
Abstract
Acupuncture is an integrative therapy with strong evidence to support its use in the oncology setting, yet barriers exist for implementation into conventional medical clinics. Though acupuncture is recommended in clinical practice guidelines for oncology, there is little data in the literature showing how acupuncture and other related therapies, including herbal medicine are successfully implemented in some oncology clinics, while others experience barriers to care. To characterize the current use of acupuncture (ACU) and herbal medicine (HM) in oncology clinics, we collected general demographic and usage data from 5 example clinics. In addition, to better understand the barriers faced by ACU and HM clinics in implementing acupuncture as a treatment modality, a survey was deployed to 2320 members of the Society for Integrative Oncology. This article examines the characteristics of oncology settings around the world, and shares data from the survey on the use of these therapies in the field of oncology. The primary barrier to acupuncture care, as reported by providers, was cost. With just under 70% of the oncologists reporting it as the most important obstacle. Additional barriers to implementation included concerns about competency and training, accessibility and safety of herbal medicine during treatment. Though acupuncture is being incorporated into more conventional oncology settings, organized strategies for implementation involving payers and policymakers is needed.
Keywords
Introduction
Acupuncture 1 is an integrative therapy with high level of evidence to support its use for cancer patients in active treatment. As of 2016, 73.3% of NCI designated cancer centers offered acupuncture services to their patients 2 and numerous clinical guidelines include acupuncture for the management of symptoms in cancer care.3,4 Despite the growing evidence and use, there is little data indicating how acupuncture and other related therapies, like herbal medicine, have been implemented or sustained in oncology practice. For example, a 2020 review of the oncology acupuncture program literature yielded no results.
To understand the barriers when referring to acupuncture and herbal medicine providers, a roundtable discussion of stakeholders, including oncologists, acupuncture and herbal medicine providers and other oncology providers and administrators, gathered at a Society for Integrative Oncology (SIO) annual meeting. SIO is an international society whose mission is to advance evidence-based, comprehensive, integrative healthcare to improve the lives of people affected by cancer. The gaps in knowledge and literature within the oncology community and the published data on acupuncture and herbal medicine in oncology led to a recommendation to collect baseline data on barriers to implementing acupuncture and herbal medicine in the oncology setting. This article examines characteristics of acupuncture and herbal medicine programs in 5 oncology settings around the world, and shares data from an SIO Acupuncture Special Interest Group (SIG) survey of licensed acupuncturists and allied medical providers on the use of acupuncture and herbal medicine in oncology. We also examined the data from “A Survey of Licensed Acupuncturists in the San Francisco Bay Area: Prevalence of Treating Oncology Patients.” 5 From these source materials, we highlight common challenges to sustainability, and propose ways to overcome these challenges, best practices, and future steps.
There are many systems of Asian medicine, which includes acupuncture, taught and practiced worldwide. 6 While it is generally accepted that acupuncture and the theories of Asian medicine originated in China, there are systems that developed in Japan, Korea, and Vietnam, as well as in European countries and the United States. The authors use the term acupuncture and herbal medicine “AHM” to encompass all the lineages and related practice styles and to describe a variety of different treatment modalities including acupuncture, Chinese herbs, diet, nutrition, supplements, and manual/movement therapies. The term AHM has recently been adopted by the profession. Both the educational council, Council of Colleges of Acupuncture and Herbal Medicine (CCAHM), 7 and the accreditation commission, Accreditation Commission for Acupuncture and Herbal Medicine (ACAHM), 8 in the US, have changed their names to remove the term Oriental medicine and replace it with acupuncture and herbal medicine in an effort to reduce bias and discrimination within this field of medicine, consistent with anti-racist practices.
A survey conducted in 2021 by Yang et al surveyed CSIO (China Society for Integrative Oncology) oncologists and their colleagues on the characteristics, status, and challenges of integrative oncology in China. 9 While the term integrative oncology may not be as well known in China, Acupuncture and Herbal Medicine is commonly used there in academic institutions, provincial hospitals and TCM hospitals. Attitudes toward AHM are largely positive among oncologists and the public, and barriers to access are low due to public funding. The notable differences in the practice of AHM in China and western countries are that Chinese herbal medicine is the most widely used modality compared to acupuncture in the West and AHM is more widely practiced in hospitals in China, often delivered in an integrated way with other cancer conventional interventions.
Acupuncture/AHM in Cancer Care
In 1997 a 12-member panel at a National Institutes of Health Consensus Conference concluded that “there is clear evidence that needle acupuncture treatment is effective for postoperative and chemotherapy nausea and vomiting.” 10 Numerous clinical trials have demonstrated the effectiveness of acupuncture for other cancer-related symptoms11 -14 including cancer related pain, chemotherapy induced peripheral neuropathy, fatigue, hot flashes, xerostomia, lymphedema, dyspnea, cachexia, dysphagia, post-operative pain, anxiety, depression, insomnia, constipation, diarrhea and the arthralgias associated with aromatase inhibitor therapies. The growth in data on the safety and efficacy of acupuncture in the treatment of cancer related symptoms and treatment side effects has been a driving factor behind the inclusion of evidence-based recommendations of acupuncture in public health statements by national and state governments, health departments 15 and clinical practice guidelines for patients with lung 3 and breast 4 cancers. The inclusion of acupuncture in these clinical practice guidelines indicates broad support of acupuncture and an increasing acceptance of including acupuncture in standard cancer care by oncologists, conventional medical providers, and health systems including cancer centers.
