
Abstract
Objective. The aim of this study is to evaluate the efficacy and safety of acupuncture for radioactive iodine (RAI)–induced anorexia in thyroid cancer patients. Methods. Fourteen thyroid cancer patients with RAI-induced anorexia were randomized to a true acupuncture or sham acupuncture group. Both groups were given 6 true or sham acupuncture treatments in 2 weeks. Outcome measures included the change of the Functional Assessment of Anorexia and Cachexia Treatment (FAACT; Anorexia/Cachexia Subscale [ACS], Functional Assessment of Cancer Therapy–General [FACT-G]), Visual Analogue Scale (VAS), weight, body mass index (BMI), ACTH, and cortisol levels. Results. The mean FAACT ACS scores of the true and sham acupuncture groups increased from baseline to exit in intention-to-treat (ITT) and per protocol (PP) analyses; the true acupuncture group showed higher increase but with no statistical significance. Between groups, from baseline to the last treatment, statistically significant differences were found in ITT analysis of the Table of Index (TOI) score (P = .034) and in PP analysis of the TOI (P = .016), FACT-G (P = .045), FAACT (P = .037) scores. There was no significant difference in VAS, weight, BMI, ACTH, and cortisol level changes between groups. Conclusion. Although the current study is based on a small sample of participants, our findings support the safety and potential use of acupuncture for RAI-induced anorexia and quality of life in thyroid cancer patients.
Introduction
Cancer patients suffer from a variety of treatment-related side effects while going through a debilitating treatment process to eliminate cancer. With today’s improvement in cancer therapies and prolonged survival, more patients are experiencing complications leading to poor quality of life.1,2 Anorexia, defined as loss of appetite, is one of the most common problems for cancer patients, impairing their quality of life (QOL) and delaying the recovery process.3-5
During radioactive iodine (RAI) treatment of thyroid cancer patients, radioiodine is taken up and concentrated in thyroid follicular cells via membrane sodium-iodine transporter. Although the sodium-iodine transporter is mainly found in the thyroid tissue, it can also be found in several other tissues (stomach, salivary glands, lactating breasts, thymus, nasal mucosa, lacrimal glands, placenta), and the traveling radioiodine can cause damages to these sites.6-8 Of the RAI-related side effects in differentiated thyroid cancer patients, gastrointestinal complaints including appetite loss, nausea, and vomiting are reported to be highest in incidence. 9
Recently, trends of incorporating acupuncture in clinical settings of major cancer centers to manage cancer-associated symptoms and conditions are on the rise. 10 Clinical research to scientifically support acupuncture is being conducted with many studies showing preliminary positive outcomes.11,12 However, no attempt has been made yet to study the effect of acupuncture for RAI-induced anorexia in thyroid cancer patients.
The objective of this study was to evaluate the effect and safety of acupuncture for RAI-induced anorexia in thyroid cancer patients by comparing the true acupuncture to sham acupuncture using the Functional Assessment of Anorexia and Cachexia Treatment (FAACT; Anorexia/Cachexia Subscale [ACS], Functional Assessment of Cancer Therapy–General [FACT-G]), Visual Analogue Scale (VAS), weight, body mass index (BMI), ACTH, and cortisol values.
Methods
Participants
The patients were recruited through recruitment posters placed inside of the Dunsan Korean Medicine Hospital of Daejeon University from August 2013 to February 2014. Eligibility criteria were 20 to 65 years of age, thyroid cancer patients suffering from RAI-induced anorexia who had received the RAI therapy 10 to 60 days before, VAS for anorexia score >4, and people who are literate and have ability to understand and sign the informed consent. Exclusion criteria were impossible oral intake; mental diseases such as dementia, delirium, depression, and so on; people who have cancer-related pain that can directly affect appetite or calorie intake within the 2 weeks of clinical study screening; other diseases that can influence appetite (eg, hypoadrenalism); people who are on appetite stimulants (eg, megestrol acetate, corticosteroids, thalidomide); Eastern Cooperative Oncology Group (ECOG) performance status >2; pregnancy; and others who have difficulty participating in the treatment and data collecting procedure. Informed consent was obtained from all patients before enrollment, and the study protocol was approved by the Institutional Review Board at Dunsan Korean Medicine Hospital of Daejeon University (protocol registered on www.cris.nih.go.kr, KCT0000949: https://cris.nih.go.kr/cris/en/search/search_result_st01.jsp?seq=3276).
