team-based approach could help reduce healthcare disparities faced by MUPs in accessing safe, evidence-supported, and realistic CAM therapies.
Limitations, Conclusion, and Future Directions
This study had limitations. The number of respondents in our study was relatively small, and due to the demographics of the city of Atlanta (with 51% African American and only 4% Hispanic population), 20 were predominantly composed of African American patients. As Hispanic cancer patients are known to have higher CAM use, 21 our results may have limited generalizability. Additionally, the questionnaire used in the study was not a previously validated survey tool or validated in a pilot setting in our population. Though our study involved a small sample of the underserved African American cancer population, the results are thought- provoking. CAM appears to be underutilized in cancer patients from MUPs, further contributing to healthcare disparities facing this population. CAM options that necessitate additional personal care expenses are minimally available to MUPs. Despite a low prevalence of use, CAM users reported benefit of the adjunctive therapies. Though a small study size limits our ability to compare benefits of various types of CAM, meditation was the most utilized, hence most beneficial modality in our study. Among non-users, there was an overwhelming interest in gaining information and exploring CAM as adjuncts in their cancer care. Given the reported benefits and interest in CAM therapies among our surveyed MUP, there exists an unmet need for delivery of these care modalities to MUPs. Thus, the development of structured programs involving oncologists and other health care providers including pharmacists and social workers to help patients make informed decisions about CAM options that could be integrated easily with standard cancer therapy is of utmost importance. This coordinated approach would facilitate the delivery and safe implementation of CAM to MUPs, address a current area of healthcare disparity, and lead to better symptom control and improved cancer outcomes.
Supplemental Material
sj-docx-1-ict-10.1177_15347354211051622 – Supplemental material for Awareness, Use and Outlook of Complementary and Alternative Medicine (CAM) Options in an Underserved, Uninsured Minority Cancer Patient Population
Supplemental material, sj-docx-1-ict-10.1177_15347354211051622 for Awareness, Use and Outlook of Complementary and Alternative Medicine (CAM) Options in an Underserved, Uninsured Minority Cancer Patient Population by Shahla Bari, Iloabueke Chineke, Alicia Darwin, Anam Umar, Heather Jim, Jameel Muzaffar and Omer Kucuk in Integrative Cancer Therapies
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, or authorship. Publication of this article was supported by a Weill Foundation educational grant.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.