
Abstract
Background. Peripheral neurotoxicity caused by oxaliplatin (OXA) chemotherapy is the main limitation preventing continuation of chemotherapy in patients with gastrointestinal cancer. The purpose of this study was to determine the efficacy of external use of Chinese herbal medicine (CHM) on the incidence of cumulative OXA-induced peripheral neurotoxicity (OIPN). Method. Scientific literature databases were searched to identify controlled clinical trials analyzing CHM in OIPN. Clinical studies that included at least 1 relevant primary outcome were analyzed by 2 independent reviewers. Meta-analysis was performed on the software RevMan 5.3. Results. 700 cancer patients of 9 studies were reported, of whom 352 received external CHM and 348 received warm water baths, conventional medicine, or no intervention as controls. Neurotoxicity incidence (Levi grade ≥ 1) was significantly decreased in CHM group, compared with no intervention (P < .01). The incidence of cumulative neurotoxicity (Levi grade ≥2) was also significantly lower in the CHM group than in all the control groups (P < .05), and the cumulative neurotoxicity in the CHM group was significantly reduced (Levi grade ≥ 3) in comparision with no intervention (P < .01). These results were consistent with those of the subgroup analyses for preventing OIPN at each of the chemotherapy treatment cycles. There was no difference in the incidence of adverse events between groups (P > .05). Conclusion. External use of CHM may be beneficial in preventing the OXA-induced cumulative neurotoxicity. However, given the low quality of the evidence, the results should be interpreted with caution.
Keywords
Introduction
Oxaliplatin (OXA) is a chemotherapeutic agent frequently prescribed to treat gastrointestinal cancer. 1 However, neurotoxicity induced by OXA is a common side effect 2 . In general, OXA-induced peripheral neurotoxicity (OIPN) occurs when OXA infusion is continued for 4 or more cycles.3,4 High cumulative doses of OXA have a concomitant increase in chronic peripheral nerve damage. The incidence of chronic peripheral neuropathy can be up to 85%.4,5 Clinical symptoms are characterized by distal sensory loss, suppression of deep tendon reflexes, and changes in proprioception.6,7 These side effects not only affect a patient’s quality of life,8-10 but also limit patient compliance with cancer treatment. This can result in OXA dose reduction and discontinuation.5,11 Strategies for preventing cumulative OIPN currently include intravenous calcium and magnesium, glutathione, venlafaxine, and calmangafodipir.12-14 However, pharmacological management is limited, and there is a lack of consensus on optimal prevention strategies.12-14
There is a growing interest in the use of complementary medicine to help individuals manage their cancer treatment journey and survivorship. 15 Chinese medicine plays an important role in cancer care in China. 16 Based on its own distinctive principles and comprehensive theory, it is also one of the oldest medical systems in the world. Chinese herbal hand and foot baths administered periodically over several weeks have been used in China for the management of OIPN. Topical Chinese herbal medicine (CHM) therapy exerts its effect through the skin with relatively minimal systemic uptake or distribution. Recent reviews have reported on the use of herbal medicines (including CHMs) for chemotherapy-induced peripheral neuropathy.17-20 However, interpretation of the evidence from these reviews was limited by the inclusion of quasi–randomized controlled trials (RCTs), variation in the form and dosing characteristics of the intervention, and poor reporting. The primary aim of our systematic review is to provide an update of the evidence describing the effectiveness and safety of external use of CHM for preventing chronic OXA-induced peripheral neuropathy.
Methods
Our systematic review adopts the preferred reporting protocol for systematic reviews and meta-analyses as outlined by the PRISMA statement (Appendix). 21 The review protocol was registered in PROSPERO (https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=94301).
Search Strategy
A comprehensive search was conducted to identify all relevant studies regardless of language or publication status. Databases searched included MEDLINE, EMBASE, CINAHL, The Cochrane Library (Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials), and Chinese databases China National Knowledge Infrastructure (CNKI), Wangfang, and VIP. All databases were searched from inception to November 2018. MEDLINE and CNKI search strategies are shown in Appendix.
Eligibility Criteria
RCTs were included without restriction of language. For articles not published in English or Chinese, translators were used. Crossover studies were generally excluded because of potential carryover effects.
Studies were included if patients were >18 years old, with any type of cancer and receiving OXA regimens over at least 4 cycles. Patients were excluded if they had a history of peripheral neuropathy resulting from any cause or any coexisting condition that could impair peripheral nerve function. Permitted control groups included placebo-designed herbal baths, warm water baths, conventional medicine (eg, intravenous calcium and magnesium, mecobalamin), or no intervention. Studies that added or compared external CHM with additional unknown potentially active treatments (eg, wash, gel, or cream) were excluded. Clinical studies that included at least 1 relevant primary outcome were eligible for analysis.