Randomization and Blinding
Random numbers for the allocation sequence were generated by computer (using SPSS 21 statistical software package). A computer program (The Biased Coin Method) that allows the patients to be assigned to either the true acupuncture group or the sham acupuncture group in a 1:1 ratio was used. The random numbers were then sealed in opaque envelopes. Both the patients and acupuncturist were blinded to the treatment allocation as the true or sham needles were handed out by a nursing assistant at the beginning of each treatment.
Intervention
Three treatment sessions were given each week for 2 weeks by a single experienced acupuncturist (total 6 treatments). The frequency and treatment time of acupuncture varies according to subjects for study or diseases,13,14 but there are reports that when performing therapeutic acupuncture for symptom relief, mostly manual acupuncture is used and the effects are induced slowly and recognized after a course of perhaps 4 to 8 treatments. 15 At least 2 treatments in a week are required in clinical acupuncture trials. 16
For true acupuncture, intradermal type T needles (thickness 0.2 mm, length [depth] 1.5 mm, diameter 2 mm; Dongbang Inc, South Korea) were administered bilaterally into 5 acupuncture points (LI4, LR3, ST36, SP6, KI2). The acupuncture points were chosen based on the Textbook of Korean Society of Acupuncture. 17 For sham, we used Kim’s sham acupuncture needles, 18 which have the same structure, color, and shape of the intradermal type T needles with the exception of the blunt tip. The blunt tip makes it impossible to penetrate the skin but gives the similar tactile sensation to that of the real T-shaped intradermal needle. No manipulations of the needles were conducted to acquire “de qi” sensation in both groups. The needles were left in for 30 minutes considering more than 15 to 20 minutes of needle placing time are required in clinical acupuncture trials. 16
Outcome Measures
The patients were asked to complete the FAACT questionnaire (version 4). 19 The FAACT questionnaire was designed to complement FACT-G by addressing the anorexia/cachexia-related concerns. The FACT-G is a validated 27-item, patient-rated measure of QOL for cancer patients of any type. It covers the areas of Physical Well-Being (7 items), Social/Family Well-Being (7 items), Emotional Well-Being (6 items), and Functional Well-Being (7 items). In addition to the FACT-G items, the FAACT has additional 12 items under the ACS category. All FAACT items score from 0 = not at all to 4 = very much, and the total score ranges from 0 to 156. Higher scores imply a better state of the patient. The VAS anorexia scale, 20 which ranges from 0 = normal appetite to 10 = no food intake possible, was also used. Weight and BMI were measured using “Inbody” body composition device (biospace, Cheonan, South Korea). The FAACT, VAS, weight, and BMI data were collected before the initial treatment, after the first and second weeks of treatment (visits 4 and 7), and at follow-up 2 weeks after the last treatment (visit 8).
ACTH and cortisol values were followed as an outcome measure to check the correlation with the other measures. To reduce time difference value, the participants’ blood samples were obtained after completing their second week of treatment (visit 7; Table 1).
Schedule for Treatment and Outcome Measurement.

Abbreviations: VAS, Visual Analogue Scale; FAACT, Functional Assessment of Anorexia and Cachexia Treatment; BMI, body mass index.
Safety
The majority of acupuncture-related adverse events reported are generally minor and limited to local symptoms such as pain or bruising at the needling site. However, a 2013 systematic review of the case reports points out that serious adverse events associated with acupuncture are rare, but it is not without risk. 21 All patients were checked for any acupuncture-related and unrelated adverse events before, during, and after treatment by the practitioner by monitoring the acupoints used and asking about any after-treatment discomfort symptoms.
