
Abstract
Objective
To analyse the clinical characteristics of extra-thyroid 99mTc-pertechnetate uptake in order to explore the effect of the phenomenon on radioactive iodine (RAI) therapy for differentiated thyroid carcinoma (DTC) and its clinical significance.
Methods
This study retrospectively selected patients with DTC and extra-thyroid 99mTc-pertechnetate uptake. The clinical features, location, location count and extra-thyroid 99mTc-pertechnetate uptake distribution were analysed, combined with the uptake rate, stimulated thyroglobulin (sTg) level, post-therapy whole-body scan and curative effect.
Results
A total of 38 patients were enrolled in the study and 65 extra-thyroid 99mTc-pertechnetate foci were detected. Thirty-four patients showed abnormal 99mTc-pertechnetate uptake in the lymph nodes (26 of 38; 68.4%), lungs (four of 38; 10.5%) and bones (four of 38; 10.5%). The corresponding uptake rates were 0.2%, 0.2% and 0.8%, respectively. The uptake rate and sTg were significantly positively correlated (r = 0.36). 131I uptake was found in 36 patients at the 99mTc-pertechnetate uptake site. The number of iodine uptake foci was significantly higher than that of 99mTc-pertechnetate uptake foci. The sTg value and pathological staging significantly differed between the excellent and nonexcellent response groups (Z = –2.947 and Z = –2.348, respectively).
Conclusion
Extra-thyroid 99mTc-pertechnetate uptake mostly indicated metastases with specific clinical features, which may have prognostic value for the judgment of iodine uptake function and the RAI therapy plan.
Introduction
Differentiated thyroid carcinoma (DTC) is the most common malignant tumour of the head and neck that is formed from thyroid follicular cells; 1 and it includes papillary carcinoma, follicular carcinoma, Hürthle cell carcinoma and poorly differentiated carcinoma. 2 DTC accounts for more than 90% of thyroid cancers overall. 1 According to the 2015 American Thyroid Association (ATA) guidelines, radioactive iodine (RAI) therapy is recommended for all high-risk and selective intermediate-risk patients with DTC. 3 99mTc-pertechnetate has long been used in clinical practice as an imaging agent for evaluating thyroid diseases; and it is cheap, widely available, has ideal imaging characteristics and favourable dosimetry. 4 99mTc-pertechnetate scanning is commonly used to detect any thyroid remnants following thyroidectomy and it may provide beneficial data on the extent of remnant tissue without the need for 131I or 123I. 5 The 99mTc-pertechnetate uptake of the thyroid bed can be used as a marker of thyroid remnants, but a lack of uptake does not indicate the absence of thyroid remnants, it just suggests a small volume of remnants. 6 Over the last few decades, extra-thyroid 99mTc-pertechnetate uptake has rarely been reported.7,8 Furthermore, almost all available literature includes case reports,9–14 most of which confirmed DTC metastases.
The present study retrospectively analysed the clinical characteristics of extra-thyroid 99mTc-pertechnetate uptake in order to explore the effect of the phenomenon on RAI therapy for DTC and its clinical significance.
Materials and methods
Study population
This study retrospectively screened consecutive patients with DTC that underwent total/near-total thyroidectomy with central and/or lateral cervical lymph node dissection, and then received the initial RAI therapy following 99mTc-pertechnetate scanning at the Department of Nuclear Medicine, The Cancer Hospital of the University of Chinese Academy of Sciences (Zhejiang Cancer Hospital), Institute of Basic Medicine and Cancer (IBMC), Chinese Academy of Sciences, Hangzhou, Zhejiang Province, China between January 2007 and January 2017. According to the location of extra-thyroid 99mTc-pertechnetate uptake, a subgroup of these patients was included in this study. All patients met the following inclusion criteria: (i) they had undergone total/near-total thyroidectomy and had a postoperative pathology test that indicated DTC; (ii) they had thyrotropin (TSH), stimulated thyroglobulin (sTg) and Tg autoantibodies (TgAbs) measurements after being on a low-iodine diet and thyroid hormone withdrawal (THW) for 3–4 weeks; (iii) they had 99mTc-pertechnetate scanning with additional single-photon emission computed tomography/computed tomography (SPECT/CT) following THW, which revealed at least one region of extra-thyroid 99mTc-pertechnetate uptake; (iv) they had no history of a second primary tumour; (v) they provided signed informed consent before RAI therapy.
