
Abstract
Background:
Cancer-related fatigue (CRF) has an enormous adverse impact on quality of life and subsequent therapy of cancer patients. Complementary and alternative medicine (CAM) is reported to improve CRF in many systematic reviews (SRs), but the effects are controversial because of variations in the quality and outcomes.
Methods:
Thirteen databases were searched from inception to September 2022. Only SRs of randomized controlled trials (RCTs) were included. We assessed the quality of included SRs with the AMSTAR-2 tool, the strength of evidence with the GRADE system, the risk of bias with the ROBIS tool, and the integrity of SRs with the PRISMA checklist.
Results:
We included 30 eligible SRs (27 meta-analyses). Based on the AMSTAR-2 tool, 29 SRs were rated as “critically low” quality, and only one was rated as “low” quality. With the ROBIS tool, 19 SRs demonstrated a low risk of bias. According to the PRISMA checklist, no SRs reported all the items, and 10 SRs sufficiently reported over 70%. Based on the GRADE system, 7 outcomes were assessed as high-quality evidence.
Conclusion:
This overview demonstrates promising evidence for the effectiveness of CAM interventions in the treatment of CRF in adults. The roles of qigong, music, auricular point therapy, and dietary supplements in CRF need further evaluation. Although findings are mixed, it is recommend to select appropriate CAM to manage cancer-related fatigue under the guidance of physicians. More studies with rigorous methodological designs and sufficient sample sizes are needed.
Keywords
Introduction
Cancer seriously endangers human health. The latest statistics show that 19.3 million new cases and 10.0 million cancer deaths are expected worldwide in 2020. 1 Given cancer itself and the advanced treatments, many symptoms occur in cancer patients and survivors. Among them, fatigue is a common and universal symptom.
Cancer related fatigue (CRF), caused by cancer or cancer treatment, is perceived as a distressing, persistent sense of tiredness or exhaustion characterized by physical, emotional, and/or cognitive fatigue. 2 It has an enormous adverse impact on the usual functioning, quality of life (QoL), and subsequent therapy of cancer patients, which leads to poor prognosis. According to a meta-analysis involving 144 813 patients, the prevalence of CRF was 52%. 3 In addition, other reports have shown that 80% of cancer patients after chemotherapy experience CRF, and almost 25% of cancer survivors are also affected by CRF, lasting from months to years, even over a decade.4,5 Therefore, it is essential to deliver an effective, safe and individualized therapeutic strategy for CRF.
Numerous pharmacological and non-pharmacological interventions have been evaluated in patients with cancer to target the fatigue outcome associated with the condition. However, there are no approved drugs used in CRF treatment. CAM interventions, including 5 categories (mind-body therapies, biologically based practices, manipulative and body-based practices, energy healing, and whole medical systems), are widely employed to improve human health among physicians, acupuncturists, and physical therapists domestically and abroad. In recent years, the effect of yoga, acupuncture, massage, and other CAM interventions on CRF has gained increasing interest. Many studies6,7 report that CAM interventions can reduce fatigue in cancer patients and improve QoL, which is recommended by current guidelines as a kind of therapeutic strategy for the management of CRF.
However, current evidence shows heterogeneous effects, and related SRs have differences in the quality and outcomes, which causes the controversial efficacy of CAM on CRF. A feasible method to address this problem is to conduct an overview of previous SRs, which is exactly what we studied. This overview aimed to assess the quality of previous SRs and assimilate the existing evidence base to promote determining effective evidence-based interventions for CRF in adults and help clinicians to interpret the evidence.
Methods
The prospective protocol has been registered in PROSPERO with the number CRD42022304282. This overview of SRs was performed under the latest recommendations from the Cochrane Handbook and reported based on the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines (Supplemental Appendix 1). 8 No ethical approvals were required for this study.
Criteria for Inclusion and Exclusion
We only included SRs of RCTs and excluded SRs of non-randomized clinical trials, quasi-randomized clinical trials, and observational cohort studies. There were no restrictions on language and publication status. The target participants were adults greater than 18 years and patients with any type and stage of cancer. The interventions of SRs were CAM treatments, such as mind–body therapies (meditation, yoga, Tai Chi, etc.), manipulative and body-based practices (massage, reflexology, etc.), biologically based practices (dietary supplements, special diets, etc.), energy healing (reiki, therapeutic touch, etc.), or whole medical systems (traditional Chinese medicine, Ayurvedic medicine, etc.). The comparators were placebo, usual care, standard care, standard treatment, no interventions, or sham interventions. The primary outcome was fatigue, which must be reported in the included SRs. Secondary outcomes included QoL, depression, anxiety, sleep, pain, physical function, body mass index, biological indices, adherence, and adverse events.
Literature Searches
Two reviewers (QLZ and RZ) systematically and independently searched any published or ongoing SRs in the following databases from inception to September 2022: China National Knowledge Infrastructure (CNKI), Wan Fang database, Chinese biomedical literature service system (SinoMed), Chongqing VIP Database, MEDLINE (via PubMed), Web of Science, CINAHL, Scopus, OVID (including PsycInfo), Embase, PEDro, Cochrane Library, and PROSPERO. There were no limitations on language. Also, we manually searched all references of included studies to guarantee that no relevant SRs were eliminated by the electronic searches. We used the combination of text words and the Medical Subject Headings terms as a search strategy. Detailed electronic search strategies used in all databases are shown in Supplemental Appendix 2.
Study Selection
Two reviewers (QLZ and RZ) independently screened studies by titles and abstracts for possible inclusion. The full-text reports were also reviewed to assess appropriateness for final inclusion. Any inconsistencies were negotiated with a third reviewer (LXL) to resolve. Studies that were not eligible for enrollment were excluded, and the reasons were recorded.
Data Extraction
Two reviewers (YW and LXL) separately extracted essential information from included SRs into a normalized table after double-checking. Any disagreements were resolved by consensus with a third reviewer (QW). The extracted information included author, publication year, number of included primary studies and participants, type of cancer, type of CAM intervention and control, the approach of quality assessment, method of CRF evaluation, outcome indicators, and conclusion.