In addition to the recommendations in clinical practice guidelines, acupuncture is recommended by the American Cancer Society (ACS) for the treatment of side effects associated with conventional cancer therapy and cancer-related ailments. 16 According to Kilian-Kita et al “acupuncture may become an interesting and valuable addition to conventional medicine.” 17 Towler et al stated in their review, “Acupuncture should be considered for symptom management where there are limited treatment options, using current peer-reviewed guidelines and clinical reasoning.” 18
Evidence on the safety and efficacy of Chinese herbal medicine during cancer treatment is limited, and more studies are needed. Ho et al found that the addition of Chinese herbal medicine to conventional treatment was associated with better tumor response as well as prolonged survival in women with breast cancer. 19 A meta-analysis of patients taking Chinese herbal medicine containing Astragalus-containing Chinese herbal medicine along with chemotherapy has shown benefit in enhancing curative effect and reducing side effects for cervical cancer patients. 20 Shen et al cites additional meta-analyses on Astragalus-containing Chinese herbal medicine in non-small cell lung cancer, breast cancer and gastric cancer patients, however, as noted by the authors, the risk of bias is high as many of the studies were of poor design. A 2006 meta-analysis that evaluated Chinese herbs with platinum-based chemotherapy in non-small cell lung cancer concluded that Chinese herbal medicine based on Astragalus (Huang Qi) may increase the effectiveness of platinum-based chemotherapy when used in conjunction with platinum-based chemotherapy in non-small cell lung cancer. 21 However, a 2016 meta-analysis on randomized controlled trials of Chinese herbal medicines combined with fluorouracil-based chemotherapy by the same author reported poor methodological quality of the studies with high frequency of low-quality and/or biased studies of Chinese herbal medicine undermining confidence in the results. 22 Research in 2018 of 6939 lung cancer patients in Taiwan investigated the frequencies and patterns of Chinese herbal medicine treatment for lung cancer patients and its effect on their survival probability. The conclusion was that the use of Chinese herbal medicine as adjunctive therapy might reduce the mortality hazard ratio of lung cancer patients. 23 Zhang et al reported evidence for reducing damage from radiation in mice and cell studies by Chinese herbs. 24 In a review article, Ross (2014) reported curcumin (Yu Jin and Jiang Huang) was shown to potentiate the antitumor effect of some anti-cancer medications and attenuate side effects such as gastrointestinal effects. 25
AHM is a whole-person medical system. AHM practitioners frequently treat multiple complaints simultaneously. People diagnosed with cancer often experience multiple physical and emotional symptoms concurrently. The concept of cancer symptom clusters is defined as the co-occurrence of 2 or more related symptoms. 26 A review of 18 studies by Kim et al 27 found that the most common symptoms experienced by patients with cancer during treatment were fatigue, dry mouth, insomnia, drowsiness, mood disturbance, and pain and that more than 5 concurrent symptoms were experienced by 22% to 30% of patients. A unique benefit of AHM therapies in cancer symptom management is its use as a single therapy for multiple complaints or symptom clusters. These single interventions can reduce polypharmacy, drug interactions, and side effects, as well as reduce the cost of treatment per patient.
Methods
Our aim was to identify barriers to integrating acupuncture and herbal medicine (AHM) with conventional oncology care. In order to accomplish this aim, we gathered both quantitative and qualitative data.
To evaluate the challenges facing AHM practices in the field of oncology, we surveyed active Society for Integrative Oncology (SIO) members, inactive members, and affiliates (Supplement 1). The survey was an online branched survey for AHM and conventional medical providers to ask specific questions related to the provider’s specialty. It was sent to 2320 members, past members and affiliates of SIO. The survey was approved by Indiana University School of Medicine IRB number (2005829320). An invitation to take the online survey was sent to 2320 members and affiliates of SIO. Survey Monkey was used to administer the questionnaire. We used a previous survey 5 of licensed acupuncturists treating oncology patients in the San Francisco Bay Area to assist in the design of our survey.
For our qualitative exploration, we selected 5 oncology clinics that members of the SIO Acupuncture Special Interest Group (SIG) are employed at and compared their business practice characteristics and use of AHM in oncology. These clinics are located within hospitals and academic centers or are community-based and include diverse AHM practice models that interact with conventional oncology providers. We also conducted narrative interviews of these 5 AHM providers. The providers were asked to share information about their clinical settings and business models, including barriers to sustainability (Supplement 2). Interviews were conducted from August to October 2020.
The 5 clinical settings included: Memorial Sloan Kettering Cancer Center (MSK), an NCI designated comprehensive cancer treatment center and academic research institution; California Cancer Associates for Research and Excellence, a community outpatient center; Chicken Soup Chinese Medicine, a private practice with a focus on integrative oncology, Refuot integrative medical center, an Israeli integrative center with integrative research mainly on herbal medicine in oncology; and Seattle Cancer Care Alliance (SCCA), a non-profit NCI-designated comprehensive cancer center focusing on cancer treatment, research and education. On April 1, 2022, Seattle Cancer Care Alliance and Fred Hutchinson Cancer Research Center merged to form Fred Hutchinson Cancer Center.
For each setting, we interviewed the AHM providers about the clinical practice, the integrative oncology services provided, the most common conditions treated by AHM practitioners, the impact of AHM services on patient care, the advantages and challenges of each practice, the reimbursement and employment models, and the history of integrative oncology at each setting.
Results
Statistical Methods
The majority of responses to the survey are presented as a percentage of total responses with no analysis conducted. However, questions that consisted of either a response by a Likert scale or multiple choice were analyzed using descriptive statistics with median, mean and standard deviation provided.
Survey Results
The survey was sent to 2320 members, past members and affiliates of SIO, and was closed after 14 days. We received 219 responses to the survey, 88 from AHM providers (79 completed) and 131 from conventional medicine providers (109 completed). This is a 9.44% response rate. Respondents included AHM providers, oncologists, other oncology providers, administrators and caregivers (Figure 1).

What is your role?.
To better understand the clinical practices of AHM providers, we asked respondents what style of acupuncture they practiced, what modalities they used in treating cancer patients, what percentage of cancer patients they treat in their clinics and what stage of diagnosis patients are in when they seek out AHM therapies.
When surveying the AHM providers, it was important to consider the many styles of acupuncture. 6 The results showed that 82.28% of respondents reported their primary style of acupuncture as Traditional Chinese Medicine, 5.06% reported Japanese Meridian style and 3.80% reported Five Element style, all traditional styles. Zero percent was reported for Richard Tan style, taught in many acupuncture programs, and French Energetics-Helms’s style, taught to many medical doctors.
