
Abstract
Background. Eurythmy therapy (EYT) is a mind–body therapy used in anthroposophic medicine. Recently, the authors were able to show that at comparable workloads, EYT stimulated heart rate variability (HRV) whereas conventional ergometer training attenuated HRV. Furthermore, a long-term improvement of quality of life (QoL) and stress coping strategies by EYT could be shown. Objective. This study aimed to evaluate the long-term effects of EYT training on HRV. Design: A total of 23 healthy women (mean age = 44.57 ± 8.04 years) performed 10 hours of EYT over a period of 6 weeks. Electrocardiograms were recorded before and after the EYT trial. HRV was quantified by the extent of high (HF), low (LF), very low (VLF), and ultra low frequency (ULF) oscillations of heart rate. Results. Autonomic regulation was significantly changed following the EYT training compared with baseline. Especially the proportion referring to the total power (P) of HF/P and LF/P increased, whereas ULF/P and (ULF+VLF)/P decreased after the training period. Conclusion. EYT shifted the autonomic regulation proportionally referring to the total power mainly caused by changes of ULF and VLF components of HRV. The LF and HF spectral components were also decreased following EYT while their proportion in relation to the total variance of the power spectrum was increased. The proportional enhancement of the higher frequency and the decrease of the ULF and VLF components are probably an indicator of an improvement of autonomic regulation processes by more relaxed physical activity after the EYT training, thus supporting the plausibility of the improved QoL and better stress coping strategies.
Introduction
Eurythmy therapy (EYT) is a movement therapy from the field of anthroposophic medicine, which has been practiced for about 80 years. 1 According to the viewpoint of anthroposophic medicine, in a healthy person the forces of the physical, emotional, and spiritual–individual levels of the human being interact harmoniously with each other. Illness occurs when the state of harmony between these different forces becomes disrupted. EYT is a therapeutic approach for restoring a healthy balance between these different levels of the human being. In EYT, meditative exercises are combined with therapeutic movement sequences. It is used in numerous acute and chronic indications according to specified guidelines. In addition to its therapeutic application in manifest illness, EYT is also used with salutogenic or health-promoting aims. Initial results from cohort studies indicate that EYT can improve symptoms and quality of life (QoL) in patients suffering from chronic illnesses.1-3 Improvement of the modulation of the autonomic nervous system associated with better physical health, better performance, and better QoL.4-9 However, a decrease in various HRV parameters is associated with many chronic diseases. 10 Studies conducted in healthy individuals show that various types of mental stress decrease vagal activity by withdrawal of the high-frequency component of HRV.11,12 Psychometric data always have a subjective element and can potentially be biased by various factors (desire to please, etc). It is known that psychophysiological stress is relayed to the body by the hypothalamic–pituitary–adrenal axis (neuroendocrine route, eg, cortisol) and the sympathetic nervous system (neuronal route, eg, catecholamines) as the 2 main pathways. 13 Therefore in this study, in addition to the questionnaires, we also performed measurements of HRV as an objective noninvasive measurement of cardiovascular physiology. The significance of HRV in this context is that in many illnesses improved HRV is associated with a better clinical course,14-19 response to a therapeutic intervention or improved QoL.20-23 It can thus be regarded as a kind of “salutogenic marker” on a functional physical level, as HRV is modulated by diverse neuronal, humoral, physical, and emotional factors.24-26
A general reduction in the modulation of the autonomic nervous system is found in patients with major depression,14,27 heart attack,15,28 and diabetes mellitus16,29,30 and is a reliable predictor for complications and poor prognosis after myocardial infarction, 31 for example. In reverse, a favorable course or response to a treatment can be associated with improvement of HRV parameters26,31,32 and can be reflected in a measurably better QoL in both healthy4,8 and sick subjects.17,22,33-36 In patients with cancer, it was shown that autonomic nervous system (ANS) dysfunction can occur in the course of the illness. 37 Up to 80% of patients with advanced disease can show dysfunction of the ANS and specifically deterioration of HRV. 37 The significance of this ANS dysfunction for patients with cancer is not yet fully understood, but some investigations have shown an association with worse survival. 37 There are, however, relatively good data on the association of stress, fatigue, and HRV. 38 Patients with chronic stress or fatigue can show reduced HRV. As stress and fatigue are symptoms often found in patients with cancer it would seem appropriate to measure HRV parameters as a physiological outcome parameter of mind–body therapies in addition to psychometric data. Improvement of HRV parameters has been shown for some mind–body therapies.39,40
It is known that body therapy approaches and meditation techniques from the field of complementary medicine or nonpharmacological techniques, such as yoga,41,42 t’ai chi, Qigong,43,44 or even merely reciting a poem, 45 for example, can have a positive influence on HRV. We were also able to show this for EYT. 46 Yoga41,42 and cyclic meditation 47 have also been shown to have longer term physiological effects on HRV parameters. It was found for both yoga and meditation that the long-term effect takes the form of stimulation of the ANS with a shift toward vagal dominance.