Assessment of Included Systematic Reviews
Two reviewers (QW and TTL) independently assessed the quality, risk of bias, integrity, and strength of evidence of included SRs. Disagreements and inconsistencies were resolved by a third reviewer (PJL).
AMSTAR-2, 9 a critical appraisal tool for SRs, was utilized to assess the quality of each SR. There are 16 items in the checklist, involving 7 critical items and 9 non-critical items. Responses for items were coded as “yes,” “no,” or “partial yes,” denoting a positive result, no relevant information provided, or partial adherence to the standard, respectively. We categorized the quality of included reviews as “high,” “moderate,” “low,” and “very low” based on the number of critical or non-critical weaknesses.
The ROBIS tool, 10 including 4 domains of 3 phases, was applied to assess the risk of bias of included reviews as “low,” “high,” or “unclear,” if the signaling questions for the domains were answered with “yes/probably yes,” “no/probably no,” or “no information,” respectively.
The PRISMA checklist, 8 including 27 items, was performed to evaluate the integrity of included reviews, and each item was responded to “yes,” “no,” or “partial yes.”
The GRADE system was used to assess the quality of evidence. 11 RCTs were evaluated as “high quality” at first, and the levels lowered according to the presence of bias risk, publication bias, imprecision, inconsistency, or indirectness. The strength of evidence was categorized into 4 levels (very low, low, moderate, and high).
Data Analysis
A descriptive analysis of included SRs was conducted. We summarized and showed the pooled results of included SRs. For dichotomous data, the risk ratio (RR) or odds ratio (OR) with 95% confidence interval (CI) was recorded. For continuous data, the mean difference (MD) or standardized mean difference (SMD) with 95% CI was recorded. For SR without meta-analysis, the main results of primary RCTs were recorded.
Results
Literature Search
Of15 623 related studies retrieved through 13 databases and 10 records identified through manual searching, 9208 duplicates were excluded. We excluded 6266 studies after screening the titles and abstracts and 129 records after reviewing the full texts. Finally, we included 30 SRs for further analysis (Figure 1).12-41 One hundred twenty-nine excluded records and the reasons for excluding them are provided in the Supplemental Appendix 3.

Flowchart of the selection process.
Study Characteristics
Thirty SRs (27 meta-analyses) reported 5 to 67 RCTs and 394 to 5465 participants were eligible for inclusion. All SRs were published in the latest 15 years, 11 of which were published in 2021. Twenty SRs were conducted by China, while the rest of the 10 were performed by 8 other countries, including America, Brazil, Canada, etc. Nine SRs only included participants with breast cancer, one only enrolled patients with lung cancer, one did not report types of cancer, and others incorporated participants with mixed cancer. Three SRs did not conduct meta-analyses.35,36,39 Among the 27 meta-analyses, 16 performed subgroup analyses, and 13 conducted sensitivity analyses.
Thirteen SRs assessed the effects of mind-body therapies (yoga, Tai Chi, qigong, music, and dance); 9 evaluated acupoint stimulation interventions (acupressure, acupuncture, moxibustion, and auricular point); 2 assessed manipulative and body-based practices (massage and reflexology); 3 evaluated dietary supplements; 2 assessed mixed CAM interventions; and 1 estimated kanglaite injection (a kind of traditional Chinese medicine injection).
Eighteen SRs reported on QoL; 11 involved depression and anxiety; 8 provided fatigue-related symptoms (sleep, pain, body mass index and physical function.); 1 reported the biological indices (cortisol and IL-6); 2 provided adherence; and 17 reported adverse events.
For the methodology quality assessment, most (n = 24) reviews used the Cochrane risk-of-bias tool, 2 used the Jadad scale,37,39 4 assessed the quality with one each through the Delphi list, 18 PEDro scale, 20 JBI’s tool, 21 and CONSORT guideline. 23 The complete characteristics of included SRs are shown in Table 1 and Supplemental Appendix 4.