The primary outcome was the incidence of neurotoxicity measured by standardized and validated clinical assessment tools. These tools included, but were not limited to, patient-reported outcomes, clinician-rated neuropathy assessments, and functional measures (eg, nerve conduction velocity [NCV]). In this review, the clinician-rated neuropathy assessments used the World Health Organization (WHO) Common Toxicity Criteria for Peripheral Neuropathy, National Cancer Institute Common Toxicity Criteria (NCI-CTC), the Levi grade, and Toronto Clinical Neuropathy Score. Secondary outcomes included safety outcomes (eg, adverse event reporting), performance/functionality measures, OXA dosage associated with time to neuropathy and its severity, and discontinuation or change in OXA dosage caused by OIPN. We also considered subgroup analysis for these outcomes at different time points (number of cycles) of chemotherapy, if data were available.
Data Extraction
The relevant data were extracted by 2 authors (JH and XZ) working independently, including patient demographics and cancer types, chemotherapy types, and the effect of the intervention and the control on OXA-related neurotoxicity (Table 1).
Summary of the Included Randomized Controlled Trials of External Chinese Herbal Medicine for Preventing OIPN.

Abbreviations: OIPN, OXA-induced peripheral neurotoxicity; XELOX, oxaliplatin + capecitabine; NCI-CTC, National Cancer Institute Common Terminology Criteria for Adverse Events Sensory Neuropathy Scale; MNCV, motor nerve conduction velocity; SNCV, sensory nerve conduction velocity; FOLFOX, oxaliplatin + 5-fluorouracil + calcium folinate; ADL, Activities of Daily Living; OXA, oxaliplatin; TTN, time to neuropathy; CTx, chemotherapy treatment; QoL, quality of life; KPS, Karnofsky Performance Score; WHO, World Health Organization; L-OHP+S1, Oxaliplatin + Tegafur Gimeracil Oteracil Potassium Capsule; TCSS, Toronto Clinical Scoring System.
Statistical Methods
RevMan 5.3 software was used for the meta-analysis. 22 Dichotomous variables were analyzed with odds ratios (ORs) and continuous outcomes with mean differences (MDs) at a 95% CI. Two-sided P values were computed for the differences between dichotomous variables and continuous variables, which were considered significant at P <.05. The random-effects model (the DerSimonian and Laird method) or fixed-effects model (the Mantel-Haenszel method) was used for variables of heterogeneity, when explored using the χ2 test with significance set at P ≤.100 or P >.100, respectively. 23 Further analyses of available outcomes were performed at each of the chemotherapy treatment cycles to verify the accuracy of the results. The risk of included studies bias was assessed in accordance with the guidelines of the Cochrane Collaboration. 23