Statistical Analysis
We conducted the analysis using the SPSS statistical package program (ver. 21). Data analysis of baseline characteristics was based on the intention-to-treat (ITT) population, which included all participants who were randomized. Primary and secondary outcomes were mainly based on the data of the ITT population and also analyzed based on per-protocol (PP) population as an extra supportive analysis. Data analysis of safety was based on the ITT population. Baseline characteristics are presented as mean ± standard deviation (SD) for continuous data including the FAACT, VAS, weight, BMI, ACTH, and cortisol values. Normality of the data was tested using the Shapiro–Wilk test. Comparing the true and sham acupuncture groups, Mann–Whitney U test was used at baseline for continuous data and to compare the mean differences from baseline to the end of treatment for primary and secondary outcomes. We were concerned about small sample sizes, so we had to consider the results of nonparametric tests together with the conventional Student’s t test. The level of significance was set at .05.
Results
Participants
There were 13 female patients and 1 male patient. Demographic information and baseline characteristics of the 14 patients are shown in Table 2. No statistically significant differences were found between the 2 groups in age, weight, BMI, and baseline values. Of the 14 participants, 2 patients dropped out, one from each group, and 12 completed the treatment. The reason for dropping out was traveling difficulties for both patients.
Demographic Information and Baseline Characteristics. a
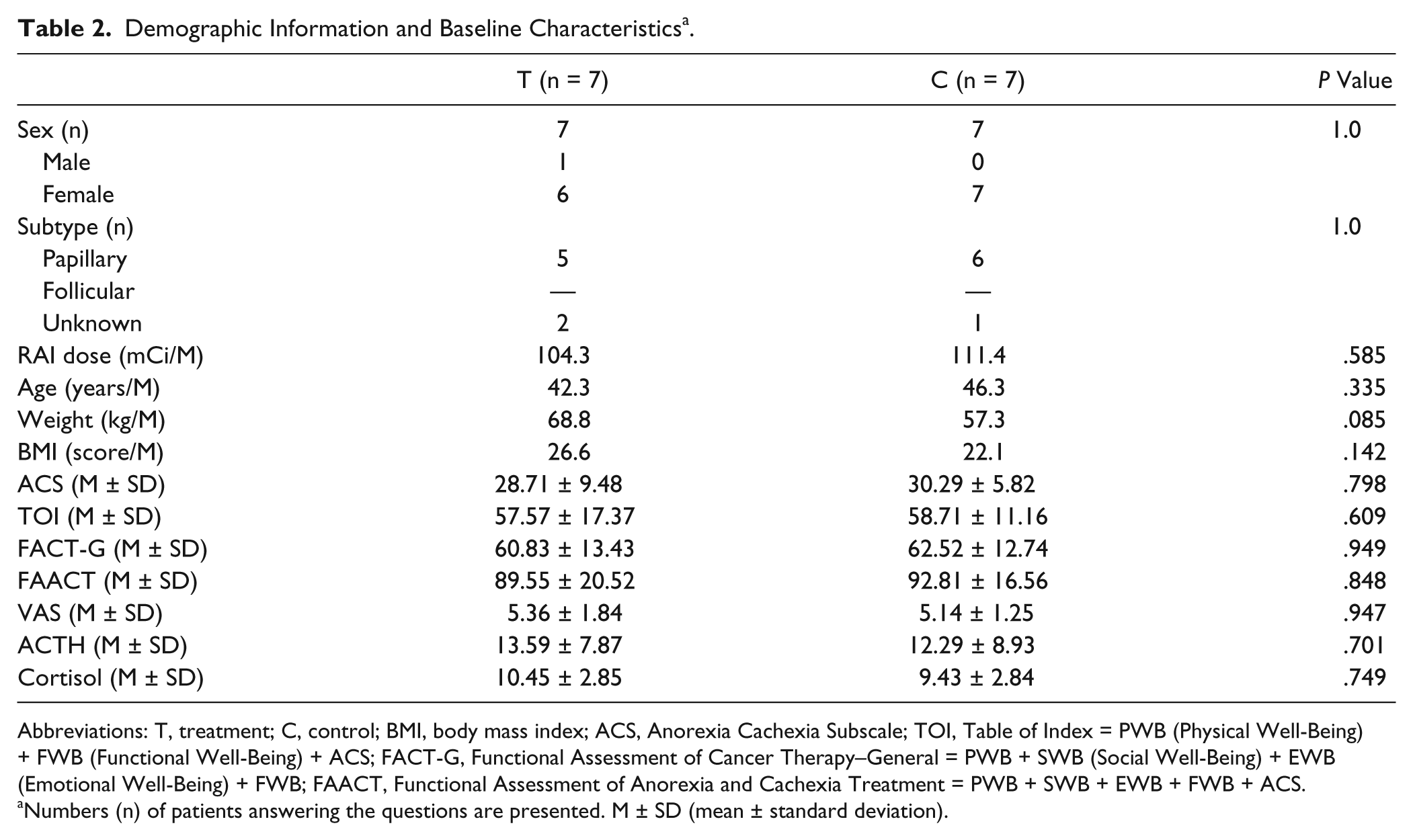
Abbreviations: T, treatment; C, control; BMI, body mass index; ACS, Anorexia Cachexia Subscale; TOI, Table of Index = PWB (Physical Well-Being) + FWB (Functional Well-Being) + ACS; FACT-G, Functional Assessment of Cancer Therapy–General = PWB + SWB (Social Well-Being) + EWB (Emotional Well-Being) + FWB; FAACT, Functional Assessment of Anorexia and Cachexia Treatment = PWB + SWB + EWB + FWB + ACS.
