
Abstract
Introduction
According to Global Cancer Statistics (2018), the global cancer burden has risen to 18.1 million new cases and 9.6 million cancer deaths. 1 The most common symptoms that patients with cancer exhibit are pain and fatigue as a result of treatment. 2 Additionally, in the general population, depression and anxiety affect up to 20% and 10% of patients with cancer, respectively, in contrast to 5% and 7%, respectively, in the past year. 3 Muscle dysfunction is also a common phenomenon in cancer, where patients across a wide range of diagnoses are subject to impaired muscle function. 4 Because patients with cancer experience various symptoms, their quality of life (QOL) is of major concern. 5 Muscle dysfunction and sarcopenia have been associated with poor performance status, increased mortality risk, and greater prevalence of treatment side effects. 6 However, as indicated by systematic reviews and meta-analyses, physical exercise has beneficial effects on QOL, 7 muscle strength, muscle function, and aerobic fitness, 8 and cancer-related fatigue in patients with cancer.9 -11 Adults with cancer are advised that exercise can provide QOL and fitness benefits during or after treatment. Systematic reviews examining patients with all cancer types have shown the positive influence of physical exercise on QOL during the course of active treatment. 12
Physical exercise can also be an effective method of improving the patient’s exercise capacity, physical and cardiovascular function, and strength. It can also lower the risk of cancer recurrence and improve the odds of mortality. 13 Another review also showed that patients with cancer who performed physical exercise following their diagnosis were observed to have a lower relative risk of cancer mortality and recurrence and experienced fewer or less severe adverse effects. Therefore, it is safe to speculate that physical exercise is an important adjunct therapy for cancer. 14 This systematic review and meta-analysis of randomized controlled trials (RCTs) aimed to determine how physical exercise, such as resistance exercise and aerobic exercise, affects mortality and recurrence in patients with cancer at all survival time.
Methods
Protocol
We adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. 15 We used a prespecified protocol, registered with PROSPERO (CRD:42019140268).
Search Strategy
Literature searches were conducted in MEDLINE, CINAHL, the Cochrane Library, Scopus, ProQuest, and PEDro for articles published before May 2019. The search strategy was conducted on the aforementioned databases based on the following MeSH terms: “cancer,” “tumor,” “randomized controlled trial,” “exercise,” “rehabilitation,” and “physical therapy.” The phrase “disorder for cancer” was also used for the search (eg, lymphoma, hematopoietic malignancy, carcinosarcoma). In addition, the words “mortality,” “recurrence,” and “prevalence” were added to the search terms.
Selection Criteria
The inclusion criteria consisted of randomized controlled clinical trials that included patients with cancer and cancer survivors in any setting; the intervention group performed physical exercise and its effects on mortality were evaluated. Systematic reviews, editorials, cross-sectional studies, case reports, and case series were excluded. Exercise guidance was also excluded from the intervention. A control group, which did not receive any (major) exercise intervention, was used for comparisons. The different stages of study selection are shown in Figure 1. The titles and abstracts of all retrieved articles were screened by 5 independent reviewers to ensure their eligibility. Full-text articles were retrieved for review when there was an indication that they met the inclusion criteria or when there was insufficient information in the abstract and title to make a decision. To perform meta-analysis, data details were examined. Final inclusion of eligible RCTs was determined in consensus meetings in which all authors participated.

Study flow diagram of the selection process.
Data Extraction
Two reviewers were responsible for data extraction. When the data in the full text of an article were deemed insufficient, the authors of the article were contacted by email for further information. The following data were extracted from each included study: first author’s last name, publication year, cancer type, sample size, type of exercise, duration and timing of exercise, and observation period. Mortality, recurrence, and prevalence data were selected for meta-analysis.
