
Abstract
Background. Traditional Chinese herbal medicine (TCHM) is widely used for advanced gastric cancer (AGC) in China. In this study, the authors analyzed the prognostic factors of selected patients with AGC, and further studied the efficacy of TCHM (a herbal formula for invigorating spleen, formerly named Wei Chang’ An) on AGC. Methods. Patients with uncured AGC were prospectively enrolled. All patients were enrolled to either the TCHM group or non-TCHM group. TCHM was administered orally to the patients in the TCHM group for 3 months or more. Cox regression analysis was performed to determine survival trends adjusted for clinical and demographic factors. Kaplan–Meier curves were used to assess the differences in survival time. Results. There were a total of 399 eligible patients with histologically confirmed adenocarcinoma of the stomach from 2001 to 2009. In the overall group, Cox regression analysis suggested that histological type (P = .016), radiotherapy (P = .000), cycle of chemotherapy (P = .000), and TCHM (P = .000) were independent prognostic factors. In a stratification analysis of stage for 213 patients who received 3 or more cycles of chemotherapy, there was a significant increase in median overall survival from 14.0 (non-TCHM group) to 20.0 (TCHM group) months (hazard ratio [HR] = 0.538, 95% confidence interval [CI] 0.385-0.750, P = .000). Among 186 patients who did not receive chemotherapy, but best supportive care, there was a significant increase in median overall survival from 7.0 (non-TCHM group) to 14.8 (TCHM group) months (HR = 0.443, 95% CI = 0.299-0.657, P = .000). Conclusions. TCHM has an important potential value for improving the prognosis of patients with AGC.
Keywords
Introduction
Gastric cancer currently ranks second in global cancer mortality. 1 Overall, 80% to 90% of all patients are either diagnosed at an advanced stage when the tumor is inoperable or develop a recurrence or metastasis within 5 years. Patients with advanced gastric cancer (AGC) have a poor prognosis with a median survival time of 4.3 months with best supportive care (BSC), whereas median survival time of advanced gastric cancer patients with chemotherapy ranges from 8.6 to 13.0 months.2-6 If patients accept high-priced molecular targeted therapy, the overall survival time is extended by 3 months according to results of phase II studies.7-9 In the FOLCETUX study, at the median follow-up time of 11 months, 55.3% of patients with cetuximab in combination with FOLFIRI were alive, with a median expected survival time of 16.0 months. In the ToGA trial, a new phase III study, the median overall survival (OS) was longer for a trastuzumab combination with chemotherapy versus only chemotherapy by 2.4 months. 10 In the past 30 years, hundreds of formulae have been recorded as improving survival of AGC, but the evidence base for these formulae has not yet been evaluated. The traditional Chinese herbal medicine (TCHM, a herbal formula for invigorating spleen, formerly named Wei Chang’An), which was prescribed by practitioners of traditional Chinese medicine based on clinical experiences and pharmaceutical screening, could inhibit gastric cancer cells MKN45, SGC-7901 growth in vivo on our previous studies.11-14 But large sample controlled trial was still lacking to evaluate its efficacy. OS was considered the “gold standard.” When studies can adequately assess survival, OS is usually the preferred endpoint. 15 In this study, the possible survival benefit of TCHM treatment for AGC was addressed by using such methods as multivariate analysis while employing OS as the primary endpoint.
Methods
Patient Characteristics
Between January 1, 2001, and November 30, 2009, 399 patients were enrolled at the Department of Oncology, Longhua Hospital, Shanghai University of Traditional Chinese Medicine and the Department of surgery, Renji Hospital, Shanghai Jiao Tong University School of Medicine.