Of the 79 AHM respondents, 55 reported that they practice in an integrative setting with allied health care providers. Respondents were asked what types of cancer patients they treat, with the option to select all that apply. Most reported treating those undergoing active treatment followed by those in post-treatment and those who have been newly diagnosed (Figure 2).

Please indicate which types of cancer patients you are treating in your practice.
To assess financial sustainability and clinic volume when including AHM in the conventional oncology setting, we asked respondents how many patients they treat in an hour. Though most respondents reported treating 2 or more patients per hour, there were 18 (22.78%) who reported treating only 1 patient per hour (Figure 3).
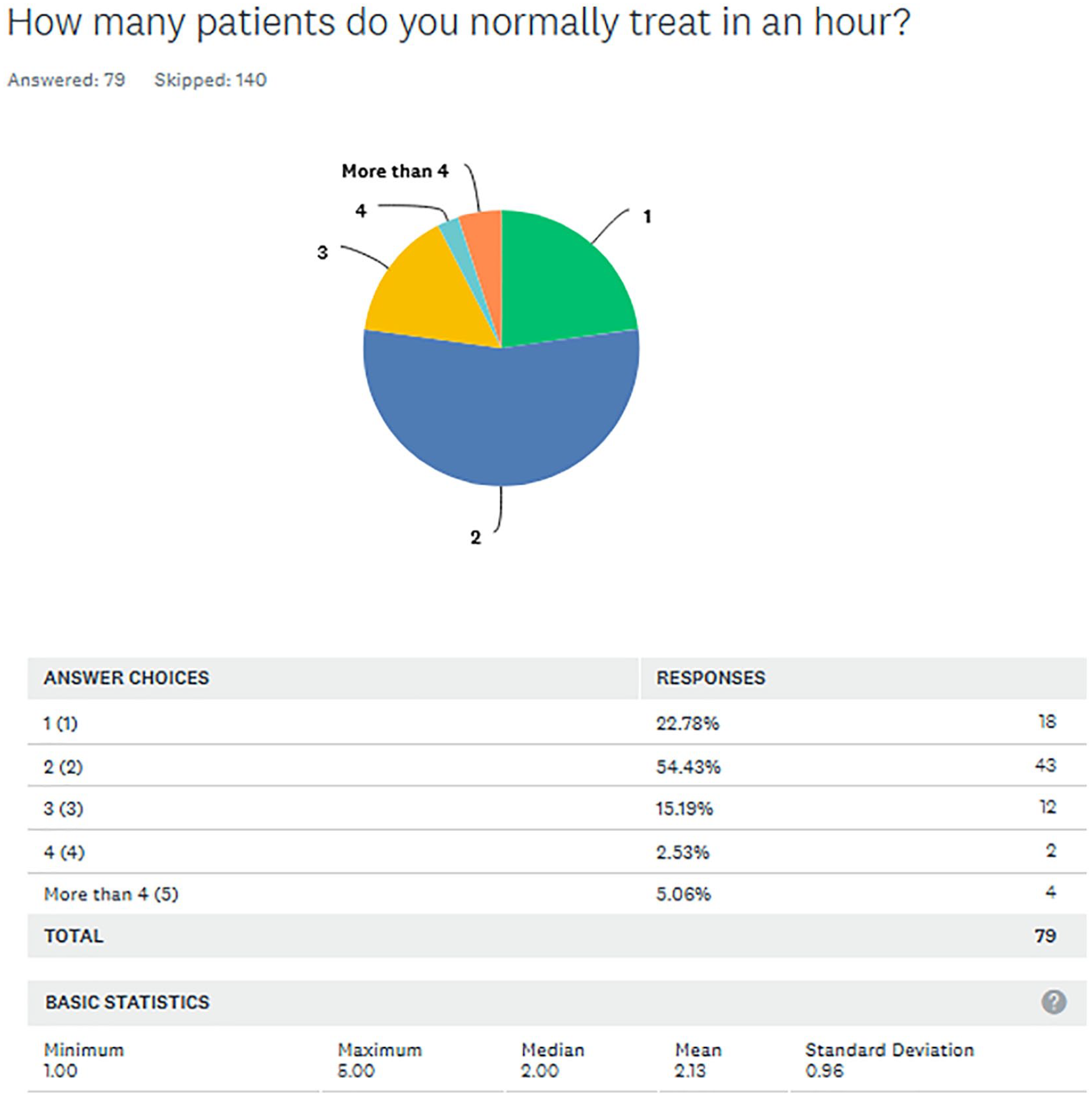
How many patients do you normally treat in an hour?.
AHM practitioners reported using multiple modalities when treating cancer patients with acupuncture as the most predominant modality (Figure 4).