EYT is often used in patients with cancer. The prime goals in this case are to improve quality of life, reduce stress, treat fatigue symptoms, and also to support pain control treatment. As there are practically no clinical data available as yet, we were interested in the general effect of EYT in stressed but healthy subjects as a model.
This article focuses on a subgroup of a larger controlled nonrandomized study on the impact of a 6-week eurythmy therapy training on stress coping strategies and health-related quality of life in healthy middle-aged subjects. 48 The aim of present analysis on a subgroup of 23 subjects (single-arm) who consented to electrocardiogram (ECG) recordings was to determine the physiological effect of a 6-week course of EYT therapy on healthy but stressed subjects and to establish whether the known short-term improvement in HRV 46 is also detectable in the long term. Within this pre–post analysis of the EYT group only, a special focus of the HRV study was to evaluate nonlinear HRV parameters 49 (symbolic dynamic) known to be associated with psychopathological changes such as depression and their established propinquity to the clinical burnout—or depressive symptomatology. 14 These investigations will provide first scientific data on the effect of EYT with regard to its frequent use in oncology.
Subjects and Methods
Study Design
The subjects were recruited from a population of teachers and nursery teachers. A total of 74 healthy subjects (no regular use of medication) aged between 31 and 59 years (mean age 45.97 years, 23 women) were admitted to the study after giving written informed consent. The study was conducted as controlled (nonrandomized) two-arm study. Within the EYT group, 13 out of 68 subjects (19.1%) dropped out over the period of 6 weeks, compared with 3 out of 22 subjects in the control group (13.6%; Figure 1). There was no patient dropout within the group that consented to the ECG recordings affecting the present analysis. The EYT group and the control group were recruited separately from the same population and in the same space of time. The EYT group was given an intervention of 2 treatment sessions per week over a period of 6 weeks. Before the beginning of the EYT a baseline visit was performed in both groups at which the psychometric parameters were recorded. Because of limited technical capacity, only 30 subjects participated in the ECG recordings. The subjects in the EYT group had to consent separately to the ECG recordings and were included in order of appearance. The level of activity was controlled by requesting the subjects to do no special sportive or other unusual activity, to drink no alcohol, and not to consume stimulative substances. In the EYT group (n = 30), 23 women consented to recording of a 24-hour ECG before and after the EYT (Figure 1). The HRV analysis was preplanned in form of a pre–post analysis of the subgroup that consented to these additional ECG recordings. Therefore, we did the analysis of HRV parameters exclusively in this subgroup of 23 women and not in the total of 55 subjects. The study was approved by the Ethics Committee of the Charité–Universitätsmedizin Berlin.