Quality Assessment
Assessment of the methodological quality of studies, including their risk of bias, was conducted using the Cochrane tool for assessing risk of bias. 16 This tool includes the following 7 domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other potential sources of bias. Two trained reviewers scored each item according to the criteria established by Higgins et al in 2011. 16 Potential disagreements were resolved during consensus meetings with all authors present. The quality of studies was rated using the Grading of Recommendation Assessment, Development, and Evaluation (GRADE) criteria. 17
Data Analysis
All statistical analyses were conducted using the Review Manager software, version 5.1. 18 We calculated the risk ratio (RR) for each report to investigate the effect of exercise on mortality and recurrence. The standardized mean difference with 95% confidence intervals (CIs) was calculated for quantitative indices. The random-effect model was used as the pooling method. We also assessed the statistical heterogeneity using the I2 statistic. Furthermore, we adopted the levels of I2 that were suggested by the Cochrane Handbook for Systematic Reviews of Interventions (I2 values of 0%, 25%, 50%, and 75% represented no, low, moderate, and high heterogeneity, respectively). The threshold for interpreting the I2 value can be misleading. Therefore, we determined the importance of the observed I2 value by assessing the magnitude and direction of the effect, as well as the strength of evidence for clinical heterogeneity.
Results
Study Selection
The database searches retrieved 2868 references, which were reduced to 2698 after the exclusion of duplicate articles. The remaining 2698 studies were screened by title and abstract, resulting in the exclusion of 2384 studies due to irrelevant study designs or discrepancies regarding the population or the intervention type. A full-text review was performed for 314 RCTs, and 306 RCTs were excluded. Figure 1 shows the outcome of the search and study selection process. The included studies were conducted in the following countries: 3 in Germany,19 -21 2 in Australia,22,23 and 1 each in Canada, 24 the United States, 25 and Switzerland. 26
Study Characteristics
Detailed characteristics of the 8 RCTs are shown in Table 1. Subjects in 2 of the RCTs23,24 were patients with breast cancer postsurgery. These studies showed that aerobic exercise and resistance exercise had a positive effect on the survival of cancer patients. In other RCTs, the subjects were patients who were diagnosed with lung cancer. In this study, aerobic exercise had a positive effect on the survival period. 22 Patients in other RCTs 26 received any intervention before surgery. This study showed that high-intensity interval training resulted in mortality reduction. One RCT was intended for patients who were candidates for allogeneic hematopoietic stem cell transplantation. 21 The rest of the RCTs included patients with various cancer diagnoses,19,20 with one of the RCTs targeting patients with cancer who had heart failure. 25 This study showed that aerobic exercise had an effect on the reduction of all-cause mortality.
Characteristics of the Included Studies.

Abbreviations: Ex, exercise group; Con, control group; VO2max, maximum rate of oxygen consumption; DFS, disease-free survival; DDFS, distant DFS; RFI, recurrence-free interval; MET, metabolic equivalent of task; PFS, progression-free survival; NRM, non-relapse mortality; TM, total mortality.
Interventions in the RCTs were roughly classified into 2 categories: a short-term intervention rehabilitation program (with a duration of 2 weeks) that was performed in a hospital setting19,20 and ambulatory treatment or home exercise (with a duration of 2-8 months) for long-term outpatients.21 -26 Regarding the content of the interventions, aerobic exercise and/or resistance training was conducted in all RCTs.
Study Quality
Risk of bias assessment is shown in Figures 2 and 3. Risk of bias for other bias domains varied across the included studies. Due to the nature of the interventions, it was expected that blinding of the participants and the personnel who delivered the interventions would be impossible. Consequently, the risk of performance bias in all studies was high. The quality of the studies rated by GRADE was moderate in each outcome (Table 2).