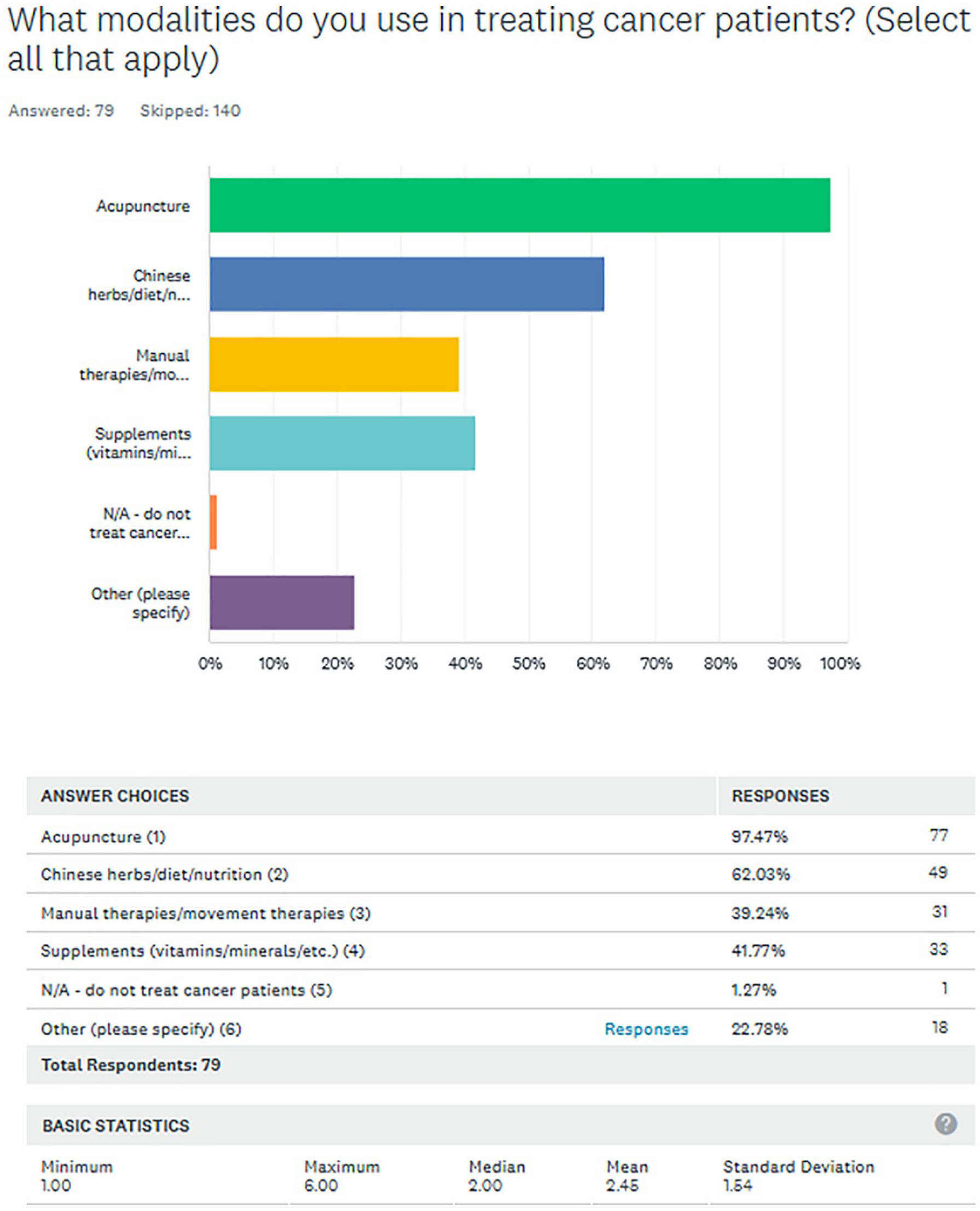
What modalities do you use in treating cancer patients?.
In the survey, all respondents were asked open-ended questions about any barriers they experienced regarding the use of Chinese herbs with oncology patients. Some respondents reported a fear of drug-herb interactions or reported lack of research concerning efficacy and safety as a barrier, and some providers were unable to administer Chinese herbs because either the hospital or oncologist forbids it.
Out of 131 conventional medicine practitioners surveyed, 109 completed surveys were received. Two respondents, 1.83%, did not think acupuncture should be offered in oncology clinics (Figure 5).

Do you think acupuncture should be offered in oncology clinics?.
Of the 109 completed surveys in the branch for conventional Western medical providers, 70 (64.22%) reported working in an integrative clinic with both licensed acupuncturists (L.Ac.) and allied health providers, 68 (62.39%) reported that the L.Ac. they work with is certified by National Certification Commission Acupuncture and Oriental Medicine (NCCAOM). We also asked if a non-acupuncturist such as a chiropractor or physical therapist was practicing acupuncture or dry needling in their clinic and 18 (16.51%) reported Yes.
To understand why patients are referred for acupuncture in the oncology setting, we included symptoms commonly associated with cancer treatment for which acupuncture has evidence of effectiveness. We asked respondents to rank from 1: most referrals to 4: least referrals (Figure 6).

In your paractice, what is the primary reason for acupuncture referral in oncology setting?.
Figure 7 shows that cost was the primary barrier to respondents referring patients to acupuncture. All other barriers were ranked considerably lower by conventional medical providers surveyed. The second most reported barrier was concern about competency and training which scored a 2.92. In the survey the third reported barrier was lack of certification. Patient safety ranked lowest of the 4 barriers to referring to an acupuncturist. More than one-third of the respondents did not report these 3 options as barriers.

What is the primary barrier to referring to an acupuncturist?.
Interview Results
Memorial Sloan Kettering Cancer Center, a Cancer Treatment and Academic Research Institution
Memorial Sloan Kettering is the oldest and largest private dedicated cancer hospital in the US, founded in New York in 1884 and records roughly 500 000 visits per year.
The Integrative Medicine Service at MSK was founded in 1999 with support and vision from Laurance Rockefeller and the leadership of founding service chief Barrie Cassileth, Ph.D. The mission is to lead the world in discovery, translation and dissemination of evidence-based integrative therapies to improve the lives of those who have been touched by cancer.
The Integrative Medicine Service at MSK is currently led by Jun Mao, MD, MSCE and has 35 Integrative Oncology providers, including 5 physician faculty, a nurse practitioner, a pharmacist and certified practitioners in acupuncture, massage, music therapy, exercise, tai chi, yoga, dance therapy, art therapy, meditation and guided imagery.
Acupuncture is provided by 4 full-time licensed acupuncturists, 1 to 2 part-time trainees, and 3 of the 4 faculty physicians who are certified in acupuncture. Acupuncture treatments are provided at the bedside at Memorial Hospital, as well as at MSK ambulatory sites. Most ambulatory acupuncture is provided at The Bendheim Integrative Medicine Center in Manhattan, which is open 6 days per week. Acupuncture is also offered at 6 MSK regional ambulatory care sites in the NY and NJ suburbs on a more limited schedule.
The most common referral for acupuncture at MSK is pain, either musculoskeletal, neuropathic or malignant. Other common referrals are for side effects of medication such as hot flashes, joint pains and nausea, as well as general support during chemotherapy or other active treatment. The specialties that refer most frequently to acupuncture are breast and gastrointestinal oncology, followed by gynecological, prostate, respiratory cancers, and lymphoma.