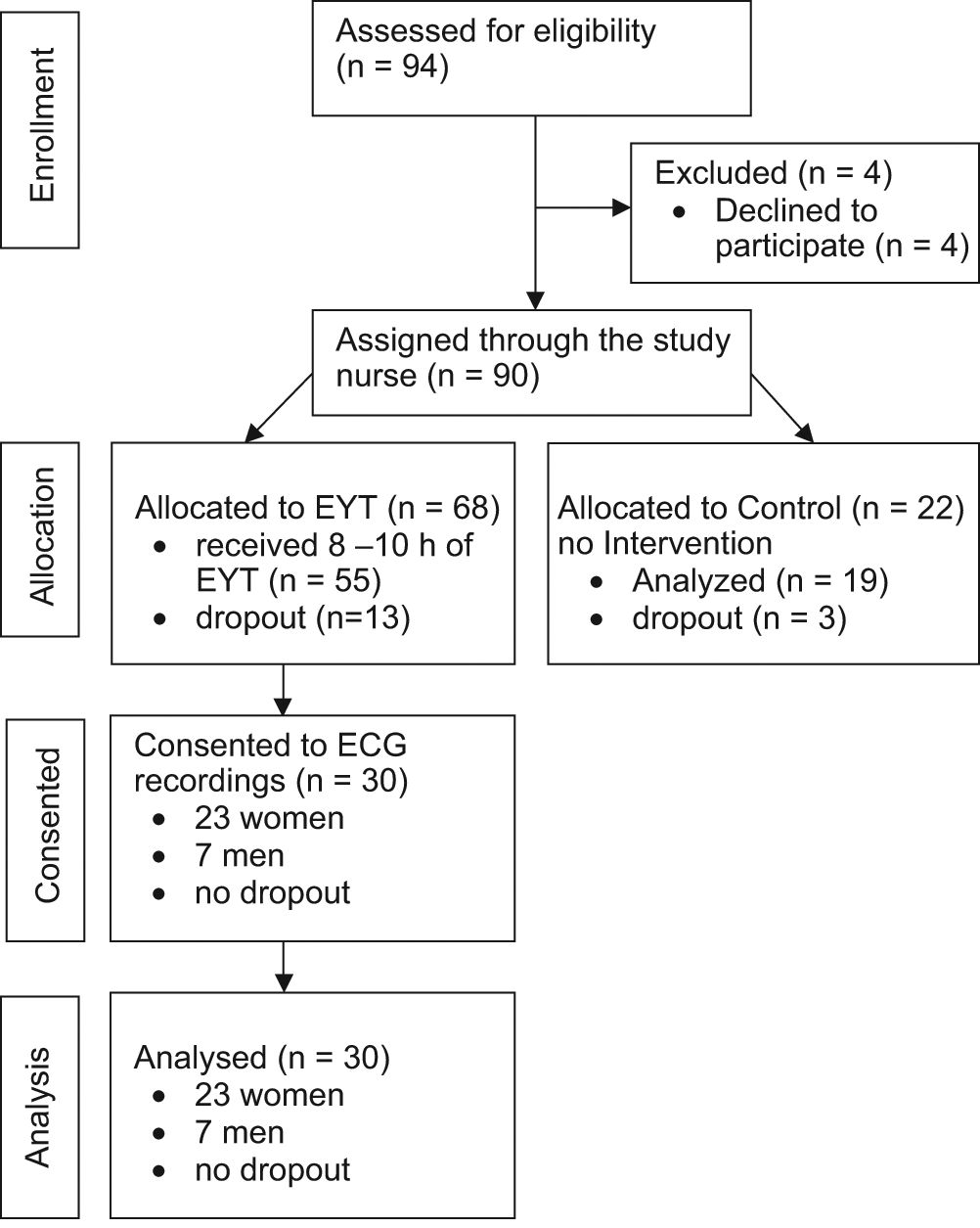
CONSORT diagram showing the flow of participants through the trial
Eurythmy Therapy Intervention
Two EYT therapists participated and conducted the training. The exercises were learned gradually over 2 weeks and repeated in each treatment unit (45 minutes) so that the subjects were able to perform them independently later. The sequence followed an identical pattern throughout the 6 weeks. The rhythm exercises are special EYT exercise sequences performed on the basis of the speech rhythms of verses or poems. Lyrical patterns or rhythms such as the hexameter (the classical meter of epic poetry), dactyl (a meter consisting of 1 heavy [long] syllable followed by 2 light [short]) syllables) or anapest (reverse of dactyl) or other variations are used. These involve rising and falling speech rhythms translated into movement, and acceleration and deceleration. In addition, ball exercises, rod exercises, stepping exercises, and central speech sound exercises with consonants (L and M) formed a part of each treatment unit. The essential element of these movement exercises is the alternation between tension and relaxation and a harmonious relationship between inhalation and exhalation. For the emotional (soul) sector, exercises on spatial orientation and boundary formation and geometric exercises for inner structuring (iamb and trochee) were used. This was followed by speech sound exercises with vowels: O, E, U, and soul exercise with E. Concluding exercises with a meditative character in combination with physical movement were, for example, “I have calm within myself, I have within me the forces that give me strength.” These EYT exercises were chosen because we supposed that this combination will have some impact on the HRV as well as on the clinical outcome parameters concerning QoL and stress.