Characteristics of Included Systematic Reviews.
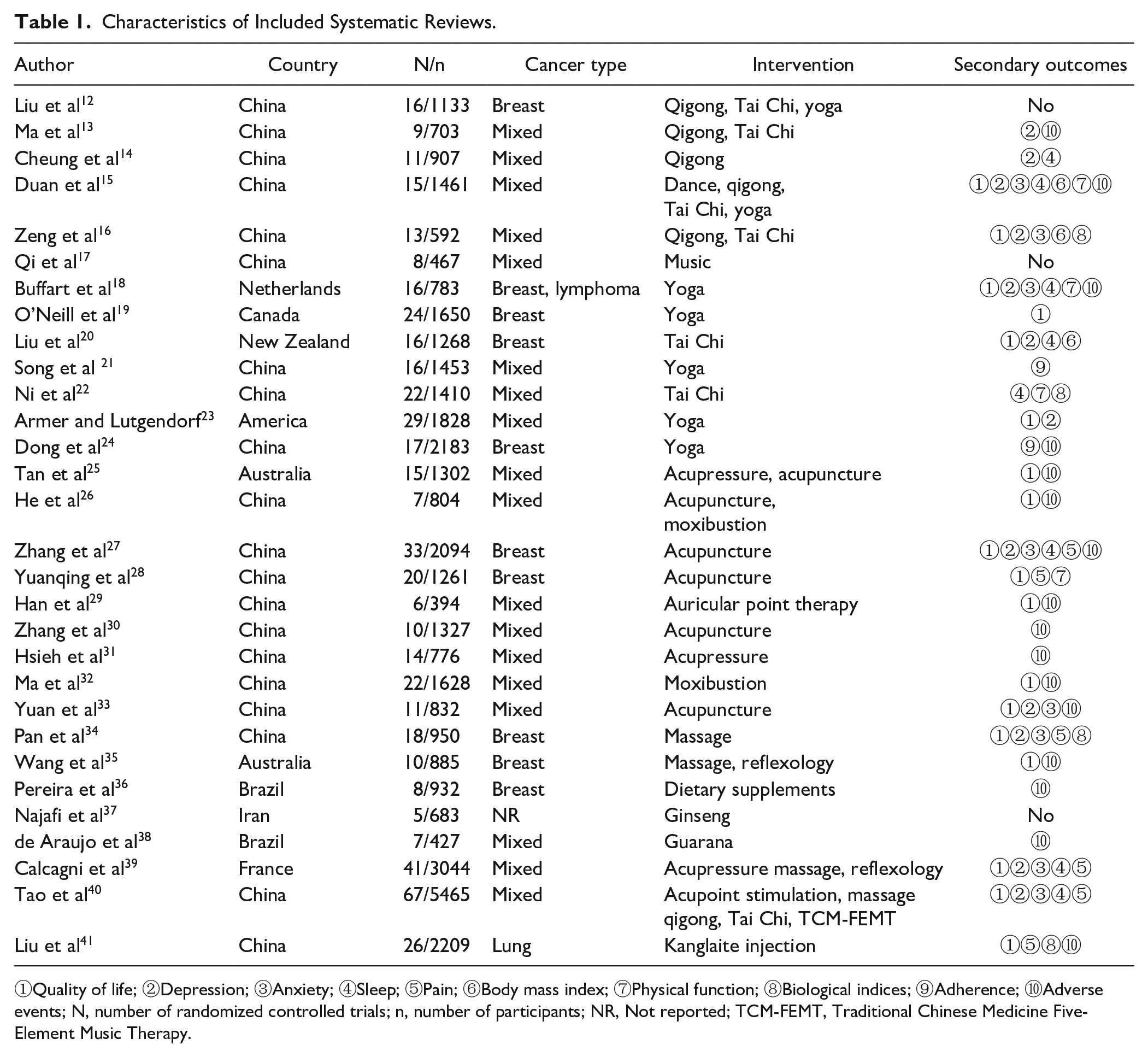
①Quality of life; ②Depression; ③Anxiety; ④Sleep; ⑤Pain; ⑥Body mass index; ⑦Physical function; ⑧Biological indices; ⑨Adherence; ⑩Adverse events; N, number of randomized controlled trials; n, number of participants; NR, Not reported; TCM-FEMT, Traditional Chinese Medicine Five-Element Music Therapy.
The Methodological Quality of Included SRs
The methodological quality of all included SRs was no higher than “low” (Table 2). Twenty-nine SRs were rated as “critically low,” and only one 31 was rated as “low.” The questions with PICO were described in all studies except three,34,36,37 and prior study protocols were established in 8 studies. Only one SR 13 explained why selected RCTs for inclusion. All except one SR, 41 which did not provide any search terms or strategies, undertook a comprehensive literature search. Five SRs did not select studies or extract data in duplicates. One SR 12 did not describe comparators of included studies. Two SRs37,39 did not use proper techniques to assess the risk of bias. No SRs afforded checklists of excluded studies and the reasons for excluding them. Only one SR 38 reported the funding sources for the primary studies. Most SRs reported potential conflicts of interest, but few assessed publication bias. All meta-analyses used appropriate methods for results combination, but only one 31 conducted a meta-regression analysis to evaluate possible impacts of bias risk on the results. When discussing the results, 26 SRs (86.67%) accounted for the bias risk, and 25 SRs (83.33%) considered heterogeneity.
AMSTAR-2 Tool of Methodological Quality Assessment of Included Systematic Reviews.

The key items of the AMSTAR-2 tool; I, Item; Y, Yes; N, No; PY, Partial yes.
Risk of Bias of Included SRs
We applied the ROBIS tool to evaluate the risk of bias in included SRs (Table 3, Figure 2). In phase 1, the target questions of all SRs matched or partially matched the study questions. In phase 2, we identified the risk of bias in the study process through 4 domains: study eligibility (domain 1), study selection (domain 2), data collection and quality appraisal (domain 3), and data synthesis and findings (domain 4). There were 22, 16, 17, and 8 SRs with low risk of bias in domains 1, 2, 3, and 4, respectively. One SRs were assessed as unclear risk of bias in domains 2 and 3. We considered the overall bias risk of included SRs in phase 3. Nineteen SRs were demonstrated as low bias risk, and 11 were evaluated as high bias risk.
ROBIS Tool of Risk of Bias of Included Systematic Reviews.

 Low risk;
Low risk;  High risk;
High risk;  Unclear risk; Y, Yes; PY, Partial yes.
Unclear risk; Y, Yes; PY, Partial yes.

Graphical presentation for ROBIS tool of risk of bias.
Reporting Quality of Included SRs
Reporting quality and integrity of included SRs were evaluated with the PRISMA checklist, including 27 items (Table 4). No SRs reported all items. Ten SRs sufficiently reported over 70% of all items, and only one reported less than 50%. All SRs adequately introduced their rationales and objectives. In the methods section, eligibility criteria and information sources were well reported (100%). Most SRs specified how to identify studies, extract data, and evaluate the quality. In the results section, more than 85% of SRs provided general characteristics, bias risk, and primary outcomes of included studies. 86.7% of SRs discussed any limitations and implications of included studies. Ninety percent of SRs described the funding sources and declared any competing interests. Overall, the central reporting limitations consisted of registration and protocol (23.3%), abstract (0%), search strategy (10%), assessment and results of reporting bias (26.7%), assessment and results of evidence certainty (10%, 13.3%), and study selection (3.3%).
Compliance of PRISMA Checklist of Included Systematic Reviews.

Abbreviations: Y, Yes; N, No.
