
Abstract
Keywords
Introduction
Based on the international GLOBOCAN survey 2012, colorectal cancer (CRC) was the third most common cancer in men and the second most common in women. The age standardized rate (ASR), as cases per 100 000 of population, showed higher incidence in Europe (37.3 males; 23.6 females) and northern America (30.1 males; 22.7 females) compared with eastern Asia (22.4 males; 14.6 females). 1 In China, CRC was the fifth most common cancer in men and the fourth most common in women. 2 CRC incidence increased from an ASR of 12.8 (14.1 males; 11.5 females) in 2003 to 16.8 per 100 000 (19.7 males; 14.0 females) in 2011 and overall mortality rose from 5.9 to 7.8 per 100 000. 3
Chemotherapy-induced peripheral neuropathy (CIPN) is a side effect of a number of chemotherapeutic agents including oxaliplatin, cisplatin, vincristine, and taxanes. CIPN mainly affects the hands and feet and the typical symptoms include numbness, parathesia, pain, and hypersensitivity to mechanical and/or cold stimuli. 4 The overall prevalence of CIPN, based on a review of 31 clinical trials, was 68.1% within the first month following chemotherapy declining to 30% at 6 months or longer, however, prevalence varied considerably with the type of chemotherapy. 5 In CRC, oxaliplatin-based chemotherapies are a principal cause of CIPN. This involves an acute phase soon after infusion, which typically resolves, and a chronic type which is related to the accumulated dose of oxaliplatin and can persist for years. This type can significantly impair quality of life and may be a reason for ceasing adjuvant or palliative treatment for CRC.4,6 In a study of FOLFOX4 for metastatic CRC, there was neurosensory toxicity in 68% of patients, 16.3% of patients had cumulative paresthesia that interfered with function, and 3.8% ceased treatment after 4 months or more due to sensory neuropathy. 7 A study of FOLFOX4 and XELOX for metastatic CRC reported that grade III/IV neurosensory toxicity was about 17% in each regimen, whereas grade III hand-foot syndrome was 6% for XELOX versus 1% for FOLFOX4, and was 30% versus 10% for all grades. 8
Hand-foot syndrome (HFS), also known as palmar-plantar erythrodysesthesia, involves tingling, numbness and/or pain of the palms and soles complicated by edema, cracking, blistering and desquamation and hyperpigmentation. Of the drugs used in CRC, capecitabine and 5-fluorouracil (5-FU) can produce HFS, which, when severe, can lead to cessation of therapy.9,10
A number of interventions for the prevention or treatment of CIPN have been tested in clinical trials. The combinations of calcium gluconate and magnesium sulfate, vitamin E, and glutathione have all shown initial promise but no convincing effects in controlled clinical trials; however, duloxetine was found to improve symptoms due to oxaliplatin or paclitaxel.11-13 Monosialotetrahexosylganglioside sodium (GM-1) injection reduced CIPN due to oxaliplatin in a retrospective study and a prospective study.14,15 A number of other systemic and topical therapies are currently undergoing clinical trials. 12 The current management of HFS is mainly symptomatic with emollients, wound care, analgesics, and topical steroids for less severe reactions. A number of treatments have been trialed with promising results for turmeric 16 and silymarin. 17 However, effective therapies for higher grade HFS have yet to be confirmed.9,18
Previous reviews of CIPN have investigated the effects of (a) various Chinese herbs for oxaliplatin-induced CIPN in various cancers, 19 (b) the herbal formula Goshajinkigan in the prevention of CIPN in various cancers,20-22 (c) and lifestyle factors, including the use of herbal medicines and supplements in the management of CRC. 23
The present systematic review and meta-analysis focuses on randomized controlled trials (RCTs) that tested herbal medicines used in traditional medicine in China, Korea, and Japan in the integrative management of CIPN resulting from treatment for CRC. It aims to assess the effects of the herbal medicines on the prevention and treatment of CIPN and identify any promising directions for future research.
Methods
Searches were conducted of (a) major English language biomedical databases—PubMed, Embase, CINAHL, AHMED, and Cochrane Library; (b) major Chinese language biomedical databases—Chinese BioMedical Literature Database (CBM), VIP Database for Chinese Technical Periodicals (CQVIP), China National Knowledge Infrastructure (CNKI), and Wanfang Data from their respective inceptions to February 2018; and (c) reference lists in studies and reviews (Supplementary 1 PubMed search strategy). Only prospective RCTs were included.
Included participants had been diagnosed with colorectal, colon, or rectal cancer by pathology; had received chemotherapy; and were aged 18 years or older. Studies that included participants with other cancers or other diseases were excluded.
The test interventions were herbal medicines used in traditional medicine in China, Korea, and/or Japan. These could be administered orally and/or topically. Injections were excluded. Studies in which the details of the herbal therapy were unclear were excluded.
The control interventions were placebo for the herbal therapy, conventional chemotherapy or no additional intervention. Co-interventions were conventional chemotherapy for CRC plus usual care. The conventional therapies were required to be the same in each group. The study setting could be a hospital or clinic.
Studies that reported numerical data for an outcome directly related to CIPN and/or HFS due to chemotherapy for CRC were included.