Major inclusion criteria were as follows: age 18 years or older; histologically proven gastric adenocarcinoma; stage classification and the assessment of resected specimens according to the guidelines of UICC (International Union against Cancer, 2002); Karnofsky performance status higher than 60; no prior palliative chemotherapy; adequate hepatic, renal, and hematologic function defined as indicated below: white blood cells ≥4.0 × 109/L, absolute neutrophil count ≥2.0 × 109/L, hemoglobin ≥80 g/L, platelet count ≥80 × 109/L, alanine aminotransferase <180 U/L, total bilirubin <86 µmol/L, creatinine ≤1.2 mg/dL; an expected survival of at least 3 months; no serious complication (ie, massive hemorrhage of gastrointestinal tract, complete obstruction of the digestive tract, gastrointestinal perforation, gravis icterus, non-cancer-induced fever higher than 38°C). Patients were well informed with long-term follow-up. Major exclusion criteria were as follows: concurrent cancer, pregnant or breast-feeding women, severe mental disorder, systemic administration of corticosteroids, active bacterial infection or mycosis, affecting systemic condition, unstable angina or myocardial infarction within 6 months of the trial, uncontrolled significant comorbid conditions, patients with molecular target therapy, or if patient could not comprehend the purpose of the study and could not comply with its requirements.
Treatment
In this prospective study, all patients were enrolled to either the TCHM group or the non-TCHM group.
Traditional Chinese herbal medicine formula was taken orally for 3 months or more in the TCHM group. The herbal formula for invigorating spleen (TCHM) was prescribed by practitioners of traditional Chinese medicine at the Department of Oncology, Longhua Hospital. In the TCHM formula, herbs with invigorating spleen function were the principal elements. The following primary TCHM formula in gastric cancer treatment was used: Radix pseudostellariae 12 g, Stir-fried Rhizoma atractylodis macrocephalae 12 g, Poria cocos 30 g, Sargentodoxa cuneata 30 g, Concha ostreae 30 g, Prunellae vulgaris 9 g, decoction, 2 to 4 times daily per os continuously. The herbal components in the formula had been mainly provided by 2 Chinese herbal medication factories with quality control (certified GMP). The core TCHM formula remained in all treatments; changes (herbs added) were only done based on patient’s symptoms every 2 weeks. All patients received written instruction to prepare the decoction every time they took the medication.
All patients were scheduled to receive three or more cycles of chemotherapy continuously based on fluorouracil or together with cisplatin/oxaliplatin, anthracycline or paclitaxel/docetaxel. The chemotherapy was given for 5 to 8 days every 21 to 28 days accordingly. Treatment for both groups was continued until one of the following occurred: disease progression, intolerable toxicity, patient’s withdrawal, or termination by the attending physician. All cases have been followed up and included in the final analysis.
Statistical Analysis
The primary endpoint was overall survival, defined as time from the day of histologically proven gastric adenocarcinoma or the confirmed date of recurrent/metastatic disease until death from any cause.
Follow-ups based on appointments, scheduled questionnaires, and telephone survey, were carried out till the study termination date of April 1, 2010 or outcome and endpoints were well established.
Multivariate Cox regression analysis was performed to determine survival trends adjusted for clinical and demographic factors (gender, age of onset, tumor location, histological type, cycles of chemotherapy, radiotherapy, TCHM). The baseline comparison was analyzed by using χ2 test between the TCHM and non-TCHM groups. Kaplan–Meier curves were used to assess the differences in survival time based on the baseline comparison results. The log-rank test with a 2-sided 5% significance level was used to make treatment comparisons. Data analysis was done using SPSS version 15.0.
Results
Patients
The longest follow-up period was 101.4 months and the shortest was 3.1 months. The median follow-up period was 37.6 months. The dropout rate was 5% (20/399). In 399 eligible patients (TCHM = 145; non-TCHM = 254) with locally advanced/recurrent/metastatic disease and confirmed adenocarcinoma, 305 patients (76.4%) died of disease, 93 patients (23.3%) were alive, and 1 patient (0.3%) died of unrelated cause. All the patients had no prior palliative chemotherapy. See details of baseline characteristics in Table 1.
The Details of Baseline Characteristics of Patients With Advanced Gastric Cancer.

Abbreviation: TCHM, traditional Chinese herbal medicine (herbal formula for invigorating spleen).
Survival Analysis of Overall Group
The median OS was 12.5 months for the overall group. The longest overall survival time was 101.4 months, and the shortest overall survival time was 3.1 months.
The median OS was 17.9 months for TCHM and the median OS was 8.9 months for non-TCHM (P = .000) Figure 1). Cox regression analysis showed that histological type (P = .016), radiotherapy (P = .000), cycle of chemotherapy (P = .000), and TCHM (P = .000) were independent prognostic factors. The hazard ratio (HR = Exp[β]) of TCHM was 0.493, and 95% confidence interval was from 0.384 to 0.634. See details in Table 2.