Numbers (n) of patients answering the questions are presented. M ± SD (mean ± standard deviation).
Anorexia Cachexia Subscale
The mean ACS score increased with treatment in both true and sham groups. In the true acupuncture group, the ACS score was most increased after the first week of treatment (after 3 treatments) and it stayed increased until the final visit. In the sham group, the ACS score did not show much change until the end of all 6 acupuncture sessions but went up after the 2 weeks of follow-up period. The increase of the ACS score in the true acupuncture group from baseline to exit was greater than that of the sham group, but the differences had no statistical significance in ITT and PP analyses (Tables 3 and 4).
Analysis of ACS Outcome in ITT and PP. a

Abbreviations: ACS, Anorexia Cachexia Subscale; ITT, intention to treat; PP, per protocol; T, treatment; C, control.
Numbers (n) of patients answering the questions are presented. M ± SD (mean ± standard deviation).
Analysis of ACS Outcome Changes in ITT and PP. a

Abbreviations: ACS, Anorexia Cachexia Subscale; ITT, intention to treat; PP, per protocol; T, treatment; C, control; t, Student’s t; P, P value from Student’s t test; P (M-W), P value from Mann–Whitney test.
Numbers (n) of patients answering the questions are presented. M ± SD (mean ± standard deviation).
FACT-G, FAACT, and TOI
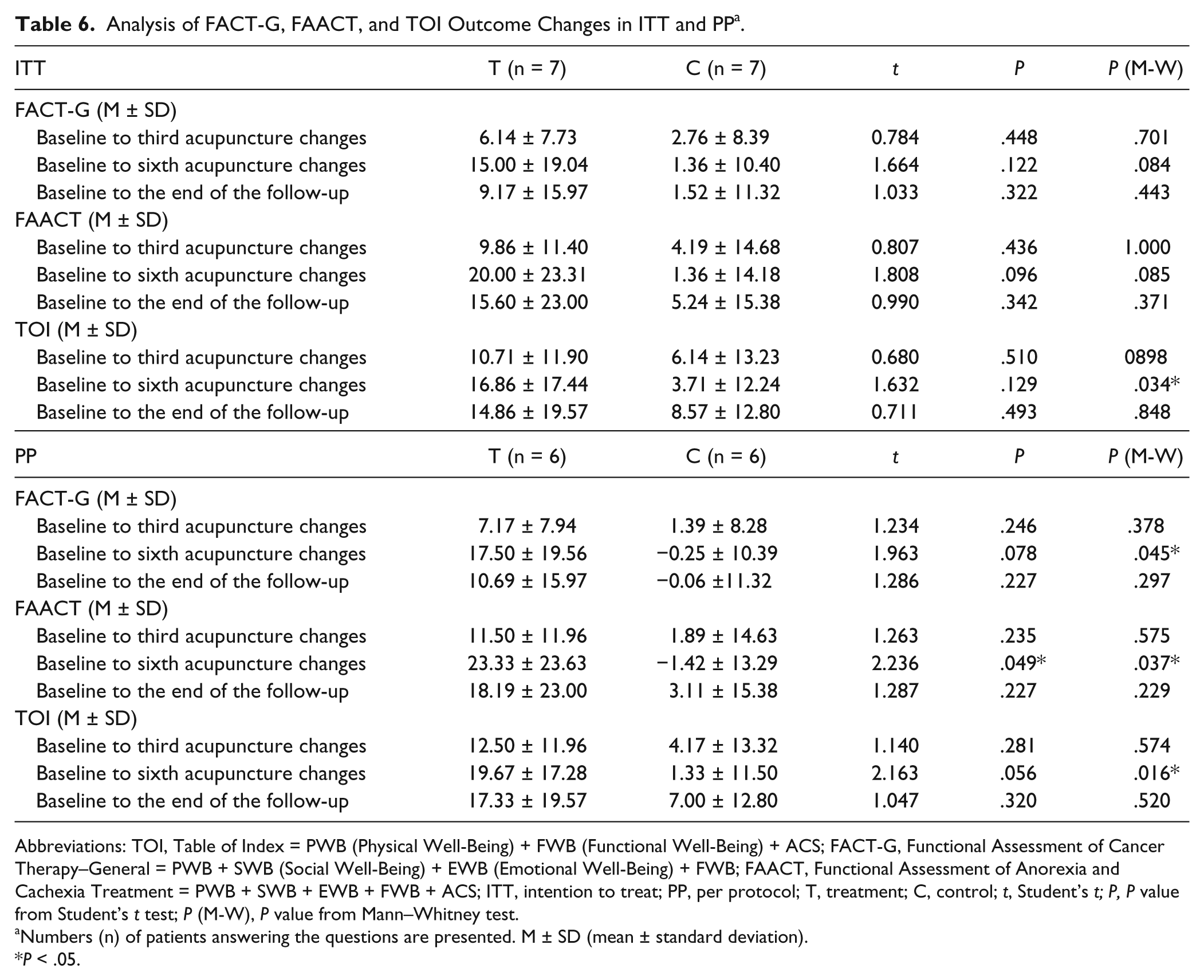
The mean FACT-G score indicating QOL of the patients increased in both groups using ITT analysis, but only the QOL of true acupuncture group increased in PP analysis. In ITT analysis, the mean increase of the true acupuncture group was greater than that of the sham group (T: 9.17 ± 15.97; C: 1.52 ± 11.32) from baseline to exit. The increase was gradual with a small drop following the last visit. A statistical significance was found in the difference of FACT-G changes between baseline and after sixth acupuncture treatment in PP analysis (P = .045).