Search results were screened by 2 reviewers and full-text articles were obtained for any paper considered a potential inclusion. These were assessed against the inclusion and exclusion criteria. Data were extracted to a predesigned spread-sheet for citation details (year, country; study design, duration, setting); methodological aspects; participant characteristics (number, age, gender, cancer type); details of interventions (herbal therapy, type of chemotherapy, type of conventional care); details of outcome measures; data for included outcome measures; safety, dropouts, and adverse events in each group. If there were any disagreements between reviewers, a third reviewer was consulted. In the case of discrepancies in the published data it was planned to contact authors but this was not required. Risk of bias was assessed using the Cochrane tool by 2 reviewers independently with a third reviewer available for consultation to resolve any issues. 24
Assessments of effect sizes were based on published data and conducted in Stata 12 or RevMan 5.3. Meta-analyses were conducted when studies were comparable and used the same outcome measures. Random-effects models with 95% confidence interval (CI) were applied. Heterogeneity was quantified as I2. Publication bias was assessed using a funnel plot and Egger’s test for asymmetry when ten or more studies were available. Subgroup analyses were planned based on participant characteristics such as cancer type (colorectal, rectal, colon); type of herbal intervention; type of chemotherapy; type of conventional care; and methodological quality. Sensitivity analyses were planned to explore sources of heterogeneity and any effects of the use of Chinese medicine syndrome differentiation.
Results
Sixty-three RCTs of herbal therapy for CIPN and/or HFS associated with treatment for CRC were identified (Figure 1). Three studies were conducted in Japan, none in Korea, and 60 in various locations in mainland China.25-87

Flow diagram of the search, screening, and inclusion process.
The studies enrolled 4286 participants ranging in age from 18 to 88 years. The mean ages ranged from 40 to 72.7 years (not all studies reported mean age). Fifty-two participants dropped out in total, so 4234 participants completed. These included 2509 males and 1738 females (not all studies reported gender). All participants were diagnosed with CRC in 52 studies, with colon cancer in 10 studies, and rectal cancer in 1 study. Twenty-two studies reported Chinese medicine syndrome differentiation (Table l). The most common feature of the syndromes was “spleen deficiency” Pi xu 脾虚 (Supplementary Table S4).
Characteristics of Included Studies of Integrative Herbal Medicine for Chemotherapy-Induced Peripheral Neuropathy and Hand-Foot Syndrome in Colorectal Cancer.

Abbreviations: CHM, Chinese herbal medicine; CRC, colorectal cancer; NS, no specific formula name; HIPEC, hyperthermic intraperitoneal chemotherapy; CIPN, chemotherapy-induced peripheral neuropathy; GM-1 injection, monosialotetrahexosylganglioside sodium injection.
Location at which the study was conducted: 1, China; 2, Japan.
Mentioned that syndrome differentiation was used.
One study 45 included 3 groups so it was included in 2 comparisons: herbal medicine versus XELOX and herbal medicine plus XELOX versus XELOX. Another study 73 involved 4 groups (n = 30 per group): (1) herbal medicine plus mFOLFOX6, (2) mFOLFOX6, (3) herbal medicine plus calcium gluconate and magnesium sulphate plus mFOLFOX6, and (4) calcium gluconate and magnesium sulfate plus mFOLFOX6. This study was included in 2 comparisons (groups 1 vs 2; and 3 vs 4).
Test interventions included: orally administered herbal medicine (58 studies) and topical herbal medicine (5 studies). All groups used a form of usual care. The chemotherapy regimens included: FOLFOX type in 37 studies (FOLFOX4, 19 studies; FOLFOX6, 2 studies; mFOLFOX6, 13 studies; FOLFOX, 1 study; FOLFOX series, 1 study; FOLFOX4/FOLFOX6, 1 study); XELOX, 17 studies; XELODA, 2 studies; XELIRI, 1 study; FOLFIRI, 1 study; SOX (S1 + oxaliplatin), 2 studies; and hyperthermic intraperitoneal chemotherapy (HIPEC), 2 studies. Five studies used a placebo for the herbal medicine. Study durations ranged from 4 weeks to 6 months but in some studies, treatment was discontinuous. Outcome data were available for CIPN (60 studies), and HFS (12 studies), with 9 studies reporting both outcomes.
The most frequently used herbal formula was Goshajinkigan (Niu che shen qi wan) 牛车肾气丸, which was tested in 3 studies (Table 1). Another 3 formulae were tested in 2 studies each: Qi fu long kui tang 芪附龙葵汤,80,86 Wei tiao san hao fang 微调3号方,30,66 and Xiao liu tang 消瘤汤.76,82 Some other formulae had the same names but different ingredients, so these were considered to be different formulae.
The herbs most frequently used in the oral formulae were the following: Astragalus membranaceus (n = 40), Atractylodes macrocephala (n = 38), Poria cocos (n = 36), Coix lacryma-jobi (n = 29), Glycyrrhiza uralensis (n = 28), Codonopsis pilosula (n = 25), Paeonia lactiflora (n = 21), Hedyotis diffusa (n = 18), Scutellaria barbata (n = 15), and Citrus reticulata (n = 14). The herbs most frequently used in the 5 hand and foot bath formulae were Carthamus tinctorius (n = 4), Astragalus membranaceus (n = 4), Cinnamomum cassia (n = 3), and Prunus persica (n = 3) (see Supplementary Tables S1 and S2 for Chinese names).