Ambulatory acupuncture is an out-of-pocket expense, though patients who have coverage through their health insurance may submit claims for reimbursement directly to their insurance providers. Bedside acupuncture is provided at Memorial Hospital and must be ordered by an NP or MD; these treatments are provided at no-charge to the patient. An acupuncturist is on site at Memorial Hospital 4 days per week to handle inpatient referrals.
In addition to patient care, acupuncturists and faculty from MSK Integrative Medicine lead talks and workshops for patients, oncologists and support staff about the benefits of acupuncture for oncology patients. Online and in-person trainings are also offered to licensed acupuncturists interested in learning about working with oncology patients. Memorial Sloan Kettering sponsors and hosts integrative oncology conferences that draw leaders in the field from around the world. Courses are promoted through social media postings and internal marketing.
Memorial Sloan Kettering’s Integrative Medicine Service has conducted numerous clinical trials on acupuncture for symptomatic care in cancer patients. Staff acupuncturists provide study interventions, with support from clinical research coordinators.
California Cancer Associates for Research and Excellence, a Community Outpatient Center
California Cancer Associates for Research and Excellence (cCARE) is a community outpatient practice located in San Diego and Fresno, CA. Within San Diego, cCARE has 5 offices. In 2009, 2 AHM practitioners approached cCARE asking if they could provide services to patients after normal business hours. As interest started to increase, the 2 practitioners gave talks about the benefits of AHM to patients while they were in the infusion center receiving chemotherapy. They offered the staff discounted treatments so they could experience the benefits of AHM as well. Eventually the demand for services increased and the practitioners began to offer treatment 3 days per week in 2 different offices.
In 2011, one AHM practitioner developed a full-time practice within the walls of cCARE. In 2012 5 other practitioners with different specialties were hired and extended integrative oncology (IO) services to 3 cCARE offices. In 2016, lack of space and feasibility became an issue, and the IO team was dissolved. Currently, one practitioner provides all IO services for cCARE, including acupuncture, Chinese herbal medicine, functional medicine, and nutrition. Services are provided in one office, although referrals come from all the cCARE offices. There is a rental agreement between the IO practitioner and cCARE, which allows for designated treatment rooms for IO services.
The most common conditions treated are peripheral neuropathy, fatigue, and neoplastic pain. The major barrier to IO services for patients at cCARE is cost. All IO services are an out-of-pocket expense. Insurance is not accepted.
Chicken Soup Chinese Medicine, a Private Practice With a Focus on Integrative Oncology
Chicken Soup Chinese Medicine is an Integrated Chinese Medicine practice located in San Francisco, CA. This private clinic was established in 1990 (after the closure of Quan Yin Acupuncture and Herb Center due to the Loma Prieta earthquake). Chicken Soup primarily focuses on treating patients with chronic viral illness, HIV, complex gynecology, and cancer. Early on, the founder developed relationships with other medical providers at the San Francisco AIDS Alternative Healing Project and Quan Yin Healing Arts Center, which expanded her work in the field of oncology.
Currently, there are 3 (2 fulltime and 1 part-time) practitioners at Chicken Soup Chinese Medicine. They provide integrative care including complex consultations, acupuncture, Chinese herbal medicine, natural supplementation, nutrition, and therapeutic massage. Case management is also provided for oncology patients in conjunction with conventional Western practitioners. Services are provided in one office, and referrals come from oncology practices, oncology patients, primary care practices and the internet. Private insurance and Medicare Advantage plans are accepted for all services that insurance will reimburse—often acupuncture only, often therapeutic massage, and in some cases consultations and treatment plans. The Misha Ruth Cohen Education Foundation, located within the same setting, also provides subsidized care for a limited number of oncology patients.
The most common conditions treated are peripheral neuropathy, fatigue, low blood counts, and nausea/lack of appetite. The major barrier to IO services is the lack of understanding about services and benefits of integrative oncology services by other providers.
Refuot, an Integrative Medical Center, is a Clinical Practice Comprised of Clinicians in the Fields of Chinese & Japanese, Homeopathic, Complementary and Biomedical Medicine
Refuot Integrative Medical Center is located in Tel Aviv, Israel. The center was established in the 1995 and it includes integrative practitioners, mainly Chinese medicine specialists with a focus on treating pediatric, orthopedics, and cancer patients. From the setup of the center there was an intention to have a mixed practice of practitioners with an MD background and non-MD’s. This center was one of the pioneering clinics which maintained an ongoing relationship with conventional medical center and carried out integrative research mainly on herbal medicine focused on oncology.
Currently, the 20 part time practitioners at Refuot provide integrative care including acupuncture, Chinese herbal medicine, natural supplementation, nutrition, homeopathy, reflexology and Shiatsu. Referrals come from word of mouth, social media and medical referrals.
The most common conditions treated are general recovery or side effects of conventional cancer treatments, low immunity and WBC count, fatigue, peripheral neuropathy and menopausal symptoms. The major barriers to IO services are lack of public awareness of the benefits, financial barriers, and fear of interaction with conventional treatment.
Seattle Cancer Care Alliance, a Comprehensive Cancer Center Focusing on Cancer Treatment, Research and Education
Seattle Cancer Care Alliance (SCCA), the first NCI-designated comprehensive cancer in the Pacific Northwest, is a non-profit institution focusing on cancer treatment, research and education. Founded in 1998, SCCA is an alliance of 3 partner organizations, including the Fred Hutchinson Cancer Research Center, University of Washington Medicine and Seattle Children’s Hospital. SCCA began offering care to patients in 2001 and treats over 40 000 unique patients per year. Seattle Cancer Care Alliance has 9 clinical care sites 28 in the region as well as Network affiliations with hospitals in 5 states. On April 1, 2022, Seattle Cancer Care Alliance and Fred Hutchinson Cancer Research Center merged to form Fred Hutchinson Cancer Center.