Results
Literature Search and Characteristics of Included Studies
A total of 961 potentially relevant references were identified. After reading the titles and abstracts, 62 duplicate articles were excluded and 850 studies that did not meet the eligibility criteria were removed. A total of 49 references were retrieved for further assessment. After full-text reviews, 9 trials were included in the analysis (Figure 1).24-32 All the included trials were conducted in China and published from 2010 to 2017. All trials used random number tables for randomization. However, inadequate allocation concealment as well as lack of blinding of participants and personnel was identified as high risk of bias for all trials (Figure 2). Five trials reported dropouts.27-31 One implemented an intention-to-treat analysis, 27 and one with a more than 20% drop-out rate in the control group was assessed to be at a high risk for bias. 28 For 3 trials, it was assessed that the proportion of missing outcomes was not sufficient to have a clinically relevant impact on the intervention effect estimate. Overall, most studies reported prespecified outcomes, but only 1 study that did not report expected outcomes was deemed to be at high risk of bias. 28
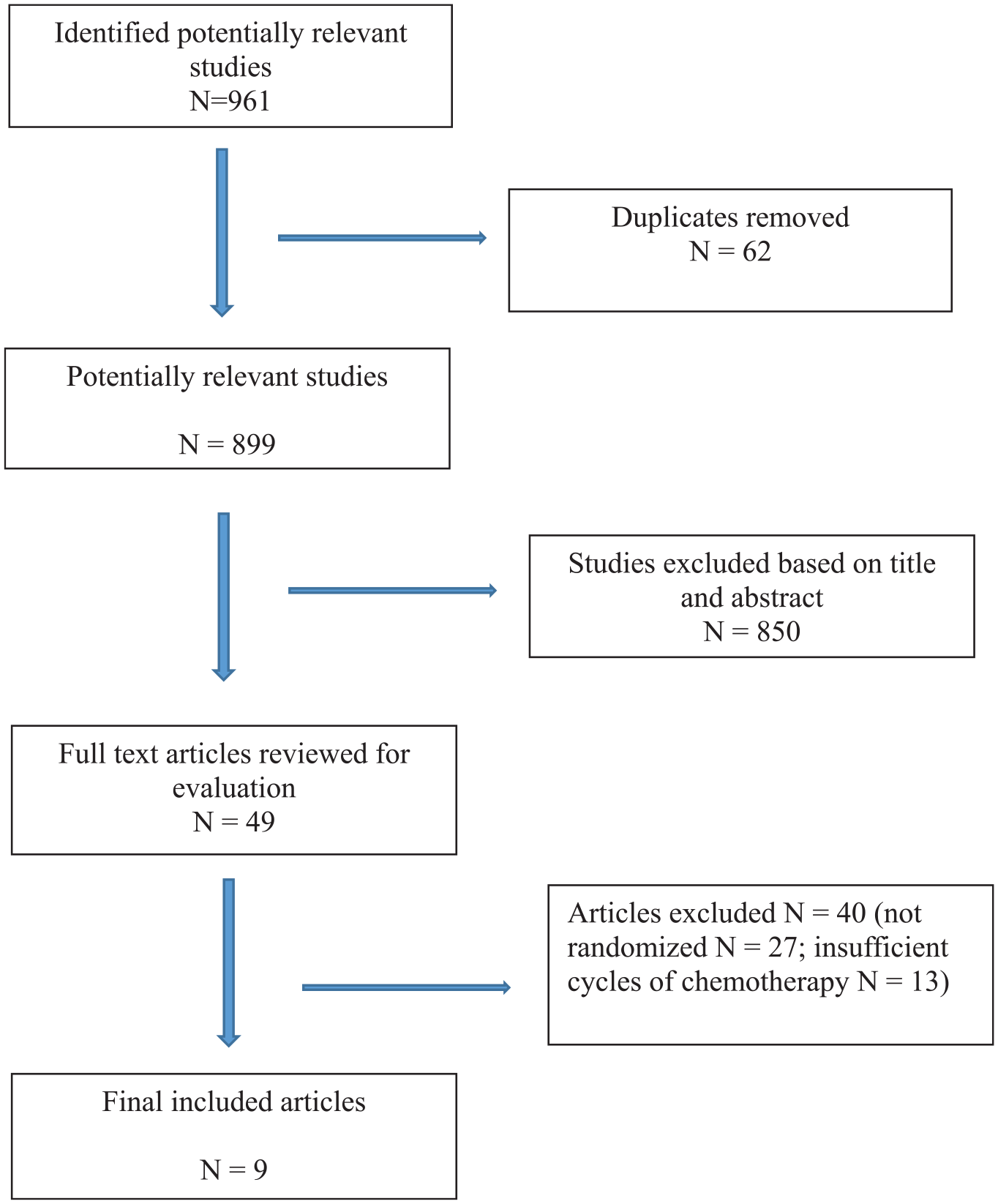
Flowchart of the selection of publications included in the meta-analysis.

Summary of risk of bias (“+,” low risk of bias; “?,” unclear risk of bias; “-,” high risk of bias).
Participants
In total, 700 participants with chemotherapy were included in these 9 trials, of whom 352 received Chinese herbal hand and foot baths (CHM group) and 348 were in one of the control groups. The average size of the trials was 82 participants, ranging from 44 to 128 per trial. Four trials enrolled both inpatients and clinic outpatients (n = 317 patients, 45.3%).29-32 One study recruited solely from inpatients. 28 The remaining 4 trials did not specify the clinical setting (n = 314 patients, 44.9%).24-27 All trials included both adult male and female patients, with 55% of participants (n = 386) being male. All participants were diagnosed with gastrointestinal cancer. Types of cancer included colorectal cancer (n = 499 patients, 71.3%), gastric cancer (n = 190 patients, 27.1%), and esophageal cancers (n = 11, patients, 1.6%). Cumulative OXA dose varied from 340 to 1040 mg/m2, with a mean value at 671 mg/m2.