Risk of Bias
Of the 63 studies, 31 were judged as low risk for sequence generation since a proper method was described, three were judged high risk since a standard method appears not to have been used, and the remainder were unclear due to lack of information. Allocation concealment was described properly in 8 studies that were judged low risk, whereas the others did not mention this and were judged as unclear risk. For blinding, 5 studies blinded participants while 4 of these also blinded personnel and outcome assessors. These were judged low risk for these domains while the other studies which did not mention blinding were judged high risk. For incomplete outcome data, most studies had few if any dropouts and were judged as low risk, but in 2 studies some inconsistencies in dropout reporting led to a judgement of unclear risk. For selective outcome reporting, the majority did not have a protocol but reported on all outcomes mentioned in their methods, so these were judged unclear risk. The 2 studies for which protocols were available were judged low risk (Table 2).

Risk of bias categories: SG, sequence generation; AC, allocation concealment; BPt, blinding of participants; BPn, blinding of personnel; BOA, blinding of outcome assessment; IOD, incomplete outcome data; SOR, selective outcome reporting.
Risk of bias judgments: L, low risk; U, unclear risk or no information specified; H, high risk.
The difference in dropout rates between treatment and control groups did not exceed 20% in any study. Oki 2015 and Kono 2013 had an available protocol. Nishioka 2011 and Cheng 2017 had trial registration numbers but the protocols could not be accessed.
Studies of Orally Administered Herbal Medicine
The studies included 1 study of oral herbal medicine plus GM-1 injection versus GM-1 injection alone for CIPN, 78 1 study of herbal medicine versus chemotherapy, 45 52 studies of herbal medicine plus chemotherapy versus the same chemotherapy, and 5 studies of herbal medicine plus chemotherapy versus placebo plus the same chemotherapy.
Herbal Medicine Plus GM-1 Injection for CIPN
In 1 study (No. 54) all participants had CIPN due to previous oxaliplatin-based chemotherapy for CRC. 78 All received GM-1 injection for the CIPN and the test group also received the herbal medicine. Based on modified World Health Organization (WHO) criteria, 88 there was no significant difference in the incidence of grade III plus IV CIPN (relative risk [RR] 0.50 [0.05, 5.24]) which was very low in both groups, or in all grades of CIPN (RR 0.83 [0.66, 1.04], n = 64).
Herbal Medicine Versus Chemotherapy for Hand-Foot Syndrome
One study (No. 21) compared herbal medicine without chemotherapy with XELODA and reported data for HFS. 45 It included 3 groups (45 participants per group). All participants had advanced CRC and had previously received first-line chemotherapy. In this study, they were receiving maintenance treatment. The control group received XELODA as two 3-week cycles. There were no dropouts. For incidence of HFS after 2 months treatment there was no statistical difference between groups (RR 0.33 [0.04, 3.09], n = 90). The results for the herbal medicine plus XELODA arm are reported below.
Herbal Medicine Plus Chemotherapy Versus Chemotherapy
In 57 studies, an orally administered herbal medicine was combined with chemotherapy and compared to the same chemotherapy. In 5 of these studies a placebo for the herbal medicine was used in the control group.31,47,59,64
Chemotherapy-Induced Peripheral Neurotoxicity
Fifty-four studies reported on CIPN. Thirty-three studies used the WHO criteria, 7 studies used Levi’s modified WHO criteria, 88 10 studies used the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE) criteria, 2 studies63,64 used the Neurotoxicity Criteria of Debiopharm (DEB-NTC), and 3 studies did not specify the criteria. Meta-analysis results were reported separately for each of these outcome measures.
For WHO grades III plus IV CIPN, 17 studies had zero events in both groups so 14 studies were included in the meta-analysis (Table 3). For the pool of seven studies of FOLFOX4, there was no difference between groups (RR 0.41 [0.16, 1.04], I2 = 0%), but there was a significant reduction in the single study of mFOLFOX6 and there was a significant reduction in CIPN in the integrative therapy groups in the pool of 9 studies that used similar chemotherapies (RR 0.33 [0.16, 0.70], I2 = 0%). There was no difference between groups in the pooled result for 3 studies of XELOX or any of the other subgroups but the total result for 14 studies showed a significant reduction in the incidence of grade III/IV CIPN in the integrative groups (RR 0.42 [0.23, 0.77], I2 = 0%).
Integrative Herbal Medicine: Chemotherapy-Induced Peripheral Neurotoxicity (WHO Grades III + IV). a

Abbreviations: WHO, World Health Organization; CI, confidence interval; RR, relative risk; RCT, randomized controlled trial.
All studies used oral herbal medicines combined with chemotherapy versus the same chemotherapy.
Statistically significant.
These chemotherapy regimens all used oxaliplatin, 5-fluorouracil (5-FU) plus leucovorin (LV).
For all grades of CIPN (WHO criteria), 33 studies reported data, but 1 study had no events in both groups, so 32 studies were included in the meta-analysis (Table 4, Supplementary Figure S1). There was a significant reduction in CIPN in the pooled result for all 14 studies that used FOLFOX4 (RR 0.77 [0.66, 0.89], I2 = 0%) but there was no significant difference between groups in the subgroup of FOLFOX4 as adjuvant chemotherapy after radical surgery. In the pool of 18 studies of similar chemotherapies, there was a significant difference between groups (RR 0.70 [0.52, 0.96], I2 = 88%) but the heterogeneity was considerable. This was due to 1 study, 74 which reported that all participants had CIPN at baseline. When this study was removed from the pool, the heterogeneity was reduced to zero and the significant reduction in CIPN in the integrative therapy groups remained (RR 0.75 [0.66, 0.86], I2 = 0%, n = 1116). In the 10 studies of XELOX, the pooled result showed no difference between groups and there was no difference for SOX or XELIRI. In the total pool of 32 studies, there was a significant reduction in CIPN in the integrative therapy groups, but the heterogeneity was considerable (RR 0.78 [0.66, 0.91], I2 = 71%). When the study in which all participants had CIPN 74 was excluded the result was similar but without heterogeneity (RR 0.83 [0.76, 0.91] I2 = 0%). Seventeen studies employed syndrome differentiation. These found a similar result to the total pool but without heterogeneity.