The SCCA Integrative Medicine Program 29 was established in 2017 and opened to patients in 2018. The Integrative Medicine program is housed within the SCCA Supportive Care Division, which also includes Palliative Medicine, Pain, Psychiatry/Psychology, Social Work, Nutrition, Physical Therapy, and Spiritual Health. Integrative Medicine activities span organizations across the Alliance to accomplish its clinical, research and education goals. The SCCA Integrative Medicine clinical program offers billable clinical services currently offered by 6 providers: Integrative Medicine outpatient consults are offered by a naturopathic physician and an integrative medicine-trained advanced practice provider (nurse practitioner), and outpatient acupuncture is provided by 4 staff acupuncturists. Prior to the COVID-19 pandemic, free twice weekly in-person yoga classes for patients and caregivers were offered by a yoga teacher. As SCCA expands its clinical reach to additional sites, the Integrative Medicine program is expanding existing services to all SCCA sites and plans to hire additional providers. As with many healthcare institutions, the COVID-19 pandemic prompted the roll-out of telehealth services across SCCA, including the Integrative Medicine program where ongoing telehealth services are offered by the naturopathic physician and nurse practitioner.
In 2020, the Integrative Medicine team saw approximately 90 unique patients per month and conducted 125 to 150 visits each month via in-person ambulatory treatments and telemedicine. The acupuncture team treated approximately 45 unique patients per month and conducted 90 acupuncture treatments per month on average in 2020. Insurance is accepted and billed in-house for all integrative medicine services at the SCCA. Patients without insurance coverage have the option to self-pay. Washington State is unique in the United States in that in 1996, the insurance commissioner mandated that private payors cover naturopathic medicine, acupuncture, massage, and chiropractic clinical services. The exception to the billable services is group yoga classes which are offered free-of-charge and all patients and caregivers are welcome. All integrative medicine appointments require a referral from an SCCA provider and patients must be receiving oncologic care at SCCA, University of Washington, or Seattle Children’s Hospital to be seen in Integrative Medicine. The most common referral for acupuncture at SCCA is pain, either musculoskeletal, neuropathic or malignant. Other referrals are side effects of medication such as hot flashes, joint pain and nausea. Patients require a referral by a member of their oncology care team through an order placed in the EMR. The departments that refer most frequently to acupuncture are breast and gastrointestinal oncology. At SCCA, Chinese herbal medicine is not offered.
Currently, the demand for acupuncture services at SCCA exceeds capacity with a 2- to 3-month waitlist for patients. In order to facilitate acupuncture care for patients, the Integrative Medicine team has created patient education materials to provide information on how to work with acupuncturists in the community and has developed a list of regional acupuncturists based on a set of criteria to assess the level of training and experience with oncology acupuncture.
Expanding the evidence-base for integrative oncology research is a core goal of the Integrative Medicine program. Dr. Heather Greenlee, ND, PhD, MPH is the founding Medical Director of the SCCA Integrative Medicine program and runs a research program out of the Public Health Sciences and Clinical Research Divisions of the Fred Hutchinson Cancer Research Center. 30 The research uses observational studies and clinical trials to study integrative medicine and lifestyle interventions to improve cancer prevention and cancer survivorship, including diet, physical activity, weight management, acupuncture, dietary supplements and mind-body medicine. The research team includes a staff scientist, research coordinators, and administrative staff. Specific to Integrative Medicine, the research team currently includes 5 per diem clinical research acupuncturists who are trained and overseen by staff acupuncturists. Research acupuncturists are hired and work as needed to provide acupuncture treatments on funded acupuncture clinical trials across SCCA. In addition to clinical and research endeavors, the team is committed to providing integrative medicine training and education to patients and providers, including oncology fellows, and nurse practitioners. The Integrative Medicine program participates in 2 formal clinical training programs, including the Supportive Care Rotation of the University of Washington/Fred Hutchinson Hematology and Medical Oncology Fellowship and the Advanced Practice Provider (APP) Fellowship in Oncology and Stem Cell Transplant. The trainees attend and participate in regular case management meetings and have the opportunity to observe the integrative medicine clinics. The integrative medicine staff offers in-service trainings on the evidence for integrative medicine to SCCA providers to better inform the staff on incorporating integrative medicine into patient treatment plans. SCCA produces educational resources on integrative medicine, including mind-body/meditation techniques, resources for improving sleep and the use of acupressure for symptom control, for patients and caregivers (Table 1).
Demographics of Integrative Oncology (IO).

All numbers are approximate numbers for 2020.
Cost and Reimbursement of Acupuncture and Chinese Herbal Medicine Services.

All numbers are approximate numbers for 2020.
Does not accept Health Funds overage.
Common Conditions Treated by AHM Practitioners.*

Based on practitioner experience.
Future Steps.

Discussion
This initial data provides a baseline understanding of ways AHM practitioners in the SIO community integrate AHM with oncology-care and supports a larger qualitative examination of the delivery of AHM in these setting in the future.
The authors have identified limitations to the survey design that will inform future surveys and may be of value in better understanding practices and identifying potential barriers. The limitations include: (1) Chinese herbs and dietary recommendations were grouped together since some herbs are food and food is medicine. Separating the use of Chinese herbs, diet, and nutrition in survey questions could improve the quality of data; (2) including questions on the demographics and practice details of respondents in future surveys may narrow the data and facilitate further analysis; (3) there was a low response rate. Strategies to increase response rates will be explored in future surveys; (4) data was collected before the COVID 19, and some clinics reduced in-patient visits during the pandemic.
Referral to Acupuncture
It was not surprising that pain and neuropathy were the primary reasons for a medical oncologist to refer a patient to acupuncture. These conditions are also among the common conditions treated by AHM reported in the interviews. There was a notable lack of referrals for immune support, despite some evidence in the literature on effects of acupunctures on neutropenia in patients receiving myelosuppressive chemotherapy 31 and other aspects of the immune system. 32
Solutions to Overcome Barriers and Provide Hands-on Tools for AHM Practitioners to Deliver the Highest Level of Integrative Care
According to the SIO Survey, almost 70% of the conventional Western medicine providers reported the primary barrier to referral to an acupuncturist is cost, scoring a 3.62 in a 4-point Likert scale (Figure 6). The authors surmise this may be due to inconsistent and minimal insurance reimbursement and patients’ ability to pay, or lack of insurance coverage. All outpatient visits at the centers examined in this report are cash-pay. Three of the 5 centers (Chicken Soup, Refuot, SCCA) bill insurance to offset costs if the patient has coverage for acupuncture. Incorporating acupuncture coverage under more insurance policies is a needed solution to the cost barrier. 32
The primary barrier reported by oncologists for the use of Chinese herbal medicine was safety and concerns including herb-drug interactions. As reported above, patient safety ranked lowest of the 4 barriers to referring to an acupuncturist.