The mean FAACT score changes correlated with the ACS and the FACT-G results, as the FAACT score is the sum of the FACT-G and ACS scores. The true acupuncture group has shown higher increase from baseline to exit in both ITT (T: 15.60 ± 23.00; C: 5.24 ± 15.38) and PP analyses (T: 18.19 ± 23.00; C: 3.11 ± 15.38). A statistical significance was found in the difference of FAACT changes between baseline and after sixth acupuncture treatment in PP analysis (P = .037).
The Table of Index (TOI) score indicates physical/functional outcomes. It is calculated by adding up PWB, FWB, and ACS scores. Again, the TOI score increase was higher in the true acupuncture group in both analyses. In the PP analysis, the difference in TOI score changes from baseline to exit between groups (T: 17.33 ± 19.57; C: 7.00 ± 12.80) was higher than that of the ITT analysis (T: 14.86 ± 19.57; C: 8.57 ± 12.80). A statistical significance was found in the difference of TOI changes between baseline and after sixth acupuncture treatment in ITT and PP analyses (P = .034, P = .016; Tables 5 and 6).
Analysis of FACT-G, FAACT, and TOI Outcome Changes in ITT and PP. a

Abbreviations: ITT, intention to treat; PP, per protocol; T, treatment; C, control; TOI, Table of Index = PWB (Physical Well-Being) + FWB (Functional Well-Being) + ACS; FACT-G, Functional Assessment of Cancer Therapy–General = PWB + SWB (Social Well-Being) + EWB (Emotional Well-Being) + FWB; FAACT, Functional Assessment of Anorexia and Cachexia Treatment = PWB + SWB + EWB + FWB + ACS.
Numbers (n) of patients answering the questions are presented. M ± SD (mean ± standard deviation).