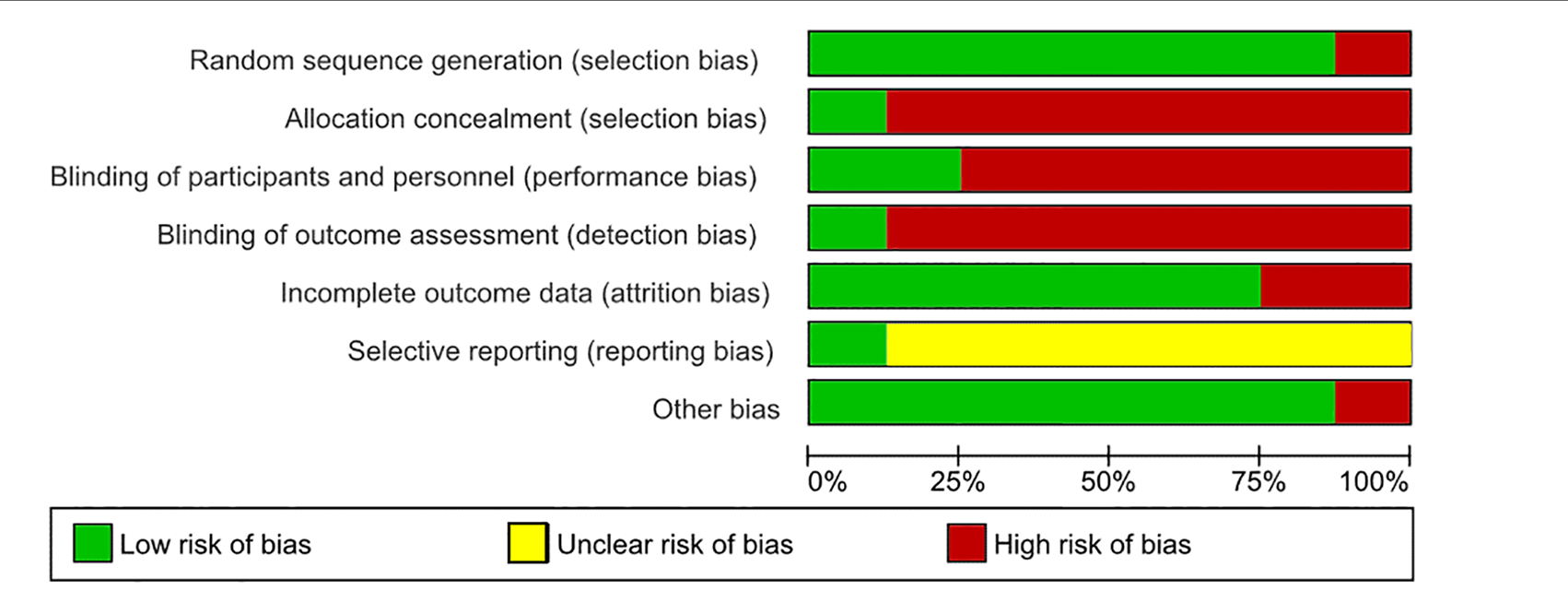
Risk of bias graph based on the Cochrane Collaboration’s tool for assessing risk of bias.

Summary of risk of bias based on the Cochrane Collaboration’s tool for assessing risk of bias.
GRADE Evaluation.

Abbreviations: GRADE, Grading of Recommendation Assessment, Development, and Evaluation; CI, confidence interval; RR, risk ratio.
All studies were judged to include a risk of bias.
Effect of Exercise on Risk of Mortality and Recurrence
As a result, 9 exercise groups from 8 RCTs were included in a random-effects meta-analysis. This analysis comprised 656 patients in the exercise groups and 579 patients in the control groups. The efficacy of exercise in terms of risk of mortality and recurrence in patients with cancer was then estimated using a forest plot.
The meta-analysis of 9 exercise groups from 8 RCTs showed that physical exercise significantly reduced the risk of mortality in patients with cancer and in cancer survivors (RR = 0.76, 95% CI = 0.40-0.93, I2 = 0%, P = .009, n = 1235; Figure 4).

Risk ratio for the effect of exercise on mortality in cancer patients and survivors.
Cancer recurrence data were available in only 2 RCTs,23,24 one of which included 2 exercise groups. Thus, meta-analysis of 3 groups from 2 RCTs was performed, showing the effect of exercise on significant reduction of recurrence risk in cancer survivors (RR = 0.52, 95% CI = 0.29-0.92, I2 = 25%, P = .030, n = 661; Figure 5).

Risk ratio for the effect of exercise on recurrence in cancer survivors.
Discussion
This systematic review and meta-analysis attempted to examine the evidence regarding the benefits of physical exercise on mortality and recurrence in patients with cancer. This review included breast, lung, hematological malignancy, and various cancer diagnoses. To the best of our knowledge, this is the first meta-analysis to determine the effects of exercise on mortality and recurrence in patients with cancer. Our quantitative analysis indicated that there is evidence to support the notion that physical exercise can improve the rates of mortality and recurrence in patients with cancer.