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Cancer Hospital of the University of Chinese Academy of Sciences (no. HYX20200423; 23 April 2020). All patients provided written informed consent.
Imaging protocol and image analyses
Thirty minutes after intravenous administration of approximately 185 MBq of 99mTc-pertechnetate, anterior images of the neck were acquired using a gamma-camera equipped with low-energy and high-resolution collimators (Discovery NM/CT670; GE Healthcare, Piscataway, NJ, USA), with a 20% window centred around the 140 KeV peak and a 256 × 256 computer matrix. The radioactivity counts of full and empty needles were performed before and after injection, and the 99mTc-pertechnetate uptake rate was determined using the region-of-interest technique as previously described. 15 The uptake rate (%) = (counts over remnant thyroid tissue or extra-thyroid focus – background counts)/counts of injected activity × 100%. 16 99mTc-pertechnetate whole-body scanning (99mTc-WBS) was performed after obtaining anterior images in the continuous mode with a scanning speed of 15 cm/min. Additional SPECT/CT was performed depending on the 99mTc-WBS findings with dual-detector 180° acquisition, angular step of 3°and 15′′ per step/view. The CT acquisition was performed with a 16-slice elicoidal, 140kV and 2.5mA. The post-treatment whole-body scan (Rx-WBS) and SPECT/CT were conducted 5 days after the administration of 131I with the same technique except that the energy window was 364KeV with high-energy collimators.
The results of 99mTc-WBS combined with SPECT/CT were analysed separately by two experienced nuclear medicine physicians (L.F.Y. & S.C.C.) that were unaware of the Rx-WBS/SPECT/CT results. A clearly visible focus of 99mTc-pertechnetate uptake above the background level outside the thyroid bed was defined as extra-thyroid 99mTc-pertechnetate uptake. Unidentifiable thyroid residue or suspected metastatic lesions with anatomical findings from CT were excluded.
Follow‑up and response assessment
A regular follow-up was performed after the initial RAI therapy and the follow-up duration was 12–108 months. The response was classified as excellent response (ER), biochemical incomplete response (BIR), structural incomplete response (SIR) and indeterminate response (IDR), according to the 2015 ATA guidelines. 3 The latter three are collectively referred to as non-excellent response (NER).
Statistical analyses
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 26.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics are shown as mean ± SD for continuous variables and as the number of patients (%) for categorical variables. The 99mTc-pertechnetate uptake rates were evaluated using the Kruskal–Wallis test. Spearman’s rho was used to analyse the correlation between 99mTc-pertechnetate uptake and other parameters. The correlation parameters between the ER and NER groups were compared using the Mann–Whitney U-test. A P-value < 0.05 was considered statistically significant.
Results
This retrospective study screened 4930 patients with DTC. Out of these patients, 38 (15 males and 23 females) patients were included in this study. The baseline demographic, clinical and pathological data are summarized in Table 1. The TSH level in eight patients was < 30 mIU/l after 4 weeks of THW and there were only a small number of thyroid residuals. Among the 38 patients with DTC, 35 (92%) had an sTg level > 10 ng/ml during the first 131I treatment.
Demographic, clinical and pathological characteristics of patients with differentiated thyroid carcinoma (n = 38) that were included in a retrospective study of the clinical characteristics of extra-thyroid 99mTc-pertechnetate uptake.

Data presented as n of patients (%).
aRefers to papillary carcinoma and follicular carcinoma in the different lobes of the thyroid.
AJCC, American Joint Committee on Cancer; TSH, thyrotropin (TSH); sTg, stimulated thyroglobulin; TgAbs, thyroglobulin autoantibodies.