Integrative Herbal Medicine: Chemotherapy-Induced Peripheral Neurotoxicity (WHO All Grades). a
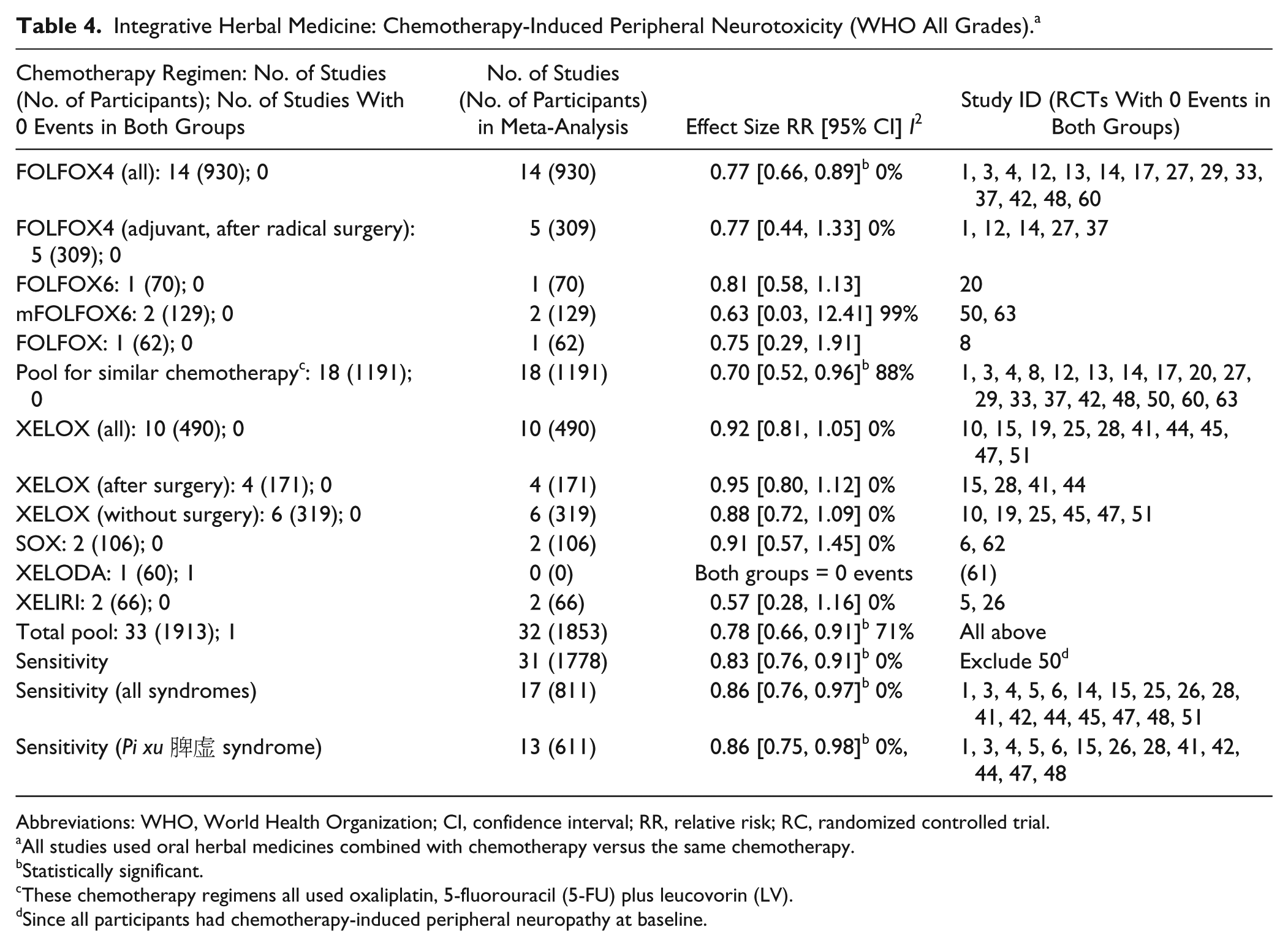
Abbreviations: WHO, World Health Organization; CI, confidence interval; RR, relative risk; RC, randomized controlled trial.
All studies used oral herbal medicines combined with chemotherapy versus the same chemotherapy.
Statistically significant.
These chemotherapy regimens all used oxaliplatin, 5-fluorouracil (5-FU) plus leucovorin (LV).
Since all participants had chemotherapy-induced peripheral neuropathy at baseline.
Seven studies used Levi’s criteria 88 (Table 5, Supplementary Figure S3). For grades III plus IV CIPN, the pooled result for 6 studies found there was a significant reduction in the integrative therapy groups (RR 0.28 [0.11, 0.69], I2 = 0%). For all grades, the pooled result for 8 studies showed a significant reduction in CIPN in the integrative groups (RR 0.54 [0.38, 0.76], I2 = 82.3%) but heterogeneity was considerable. This was due to 2 studies of FOLFOX regimens that reported high incidences of CIPN in both groups (70%-80%).62,81 When excluded in the sensitivity analysis, the pooled result of 5 studies remained significant without heterogeneity.