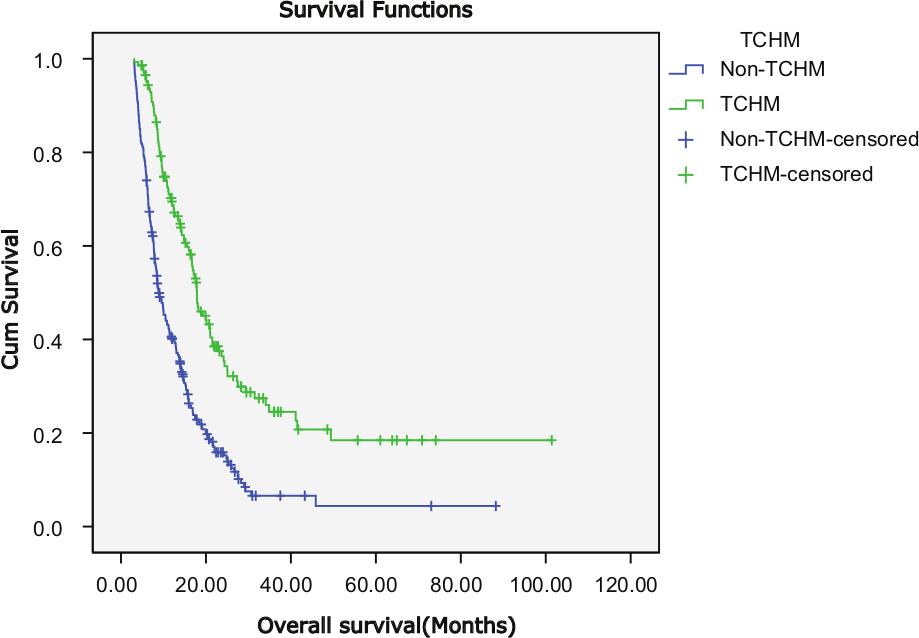
The median OS was 17.9 months for TCHM and the median OS was 8.9 months for non-TCHM (P = .000) in overall group.
Multivariate Analysis of Factors Influencing Survival of Patients With Advanced Gastric Cancer.

Abbreviations: SE, standard error; CI, confidence interval; HIST, histological type; CHEM, chemotherapy cycle; RADI, radiotherapy; TCHM, traditional Chinese herbal medicine (herbal formula for invigorating spleen).
Although Cox regression multivariate analysis suggested that TCHM was an independent prognostic factor and the median OS for TCHM was longer than that for non-TCHM, there was a significant difference in proportions in comparing chemotherapy between the TCHM and non-TCHM groups (P = .000). Therefore, we should not assess the differences in survival time between TCHM group and non-TCHM group directly. The study population divided into a subgroup of patients with 3 or more cycles of chemotherapy and a subgroup of patients with nonchemotherapy. The cases in control group of nonchemotherapy subgroup received best supportive care (see the Subgroup Analysis section).
Safety and Toxicity
The treatment was generally well tolerated. At a median TCHM invasion time of 13.1 months, there were no TCHM-related adverse events observed. No patient died related to TCHM treatment.
Subgroup Analysis
Subgroup of Patients With 3 or More Cycles of Chemotherapy
In a stratification analysis of stage for 213 patients who received 3 or more cycles of chemotherapy (98 cases in the TCHM group and 115 cases in the non-TCHM group), 60 patients (61.2%) in the TCHM group and 88 patients (76.5%) in the non-TCHM group died. Multivariate Cox regression analysis was performed to determine survival trends adjusted for clinical and demographic factors (gender, age of onset, tumor location, histological type, first chemotherapy regimen, radiotherapy, TCHM). See details of baseline characteristics in Table 3.
Details of Baseline Characteristics of Patients With Advanced Gastric Cancer in the Subgroup of Patients With 3 or More Cycles of Chemotherapy.

Abbreviation: TCHM, traditional Chinese herbal medicine (herbal formula for invigorating spleen).
Fluorouracil.
Fluorouracil plus cisplatin/oxaliplatin.
Fluorouracil plus cisplatin/oxaliplatin plus anthracycline or paclitaxel/docetaxel.