Heart Rate Variability
From the raw 24-hour ECG data, time series of heart rate (tachogram) consisting of beat-to-beat intervals (BBI) were extracted. To obtain normal-to-normal (NN) heart beat time series, ectopic beats and disturbances or artifacts were interpolated in the given BBI series applying an adaptive variance estimation algorithm. 50
On the basis of the guidelines of the Task Force of the European Society of Cardiology, 51 the following HRV standard indices from the time and frequency domains were calculated from the tachograms.
Time domain
meanNN = mean value of NN interval time series (milliseconds)
sdNN = standard deviation of NN interval time series (milliseconds)
rmssd = square root of the mean squared differences of successive N intervals (milliseconds)
Frequency domain
Power spectra were calculated by applying fast Fourier transform with a Blackman Harris window of equidistant NN interval time series. To obtain equidistant time series, the tachograms were linearly interpolated and resampled at 10 Hz. From the spectrum the following indices were calculated:
ULF = power in the “ultra low” frequency band <0.003 Hz
VLF = power in the “very low” frequency band 0.003 to 0.04 Hz
UVLF = power in the frequency band 0.0 to 0.04 Hz
LF = power in the “low” frequency band 0.04 to 0.15 Hz
HF = power in the “high” frequency band 0.15 to 0.4 Hz
LF/HF = ratio of LF to HF power
LFn = LF power normalized as LFn = LF/(LF + HF)
HFn = HF power normalized as HFn = HF/(LF + HF)
LF/P = LF power normalized by the total power P
HF/P = HF power normalized by the total power P
P = total power in the band 0.00 to 0.4 Hz.
In addition, P-normalized indices (eg, LF/P) were calculated to illustrate the change in this frequency component in relation to the total power.
Symbolic dynamics
Symbolic dynamics is a nonlinear method that describes the global short- and long-term dynamics of beat-to-beat variability on the basis of symbolization. Methods of nonlinear symbolic dynamics analysis50,51 have been shown to be sufficient for the investigation of complex systems and describe dynamic aspects within time series. The method applied in this study (there are different approaches for deriving symbolic dynamics from a time series) is described in detail elsewhere; 50 in the following only a brief introduction is given. The NN beat-to-beat interval time series are converted into an alphabet of 4 predefined symbols (0, 1, 2, 3) according to the transformation rules based on consecutive comparison of successive BBIs. The symbols “0” and “2” reflect slight deviations (increase or decrease) from the mean NN interval, the symbols “1” and ‘3’ reflect stronger deviations (increase or decrease over the mean NN interval and in addition over a predefined limit). Then, the symbol strings are transformed into word series where each word consists of 3 successive symbols. This leads to a range of 64 different word types (000, 001, . . ., 333). Then we estimate from the word distribution the probability of occurrence (pWxxx) of each word type (xxx = 000, 001, . . ., 333) within NN interval time series. As an example, the word type 321 (consisting of the successive symbols 3, 2, 1) represents sequences of 2 decreasing BBIs followed by an increasing one and can be interpreted as a fast heart rate downregulation after a heart rate increase.
Statistics
The nonparametric Wilcoxon rank-sum test was applied for the statistical analysis of twice paired samples. The evaluation was performed on the basis of the ECGs of each subject before and after EYT. Values of P < .05 were regarded as statistically significant and values of P < .001 as highly significant.
Results
Heart Rate Variability
The ECG data from the 23 women (mean age = 42.2 years; SD = 8.2) were evaluated. Indices from the frequency domain showed a significant decrease in the region of the ultra low and very low frequencies as normalized ([ULF + VLF]/P) as well as nonnormalized indices (ULF and VLF) compared with the respective baseline measurements. This reduction of slow-range frequencies can be seen in Figure 2. In contrast to this, the normalized (related to the total power) LF and HF components LF/P and HF/P increased considerably in comparison to baseline. The beat-to-beat intervals (meanNN) and the standard deviation sdNN remained unchanged. The LF/HF ratio showed a decreasing trend (indicating increasing vagal activity), which was not, however, significant. LFn and HFn (representing more the autonomic tone) show a trend toward a more vagally dominated regulation, however, this is not statistically significant either. Table 1 shows the significant parameters differentiating between pre-EYT and post-EYT in comparison to the standard indices meanNN (or heart rate) and sdNN. The symbolic dynamics index pW321 showed a significant increase following the EYT.