Integrative Herbal Medicine: Chemotherapy-Induced Peripheral Neurotoxicity (Levi 1992 Criteria). a

Abbreviations: CI, confidence interval; RR, relative risk; RCT, randomized controlled trial.
All studies used oral herbal medicines combined with chemotherapy versus the same chemotherapy.
Statistically significant.
These chemotherapy regimens all used oxaliplatin, 5-fluorouracil (5-FU) plus leucovorin (LV).
Studies ID 38 and 57 showed very high incidences of chemotherapy-induced peripheral neurotoxicity in both groups (70%-80%), both used FOLFOX regimens.
Ten studies used the NCI-CTCAE criteria for CIPN (Table 6, Supplementary Figure S4). Nine studies reported data for grades III plus IV but there were zero events in both groups in 2 studies, so 7 studies were pooled in the meta-analysis. The pooled result found no significant difference between groups (RR 0.65 [0.37, 1.13], I2 = 26.4%). For all grades, the pooled result for 9 studies showed there was a significant difference between the integrative therapy groups and the chemotherapy alone groups (RR 0.74 [0.58, 0.94], I2 = 13.5%). The pooled result for the 2 studies that used syndrome differentiation found a similar result without heterogeneity.
Integrative Herbal Medicine: Chemotherapy-Induced Peripheral Neurotoxicity (NCI-CTCAE). a

Abbreviations: NCI-CTCAE; National Cancer Institute Common Terminology Criteria for Adverse Events; CI, confidence interval; RR, relative risk; RCT, randomized controlled trial.
All studies used oral herbal medicines combined with chemotherapy versus the same chemotherapy.
Statistically significant.
These chemotherapy regimens all used oxaliplatin, 5-fluorouracil (5-FU) plus leucovorin (LV).
This group included 4 placebo-controlled studies. When these were considered separately, for grades III + IV there was no significant difference between groups (RR 0.64 [0.30, 1.39], I2 62%, n = 421) with the heterogeneity being due to 1 study (No. 40). 64 When this was excluded the result was significant (RR 0.44 [0.25, 0.76], I2 0%, n = 239) without heterogeneity. Only 3 of the placebo-controlled trials reported data for all grades, and the pooled result was not significant (RR 0.82 [0.46, 1.47], I2 = 61%, n = 332). The heterogeneity was again due to Oki et al. 64 When excluded, the result showed a significant difference (RR 0.70 [0.50, 0.96], I2 = 6%, n = 150).
One of the studies (No. 39) that used DEB-NTC reported data suitable for analysis. It compared the formula Goshajinkigan plus mFOLFOX6 versus mFOLFOX6. 63 Some participants also received bevacizumab. The rates of grade III CIPN after 10 cycles was 0% in the integrative therapy group and 12% in the control group. After 20 cycles of chemotherapy, the rates were 33% in the integrative group, and 75% in the chemotherapy alone group, but there were no statistically significant differences between groups with regard to the incidence of grade I or higher and grade II or higher CIPN. The percentage of grade II/III CIPN in each cycle was lower in the integrative group than the control group.
Three studies did not specify the criteria for CIPN.70,82,83 For all grades of CIPN, 1 study of mFOLFOX6 in rectal adenocarcinoma with metastasis after radical surgery found no significant difference between groups (RR 1.00 [0.50, 1.99], n = 68). 70 One study of HIPEC for stage II/III CRC after surgery 82 also found no significant difference (RR 0.59 [0.34, 1.02], n = 104). In the pooled result for these 2 studies, there was no significant difference between groups in incidence of all grades CIPN (RR 0.74 [0.44, 1.23], I2 = 28%, n = 172). In the single study that only reported on perioral paresthesia associated with mFOLFOX6 after radical surgery for CRC, there was a significant reduction in the herbal medicine plus mFOLFOX6 group (RR 0.17 [0.04, 0.68], n = 60). 83
Hand-Foot Syndrome
Of the 12 studies that reported data for chemotherapy-related HFS, 6 used the WHO criteria, 5 used the NCI-CTCAE criteria, and 1 did not specify the criteria.
For grade III (WHO), data were available for 4 studies. Two of these reported zero events in both groups30,43 (Table 7). There were no significant differences between groups in the other two studies and the pooled result found no significant difference (RR 0.42 [0.06, 2.76], I2 = 0%). For all grades, there were no significant differences between groups for the studies of FOLFOX4, mFOLFOX6, XELOX, or SOX but there was a significant difference for HIPEC. The pooled result found no significant difference between groups (RR 0.59 [0.18, 1.92], I2 = 96%) but the heterogeneity was considerable. This was mainly due to 1 study of mFOLFOX6 (No. 50) that reported presence of HFS in all participants. 74 When this study was excluded from the meta-analysis pool, the heterogeneity was reduced and there was a significant reduction in HFS (all grades) in the integrative therapy groups (RR 0.62 [0.41, 0.96], I2 = 22%). The pooled result for the 2 studies that used syndrome differentiation found no significant difference between groups without heterogeneity.
Integrative Herbal Medicine: Chemotherapy-Related Hand-Foot Syndrome (WHO). a

Abbreviations: WHO, World Health Organization; CI, confidence interval; RR, relative risk; RCT, randomized controlled trial; HIPEC, hyperthermic intraperitoneal chemotherapy.
All studies used oral herbal medicines combined with chemotherapy versus the same chemotherapy.