Interventions and Controls
More than 67% (6/9) of the studies compared Chinese herbal hand and foot baths with no intervention. Of the 6 trials, one reported 3 study arms: (1) no additional intervention, (2) Ca/Mg infusion therapy, and (3) herbal bath plus Ca/Mg infusion therapy. Two additional studies compared CHM with mecobalamin, and CHM plus mecobalamin with mecobalamin alone. One study used warm water baths as the control arm. No study included specifically designed placebo herbal baths.
The active herbal formulations were varied. Nine formulae with a total of 34 herbal ingredients were investigated; 18 herbs were identified as the most frequently tested (Tables 2 and 3). Six studies reported full compositions of the herbal formulae. In contrast, 3 studies did not report all ingredients used.28,29,31 Seven studies mentioned the full dosages of herbal ingredients, whereas dosage information was missing from the remaining 2 studies.29,31 None of the studies reported any laboratory testing of the herbal ingredients for quality control or standardization. Only 1 trial cited relevant pharmacological bases for the intervention. 25 All trials administered raw herbs externally in the form of decoctions. The lengths of trial periods varied from 4 to 12 chemocycles (8-24 weeks). Six cycles were used in 4 studies, 4 cycles in 3 studies, and 8 cycles in 3 studies, and 1 study used a 12-cycle intervention. The included studies were characterized by variation in formulation, dosage administration, and duration of treatments.
Frequency of Use of the Herbs in External Chinese Herbal Formulas for OIPN.

Abbreviation: OIPN, oxaliplatin-induced peripheral neurotoxicity.
Composition of the External Chinese Herbal Formulas for OIPN.

Abbreviation: OIPN, oxaliplatin-induced peripheral neurotoxicity.
Outcome Measurements
All trials assessed the incidence of OXA-induced peripheral neuropathy as the primary outcome. The majority of trials (5/9) used Levi grading of chemotherapy-induced peripheral neuropathy.25,26,28,30,32 Two trials used the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE) criteria of chemotherapy-induced peripheral neuropathy,24,27 and 2 trials used WHO criteria of chemotherapy-induced peripheral neuropathy.29,31 Two trials reported on performance/functionality outcomes.28,29 Three trials also reported intervention-related adverse events,29-31 and 2 trials reported additional chemotherapy-induced adverse events.29,31 Three trials reported on sensory NCV (SNCV),24,26,27 and 2 of them also reported on motor NCV (MNCV).24,26
Effects of Interventions
Primary Outcome
Incidence of Levi grade ≥1 total cumulative neurotoxicity
All 9 trials reported incidence of total cumulative neurotoxicity (Levi grade scores from 1 to 4). Six trials (n = 451 patients) compared CHM with no intervention.25,26,28,30-32 For these 6 studies, a difference was found between the 2 groups in favor of CHM in reducing OIPN occurrence (OR = 0.22; 95% CI = 0.11 to 0.45; P < .01). There was moderate heterogeneity between studies (I² = 52%; Figure 3). In the subgroup analyses, in 4 trials (n = 287 patients), this outcome was in favor of CHM after 4 cycles of chemotherapy (OR = 0.21, 95% CI = 0.13 to 0.37, P < .01; I² = 24%).26,28,30,32 In 3 trials (n = 226 patients), CHM was superior to no intervention after 6 cycles of chemotherapy (OR = 0.15, 95% CI = 0.08 to 0.30, P < .01; I² = 0%).28,30,32 In 2 other studies (n = 165 patients), CHM had significant positive results after 8 treatment cycles (OR = 0.49, 95% CI = 0.24 to 1.01, P = .05; I² = 0%; Figure 4).25,31 CHM also showed a reduction in OIPN incidence compared with warm water bath (n = 55 patients; OR = 0.20, 95% CI = 0.06 to 0.69, P = .01) 28 or mecobalamin (n = 90 patients; OR = 0.18, 95% CI = 0.07 to 0.45, P < .01). 24 One trial (n = 44 patients) 27 compared CHM plus mecobalamin to mecobalamin, demonstrating a difference in favor of CHM plus mecobalamin after 8 and 12 treatment cycles (OR = 0.02, 95% CI = 0.00 to 0.11, P < .01, and OR = 0.23, 95% CI = 0.05 to 1.01, P = .05, respectively). One trial (n = 60 patients) reported no statistically significant difference in either CHM versus Ca/Mg infusion (OR = 1.00; 95% CI = 0.28 to 3.54; P > .05) or CHM plus Ca/Mg infusion versus Ca/Mg infusion alone (OR = 0.50; 95% CI = 0.15 to 1.62; P > .05). 25

Comparison of CHM and no intervention by total cumulative neurotoxicity at the end of the study.