Cost
Insurance coverage differs widely from state to state and between plans offered. A review of covered nonpharmacologic pain options among 15 U.S. insurance plans found only 1 in 5 offered acupuncture benefits. 33 In some cases, the insurer covered acupuncture therapy for a few specific conditions and often for a prespecified number of treatments. As with many covered interventions, the amount of coverage per payor can ultimately influence whether that intervention will be available in a community. Recently, Medicare confirmed it will reimburse for acupuncture therapy as a treatment for chronic non-malignancy related low-back pain. 34 However, coverage is restricted to acupuncturists who are supervised by a Centers for Medicare and Medicaid Services (CMS) approved medical provider and moreover, it does not allow access for those who could benefit from acupuncture for cancer related symptoms. Reimbursement for only one condition that does not relate to cancer poses a significant barrier to Medicare participants with cancer.
Programs at larger institutions such as Memorial Sloan Kettering can offset the lack of reimbursement by tapping into the resources available at the organization such as philanthropic and research grants, support for marketing and promotion, and a large pool of potential patients. This funding allows MSK to provide inpatient acupuncture at no cost to the patient. Access to these resources provides an advantage and may account for the larger program size and range of services offered in the institutional setting.
Accessibility
There is a relatively small number of licensed acupuncturists in the US. 35 More than 50% of licensed acupuncturists are located in California, Florida and New York alone. 35 Distribution of licensed acupuncturists is uneven throughout the US, even in states with higher per capita acupuncturists, which can lead to patients needing to travel long distances for treatment. Access is dependent on the state, insurance coverage, availability of subsidized and/or low-cost programs and rural versus urban locations.
Oncology trained acupuncturists are a small subset of licensed acupuncturists which compounds the lack of access to providers with experience and knowledge in the field of oncology. Concerns about lack of training and experience treating oncology patients was identified as the second most reported barrier for conventional medicine providers in the SIO survey, scoring a 2.92 in a 4-point Likert scale. Based on the San Francisco Bay Area survey 5 there appears to be minimal oncology specific training among licensed acupuncturists with the majority reporting 100 hours or less. Ideally, licensed acupuncturist who treat people diagnosed with cancer would acquire oncology specific training as part of the standard curriculum.
AHM services may be optimized by oncology patients if cancer centers employ AHM providers on site. Acupuncturists are keen on joining health care systems. 36 For example, acupuncturists who work at some larger centers, such as MSK and SCCA, are salaried and receive benefits. Both MSK and SCCA cancer centers educate their medical providers on evidence that supports the use of acupuncture and integrative therapies. Oncology trained acupuncturists are needed outside of cancer centers as well due to long waitlists for AHM services within cancer centers.
Our data highlighted a need for information on how to select acupuncture and AHM providers outside of cancer centers.
Safety of Chinese Herbal Medicine
Acupuncture is widely accepted as a safe intervention, 37 which was reflected in the responses to the SIO survey showing acupuncture is perceived as safe and is the most predominant modality used. Chinese herbs did not have the same perception among conventional medical providers, and our survey identified the primary barrier to use of Chinese herbal medicine with patients undergoing cancer treatments is safety and concerns including herb-drug interactions. These concerns highlight the need for more research on the safe use of Chinese herbs with people with cancer.
The use of chemotherapy and other cancer treatments comes with risks, and managing toxicities and interactions with other substances is a major concern for oncologists. The lack of knowledge about herb, supplement and drug interactions leads to the commonly held belief that Chinese herbal medicine interactions with conventional treatments are harmful. However, it should be emphasized that herbal medicine in combination with cancer treatments can either improve, interfere, or not affect the outcomes. 38 Resources on the safety of herbs in conventional medicine and AHM settings are regularly used by pharmacists, clinicians and patients to review products for potential interactions and effectiveness, such as Natural Medicines 39 a database on dietary supplements, natural medicines and complementary alternative and integrative therapies. AHM practitioners who work with oncology patients should have advanced training in Chinese herbal medicine focused on oncology. The authors recommend that training should include how to utilize a dynamic database for current interactions information.39,40 The 3 providers who prescribe herbal medicine to oncology patients all reported that they evaluate each individual patient, review relevant lab reports for each patient and provide evidence-based documentation to patients and their oncology providers on the safe use of herbs when it is clinically appropriate. While this approach to prescribing may be onerous and may limit the use of supplements and herbs in the oncology setting, the authors believe safety is the highest priority. Some providers at conventional cancer centers are unable to recommend herbs due to institutional policies. Many acupuncture curriculums include the study of herbal medicine, and there is a national certification for Chinese herbal medicine, 41 however, most states do not regulate the practice of herbal medicine.
Communication
Thirty-four percent effective communication with oncologists and oncology care teams is especially important when treating people diagnosed with cancer. 5 One consideration is the change in blood counts that can come with conventional cancer treatments. 37 If the AHM practitioner is prescribing herbal formulas, as 79% of the respondents indicated in the San Francisco Bay Area survey, communication with the oncology care team is crucial due to potential herb-drug interactions.40,42 When AHM practitioners work side-by-side with oncologists in cancer centers, proximity can facilitate these discussions.
Implementation
For acupuncture to become more integrated into conventional cancer care, better implementation strategies are needed to help ensure patients are able to follow-up on oncology team recommendations and referrals to use acupuncture 43 and have their acupuncture treatment costs covered as a part of their cancer care.3,4,15 It is important for the AHM community to become more informed about the clinical practice guideline recommendations and improve implementation of these recommendations.