Statistically significant.
These chemotherapy regimens all used oxaliplatin, 5-fluorouracil (5-FU) plus leucovorin (LV).
Since all participants had hand-foot syndrome at baseline.
Five studies used the NCI-CTCAE criteria. One reported zero grade III cases in both groups 46 (Table 8). There were no significant differences between groups in the other 2 studies and the pooled result also found no significant difference (RR 0.25 [0.03, 2.22] I2 = 0%). For all grades, there was no significant difference between groups in the subgroup results for XELOX or FOLFOX4/FOLFOX6. The pooled result showed no differences between groups in incidence of all grades of HFS (RR 0.93 [0.55, 1.55], I2 = 75.7%) with substantial heterogeneity. No single study or factor was the main contributor so a sensitivity analysis was not feasible.
Integrative Herbal Medicine: Chemotherapy-Related Hand-Foot Syndrome (NCI-CTCAE). a

Abbreviations: NCI-CTCAE, National Cancer Institute Common Terminology Criteria for Adverse Events; CI, confidence interval; RR, relative risk; CRC, colorectal cancer.
All studies used oral herbal medicines combined with chemotherapy versus the same chemotherapy.
Statistically significant.
In the single study that did not specify the criteria (No. 21), XELODA was used as a maintenance treatment in stage IV CRC. 45 There was no difference between groups in all grades HFS (RR 0.67 [0.12, 3.80], n = 90).
Topical Herbal Medicine Plus Chemotherapy Versus Chemotherapy
Five RCTs employed hand and foot baths for prevention of the symptoms of CIPN due to oxaliplatin-based chemotherapy (Table 1, Supplementary Tables S1 and S4). All used Levi’s criteria. 88
For grade III/IV CIPN, there was no significant difference between groups (RR 0.35 [0.10, 1.20] I2 = 0%), but the overall incidence was low (3 vs 13 cases). For all grades, there was a significant reduction in the number of people developing CIPN in the integrative therapy groups compared with the control groups (RR 0.69 [0.50, 0.95], I2 = 68.8%) with substantial heterogeneity (Table 9).
Herbal Hand and Foot Bath Plus Chemotherapy: Chemotherapy-Induced Peripheral Neurotoxicity (CIPN). a

Abbreviations: CI, confidence interval; RR, relative risk; RCT, randomized controlled trial.
All studies used herbal hand and foot baths combined with chemotherapy versus the same chemotherapy.
Statistically significant.
Sensitivity 1 excluded Study No. 49 group T1 to remove double counting due to this study having 2 comparisons.
Sensitivity 2 excluded Study No. 49 altogether (groups T1 and T2).
One study (No. 49) included 2 comparisons 73 and one of these used a complex control (calcium and magnesium plus mFOLFOX6), so this arm was excluded in a sensitivity analysis. This showed a marginally significant result for grades III + IV but the heterogeneity remained for all grades. In a further sensitivity analysis that excluded this study, the result was similar to that for the total pool but without heterogeneity.
Safety of the CHMs
In 49 studies, there was no mention of the safety of the herbal medicines. Ten studies stated that there were no adverse events associated with the herbal medicines. One study (No. 11) that used hand and foot bath mentioned that 1 patient in the test group had mild allergy, which was likely due to the herbal hand and foot bath. 35
In another study (No. 53), the adverse events and/or reasons for dropouts were stated for the two groups: in the CHM plus chemotherapy group, 2 refused chemotherapy, 2 had chemotherapy-related adverse reactions, and there were 2 deaths; in the chemotherapy group, 3 refused chemotherapy, 8 had chemotherapy-related adverse reactions and there were 3 deaths. 77 In this study, it was unclear whether any of the adverse events were due to the herbal medicines. In the study by Kono et al, 47 there were 3 dropouts in the CHM group and 1 dropout in the control group, but these were prior to commencement of treatment. In Nishioka et al, 63 more people discontinued chemotherapy in the CHM group (n = 13) than in the control group (n = 11); the same numbers showed progressive disease (9 vs 9); more experienced an allergic reaction to oxaliplatin (4 vs 1); and fewer had persistent grade III oxaliplatin-induced neuropathy (0 vs 1); but it was unclear whether these differences were influenced by the herbal medicine. In Oki et al, 64 the most common comorbidities were hypertension and diabetes with no between-group difference in their incidence, but the incidence of grade II or greater CIPN was higher in the integrative group at the 8-month analysis (mean 8-9 cycles) so the study was discontinued. The analysis of oxaliplatin dose showed it was higher in the integrative group, but it was unclear whether this accounted for the increased CIPN rate. Overall, no serious adverse events associated with the herbal medicines were identified but data were incomplete.
Discussion
The majority of the data were for studies that combined an orally administered herbal medicine with a chemotherapy regimen compared to the same chemotherapy regimen with CIPN as an outcome. A further 5 studies had poolable data for hand and foot baths for CIPN and 5 studies assessed orally administered herbal medicine for HFS.
Effects on CIPN
The main outcome measures were the WHO criteria, Levi’s modified WHO criteria, or the NCI-CTCAE criteria. Although these criteria are similar there are some differences, so the results were pooled separately. For each outcome measure, the more severe grades of CIPN (grades III + IV) were reported first. Such severe events are clinically relevant since they are likely to lead to chemotherapy cessation. In general, the incidences of Grade III + IV CIPN were low in both groups and a number of studies had zero events. Studies that had zero events in both groups did not contribute to the pooled results, so the incidences and identity of such studies are recorded in the results tables.