Evidence Quality of Included SRs
Given that 3 SRs did not combine the results for meta-analysis, we only used the GRADE system to evaluate the strength of evidence for CRF outcomes (51 pooled results) and other significant secondary outcomes (69 pooled results) reported in the other 27 SRs. Among 51 pooled results of CRF, 2 were assessed as “high” quality, 21 as “moderate” quality, 18 as “low” quality, and 10 as “very low” quality. As for other secondary outcomes (QoL, depression, anxiety, etc.), 3 of 69 pooled results were assessed as “high” quality, 30 as “moderate” quality, 21 as “low” quality, and 15 as “very low” quality. The certainty of the evidence was downgraded mainly due to imprecision and inconsistency. Tables 5 and 6 show the reasons for downgrading.
Summary and GRADE Quality of Evidence for CRF Outcomes Reported in the Included Systematic Reviews.

①Serious risk of bias; ②Suspicion of publication bias; ③The cumulative sample size was not enough, and/or 95% confidence interval was very wide; ④I2-value of the results was large ( ≥70%); ⑤I2-value of the results was very large ( ≥90%); BFI, Brief Fatigue Inventory; NR, Not reported; PFS, Piper Fatigue Scale.
GRADE Quality of Evidence for Significant Secondary Outcomes Reported in the Included Systematic Reviews.

①Serious risk of bias; ②Suspicion of publication bias; ③The cumulative sample size was not enough, and/or 95% confidence interval was very wide; ④I2-value of the results was large ( ≥70%); ⑤I2-value of the results was very large ( ≥90%); KPS, Karnofsky Performance Status; QoL, Quality of Life; TCM-FEMT, Traditional Chinese Medicine Five-Element Music Therapy.
Effects on Cancer-Related Fatigue
Thirteen SRs12-24 reported the effects of mind-body therapies (qigong, Tai Chi, yoga, dance, and music) on CRF (Table 5). Of these, significant reductions were observed with mind-body therapies versus control (three SRs, SMD = 0.59, 95% CI: 0.27, 0.92; moderate-quality; SMD = 1.03, 95% CI: 0.61, 1.44; moderate-quality; SMD = −0.47, 95% CI: −0.88, −0.06; low-quality)12,13,15; yoga versus control (four SRs, SMD = −0.51, 95% CI: −0.79, −0.22; moderate-quality; SMD = −0.20, 95% CI: −0.34, −0.06; high-quality; SMD = 0.45, 95% CI: 0.09, 0.82; very low-quality; SMD = −0.31, 95% CI: −0.52, −0.10; low-quality)18,19,23,24; yoga versus routine care (SMD = −0.52, 95% CI: –0.86, –0.18; moderate-quality) 21 ; qigong versus control (SMD = −0.93, 95% CI: −1.80, −0.06; very low-quality) 16 ; music versus control (SMD = −0.88, 95% CI: −1.49, −0.26; low-quality) 17 ; and a combination of Tai Chi with conventional supportive care versus conventional supportive care alone (SMD = −0.91, 95% CI: −1.30, −0.53; low-quality). 20 Furthermore, one SR did not reveal any differences in CRF level between the Tai Chi and the control group. 22 One SR showed substantial reductions of CRF post-intervention (SMD = −0.89, 95% CI: −1.59, −0.19; very low-quality), 14 but no differences were observed at 3-month follow-up between the qigong and the control group. No SRs showed increased degrees of CRF following mind-body therapies.
Nine SRs25-33 reported the effects of acupoint stimulation therapies (acupuncture, moxibustion, auricular point therapy, and acupressure) on fatigue in adults with cancer (Table 5). CRF was significantly improved with acupoint stimulation methods: acupressure or acupuncture versus standard treatment (SMD = −0.95, 95% CI: −1.66, −0.25; low-quality) or sham therapies (SMD = −0.28, 95% CI: −0.54, −0.01; moderate-quality) 25 ; acupuncture versus control (4 SRs, SMD = −0.39, 95% CI: −0.55, −0.22; moderate-quality; SMD = −1.19, 95% CI: −2.25, −0.12; very low-quality; SMD = −1.26, 95% CI: −1.80, −0.71; low-quality; SMD = −1.06, 95% CI: −1.73, −0.40; low-quality)27,28,30,33; acupressure versus control (SMD = −0.87, 95% CI: −1.19, −0.55; moderate-quality) 31 ; and moxibustion versus control (SMD = −1.17, 95% CI: −1.44, −0.90; moderate-quality). 32 Also, a combination of auricular point with standard care significantly reduced CRF compared with standard care alone (RR = 1.76, 95% CI: 1.42, 2.17; very low-quality). 29 The addition of moxibustion to routine care provided a slight improvement in severe CRF (the score of Piper Fatigue Scale ≥7 points) compared with routine care alone (OR = 0.16, 95% CI: 0.07, 0.37; low-quality), but none to mild or moderate CRF. 26
Two SRs34,35 reported the effects of manipulative and body-based practices (massage and reflexology) on CRF (Table 5). Only one SR 34 conducted a meta-analysis, showing that administration of massage versus usual care or sham massage improved CRF in adults with breast cancer (SMD = −0.61; 95% CI: −1.09, −0.13; low-quality). The other SR 35 included 10 RCTs, 7 of which revealed that reflexology or massage significantly reduced CRF, and 3 reported no significant improvement following massage compared with routine treatment and care.
Three SRs36-38 reported the effects of dietary supplements (ginseng, guarana, acetyl-l-carnitine, coenzyme Q10, etc.) on CRF (Table 5). One SR 36 without meta-analysis included 9 RCTs, 5 of which showed that CRF could be reduced with supplements of guarana extract, branched-chain amino acids, coenzyme Q10, acetyl-l-carnitine, and chlorella extract, while the other 4 reported no differences between the dietary supplements and the control group. Two SRs37,38 with meta-analyses revealed that ginseng provided significant improvements for CRF patients (SMD = 1.24; 95% CI: 0.05, 2.42; low-quality), but guarana did not (Table 5).