Comparison of CHM and no intervention by total cumulative neurotoxicity after 4/6/8 cycles of chemotherapy.
Incidence of Levi grade ≥2 cumulative neurotoxicity
Nine trials reported that CHM had an advantage in reducing the Levi grade ≥2 of cumulative neurotoxicity. Five trials (n = 346 patients) reported that the incidence of grade ≥2 cumulative neurotoxicity in the CHM group was lower than that in the nonintervention control group (OR = 0.19, 95% CI = 0.11 to 0.32, P < .01; Figure 5).25,26,28,30,32 This result was consistently reported at different stages of treatment: in 4 trials (n = 287 patients) after 4 cycles (OR = 0.20, 95% CI = 0.11 to 0.39, P < .01; I² = 0%); in 3 trials (n = 226 patients) after 6 cycles (OR = 0.15, 95% CI = 0.07 to 0.30, P < .01; I² = 0%); and in 1 trial (n = 60 patients) after 8 cycles (OR = 0.33, 95% CI = 0.12 to 0.96, P < .05; Figure 6). Compared with Ca/Mg infusion, 1 study (n = 60 patients) 25 reported that the grade ≥2 cumulative neurotoxicity was significantly decreased in the CHM (OR = 0.33, 95% CI = 0.12 to 0.96, P < .05) and the CHM plus Ca/Mg infusion groups (OR = 0.05; 95% CI = 0.01 to 0.24; P < .01). Compared with mecobalamin, 1 trial (n = 90 patients) 24 reported this outcome in favor of CHM (OR = 0.19; 95% CI = 0.06 to 0.57; P < .01) and another trial (n = 44 patients) 27 was in favor of CHM plus mecobalamin (OR = 0.22; 95% CI = 0.06 to 0.87; P < .05). Compared with a warm water bath control, 1 study (n = 55 patients) 29 reported a reduced incidence of grade ≥2 cumulative neurotoxicity in the CHM (OR = 0.19; 95% CI = 0.05 to 0.80; P < .05).

Comparison of CHM and no intervention groups by Levi grade ≥2 cumulative neurotoxicity at the end of the study.
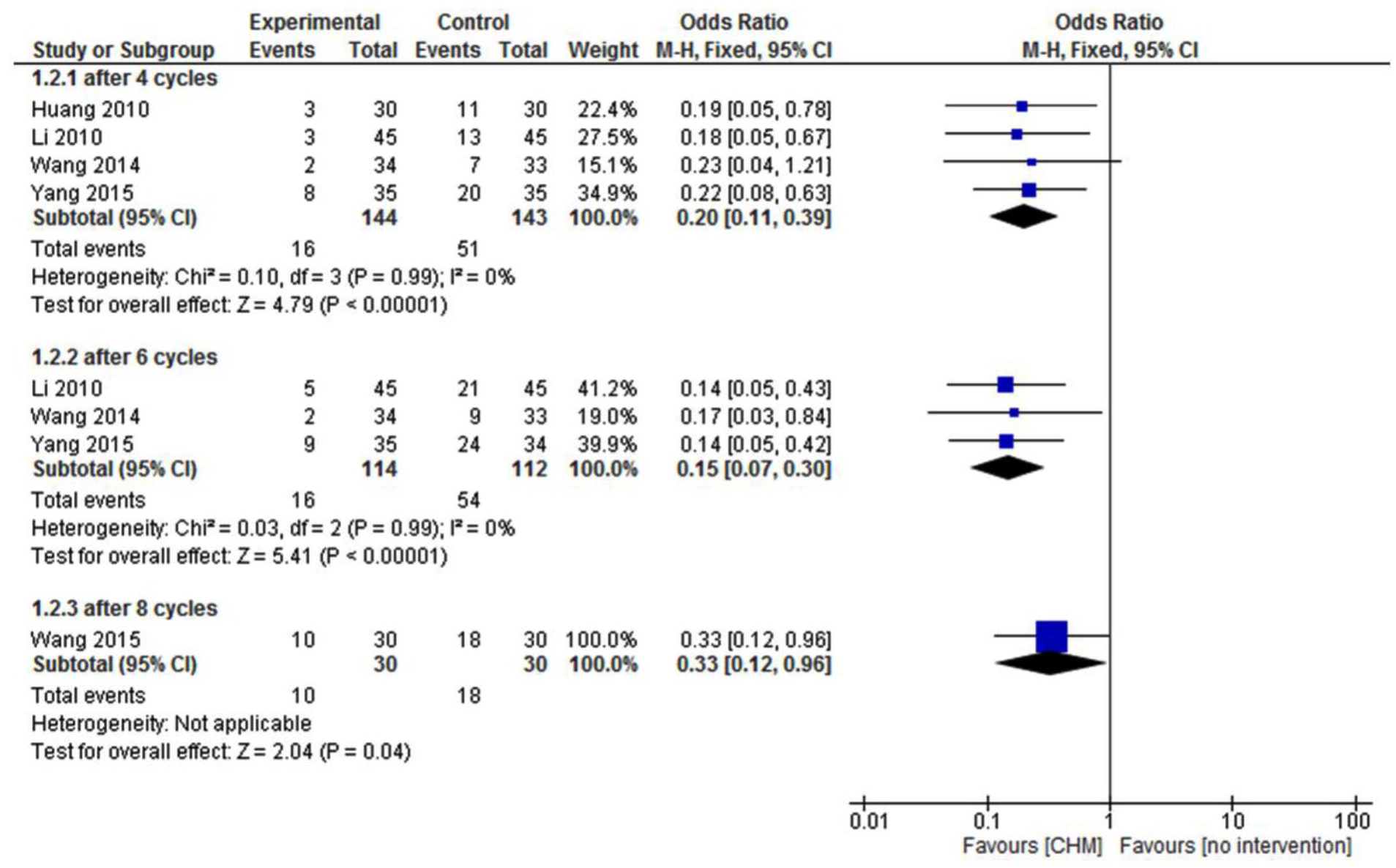