Fluorouracil plus others.
Multivariate analysis of overall survival time
Cox regression analysis suggested that only TCHM (P = .000) was an independent prognostic factor. Patients who received TCHM demonstrated better prognosis independent of other prognostic factors in multivariate analysis. The HR of TCHM in this stratification was 0.538, and 95% confidence interval was from 0.385 to 0.750. See details in Table 4.
Multivariate Analysis of Factors Influencing Survival of Patients With Advanced Gastric Cancer in Subgroup of Patients With 3 or More Cycles of Chemotherapy.

Abbreviations: SE, standard error; CI, confidence interval; TCHM, traditional Chinese herbal medicine (herbal formula for invigorating spleen).
Survival comparison
The median OS was 20.0 months for the TCHM group and the median OS was 14.0 months for the non-TCHM group. The median OS was significantly longer for TCHM versus the non-TCHM group by 6.0 months (P = .000; Figure 2).

Stratification analysis of stage for patients who received 3 or more cycles of chemotherapy showed a significant increase in median OS from 14.0 (non-TCHM group) to 20.0 (TCHM group) months (hazard ratio = 0.538; 95% confidence interval = 0.385-0.750; P = .000).
Subgroup of Patients With Nonchemotherapy
In a stratification analysis of stage for 186 patients who did not receive chemotherapy (47 cases in the TCHM group and 139 cases in the non-TCHM group), but BSC, 33 patients (70.2%) in the TCHM group and 124 patients (89.2%) in the non-TCHM group died. One patient in the non-TCHM group died of cerebral infarction. Multivariate Cox regression analysis was performed to determine survival trends adjusted for clinical and demographic factors (gender, age of onset, tumor location, histological type, radiotherapy, TCHM). See details of baseline characteristics in Table 5.
Details of Baseline Characteristics of Patients With Advanced Gastric Cancer in Subgroup of Patients With Nonchemotherapy.

Abbreviation: TCHM, traditional Chinese herbal medicine (herbal formula for invigorating spleen).
Multivariate analysis of overall survival time
Cox regression analysis suggested that radiotherapy (P = .002) and TCHM (P = .000) were independent prognostic factors. Patients who received TCHM and radiotherapy demonstrated better prognosis independent of other prognostic factors in multivariate analysis. The HR of TCHM in this stratification was 0.443, and 95% confidence interval was from 0.299 to 0.657. See details in Table 6.
Multivariate Analysis of Factors Influencing Survival of Patients With Advanced Gastric Cancer in Subgroup of Patients With Nonchemotherapy.

Abbreviations: SE, standard error; CI, confidence interval; RADI, radiotherapy; TCHM, traditional Chinese herbal medicine (herbal formula for invigorating spleen).
Baseline comparison
Baseline was compared according to multivariate analysis. According to the result of multivariate analysis in subgroup of patients with nonchemotherapy, there was no significant difference in proportions comparing radiotherapy between the TCHM group and the non-TCHM group (P = .367). Therefore, the baseline of this subgroup was equal. We assessed the differences in survival time between the TCHM and non-TCHM groups directly.
Survival comparison
The median OS was 14.8 months for the TCHM group and the median OS was 7.0 months for the non-TCHM group. The median OS was significantly longer for TCHM versus the non-TCHM group by 7.8 months (P = .000; Figure 3).

Stratification analysis of stage for patients who did not receive chemotherapy, but best supportive care, showed a significant increase in median OS from 7.0 (non-TCHM group) to 14.8 (TCHM group) months (hazard ratio = 0.443; 95% confidence interval = 0.299-0.657; P = .000).
Discussion
Gastric cancer is a multifactor and multistage process, and it is relatively difficultly to find a specific medication. Therefore, a wide consensus that combination therapy is most likely the way leading to develop new therapy strategies for gastric cancer in the future has been reached in academia.