A total of 65 extra-thyroid 99mTc-pertechnetate uptake foci were detected in 38 patients. The distribution characteristics are summarized in Table 2. In the per-patient analysis, 34 showed abnormal 99mTc-pertechnetate uptake in the lymph nodes (26 of 38; 68.4%), lungs (four of 38; 10.5%) and bones (four of 38; 10.5%); and the corresponding uptake rates were 0.2% (0.1%–0.35%), 0.2% (0.1%–0.68%) and 0.8% (0.45%–1.6%), respectively. Data on the relationship between the three subgroups showed that the uptake rate in the lymph node subgroup was significantly lower than that in the bone subgroup (Z = 2.722, P = 0.019) (Figure 1). Seven patients showed extra-thyroid 99mTc-pertechnetate uptake in two or more sites (Figure 2). One patient with superior vena cava 99mTc-pertechnetate uptake underwent chest magnetic resonance imaging (MRI) scanning before 131I therapy and this showed that the superior vena cava was significantly enlarged, with an abnormal mass in the blood vessels, high signal on T2-weighted images, enhanced scan lesions significantly enhanced and 131I uptake in this area, which was considered to be a tumour thrombus. Another patient showed 99mTc-pertechnetate uptake in the supraclavicular vessel, but no abnormality was found on ultrasound, MRI or Rx-WBS/SPECT/CT. Correlation analyses between the extra-thyroid 99mTc-pertechnetate uptake rate and sex, age, sTg, TgAb and TSH levels, pathological type and TNM stage showed a significant positive correlation between the sTg level and the 99mTc-pertechnetate uptake rate (r = 0.36, P = 0.027) (Figure 3).
Distribution of 65 extra-thyroid 99mTc-pertechnetate uptake lesions in patients with differentiated thyroid carcinoma (n = 38) that were included in a retrospective study of the clinical characteristics of extra-thyroid 99mTc-pertechnetate uptake.