Comparison of CHM and no intervention groups by Levi grade ≥2 cumulative neurotoxicity after 4/6/8 cycles of chemotherapy.
Incidence of Levi grade ≥3 cumulative neurotoxicity
Five trials (n = 346 patients) examined the effect between CHM and no intervention on the Levi grade ≥3, with a significant difference in favor of CHM (OR = 0.19, 95% CI = 0.07 to 0.52, P < .01; I² = 0%; Figure 7).25,26,28,30,32 In the relevant subgroup analyses, 4 trials (n = 287 patients), found in favor of CHM after 4 cycles (OR = 0.20, 95% CI = 0.06 to 0.70, P = .01; I² = 0%).26,28,30,32 In 3 trials (n = 226 patients), a reduction in the neurotoxicity grade was reported for CHM after 6 cycles (OR = 0.16, 95% CI = 0.05 to 0.57, P < .01; I² = 0%).28,30,32 No significant differences were observed after 8 cycles (n = 60 patients; OR = 0.19, 95% CI = 0.01 to 4.06, P > .05; I² = 0%; Figure 8). 25 However, 4 other trials found no statistical difference in grade ≥3 cumulative neurotoxicity incidence between groups. This included CHM versus mecobalamin (n = 90 patients; OR = 0.22, 95% CI = 0.04 to 1.08, P > .05), 24 CHM plus mecobalamin versus mecobalamin (n = 44 patients; OR = 0.18, 95% CI = 0.01 to 4.02, P > .05), 27 CHM versus warm water bath (n = 55 patients; OR = 0.19, 95% CI = 0.01 to 4.21, P > .05), 29 CHM versus Ca/Mg infusion (n = 60 patients; OR = 0.32, 95% CI = 0.01 to 8.24, P > .05), 25 and CHM plus Ca/Mg infusion versus Ca/Mg infusion (n = 60 patients; OR = 0.32, 95% CI = 0.01 to 8.24, P > .05). 25

Comparison of CHM and no intervention groups by Levi grade ≥3 cumulative neurotoxicity at end of the study.

Comparison of CHM and no intervention groups by Levi grade ≥3 cumulative neurotoxicity after 4/6/8 cycles OXA.