Three SRs39-41 reported the effects of mixed CAM interventions or kanglaite injection (a kind of traditional Chinese medicine) on CRF (Table 5). One SR, 39 involving 41 RCTs, did not conduct a meta-analysis due to clinical heterogeneity, of which 5 reported on CRF. Among these, 4 RCTs indicated that acupressure, massage, or reflexology therapy significantly reduced CRF. Another RCT with 286 participants showed no differences between the reflexology and the standard care or lay foot manipulation group. One SR 40 reported the effects of acupuncture, Tai Chi, or qigong on CRF. Response rates of improving fatigue assessed by Piper’s Fatigue Scale doubled with acupuncture versus control (OR = 2.40; 95% CI: 1.40, 4.13; low-quality). CRF assessed by Brief Fatigue Inventory was slightly improved for acupuncture versus control (SMD = −1.41, 95% CI: −2.58, −0.24; very low-quality), as well as for mixed CAM therapies versus control (SMD = −1.19, 95% CI: −2.19, −0.18). One SR 41 showed that a combination of kanglaite injection and chemotherapy did not significantly reduce CRF compared with chemotherapy alone based on 2 RCTs.
Effects on Quality of Life
Seven SRs reported the effects of mind-body therapies (qigong, Tai Chi, yoga, and dance) on QoL (Table 6, Supplemental Appendix 5). Significant improvements were observed in QoL with qigong versus control at 12-week follow-up (MD = 6.57, 95% CI: 2.32, 10.84; very low-quality) 16 ; yoga versus control (SMD = 0.37, 95% CI: 0.11, 0.62; moderate-quality) 18 or non-active comparators (SMD = 0.27, 95% CI: 0.07, 0.46; moderate-quality) 19 ; Tai Chi versus usual supportive care at 3-month follow-up (SMD = 0.32, 95% CI: 0.07, 0.56; moderate-quality) 20 ; and a combination of Tai Chi with usual supportive care either at 3-month follow-up or 6-month follow-up compared with conventional supportive care alone (SMD = 0.34, 95% CI: 0.26, 0.43; SMD = 0.40, 95% CI: 0.31, 0.49; both moderate-quality). 20 One SR 22 also reported that Tai Chi positively affects both the physical (SMD = 0.34, 95% CI: 0.09, 0.59; moderate-quality) and psychological domains of QoL (SMD = 0.60, 95% CI: 0.12, 1.08; low-quality). Two SRs15,23 showed no differences in the improvement of QoL respective of following qigong, yoga, or dance compared with control.
Six SRs reported the effects of acupoint stimulation therapies (acupuncture, auricular point therapy, and moxibustion) on QoL (Table 6, Supplemental Appendix 5). One SR, 25 involving 8 RCTs, conducted a descriptive analysis of QoL, of which 6 indicated that acupoint stimulation significantly improved QoL. The addition of moxibustion to routine care has a positive effect on emotional function (SMD = 0.97, 95% CI: 0.72, 1.22; moderate-quality) and global QoL (SMD = 0.81, 95% CI: 0.20, 1.43; low-quality) compared with routine care alone, but no substantial improvements were observed in role function, cognitive function, and social function. 26 QoL was also improved with acupuncture versus control (MD = 10.09, 95% CI: 7.26, 12.92; low-quality), 27 auricular point therapy plus standard care versus standard care alone (MD = 7.34, 95% CI: 5.11, 9.57; low-quality), 29 and moxibustion versus control (SMD = 0.88, 95% CI: 0.54, 1.22; high-quality). 32 A combination of auricular point therapy with standard care or moxibustion also significantly improved role function (MD = 8.99, 95% CI: 7.45, 10.53; MD = 9.39, 95% CI: 2.22, 16.56; both low-quality), emotional function (MD = 8.75, 95% CI: 6.51, 10.98; MD = 11.71, 95% CI: 4.41, 19.01; both low-quality), cognitive function (MD = 7.17, 95% CI: 4.85, 9.50; low-quality; MD = 7.96, 95% CI: 3.08, 12.85; moderate-quality), and social function (MD = 5.64, 95% CI: 4.17, 7.10; low-quality; MD = 11.01, 95% CI: 7.46, 14.56; moderate-quality) compared with standard care alone.29,32 In addition, one SR 33 revealed that acupuncture did not provide significant benefits in CRF compared with the control.
Three SRs reported the effects of manipulative and body-based practices (massage and reflexology) on QoL (Table 6, Supplemental Appendix 5). One SR 34 with meta-analysis showed that massage did not improve QoL compared with usual care or sham massage in adults with breast cancer. Two SRs conducted descriptive analyses of QoL. Four studies of one SR 35 reported QoL, of which one revealed that reflexology or massage substantially improved QoL at 6-week follow-up. In contrast, the other 3 reported no statistically significant differences between the massage or reflexology and the control group. Five studies of the other SR showed increased QoL in the massage or reflexology group, and 7 other studies reported no significant differences. 39
Two SRs reported the effects of mixed CAM interventions or kanglaite injection on QoL (Table 6, Supplemental Appendix 5). Mixed CAM therapies versus control (SMD = 0.97, 95% CI: 0.18, 1.76; very low-quality) or massage versus control (SMD = 1.31, 95% CI: 0.21, 2.41; very low-quality) significantly improved QoL, which was assessed with cancer-specific QoL scales, while acupuncture or qigong did not. 40 Acupuncture versus control provided significant improvements in QoL, assessed with means of the Karnofsky Performance Scale (KPS) (MD = 4.55, 95% CI: 0.75, 8.34; very low-quality) or remission rate of KPS (OR = 2.32, 95% CI: 1.26, 4.27; low-quality). 40 The number of patients with a ≥ 10-point improvement in the KPS score was 2-fold for kanglaite injection plus chemotherapy versus chemotherapy alone (RR = 2.05, 95% CI: 1.60, 2.64; low-quality). 41
Effects on Depression
Thirteen SRs reported depression (Table 6, Supplemental Appendix 5). Of these, three15,18,23 demonstrated significant reductions in depression following yoga compared with control, one 40 showed that traditional Chinese medicine 5-element music therapy relieved depression compared with control. Eight SRs revealed that administration of qigong, Tai Chi, acupuncture, or massage did not improve depression. Five of 41 RCTs in the other SR 39 also reported depression. Among these, 3 showed significant improvements following massage compared with visits by staff or usual care and attention, and 2 showed none.