Analysis of FACT-G, FAACT, and TOI Outcome Changes in ITT and PP. a
Abbreviations: TOI, Table of Index = PWB (Physical Well-Being) + FWB (Functional Well-Being) + ACS; FACT-G, Functional Assessment of Cancer Therapy–General = PWB + SWB (Social Well-Being) + EWB (Emotional Well-Being) + FWB; FAACT, Functional Assessment of Anorexia and Cachexia Treatment = PWB + SWB + EWB + FWB + ACS; ITT, intention to treat; PP, per protocol; T, treatment; C, control; t, Student’s t; P, P value from Student’s t test; P (M-W), P value from Mann–Whitney test.
Numbers (n) of patients answering the questions are presented. M ± SD (mean ± standard deviation).
P < .05.
VAS, Weight, BMI, ACTH, Cortisol Results
The mean VAS score decreased in both groups. In the true acupuncture group, continuous decrease was observed with treatment over time, while in the sham group the decrease was seen only after the first week of treatment and remained unchanged throughout. The VAS score decrease was greater in the true acupuncture group in both analyses, but had no statistical significance.
The mean weight and BMI were slightly increased in the true acupuncture group and slightly decreased in the sham group. However, the weight and BMI changes were minimal and had no statistical significance. The ACTH and cortisol values did not correlate with other measures and had no statistical significance (Tables 7 and 8)
Analysis of VAS, Weight, BMI, ACTH, and Cortisol Outcomes in ITT and PP. a

Abbreviations: VAS, Visual analogue Scale; BMI, body mass index; ACTH, adrenocorticotropic hormone; ITT, intention to treat; PP, per protocol; T, treatment; C, control.
Numbers (n) of patients answering the questions are presented. M ± SD (mean ± standard deviation).
Analysis of VAS, Weight, BMI, ACTH, and Cortisol Outcomes in ITT and PP. a

Abbreviations: VAS, Visual Analogue Scale; BMI, body mass index; ACTH, adrenocorticotropic hormone; ITT, intention to treat; PP, per protocol; T, treatment; C, control; t, Student’s t; P, P value from Student’s t test; P (M-W), P value from Mann–Whitney test.
Numbers (n) of patients answering the questions are presented. M ± SD (mean ± standard deviation.
Safety
No acupuncture-related adverse events were reported before, during, or after each treatment session. For unrelated adverse events, a patient had a cold and indigestion, but recovered within a few days.
Discussion
In this study, we found that true acupuncture and sham acupuncture both showed effectiveness in improving the QOL of RAI-induced anorexia in thyroid cancer patients. The ACS score of the true group steadily increased from baseline to the completion of treatment and was maintained till 2 weeks later. The underlying mechanism of acupuncture in treatment of anorexia is not clear. Studies claim acupuncture can activate both the peripheral and central nervous systems, resulting in secretion of neurotransmitters and neurohormones including endorphins, monoamines, serotonin, and encephalin that can normalize the body’s neuroendocrine function. 16 Some studies had shown that acupuncture stimulation in the extremities facilitates gastric motility through a somato-parasympathetic reflex involving the vagal nerve.22,23 The regulating effect of acupuncture may at least be partially explained by these actions. Other studies of acupoint stimulation (electroacupuncture and acupressure) for chemotherapy-induced nausea and vomiting 24 and acupuncture (both real and sham) for radiotherapy-induced nausea 14 have shown positive outcomes in improving the symptoms, and there was one study on RAI-induced anorexia in thyroid cancer patients using acupressure, which also reported positive outcome. 25
Of the 4 FACT-G subcategories (Physical, Social/Family, Emotional, Functional Well-Being), patients reported the symptoms of the physical well-being category to be most improved after the completion of treatment in both groups, and the improved feeling continued through their final visit 2 weeks after. Also, the difference in mean increase of the physical well-being category from baseline to exit in PP analysis (T: 8.17 ± 10.52; C: 5.17 ± 4.83) was notably greater than that of the ITT analysis (T: 7.00 ± 10.52; C: 6.00 ± 4.83). Little change was found in the social/family, emotional, and functional well-being categories, which did not fully replicate the previous findings of acupuncture having effect on the physical/cognitive and psycho-emotional components of the eating disorder related QOL with more influence on the later. 26 In our study, the improvement of RAI-induced anorexia related QOL was mostly through the practical physical changes produced by acupuncture.