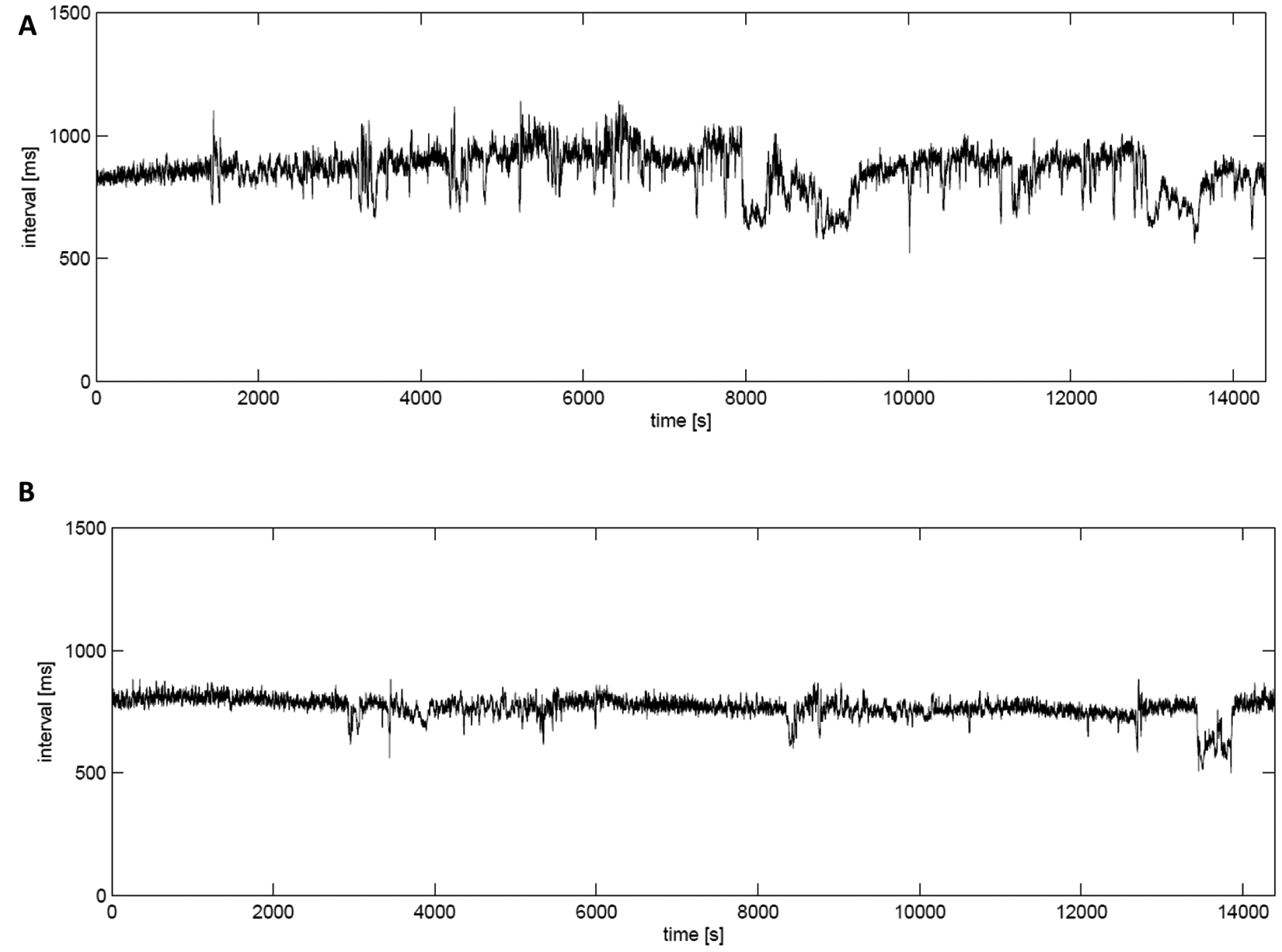
Example of reduced slow-range oscillations of the instantaneous heart rate (A) before and (B) after the eurythmy therapy exercise period of 6 weeks
Results of HRV Analysis a

Abbreviations: HRV, heart rate variability; EYT, eurythmy.