Operationally, oncology care teams will need to identify the role of AHM including when, where, and how to request it. This process may include creating a referral process including conditions appropriate for acupuncture, instructing how to place orders in the electronic medical record (EMR) and/or electronic health record (EHR) and educating care teams about appropriate referrals until acupuncture becomes embedded in the organization. 44
Competency and Training
Conventional providers reported another barrier to referring to acupuncture was concern about lack of competency and training in working with this complex patient population (Figure 6). In the San Francisco Bay Area survey, 5 Abrams et al sought to learn more about what proportion of AHM practitioners care for cancer patients, their cancer-specific training, their cancer-specific caseload, interventions utilized, their outcomes, and their communication patterns. Twenty-one percent of the licensed acupuncturists responded with 77% reporting treating patients with cancer. Seventy-six percent of the respondents reported having 0 to 100 hours of training specific to the needs of patients with cancer, with 34% reporting 101 to 1000 hours.
Lack of oncology-specific training was identified as a barrier by the conventional providers surveyed. Presently, graduate-level AHM education does not require didactic or clinical education on oncology acupuncture or acupuncture therapy in health care systems, leaving AHM practitioners to self-learn, learn on the job, or seek continuing education courses on the topic. There are few continuing education opportunities to support AHM clinicians and raise the level of clinical care provided to oncology patients. Recognizing the gap in training, members of SIO developed an Oriental Medicine Oncology Intake Checklist 45 to help AHM practitioners deliver the highest level of integrative care while evaluating oncology patients. In addition to specific intake questions that facilitate information gathering to deliver safe acupuncture treatments, the SIO Oriental Medicine Oncology Intake Checklist includes oncology resources for acupuncturists. Future steps include the development of a guide to assist patients and providers in choosing an oncology trained AHM provider.
Conclusion
Despite the growth in utilization of AHM by people diagnosed with cancer along with the expanding body of evidence to support use of AHM therapies to help manage the symptoms of cancer treatments, significant barriers exist for implementation into conventional medicine. Foremost is cost, due to limited insurance reimbursement and limits care to the underserved. Additional challenges include finding providers with specific training in oncology, coordination of care in both in-patient and outpatient settings, and concerns about the safety of using Chinese herbs with patients undergoing cancer treatment.
Better communication between AHM providers and oncologists emerged as a solution to multiple barriers. Creating a referral process including conditions appropriate for acupuncture, instructing how to place orders in the electronic medical record (EMR) and/or electronic health record (EHR) and educating care teams about appropriate referrals is needed.
It is equally as important for the AHM community to become more informed about the clinical practice guideline recommendations and improve implementation of these recommendations.
This exploration into the business of AHM in the oncology setting might serve as a starting point for future work in overcoming the barriers to providing proven AHM treatments in conventional settings as well as highlighting some distinct challenges unique to Chinese herbal medicine. An organized strategy for implementation of AHM in oncology settings involving a diverse group of federal and private payers and policymakers is needed.
Supplemental Material
sj-doc-2-ict-10.1177_15347354241226640 – Supplemental material for Characteristics and Challenges of Providing Acupuncture and Chinese Herbal Medicine in Oncology Treatment: Report of Survey Data and Experience of Five Unique Clinical Settings
Supplemental material, sj-doc-2-ict-10.1177_15347354241226640 for Characteristics and Challenges of Providing Acupuncture and Chinese Herbal Medicine in Oncology Treatment: Report of Survey Data and Experience of Five Unique Clinical Settings by Susan Veleber, Misha Ruth Cohen, Matthew Weitzman, Yair Maimon, Christine A. Adamo, Jonathan Siman, Weidong Lu, Tammy Sajdyk and Jennifer A.M. Stone in Integrative Cancer Therapies
Supplemental Material
sj-doc-3-ict-10.1177_15347354241226640 – Supplemental material for Characteristics and Challenges of Providing Acupuncture and Chinese Herbal Medicine in Oncology Treatment: Report of Survey Data and Experience of Five Unique Clinical Settings
Supplemental material, sj-doc-3-ict-10.1177_15347354241226640 for Characteristics and Challenges of Providing Acupuncture and Chinese Herbal Medicine in Oncology Treatment: Report of Survey Data and Experience of Five Unique Clinical Settings by Susan Veleber, Misha Ruth Cohen, Matthew Weitzman, Yair Maimon, Christine A. Adamo, Jonathan Siman, Weidong Lu, Tammy Sajdyk and Jennifer A.M. Stone in Integrative Cancer Therapies
Supplemental Material
sj-docx-1-ict-10.1177_15347354241226640 – Supplemental material for Characteristics and Challenges of Providing Acupuncture and Chinese Herbal Medicine in Oncology Treatment: Report of Survey Data and Experience of Five Unique Clinical Settings
Supplemental material, sj-docx-1-ict-10.1177_15347354241226640 for Characteristics and Challenges of Providing Acupuncture and Chinese Herbal Medicine in Oncology Treatment: Report of Survey Data and Experience of Five Unique Clinical Settings by Susan Veleber, Misha Ruth Cohen, Matthew Weitzman, Yair Maimon, Christine A. Adamo, Jonathan Siman, Weidong Lu, Tammy Sajdyk and Jennifer A.M. Stone in Integrative Cancer Therapies
Footnotes
Acknowledgements
The authors wish to acknowledge the board of the Society of Integrative Oncology for collaboration in developing the survey questions. We would also like to thank Jodi MacLeod, SIO secretary, for her assistance and persistence in tracking down the raw data when it was needed.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Susan Veleber is an employee of Fred Hutchinson Cancer Center. Jonathan Siman is an employee of Fred Hutchinson Cancer Center. Matthew Weizman is an employee of Memorial Sloan Kettering. Misha Cohen is the owner of Chicken Soup Chinese Medicine. Yair Maimon is the owner of Refuot Integrative Medical Center. Christine Adamo is a contracted provider for cCARE. Jennifer Stone, Weidong Lu and Tammy Sajdyk have no conflicts to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.