For incidence of grades III + IV CIPN, there was a significant reduction in the integrative therapy groups based on 14 studies that used the WHO criteria (955 participants) without heterogeneity (Table 3). However, the overall incidence at end of treatment was low, with 1.6% in the integrative groups and 4.1% in the chemotherapy alone groups (Supplementary Table S5). It is notable that the reduction was mainly in the subgroup of FOLFOX regimens. This result was similar to a previous meta-analysis of CHM plus FOLFOX4 in advanced CRC, which found slightly higher incidences (2.2% vs 6.0%). 89 In the 6 studies (485 participants) that used Levi’s criteria the meta-analysis results and the incidences (1.4% vs 9.2%) were similar (Table 5 and Supplementary Table S5). In the 7 studies (561 participants) that used the NCI-CTCAE criteria there was no significant difference between groups with some heterogeneity, and considerably higher incidence rates (8.5% vs 13.0%) (Table 6 and Supplementary Table S5).
Overall, the incidences of grade III plus IV CIPN in the WHO and Levi groups were much lower than in the trials by de Gramont et al 7 and Cassidy et al. 8 A likely reason is that most studies were of too short a duration for severe CIPN to develop. Larger proportions were evident in the FOLFOX regimens for NCI-CTCAE criteria which included 4 placebo-controlled studies (4-26 weeks’ duration).47,58,59,64 In this group, the grade III plus IV incidence was 18.9% in the chemotherapy controls (all FOLFOX), which is similar to the 17% reported by Cassidy et al, 8 versus 12.9% in the integrative therapy groups.
For all grades, the majority of studies provided nonzero data. For the 32 studies that used the WHO criteria (1853 participants) there was a significant reduction in CIPN in the integrative groups, but the heterogeneity was considerable (Table 4). Since this was due to a single study in which all participants already had CIPN at baseline, it was reasonable to exclude this study from the pooled result to obtain a more accurate estimate. This sensitivity analysis had the effect of eliminating the heterogeneity, while finding a similar result. The resultant incidence rates were 32.7% in the integrative groups and 42.8% in the chemotherapy controls. In the 7 studies that used Levi’s criteria, there was also a significant reduction in all grades CIPN in the integrative groups, but with considerable heterogeneity (Table 5). This was due to 2 studies with very high CIPN incidences in both groups (73%-82%) that found no differences between groups. When excluded, the CIPN incidence rates for the remaining five studies were 32.4% for integrative therapy versus 73.0% for the chemotherapy controls (Supplementary Table S5). For the NCI-CTCAE criteria, the pool of 9 studies (727 participants) showed a significant reduction in the integrative groups (Table 6), with incidence rates of 25.8% versus 33.3% (Supplementary Table S5). Notably, the positive results were associated with the FOLFOX regimens. In comparison, in the review by Seretny et al, 5 the mean rates of all grades CIPN were 60% at 3 months and 30% at 6 months or longer.
It was expected that the results of the subgroup of studies that used syndrome differentiation would show less heterogeneity than the overall pools since the participant groups should be less variable due to this additional selection criterion. This was evident for all grades CIPN in a number of pools. Notably, for the WHO criteria, the 17 studies that used syndrome differentiation found a benefit for adding the herbal medicine without heterogeneity, as did the group of 13 studies of Pi xu 脾虚 syndromes (Table 4).
In the studies of hand and foot baths, the pooled result for grades III + IV did not show a significant difference between groups but there were few cases in total (Table 9). For all grades, the incidences in the four studies included in the final sensitivity analysis were 60% in the chemotherapy-alone groups and 30% in the integrative groups indicating the herbal hand and foot baths produced a significant reduction in CIPN.
Effects on Hand-Foot Syndrome
For grade III HFS (WHO criteria) the incidence was very low, at 0.9% in the integrative groups and 2.8% in the chemotherapy control groups. In the studies that used the NCI-CTCAE criteria, there was only 1 case in total (Supplementary Table S5). So, there were insufficient data for a meaningful assessment.
For WHO all grades (Table 7), the pooled result for 6 studies found no significant difference between groups with considerable heterogeneity, which was due to the previously-mentioned study that only enrolled participants with HFS (grade I-II), none of whom resolved in either group. When excluded, there was a significant difference, with 23.3% incidence in the integrative groups versus 41.8% in the chemotherapy alone groups (Supplementary Table S5). In the 5 studies that used the NCI-CTCAE criteria, there was no difference between groups with substantial heterogeneity and rates of 40% in both groups (Table 8 and Supplementary Table S5).
When compared with the results reported in Cassidy et al, 8 the low rate of grade III was consistent with most studies using a FOLFOX regimen, which generally do not produce high rates. However, the single study of XELOX reported zero grade III cases in both groups. For all grades, the rates were relatively high in the WHO criteria group, due mainly to the XELOX, SOX, and HIPEC subgroups. Four of the studies in the NCI-CTCAE criteria group used XELOX and this sub-group produced the highest incidence rates (44% vs 48%), as could be expected. Adding a herbal medicine did not have a significant effect in this subgroup. Overall, the herbal medicines appeared to reduce the incidence of HFS, but the results for XELOX were heterogeneous.
Limitations of This Review
This meta-analysis was based on published data mostly from unblinded studies, so the results are likely to be biased in favor of the integrative therapy groups. Asymmetry in the funnel plot (Supplementary Figure S2) suggested bias due to missing data, due either to small studies with nonsignificant results not being published or published studies omitting mention of CIPN. Therefore, caution is required when interpreting the meta-analysis results.