This meta-analysis also revealed that exercise interventions positively affect mortality rates in patients with cancer. The existing literature has shown the benefits of physical exercise training in patients with heart failure, including the reduction of cardiovascular mortality rates. 27 Physical exercise has also been shown to improve exercise tolerance and QOL in patients with chronic obstructive pulmonary disease (COPD), as well as reduce hospital admissions and mortality rates. 28 Another study showed that physical exercise interventions improve exercise capacity in patients with chronic kidney disease (CKD) and may reduce the risk of mortality. 29 Patients with cancer may receive the same reduced mortality benefits from physical exercise as do patients with heart failure, COPD, and CKD. A previous report showed that physical activity was associated with significantly decreased hazards of cancer-specific and all-cause mortality in breast cancer survivors. 30 In addition, the same study also illustrated that physical exercise can reduce cardiovascular mortality among breast cancer survivors. 30 Furthermore, the intensity of leisure-time physical activity should be at least moderate, so that the beneficial effects of reducing overall cancer mortality can be achieved. 31 Promoting physical activity of any intensity and duration is an important approach in reducing mortality risk in the general population. 32 A dose-response association has also been observed between total leisure-time physical activity and risk of cancer-specific mortality. More vigorous physical activities have added benefits in the reduction of mortality rate in contrast to moderate physical activity. 32 Increasing physical activity after or during an exercise intervention may have an effect on the reduction of mortality rates in patients with cancer. The American College of Sports Medicine reported that physical exercise (among others) is associated with numerous health benefits, including lower risk of cardiovascular disease, type 2 diabetes mellitus, some forms of cancer, and age-adjusted all-cause mortality. 33 Exercise also contributes to the increase of muscle strength, muscle mass, and aerobic exercise stamina in patients with cancer.
This meta-analysis also showed that exercise has a positive effect on recurrence in patients with cancer. More particularly, an exercise intervention may help reduce the risk of recurrence of breast,34,35 colorectal, 36 and prostate 37 cancers. Moderate exercise seems to exert a protective effect on the immune system of the general population. 38 Dhabhar 39 suggests that the immunopotentiation from moderate exercise is due to the bidirectional effect of stress hormones on immunity, where subtle elevations are beneficial, whereas significant and sustained elevations (as seen with prolonged and/or intensive exertion) are detrimental to the host. The function of the immune system during or after anticancer therapy is important to cancer outcomes such as complications and/or the risk of recurrence. 40 Strengthening the immune system may help patients with breast cancer at increased risk of disease recurrence. 41 The knowledge of fundamental immunology suggests a suitable appreciation of the role of physical exercise in reducing the risk of cancer recurrence. 40 Furthermore, it is reported that exercise can induce apoptosis of cancer cell and inhibit the growth of cancer in animal and in vitro experiments, although the mechanism of these effects of exercise is not clear.42,43
For the findings we obtained in this study, there is no particular limitation on the type of cancer to target, and the patient population may or may not have been treated for cancer. In addition, resistance training and aerobic exercise are listed as exercise interventions, so patients with high performance status are assumed to have been targeted (the intervention for patients with low performance status needs to be considered).
This review had several limitations that should be considered. The number of studies was too small for in-depth analysis with stratification according to cancer type, treatment time frame, and type of physical exercise. Particularly, this review included various cancer diagnoses including breast, lung, hematological malignancy, and other cancers. Physical symptoms and functions were distinguished by cancer type. This meta-analysis included 8 RCTs that examined the following physical exercise types: aerobic exercise, resistance training, or a combination of the two. Differences in the types of physical exercise may have had an impact on mortality and recurrence rates in patients with cancer. In addition, false-positive results could not be excluded because trial sequential analysis could not be performed. Finally, this review was limited to studies published in English; relevant studies published in other languages may offer other findings.
Conclusion
This systematic review and meta-analysis demonstrated that physical exercise has a positive effect on mortality and recurrence rates in patients with cancer. However, the existing data may be insufficient for determining this potential beneficial effect. In conclusion, there is need for better understanding of the different types of cancer, different treatment time frames, and the implementation of an exercise intervention, as well as the best objective or subjective measure for RCT studies.
Footnotes
Author‘s Note
Jiro Nakano is also affiliated with Kansai Medical University, Osaka, Japan.
Author Contributions
SM and JN made substantial contributions to the conception and design. YH and JN were accountable for collection and assembly of data. SM, YH, TF, TT, and JN performed the literature search and data analysis. SM, YH, TF, TT, JBF, and JN were major contributors in drafting and writing the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partly supported by a Grant-in-Aid for Niigata University of Health and Welfare, as well as the MD Anderson Cancer Center Support Grant CA 016672.