Comparison of the extra-thyroid 99mTc‑pertechnetate uptake rates of patients with differentiated thyroid carcinoma (n = 38) that were included in a retrospective study of the clinical characteristics of extra-thyroid 99mTc-pertechnetate uptake. Data on the relationship among the three subgroups showed that the 99mTc pertechnetate uptake rate in the lymph node subgroup was significantly lower than that in the bone subgroup (Z = 2.722, P = 0.019; Kruskal–Wallis test). Central black horizontal lines for each organ subgroup are the medians, the extremities of the box are the 25th and 75th percentiles, and the error bars represent the minimum and maximum values.
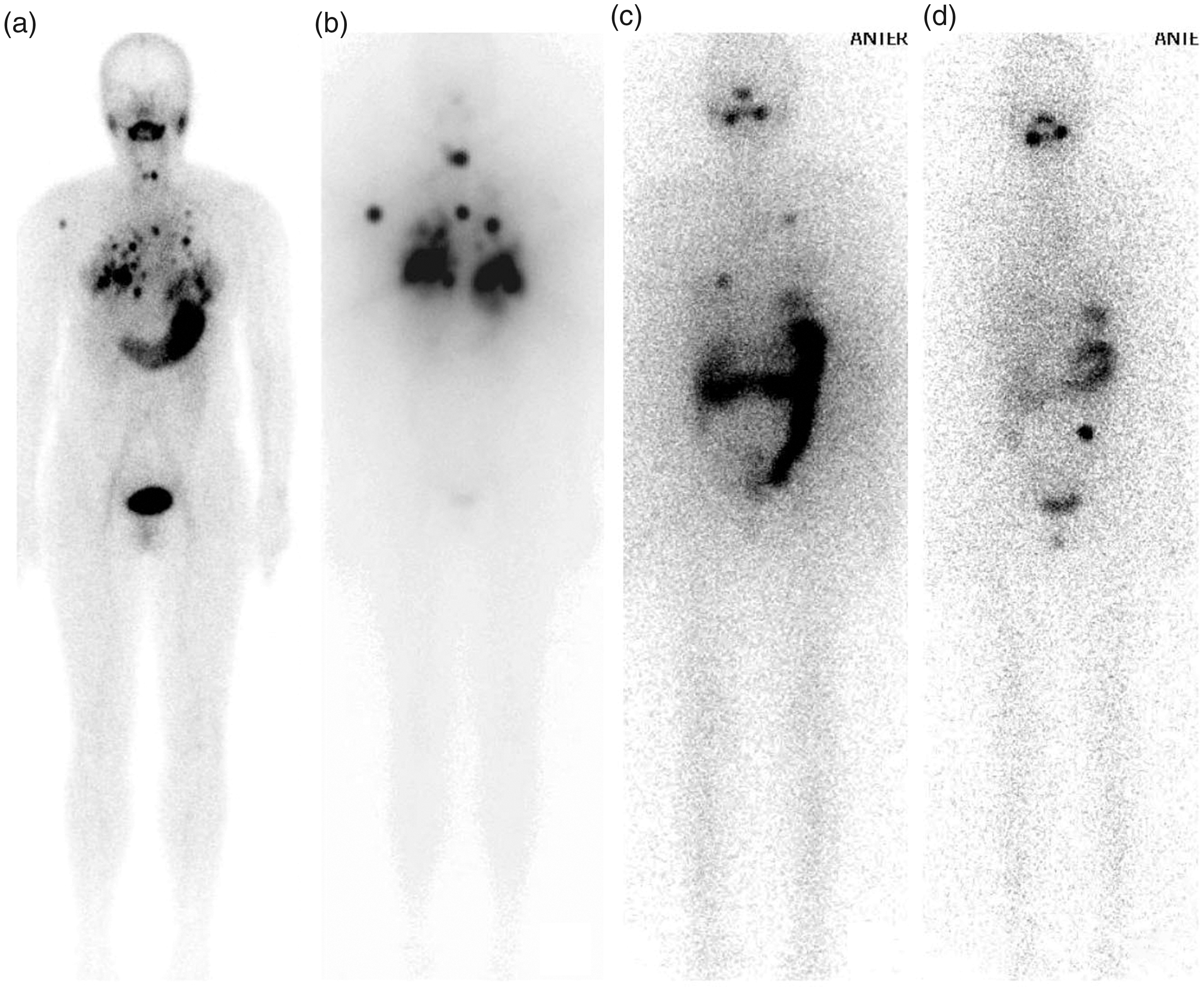
A representative patient with differentiated thyroid carcinoma showing that the pulmonary and anterior mediastinal lymph node metastases receded after three cycles of treatment with radioactive iodine (RAI). (A) A 99mTc pertechnetate whole-body scan (WBS) showed multiple radioactive nodules on both sides of the chest and mediastinum before the initial RAI treatment. (B) An 131I whole-body scan (Rx-WBS) showed almost the same metastatic lesions as the Tc-99m pertechnetate WBS after the first cycle of RAI therapy. (C) An Rx-WBS showed decreased uptake in the metastases after the second cycle of RAI therapy in comparison with (B). (D) An Rx-WBS after the third cycle of RAI therapy, which indicated complete remission of the multiple metastases.
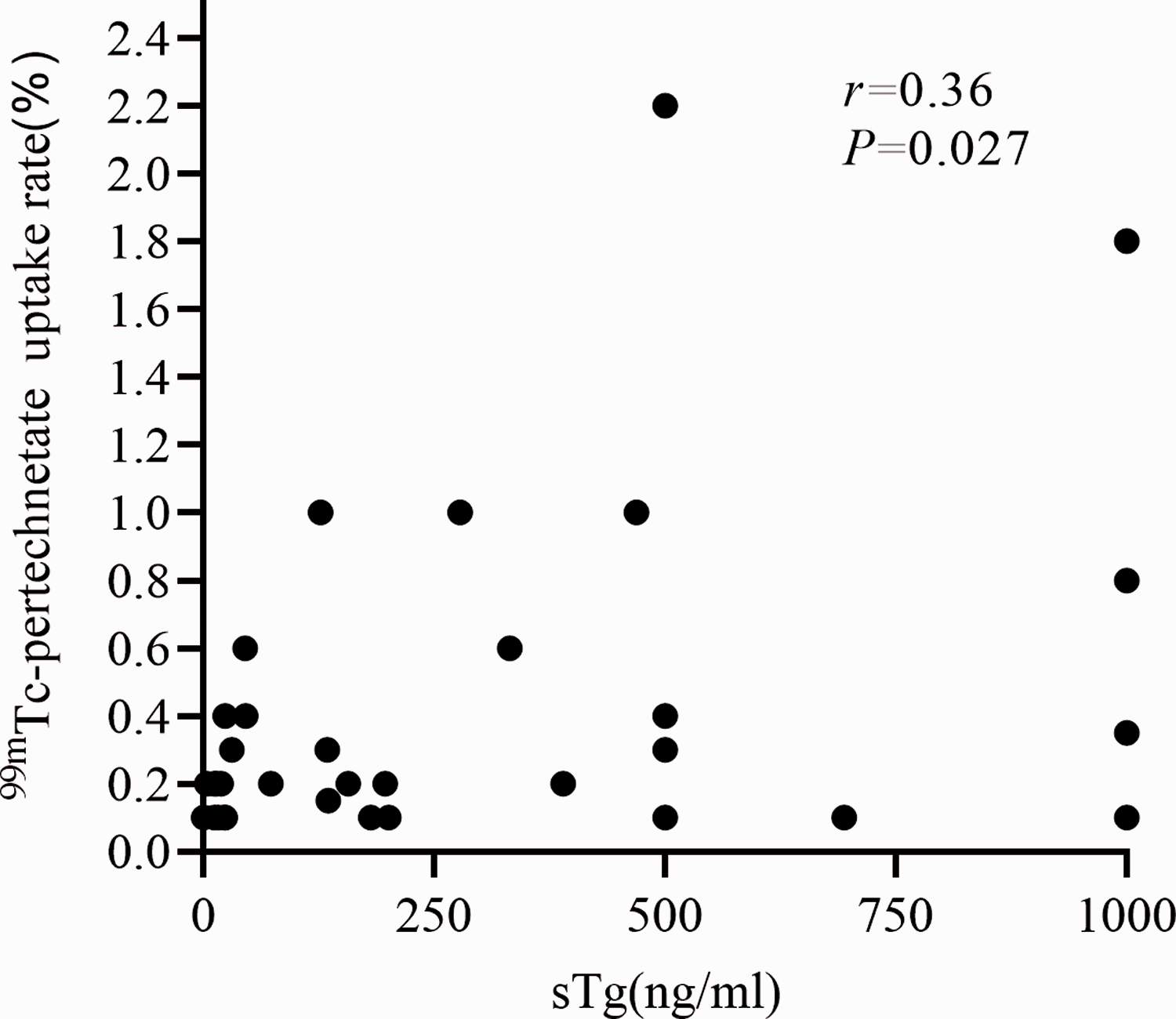
Spearman’s correlation analyses between stimulated thyroglobulin (sTg) and 99mTc-pertechnetate uptake rate of extra-thyroid lesions in patients with differentiated thyroid carcinoma (n = 38) that were included in a retrospective study of the clinical characteristics of extra-thyroid 99mTc-pertechnetate uptake. The two parameters demonstrated a significant positive correlation (r = 0.36, P = 0.027).
One patient showed 99mTc‑pertechnetate uptake in the axillary lymph node and another patient showing uptake in blood vessels, but neither patient showed obvious 131I uptake. The other 36 patients showed 131I uptake at the extra-thyroid 99mTc-pertechnetate uptake foci, with the number of 131I uptake foci being significantly more than the foci showing 99mTc-pertechnetate uptake (P = 