20 hours, females, average, and standard deviation of HRV parameters at baseline and after cessation of the training.
P is the univariate significance: *P < .05, **P < .01, ***P < .001, NS, not significant.
Discussion
In this study, we examined the long-term physiological effect of a 6-week course of EYT on relevant HRV parameters in 23 healthy moderately stressed middle-aged women after a 6-week EYT training. As we have shown in a previous published article, 52 there was a marked long-term improvement in health-related QoL, fatigue scores, and stress coping in comparison with the control group and over time. There was also a significant improvement on the AVEM (German questionnaire for Work-Related Behavior and Experience Pattern), a diagnostic instrument for burnout syndrome or a development in this direction.
In this physiological analysis, we detected that after the 6-week EYT training, there was a decrease in the very low frequency range (ULF, VLF), which indicates a decline of activity of the rennin–angiotensin system (RAS), 53 thermoregulation, and vasomotor activation. 54 This shift of the LF range can be interpreted as a slowdown leading to stress reduction consistent with the described improvements in QoL and on the AVEM scales. Moreover, the ULF and, partly, the VLF are also markers for physical activity.55,56 A reduction in the values of these indices could probably be because of a reduction of movement caused by a more relaxed behavior. Therefore we conclude that the physiological HRV data show congruently that the psychometrically measured changes can also be demonstrated physiologically indicating that the subjects not only deal more coolly and calmly with stress and are more composed but are also more physically active, and that they experience this as a gain in QoL.
Furthermore, in the higher frequency range there was an increase in HF/P as well as an increase in LF/P after training, suggesting a significant within-group training effect. Accordingly, the LF/HF ratio was not significantly changed, reflecting an unchanged autonomic balance. Several studies of longer phases of yoga training or cyclic meditation have been shown to result in improved autonomic control with an increase in parasympathetic input as measured by HF/P.41-44
In a previous controlled cross-over study on EYT, we analyzed the short-term effect on HRV measurements. In this controlled clinical study in healthy volunteers, we were able to show that EYT had a positive impact on HRV parameters 46 of cardiac physiology compared with corresponding ergometer training. We found a significant improvement in HRV parameters in the EYT group in comparison with ergometer training, and the improvement persisted for a certain time after the training phase. Following the EYT, relaxation was qualitatively and quantitatively considerably more marked in the EYT group, as measured by a significant decrease in the LF/HF ratio. It is an interesting finding that a similar effect is seen after a single EYT session. Here, deep relaxation predominates, reflected in a marked increase in the lower frequency spectrum and a decrease in autonomic balance (LF/HF) toward parasympathetic dominance. 41 We postulate that these parasympathetic effects probably occurred after each EYT session in the current and in our previous study and may result in a cumulative long-term effect.
However, the physiological influence and transformation over a longer period of time is not easy to analyze. The data of this study reflect a positive long-term influence on the entire ANS toward a marked slowdown of lower frequencies and enhanced autonomic balance. In the clinical context of reduced fatigue symptoms it seems possible that the increased HF/P power could explain a better sleep quality. This could be because of the fact that acute psychophysiological stress is known to be associated with decreased levels of parasympathetic modulation, as measured by a decreased HFn component, leading, for example, to disturbed sleep especially in rapid eye movement phases. 57
Complexity is an HRV measure of cardiac health, for example, in coronary heart disease or dilated cariomyopathy. However, complexity also plays a role in psychiatric disorders. Patients with severe depression or schizophrenia show alterations in HRV in terms of diminished complexity. In the present study, a significant increase in complexity was seen after 6 weeks of EYT. The evidence for increased values of the HRV index pw321 from symbolic dynamics in the subjects presented here might be an indicator of a development toward a more optimal HRV pattern in terms of more dominant vagal regulation. The advantage of such nonlinear indices—in contrast to linear ones—is that they also consider intermittently occurring events. The index pW321 represents the number of short-term downregulations of the heart rate probably leading to a more health protective status whereas an increased heart rate is accompanied with an increased risk. 58 It has been shown 51 that this parameter pW321 significantly differentiates between physiological and pathophysiological regulation even in different cardiac diseases. This type of pattern was also described in studies of Porta et al 59 and Guzzetti et al. 60 In their studies, the authors were able to demonstrate that such heart rate downregulation patterns are fragments of faster waves (eg, HF oscillations). At rest, mainly these classes are detected because of the contemporaneous presence of LF and HF oscillations. All these findings are supported by the linear indices LF/HF, LFn and HFn showing a trend to a more vagal activity although this was not statistically significant.