Effects on Anxiety
Eight SRs reported anxiety (Table 6, Supplemental Appendix 5). Significant improvements were observed with yoga versus control15,18; acupuncture versus control 27 ; and mixed CAM therapies versus control. 40 Three SRs16,33,34 showed no differences in the alleviation of anxiety following qigong, acupuncture, or massage compared with control. Six studies in another SR 39 also reported anxiety. Among these, 3 showed significant remissions of anxiety in the massage, reflexology, or acupressure group.
Effects on Sleep
Nine SRs reported sleep (Table 6, Supplemental Appendix 5). Sleep quality was significantly improved with CAM therapies: mind-body therapies or yoga versus control 15 ; Tai Chi versus control 22 ; and acupuncture versus control.27,40 One review 14 revealed that qigong had a positive benefit in sleep post-intervention, but no differences were observed at 3-month follow-up. Three SRs18,20,32 showed no improvements in sleep following yoga, Tai Chi, or moxibustion compared with control. Five studies in another SR 39 without meta-analysis indicated that massage versus control or acupressure versus sham acupressure significantly improved sleep.
Effects on Pain
Seven SRs reported pain (Table 6, Supplemental Appendix 5). Significant reductions were observed in pain with acupuncture versus control,27,40 and moxibustion versus control. 32 A combination of kanglaite injection and chemotherapy significantly improved chest pain compared with chemotherapy alone. 41 Two SRs28,34 revealed no significant differences between the acupuncture or massage group and the control group. One SR 39 did not conduct a meta-analysis, of these, 11 studies showed improvements in pain following massage, reflexology, or acupressure compared with control.
Effects on Body Mass Index
Four SRs reported body mass index (BMI) (Table 6, Supplemental Appendix 5). Mind-body therapies versus control 15 or Tai Chi versus control 40 conspicuously reduced BMI. Two SRs16,20 showed no statistical differences in the improvement of BMI following qigong or Tai Chi compared with control.
Effects on Physical Function
Six SRs reported physical function (Table 6, Supplemental Appendix 5). Mind-body therapies or moxibustion versus control significantly improved physical function.15,32 Tai Chi provided considerable enhancements in upper limb function, muscular strength of upper limbs, and vital capacity.22,40 In addition, 3 SRs15,18,28 showed no significant differences in physical function following yoga or acupuncture compared with control.
Effects on Biological Indices
Three SRs reported biological indices (Table 6, Supplemental Appendix 5). Tai Chi significantly improved cortisol and IL-6 compared with control. 22 The other 2 SRs16,34 showed no significant differences in cortisol following qigong, Tai Chi, or massage compared with control.
Adherence
Two SRs reported adherence to the yoga intervention (Table 6, Supplemental Appendix 5). One SR 21 with meta-analysis showed considerable differences in the adherence between the yoga and the routine care groups. In the other SR 24 without meta-analysis, 4 studies showed high adherence (>80%), and 3 revealed low adherence (could not be described as a percentage).
Adverse Events
Seventeen SRs reported adverse events (Table 6, Supplemental Appendix 5). One SR 31 with meta-analysis indicated that no substantial differences were observed in the occurrence of adverse events between the acupressure and the control group. The other SR 41 also conducted a meta-analysis, showing that kanglaite injection might increase the incidence of grade II to IV phlebitis, and decrease the incidence of grade II to IV leukopenia, thrombocytopenia, and anemia. The mind-body therapies-related adverse events reported in the SRs were transient back spasms, panic attack and foot pain, transient muscle soreness, unilateral hip pain, flu-like symptom, leg cramps, swelling of the hand, stomach pain, shoulder pain, and side pain.13,15,16,18,24
Adverse events induced by acupuncture or acupressure were pain, bruising, blood stasis, pruritus, or bleeding at the intervention site, headache, palpitations, fatigue, dizziness, nausea, and feeling of discomfort.25-27,30,33 The auricular point-related adverse events reported in the SRs were pain, discomfort, or itchiness in the stimulated ear. 29 The moxibustion-related adverse events were mild blisters, erythema, and slight itching. 32 The massage-related adverse events reported in the SRs were bruising, back pain, and increased blood pressure, which were resolved in a later massage session. 35 Adverse events attributable to dietary supplements were palpitation, tachycardia, nausea, vomiting, insomnia, anxiety, diarrhea, xerostomia, dry skin, headache, neuropathy, leukopenia, anemia, and arthralgia.36,38 No serious adverse events were reported in all included SRs.
Discussion
Main Findings
The primary results are presented in our published review. All the CAM interventions, except for kanglaite injection, showed significant potential to reduce CRF. Based on the included SRs, yoga was recommended to reduce CRF in adults with cancer, and the role of other CAM interventions requires further research. All the included CAM interventions showed significant improvements in QoL. As for psychological outcomes, yoga or acupuncture were effective in improving both depression and anxiety; and qigong or music ameliorated depression. With regard to physical outcomes, yoga, Tai Chi, or qigong enhanced physical function and improved sleep; acupuncture might improve sleep. Improvement in pain was also evident with acupuncture, moxibustion, or massage. In addition, significant improvements were observed in BMI, IL-6 and cortisol levels with Tai Chi.