0.015). A total of 39 of 104 foci (37.5%) showed metastases with 131I uptake but without 99mTc-pertechnetate uptake (diffuse 131I uptake in the lungs was defined as a lesion). Excluding physiological uptake, the presence of extra-thyroid 131I uptake foci was used as the criterion for judging the presence of metastases; and 94.7% (36 of 38) of extra-thyroid 99mTc-pertechnetate uptake foci were DTC metastases. Six patients showed 99mTc-pertechnetate uptake in metastatic lymph nodes, but these were not found by routine ultrasonography.
All patients underwent 131I therapy 1–10 times, with a cumulative dose of 3.7 to 57 GBq and a single dose of 3.7–7.4 GBq. The initial evaluation of the RAI therapy response in the 38 patients indicated ER in 15 patients (39.5%), IDR in four patients (10.5%), BIR in three patients (7.9%) and SIR in 16 cases (42.1%). A significant difference was found between the ER and NER groups for sTg level (Z = –2.947, P = 0.003) and pathological stage (Z = −2.348, P = 0.019), but not for age, sex, pathological type, TSH and TgAb levels and extra-thyroid 99mTc-pertechnetate uptake site and rate.
Discussion
A 99mTc-pertechnetate scan is often used to evaluate thyroid residue before the initial RAI therapy, but it is rarely used to detect suspected DTC metastases. The main reason is that although 99mTc-pertechnetate and iodine form monovalent anions, have similar physical and chemical properties and can be accumulated by sodium iodide symporter (Na+/I-symporter) located in the membrane of thyroid cells, 99mTc-pertechnetate cannot further participate in thyroid hormone synthesis after entering thyroid cells (and has faster elution) so the metastases from DTC generally do not show 99mTc-pertechnetate uptake. 17 Only a few papers have reported 99mTc-pertechnetate uptake in metastases.17,18 These current results showed that the vast majority of cases showing extra-thyroid 99mTc-pertechnetate uptake involved lymph node, lung and bone metastases, especially lymph node metastases, but the reason for this is not clear.