Finally, it has also been shown 61 that in normotensive individuals, moderate and intense exercise conditioning improves autonomic factors; for example, parasympathetic indices, including baroreflex sensitivity, increase, whereas sympathetic indicators decrease.
Another explanation for this increase in fast heart rate downregulations could be that the pattern of baroreflex regulation and/or the number of baroreflex occurrences was changed after EYT. The baroreflex is responsible for maintaining blood pressure. If the blood pressure increases considerably the heart rate is downregulated (pW321 represents such a downregulation) by the baroreflex. It has been demonstrated that on one hand, patients with dilated cardiomyopathy show a significantly reduced baroreflex sensitivity and a 40% to 50% lower number of correlated blood pressure–heart rate fluctuations (baroreflex activities) than controls. 62 On the other hand, we might speculate that an increase in the number of correlated blood pressure–heart rate fluctuations (as found in this study) indicates more optimum short-term blood pressure regulation. However, this hypothesis cannot be proved here because no data on blood pressure were available. Altogether, these parameters are particularly suitable for predicting cardiac mortality and other diseases.
The HRV parameters are congruent with the psychometric data and objectify the positive clinical changes and contribute to explanation of the psychological and physiological changes. Basically, with the salutogenic exercises, EYT is also aimed toward treating states such as burnout syndrome or depression. It is therefore an interesting observation that in this study low-level physical exercises combined with additional meditative exercises were able to alter behavior patterns that are relatively difficult to change and usually the province of psychotherapy, even though this was not consciously reflected. The subjects did not know, for example, that the AVEM was a test of this area.
The results of this study suggest that there are complex physiological mechanisms of the ANS that can be therapeutically influenced by various means of complementary as well as conventional medicine. Generally, a better understanding of the functioning of the ANS and the interactions, for example, with the brain, hormones, or extrinsic factors, which can influence the efficacy of therapeutic interventions or lifestyle modifications,24,25 remains a challenging but important and clinically relevant issue. 23
Against the background of these clinical data, the current use of EYT in oncology, for example, appears to be an interesting therapeutic option, which is also supported by objective evidence. In addition to the improvement of ANS dysregulation and reduction of fatigue symptoms, improved self-regulation and QoL also appear to be relevant and realistic goals. These should be investigated prospectively in patients with cancer as the next step.
Limitations of the Study
For organizational reasons, it was not possible to randomize the study. Therefore, the 2 groups were enrolled separately, which is still considerably better than allowing the subjects to choose. Nevertheless, randomization would have been qualitatively better. We therefore cannot rule out the possibility that the EYT group might have contained preferentially subjects who believed that they could benefit from a treatment aimed at stress reduction and improvement of QoL. However, this only affects the comparison of the psychometric data and not the HRV analysis. Furthermore, we are aware of the influence of respiratory rates on HRV parameters. Unfortunately, it was not feasible to monitor respiration for 24 hours in this setting. It was beyond the scope of this study to have completely standardized conditions as we were interested in real-life effects. Because of limited availability of male subjects, we have an unbalanced male/female ratio in this study with a majority of women. Therefore, the subsequent analysis was based exclusively on the data of these women. This might consequently result in a gender bias.
Conclusion
EYT is a movement therapy from anthroposophic medicine, which, when used in healthy subjects, can lead both immediately and in the long-term to improvement of QoL, activity, and stress coping. Examinations of HRV confirm this and show a positive change in autonomic regulation toward a more relaxed pattern and an improvement of complexity in the region of high-frequency oscillations. Statements on precise functional connections remain speculative. Further controlled studies should be performed to examine the clinical efficacy of EYT, for example, in patients with cancer at risk of depression, stress, fatigue, or burnout syndrome, as these clinical symptoms are associated with reduced HRV.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
This work was supported in part by SOFTWARE AG–Stiftung, Darmstadt, Germany, Zukunftsstiftung Gesundheit, HELIXOR Stiftung Rosenfeld, Stiftung zur Förderung der Heileurythmie, Stuttgart, Germany, and Dr Hauschka Stiftung, Stuttgart, Germany.