Comparison to Current Recommendations
Yoga (a kind of practice combining stretches, meditation, and breathing to relax the mind and body) is recommended by the latest international guidelines such as guidelines set by the National Comprehensive Cancer Network (NCCN), 2 American Society of Clinical Oncology (ASCO), 42 and European Society for Medical Oncology (ESMO), 43 to treat CRF in patients either undergoing active cancer treatment or post-treatment. Our study provides high-quality evidence which suggests that yoga improves CRF and increases adherence. In another study evaluating the effects of non-pharmacological interventions on CRF, yoga showed the highest impact in cancer patients after treatment. 44 Based on current evidence, the role of yoga as an effective treatment in adults with CRF is clear, but establishing the time and frequency of therapy requires further investigation.
Our review shows that qigong and music may reduce CRF, but the quality of evidence is low. Based on the current guidelines, the recommendation of qigong or music to reduce CRF still needs more research, especially in the post-treatment participants.
Tai Chi (a form of exercise that combines meditation, slow body movements, and controlled breathing) does not appear to be a viable option to treat CRF in the current guidelines. Our review provides moderate-quality and conflicting evidence for Tai Chi relieving CRF. Another study also summarized previous SRs, indicating that Tai Chi might have a beneficial effect on fatigue in patients with breast cancer. 45 A more robust conclusion needs to be further assessed through well-designed and well-conducted clinical trials.
Acupuncture is widely used worldwide to promote health and improve disease-related symptoms. Our study provides moderate-quality evidence suggesting that acupuncture relieves CRF. Furthermore, one study 46 conducted an overview to assess the effects of acupuncture-related therapies on CRF, showing potential advantages in terms of efficacy and safety. Another study 47 focused on the impact of acupuncture on cancer-related conditions, which also indicated its benefits for cancer survivors with fatigue. Based on current evidence, acupuncture is recommended for the treatment of CRF in cancer survivors.
Moxibustion, acupressure, and auricular-point therapy are also used to improve health by stimulating specific points. Our study revealed moderate-quality evidence suggesting that moxibustion and acupressure reduce CRF, and very low-quality evidence suggesting that the auricular point therapy may relieve CRF. However, they are not mentioned in any guidelines, probably due to few studies.
Massage, a type of therapy that uses the hands to manipulate the soft tissues of the body, is recommended by the NCCN guidelines to reduce CRF in patients undergoing active cancer treatment, while the ASCO guidelines suggest that additional research is needed to verify the effects. Our study provides low-quality evidence suggesting that massage alleviates CRF. However, whether massage significantly improves CRF compared with routine treatment and care is uncertain. No other study has performed an overview of previous SRs to assess the effects of massage on CRF. Given the low methodological quality and small number of primary studies, no definite conclusions can be drawn. Reflexology applies pressure at specific points on the hands or feet. Some clinical trials have revealed that reflexology relieves CRF, 35 while others observed no significant differences between reflexology and lay-foot manipulation or standard care, 39 leading to confounded conclusions. Based on the included SRs, massage and reflexology showed great potential for reducing CRF, which deserves further research.
Dietary supplements, including various products such as vitamins and herbs, are common non-pharmacological strategies used for patients with cancer. Ginseng, a herb, has been confirmed to have immunomodulatory properties. 48 Our study provides low-quality evidence suggesting that ginseng reduces CRF. However, current international guidelines have not reached a consensus on the use of ginseng because of its inconsistent effects. The use of acetyl-L-carnitine, coenzyme Q10, and guarana is not recommended to control CRF in the current guidelines due to the lack of related studies. A SR and meta-analysis revealed that guarana does not provide a significant reduction in CRF compared to placebo. 38 Larger RCTs are needed to identify the effects of dietary supplements on CRF.
Our review provides moderate-quality evidence to suggest that yoga improves depression and anxiety, and very low-quality evidence suggests that music relieves depression. Music therapy is a kind of creative outlet. In traditional Chinese medicine, it is often used according to the Five Elements theory, which may improve the efficacy of general music therapy. Current guidelines recommend music to alleviate anxiety and depression, but extensive clinical studies are needed to evaluate the potential effects of yoga.
CRF and sleep disturbances were also highly correlated. 49 Current guidelines recommend yoga or Tai Chi to improve sleep, which was also shown in our study. Furthermore, our review also provides high-quality evidence to suggest acupuncture to improve sleep. Another meta-analysis revealed that acupuncture significantly improved sleep in patients with breast cancer receiving active cancer treatment. 50 Therefore, the effects of acupuncture on sleep require further investigation. Pain is a risk factor of CRF. 3 Our review provides moderate-quality evidence to suggest that acupuncture improves pain, and low-quality evidence suggests that moxibustion relieves pain. Current guidelines recommend physical modalities (massage, acupuncture, acupressure, etc.) for improving pain; however, the effects of moxibustion on pain need to be further evaluated in more clinical trials.
Cortisol dysregulation is related to cancer development and QoL, and abnormalities in cortisol rhythm may lead to CRF. 51 IL-6, a pivotal inflammatory cytokine, is associated with cancer development and cancer-related symptoms—such as fatigue, anxiety, and depression. 52 BMI is also considered to be an important prognostic indicator of cancer. Tai Chi was the only intervention regulating cortisol, IL-6, and BMI in our study; it may also improve cancer-related symptoms or cancer prognosis. However, no differences in IL-6 levels were observed in another meta-analysis between the Tai Chi and support therapy groups. 53 Current guidelines do not refer to these findings, which should be confirmed by further studies.
Kanglaite injection is a traditional Chinese medicine, and its active substance is extracted from the herbal semen coicis. The addition of kanglaite injection to chemotherapy does not reduce CRF compared with chemotherapy alone, but improves QoL and some physical outcomes (pain, nausea, and vomiting), and decreases the incidence of adverse events. 41 However, no current international guidelines recommend kanglaite injection for the treatment of cancer or cancer-related symptoms because of the primary low-quality studies.42,43
Strengths and Weaknesses of the Review
CAM is a broad set of medical products and practices which is not part of the dominant healthcare systems. The prevalence for “current use” and “past use” of CAM in patients with cancer is around 40% and 43%, respectively, reported by a SR and meta-analysis involving 18 countries. 54 It also shows an increasing trend of CAM use in cancer from the 1970s to date. CAM is often used to lessen the side effects of cancer treatments and improve cancer-related symptoms, especially fatigue. The effects of CAM on CRF have been assessed in many studies,12-14 but given the mixed results, it remains obscure to determine effective interventions based on evidence-based medicine.