In the 5 placebo-controlled studies, the poolable results were mixed with one study showing higher rates in the integrative group 64 whereas the others showed improvements. Such data are difficult to interpret, each study showed distinct characteristics and no clear subgroups were evident.
In the larger meta-analysis pools, it was possible to identify some differences due to the chemotherapy regimen used, but there was no plausible method of taking duration of treatment or accumulated dose of chemotherapy into account due to inconsistencies in how such data were reported. These factors are likely to have influenced the incidences of CIPN and HFS and contributed to heterogeneity.
Another issue is variability in the herbal interventions. Although there were similar ingredients in many of the oral formulae, it was not clear which had been included to counter CIPN or HFS and which had been included for other reasons, since these outcomes were not primary in most studies. Goshajinkigan was the only oral formula that has been studied for reducing CIPN in multiple retrospective90-92 and prospective47,63,64 studies of CRC. Also, it has been reported to reduce the incidence of CIPN in ovarian cancer. 93 Recent meta-analyses of Goshajinkigan have shown mixed results when multiple cancer types and comparators were pooled but there was considerable heterogeneity.20,22 Although the retrospective studies of this formula showed benefits in CRC, the results of the 3 prospective studies included in this review were mixed, with 2 studies reporting benefits47,63 and 1 finding possible detriment. 64 For Goshajinkigan and the 3 other formulae that were used in 2 studies each, differences between studies in the comparators or outcome measures precluded data pooling for these specific CHMs. Consequently, it was not possible to select a best CHM intervention for CIPN or HFS.
Data on the safety of the herbal medicines were poorly reported in most studies. This was in part due to the overriding effects of the toxicity due to the chemotherapies. It was not possible to assess whether any of the herbal medicines reduced the effectiveness of the chemotherapies since parallel data sets were not available. However, previous meta-analyses that have addressed this issue found no evidence that the addition of herbal medicines to chemotherapy reduced tumor response rates.94,95
Implications for Clinical Practice and Further Research
Based on the pooled results, the evidence for reduction in grades III + IV CIPN is weak due to the small number of cases in the analyses. Larger studies of oxaliplatin regimens that are long enough in duration for severe CIPN to accumulate are needed to explore this question.
For all grades of CIPN, it appeared that addition of orally administered herbal medicines was likely to reduce less severe CIPN. However, since most studies were relatively short, it is unclear whether this effect would translate into overall reduction in incidence or severity of CIPN with longer term oxaliplatin use. It is possible that the herbal medicines delayed the onset of the CIPN but not its ultimate progression. Further study is needed to monitor the progression of CIPN in relation to accumulated oxaliplatin dose. There were very little data for non-oxaliplatin regimens, so it is not possible determine if any herbal medicines were beneficial.
The herbal hand and foot baths appear to have provided some reductions in CIPN. From a clinical perspective, the use of topical herbal medicines should reduce the potential for interactions with a patient’s medications, but it is important to note the potential for allergic reactions and to test each patient’s sensitivity to the formula before undertaking a course of treatment.
For HFS, the results of the studies showed no convincing evidence of a benefit, but there was heterogeneity in the result and the sample size was relatively small. Further studies of oral and topical preparations are needed to determine the role of herbal medicines in this condition.
Conclusions
Data on the effects of herbal medicines for CIPN and/or HFS were available for 63 RCTs. For orally administered herbal formulae combined with chemotherapies, the evidence indicated a reduction in all grades CIPN (WHO toxicity criteria) in the integrative therapy groups based on 31 RCTs with 1778 participants. Similar results were evident for other criteria but based on smaller pools. For grades III + IV severe CIPN, there were also reductions, but the evidence was weaker. The use of the herbal hand and foot baths appeared to reduce all grades of CIPN, but the results were based on a small sample. The oral herbal formulae did not appear to improve HFS. The strength of these conclusions is limited by lack of blinding in the majority of studies and the possibility of reporting bias. Future clinical studies are needed that focus on specific herbal medicines for CIPN and HFS. Experimental studies are required to determine the mechanisms of action of any promising herbs.
Supplemental Material
IM_for_CIPN_Supplementary_materials_17_10_2018 – Supplemental material for Integrative Herbal Medicine for Chemotherapy-Induced Peripheral Neuropathy and Hand-Foot Syndrome in Colorectal Cancer: A Systematic Review and Meta-Analysis
Supplemental material, IM_for_CIPN_Supplementary_materials_17_10_2018 for Integrative Herbal Medicine for Chemotherapy-Induced Peripheral Neuropathy and Hand-Foot Syndrome in Colorectal Cancer: A Systematic Review and Meta-Analysis by Yihong Liu, MMed, Brian H. May, PhD, Anthony Lin Zhang, PhD, Xinfeng Guo, PhD, Chuanjian Lu, PhD, Charlie Changli Xue, PhD and Haibo Zhang, MD in Integrative Cancer Therapies
Footnotes
Acknowledgements
We wish to thank Dr Meaghan Coyle for her help with searches.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors acknowledge the funding support provided by the China-Australia International Research Centre for Chinese Medicine (CAIRCCM)—a joint initiative of RMIT University, Australia and Guangdong Provincial Academy of Chinese Medical Sciences, China, and the Foundation for Chinese Medicine and Technology Research of Guangdong Provincial Hospital of Chinese Medicine (2017KT1820, 2016KT1571).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.