Nerve conduction velocity
There were significant differences in SNCV of both the median nerve and fibular nerve in favor of CHM treatment compared with no intervention 26 (n = 60 patients; MD 4.92 m/s, 95% CI = 2.92 to 6.92, P < .01; MD = 5.52 m/s, 95% CI = 4.08 to 6.96, P < .01) and CHM compared with mecobalamin 24 (n = 90 patients; MD = 6.22 m/s, 95% CI = 4.60 to 7.84, P < .01; MD = 5.09 m/s, 95% CI = 3.62 to 6.56, p < .01) studies. Compared with mecobalamin, 1 study (n = 44 patients) 27 reported improved SNCV in CHM plus mecobalamin after 8 (MD = 4.54 m/s, 95% CI = 0.89 to 8.19, P = .01) and 12 cycles of chemotherapy (n = 44 patients; MD = 6.77 m/s, 95% CI = 2.33 to 11.21, P < .01) but not after 4 cycles (n = 44 patients; MD = 1.77 m/s, 95% CI = −1.44 to 4.98, P > .05). CHM plus mecobalamin treatment also improved MNCV in the median and fibular nerves after both 8 and 12 cycles compared with mecobalamin alone 24 (n = 90 patients; MD = 6.88 m/s, 95% CI = 5.06 to 8.70, P < .01; MD = 8.20 m/s, 95% CI = 6.83 to 9.57, P < .01). There was no statistical difference of median motor nerve conduction between CHM and no intervention (n = 60 patients; MD = −1.22 m/s, 95% CI = −2.80 to 0.36, P > .05). 26
Toronto Clinical Neuropathy Score
One trial (n = 105 patients) using the Toronto Clinical Neuropathy Score showed that clinical neuropathy symptoms and signs were significantly improved in the CHM group compared with no intervention (MD = −2.70; 95% CI = −3.65 to −1.75; P < .01). 31
Secondary Outcomes
Safety outcomes
Three studies reported on safety outcomes.29-31 There was no significant difference in the incidence of intervention-related adverse events in the CHM compared with no intervention groups (n = 175 patients; OR = 6.11, 95% CI = 0.72 to 51.77, P > .05; Figure 9)30,31 or warm water bath (n = 55 patients; OR = 3.23, 95% CI = 0.13 to 82.71, P > .05). 29

Comparison of CHM and no intervention group by intervention-related adverse events at the end of the study.
Performance/Functionality measures
One trial (n = 79 patients) reported that CHM had a statistically significant effect on the Karnofsky Performance Score (KPS) compared with no intervention (MD = 2.79; 95% CI = 0.28 to 5.30; P < .05). 28 Another trial (n = 44 patients) reported statistically improved Activities of Daily Living (ADL) in favor of CHM plus mecobalamin compared with mecobalamin alone after 8 (OR = 14.00; 95% CI = 6.39 to 21.61; P < .01) and 12 cycles of chemotherapy (OR = 10.77; 95% CI = 1.88 to 19.66; P < .05). 27
Time to neuropathy
Three studies assessed time to neuropathy as an outcome.27,29,31 One study (n = 44 patients) reported that CHM plus mecobalamin significantly increased the time to NCI-CTC ≥1 neuropathy (OR = 144.59 mg; 95% CI = 84.17 to 205.01; P < .01) and the time to NCI-CTC ≥2 neuropathy (OR = 106.25 mg; 95% CI = 56.32 to 156.18; P < .01). 27 CHM versus warm water bath (n = 55 patients; MD = 75.20 mg, 95% CI = −56.70 to 207.10, P > .05) 29 or CHM versus no intervention (n = 105 patients; MD 83.20 mg, 95% CI = −17.58 to 183.98, P > .05) 31 demonstrated no significant differences in time to onset of WHO grade ≥2 neuropathy.
Discussion
This review aimed to explore the potential effectiveness and safety of externally applied CHM in chemotherapy-induced peripheral neuropathy. Nine studies were eligible for inclusion in our review.
The incidence of neuropathy following treatment cycles of OXA can vary. 33 From the primary outcome reported in 6 studies, it was found that external use of CHM could delay the incidence of cumulative OIPN (grade ≥ 1, 2, 3) compared with no intervention and other controls. Most studies reported these changes using the Levi Scale with end points that were variable across trials. Only 1 study utilized the Toronto Clinical Neuropathy Score.
Findings also suggest that CHM may improve QoL and increase SNCV, although data from these studies could not be pooled. There was controversy regarding the efficacy of enhancing SNCV from inconsistent data because of various chemotherapy cycles. From this review, CHM did not increase the MNCV.
The above outcome measures have been shown to detect occurrences in neuropathy over time with the administration of OXA. However, the sensitivity of either measure to detect small or moderate differences in the OIPN incidence and severity is uncertain. For example, the NCI-CTCAE was not recognized as an appropriate primary outcome measure from the latest released recommendations. 33 Thus, in the design of future studies, incorporating neurophysiological measurements, clinical examination with good reliability and interrater reliability (eg, Total Neuropathy Score clinical version (TNSc), and patient-reported outcome measurements should be considered.33,34
Safety
In general, Chinese herbal hand and foot baths were well tolerated based on the reported clinical adverse effects. There was no difference in the incidence of adverse events between CHM versus no intervention and CHM versus warm water bath. Adverse events were usually rare and reported to be mild. These adverse events included the development of a skin rash and irritation after the baths. There were no reports of systemic adverse events in these patients.