The goal of this study was to summarize the evidence to date on CAM interventions in the treatment of CRF by conducting an overview without language limitations. Only SRs of RCTs were included to reduce the risk of bias. As far as we know, this is the first comprehensive review of the association between CAM interventions and fatigue outcomes of adults with cancer.
Thirty SRs were included in our review. Only one SR was assessed as “low” or above methodological quality with the AMSTAR-2 tool, and 19 SRs were deemed low bias risk from the ROBIS tool. As for the reporting integrity evaluated by the PRISMA checklist, it was regrettable that no SR reported all 27 items. The strength of evidence was rated by the GRADE tool. There were 5 pieces of high-quality evidence (CRF, QoL, sleep, and adherence) and 51 pieces of moderate-quality evidence, which included all the outcomes except adherence.
Notwithstanding the above assessments, there was considerable heterogeneity in CRF between the included SRs. The reasons were likely multifaceted: (1) The types of cancer were multiple. Nineteen of 30 SRs included patients with mixed types of cancer; (2) The timing of outcomes assessment varied and was not clarified in many SRs, such as post-intervention, 3-month follow-up, 6-month follow-up, etc.; (3) The approaches of outcomes assessment were diverse. For instance, there were 24 different scales to evaluate CRF in the included SRs. The heterogeneity may have confounded the overall efficacy of CAM interventions in the treatment of CRF, as well as other cancer-related symptoms. Therefore, future high-quality studies are required to verify the effects.
Clinical and Research Implications
Our review shows that yoga and acupuncture improve CRF in adults with cancer, which is also recommended by the current international guidelines. Some studies have revealed that acupuncture for at least 4 times or yoga for at least 6 weeks has substantial effects on CRF.24,30 However, no consensus has been established on the unified criteria for the course or frequency of treatment. It should be well-designed in future RCTs in accordance with previous studies and be considered as a stratification factor when analyzing the results in future SRs.
Although massage relieves CRF based on one meta-analysis that included 5 RCTs 34 and the use of qigong, Tai Chi, music, moxibustion, acupressure, auricular point therapy, or dietary supplements of ginseng in reducing CRF shows some favorable results, their recommendation has not yet been agreed upon in current guidelines because of the low quality of the methodology and few studies. Considering these shortcomings, conducting high-quality and extensive clinical research in the future is essential.
Besides the interventions mentioned above, other CAM therapies, such as reiki, imagery, and hypnosis, were not assessed in our study because related SRs were not found. For example, hypnosis, a type of mind-body therapy, can make people feel calmer and more focused by channeling them into a trance-like state. A SR of 13 RCTs showed that hypnosis improves CRF and pain. 55 Therefore, the effects of other CAM interventions on cancer-related symptoms warrant further investigation.
Furthermore, our study clarifies that few specific indicators or biomarkers to assess CRF exist, which is worth pursuing in the future. For example, inflammation is supposedly a pivotal contributor to CRF, and one study evaluated the changes in IL-6 and IL-8 to explore the correlation between anti-inflammatory and CRF reduction. 56 Moreover, many RCTs using CAM interventions, such as yoga and massage, cannot be designed with double-blinding, and CRF outcomes are mostly evaluated with subjective scales. Therefore, pursuing more specific indicators or biomarkers may reduce the risk of bias.
Conclusion
This overview demonstrates that CAM interventions, particularly yoga, Tai Chi, acupuncture, moxibustion, acupressure, massage, and dietary supplements of ginseng, improve CRF in adults with cancer. The roles of qigong, music, auricular point therapy, other dietary supplements, and other traditional Chinese medicines in CRF need further evaluation, as some data show encouraging results. The evidence for improvements in QoL, depression, anxiety, and sleep was more robust than that for other outcomes (pain, physical function, and BMI) and biological indices (cortisol and IL-6). However, given the heterogeneity of the included SRs and the low quality of original RCTs, conducting further research with rigorous methodological designs and sufficient sample sizes is still necessary. Additionally, performing SRs with high quality and reporting of comprehensive findings is essential.
Supplemental Material
sj-docx-1-ict-10.1177_15347354231188947 – Supplemental material for The Role of Complementary and Alternative Medicine on Cancer-Related Fatigue in Adults: An Overview of Systematic Reviews
Supplemental material, sj-docx-1-ict-10.1177_15347354231188947 for The Role of Complementary and Alternative Medicine on Cancer-Related Fatigue in Adults: An Overview of Systematic Reviews by Peijin Li, Qian Wang, Lixing Liu, Qinglin Zhang, Rui Zhou, Yue Wang, Tingting Liu and Li Feng in Integrative Cancer Therapies
Footnotes
Author Contributions
Conceptualization: PJL, LF. Methodology: QW, QLZ. Validation: LXL, TTL, YW. Formal analysis: PJL, QW. Investigation: PJL, QW, LXL, QLZ, RZ TTL, YW. Data curation: PJL, LF. Writing—Original Draft: PJL, QW, RZ, TTL, YW. Writing—Review & Editing: LXL, QLZ, LF. Visualization: PJL, LXL, RZ. Supervision: PJL, LF. Project administration: PJL, LF. Funding acquisition: LXL, LF.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Natural Science Foundation of China [Grant Number 82104958] and the Capital Health Research and Development of Special [Grant Number 2020-2-4026]. The funders had no role in the design and performance of the study; extraction, synthesis, and analysis of the data; preparation, editing, and approval of the manuscript; and the decision to publicize the manuscript.
Ethical Statement
This research did not require ethical approval because of the study type.
Data Availability
The data that support the findings of this study are available within the article [and/or its Supplemental Material]
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.