From baseline to the completion of treatment (from visits 1 to 7), score changes in TOI was found to be statistically significant in the ITT analysis of all 14 participants, and the TOI, FACT-G, and FAACT score changes had statistical significance in the PP analysis of the 12 participants who completed the study. Though both analyses demonstrated similar results, the PP analysis with the selected population is more relevant to demonstrate the unaltered effect of intervention in a small sample study like this, especially because the patients who dropped out were not due to any adverse events caused by acupuncture but commuting difficulties.
Ghrelin, the hunger hormone that signals hunger to the brain, is reported to stimulate ACTH and cortisol secretion. 27 This link between appetite and ACTH and cortisol levels is well known. In a study, a direct association between cortisol levels and calorie intake in populations of women was demonstrated. 28 Cortisol can directly influence appetite and cravings by binding to hypothalamus receptors in the brain, or it can also indirectly influence appetite by modulating other hormones and stress responsive factors known to stimulate appetite. The reported ability of acupuncture to stimulate ACTH and cortisol secretion 14 did not reflect in our study, and we found the changes in ACTH and cortisol values to be insignificant and uncorrelated to the other outcome measures. It may have been that the dose of cortisol released was too small to have any effect, or the acupuncture treatment works differently from ghrelin’s mechanism of enhancing appetite.
In this research, we used Kim’s sham acupuncture in order to carry out a successful double-blinded study. 29 In a previous study of Kim’s sham needle, neither subjects nor acupuncturists could visually distinguish the sham needle from the real needle. 30 The downside of using Kim’s sham needles (T-shaped intradermal needles) was the small stimulus-quantity and difficulty in acquiring “de qi” sensation due to its shallow depth of insertion. In acupuncture, penetration is suggested to be the main mechanism producing effects from acupuncture, for example, by generating a release of spinal and supraspinal beta-endorphins, proinflammatory neuropeptides, and increasing peripheral circulation. 31 Another point to consider is the possible therapeutic effect of the sham needle. Kim’s sham device has a blunt tip that is pressed against the surface of the skin, which may elicit an acupressure-like effect. Lund et al 32 noted that the light touch of the skin was substantial enough to stimulate activity in C tactile afferents, which can result in emotional and hormonal reactions. This could explain why the supposedly inert control interventions are equally effective as the true acupuncture. This finding is in agreement with the findings of Moffet 33 and Lundeberg et al, 34 which suggested sham acupuncture to be as efficacious as true acupuncture, and since the sham acupuncture evidently is merely another form of acupuncture from the physiological perspective, the assumption that sham is sham is incorrect and conclusions based on this assumption are therefore invalid. Thus, these limitations of Kim’s sham needles could have played a role in achieving beneficial effects in both groups.
Limitations
A limitation of this study was the relatively small sample size. These findings cannot be generalized to the broader community based on this study alone. Another limitation was the number of treatments given and short treatment period altogether. In the future studies, larger sample size and greater numbers of treatment should be implemented. Choosing acupuncture points for RAI-induced anorexia can differ depending on the practitioner and more discussion for the ideal acupuncture point selection is also encouraged. Moreover, it would be nice to have a no treatment control group as well in order to rule out the possibility of natural recovery.
Other Benefits
Interestingly, 4 people, 3 from the true acupuncture group and 1 from the sham group, reported having improved sleep quality after being treated with acupuncture. This positive relation between sleep and acupuncture is consistent with preceding acupuncture studies on insomnia and reports on better-quality sleep while receiving acupuncture for radiotherapy-induced nausea 14 and during chemotherapy. 35 It would be of interest to further evaluate acupuncture’s underlying mechanism for insomnia and its efficacy for other types of sleep disorders as well.
Conclusion
Although the current study is based on a small sample of participants, the findings support the safety and potential use of acupuncture for RAI-induced anorexia and QOL mainly concerning the physical well-being symptoms in thyroid cancer patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grant of Korea of Health & Welfare, Republic of Korea (Project No.: CIMI-13-01-08).