How the Intervention Might Work
Herbal ingredients prescribed for OIPN often contain active compounds promoting blood circulation. In vivo, Huangqiguizhiwuwu decoction has been shown to relieve pain as well as ameliorate sciatic NCV in rats with chemotherapy-induced peripheral neuropathy. 35 AC591, a standardized extract from this herbal decoction, reduced OXA-induced cold hyperalgesia, mechanical allodynia, and morphological damage of the dorsal root ganglion. 36 Similarly, in other in vitro and in vivo studies, Radix Astragali extract, Radix Paeoniae alba extract, puerarin from Pueraria lobate, and Tanshinone IIA from Salvia miltiorrhiza were all observed to be potential nerve growth–promoting factors in peripheral nerve regeneration.37-42 In particular, Astragali Radix reduced OXA-induced cold hypersensitivity, completely blocked the onset of the proallodynia effect, and protected against neurodamage-induced pain in OXA-treated rats.39,40 However, the applicability of those animal studies to the use of hand and foot baths is not clear. 43 Because of the characteristic of OIPN, the direct topical application of herbal medicine could be an effective practice.17,18
Limitations of the Review
We only reviewed studies with patients who had not yet demonstrated any neuropathy symptoms, focusing on appraisals of the preventive efficacy of hand and foot baths. This excluded a considerable number of trials of patients with preexisting neuropathy. Although the search strategy was comprehensive, unpublished studies and those published in languages other than English and Chinese could have been unintentionally missed. All the participants were recruited from Chinese populations; so results should be interpreted with caution when applied to other ethnic groups. Publication bias cannot be excluded. Furthermore, the quality of the evidence was potentially affected when flaws in design led to high risk of bias in allocation, blinding, and selective reporting issues. Absence of multicenter or large-scale RCTs, sample size calculation, and follow-up impeded access to (long-term) reliable outcomes. Finally, the intervention group method described included the following: (1) soaking hands and feet in the herbal solution; (2) soaking between 20 and 40 minutes; (3) water temperature between 35°C and 45°C; (4) soaking once or twice a day for 5 to 21 days; and (5) beginning on the same day of initial OXA infusion or 1 day before. However, no consensus exists regarding which of these interventions is the best to address the efficacy. The review was compromised because various herbal combinations (or formula solutions) were used, and the reporting of CHM formulas (eg, herbal preparations, production, safety assessment) was inadequate. 44 Consistent inclusion of a specific OIPN intervention in future RCTs would help standardize Chinese herbal hand and foot baths and facilitate comparison across studies. Future network meta-analysis can also be conducted to compare the preventive efficacy between the different herbal formulations (or combinations).
Conclusion
To the best of the authors’ knowledge, this is the first meta-analysis that focuses on external use of CHM (hand and foot baths) for the prevention of cumulative OXA-related neurotoxicity. CHM tends to decrease the incidence of OXA-induced cumulative neurotoxicity. Importantly, no adverse events were reported significantly altering the efficacy of chemotherapy, thus enhancing patients’ tolerance to OXA treatment. However, all the included studies suffered from numerous methodological shortcomings and were, therefore, assessed to be at high risk of bias. Further high-quality prospective randomized data taking into account the characteristics of traditional Chinese medicine should be conducted to substantiate findings of the studies in this review.
Supplemental Material
Data_extraction_form_002 – Supplemental material for Can External Use of Chinese Herbal Medicine Prevent Cumulative Peripheral Neuropathy Induced by Oxaliplatin?: A Systematic Literature Review With Meta-analysis
Supplemental material, Data_extraction_form_002 for Can External Use of Chinese Herbal Medicine Prevent Cumulative Peripheral Neuropathy Induced by Oxaliplatin?: A Systematic Literature Review With Meta-analysis by Jie Hao, Xiaoshu Zhu, Caroline A. Smith and Alan Bensoussan in Integrative Cancer Therapies
Footnotes
Appendix
Search strategies for MEDLINE and CNKI.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work has supported by funding from the Western Sydney University Research Training Scheme (No. UWS18405473) and China Scholarship Council Higher Degree (Doctor of Philosophy) Program (No. CSC201506550006).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.