These current observations suggest that extra-thyroid 99mTc-pertechnetate uptake does not always indicate metastases. This current study included two false-positive patients. One patient showed 99mTc-pertechnetate uptake in the axillary lymph nodes, but no abnormality was found on other imaging examinations. In our opinion, this finding may be related to transient radioactive accumulation due to extravasation and the subsequent lymphatic drainage to the axillary lymph nodes during the injection of 99mTc-pertechnetate. Another patient showed 99mTc-pertechnetate uptake in blood vessels. In vitro experimental studies have shown that erythrocytes can show non-specific uptake of 99mTc-pertechnetate. 19 It is presumed that 99mTc-pertechnetate can be absorbed by deep venous thrombosis. 20 A previous study reported one case of gastric cancer complicated by hyperthyroidism, in which a 99mTc-pertechnetatescan revealed strip radioactive accumulation in the left upper limb and ultrasound confirmed deep venous thrombosis. 20 However, this current study could not confirm whether 99mTc-pertechnetate uptake in this false-positive patient indicated thrombosis.
To improve the ability of 131I uptake by DTC metastases, a TSH > 30 mIU/l is necessary through THW or the use of human recombinant TSH. 3 In this current retrospective study, 21.1% (eight of 38) of the patients showed no significant increase in TSH levels during the initial 131I treatment, which may be related to the good 99mTc-pertechnetate uptake and thyroid hormone secretion of the metastases. To some extent, this explains the higher sTg level before the first RAI therapy and positive correlation with the extra-thyroid 99mTc-pertechnetate uptake rate.
Diagnostic whole-body scanning (DxWBS) is often used to evaluate thyroid residue and suspected metastases, but its clinical application remains debatable due to the possible influence of the thyroid stunning effect. 21 In this current study, not all patients underwent DxWBS examination before 131I treatment, and the evaluation of metastases was mainly based on neck ultrasound and other imaging examinations such as chest CT scanning. However, lymph node metastases were found in six patients with 99mTc-pertechnetate uptake, but they were not found by routine ultrasonography, which may be related to the specificity of ultrasound diagnosis and the limitations of the scanning range. Along with routine 99mTc-pertechnetate scans, this current study undertook 99mTc-WBS/SPECT/CT for extra-thyroid 99mTc-pertechnetate uptake foci. This improved the accuracy and specificity of the diagnosis of metastases to a certain extent, making up for the lack of evaluation before RAI therapy and playing an important role in the development of treatment plans.
In this current study, the bone metastasis group showed stronger 99mTc-pertechnetate uptake than the lymph node metastasis group. The uptake rate was 0.8% (0.45%–1.6%) versus 0.2% (0.1%–0.35%), which may be related to the larger range of bone lesions and more 99mTc-pertechnetate uptake lesions, or to the partial volume effect. In addition, these current results showed similarities with some previous studies.7–9 There was high consistency between extra-thyroid 99mTc-pertechnetate uptake foci and 131I uptake foci, and the latter were greater in number. A previous study prospectively compared 99mTc-WBS combined with neck and chest SPECT/CT and Rx-WBS in 56 patients with post-surgical DTC; and found that the coincidence rate of the two scans was 84%. 9 In the four subgroups of the thyroid bed, lymph nodes, lungs and bones, the coincidence rates of the two scans were 89.5%, 55%, 82.6% and 50%, respectively. 9 In this current study, a comparative analysis of the ER and NER groups provided the preliminary finding that the higher the sTg level at the first RAI therapy, the later the pathological stage, possibly indicating a poor curative effect and prognosis. However, the patients in the current study were unique patients with extra-thyroid 99mTc-pertechnetate uptake, which is a relatively rare clinical presentation. Therefore, the sample size was small, so the results cannot necessarily be applied to all metastatic patients undergoing RAI therapy. Thus, future studies should be performed with larger sample sizes.
In conclusion, these current results showed that although the sensitivity of 99mTc-pertechnetate scans in detecting metastases was low, extra-thyroid 99mTc-pertechnetate uptake mostly indicates metastases in patients with DTC after thyroidectomy. Additional 99mTc-WBS/SPECT/CT offers incremental value over planar scans in increasing diagnostic accuracy and reducing pitfalls, which may have prognostic value for the judgment of iodine uptake function and the RAI therapy plan.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper was partially supported by the Natural Science Foundation of Zhejiang Province of China (no. LY17H180005).