Regimens containing fluorouracil, cisplatin/oxaliplatin, anthracycline (ECF)/docetaxel (DCF) are usually regarded as the first-line regimens of chemotherapy. The median survival time of advanced gastric cancer patients with chemotherapy ranges from 8.6 to 13.0 months.2-6 There is no difference of overall survival between different regimens of chemotherapy. Previously we had applied univariate and Cox regressions to analyze the influence of the clinical, pathological and therapeutic variables on the prognosis of gastric cancer patients. The results showed that the formula for invigorating spleen was an independent prognostic factor.16,17
For the entire group of this study, Cox regression analysis suggested that the histological type (P = .016), cycle of chemotherapy (P = .000), TCHM (P = .000), and radiotherapy (P = .000) were independent prognostic factors. The HR of TCHM was 0.493, and 95% confidence interval was from 0.384 to 0.634. There was no toxicity related to TCHM, with a median TCHM intervention time of 13.1 months.
Previous studies showed that chemotherapy or chemoradiotherapy could improve the overall survival of advanced gastric cancer patients. Chemotherapy could prolong the OS by 4.3 to 8.7 months.2-6 Postoperative chemoradiotherapy should be considered for all patients at high risk for recurrence of adenocarcinoma of the stomach or gastroesophageal junction who have undergone curative resection. 18 Our result was consistent with the results of the previous studies.
For the entire group, Cox regression multivariate analysis suggested that chemotherapy was an independent prognostic factor. Hence, the study population was divided into subgroups of patients with 3 or more cycles of chemotherapy and subgroup of patients with nonchemotherapy. In a stratification analysis, patients who received 3 or more cycles of chemotherapy, a significant increase in median overall survival from 14.0 (non-TCHM group) to 20.0 (TCHM group) months was found. For patients who did not receive chemotherapy, but BSC, Cox regression analysis suggested that radiotherapy (P = .002) and TCHM (P = .000) were independent prognostic factors. There was no significant difference comparing the proportions of patients receiving radiotherapy between the TCHM and the non-TCHM groups (P = .367). Therefore, the baseline of this subgroup was equal. Our analysis showed a significant increase in median OS from 7.0 (non-TCHM group) to 14.8 (TCHM group) months.
Based on the symptoms and characteristics of patients and guided by the theories of traditional Chinese medicine, a formula was designed to contain a combination of different kinds of plants or minerals to improve clinical efficacy. We designed a primary traditional Chinese herbal medicine formula, formerly named Wei Chang’An in the 1980s entirely based on traditional Chinese medicine theories, in which invigorating spleen herbs are the principal elements, whereas heat-clearing and detoxicating herbs, blood stasis removing herbs are adjuvant components to assist the effects of the herbal formula for invigorating spleen. The following primary TCHM formula was used: Heterophylly falsestarwort root, Stir-fried Atractylodes macrocephala, Poria cocos, and so on. The action of Heterophylly falsestarwort root was to replenish qi and invigorate the spleen function, and also to promote fluid secretion and moisten the lung. The action of Stir-fried Atractylodes macrocephala was to invigorate the function of the spleen and replenish qi, to eliminate damp by causing diuresis, to arrest excessive perspiration, and to prevent miscarriage. The action of Poria cocos was to cause diuresis, to invigorate the spleen function, and to calm the mind.
In our previous studies, it was found that the TCHM formula decoction had an inhibitory effect on the growth of both orthotopic and subcutaneous transplanted gastric cancer SGC-7901 in nude mice. Apoptosis was enhanced and cell proliferation was inhibited in human gastric cancer xenografts in nude mice after our TCHM treatment. The mechanism of invigorating spleen formula for gastric cancer is probably related to their inhibitory effect on tumor cell proliferation and induction of apoptosis in vivo. This TCHM formula induced apoptosis through the caspase-9 and caspase-3 pathway in vivo. Its mechanism might be involved in the downregulation of Stat3 and Bcl-2 genes.11-14
Although gastric cancer is a global disease, it is not uniform. There are differences in the presentation and management of patients with gastric cancer in different countries and regions. Specifically, as observed in AVAGAST, Asian patients with AGC more commonly receive second and further lines of therapy. 19 In China, almost all the patients want to choose aggressive treatments. If they have a better socioeconomic status, they would choose more expensive regimens, such as molecular targeted therapy. Traditional Chinese medicine (including TCHM formula) is less expensive in comparison to other treatments in the country, especially the expensive molecular targeted therapy.
Randomized controlled trials are considered the best evidence. Though our non–randomized controlled study limited its ability to provide robust evidence, the result of this study further revealed that TCHM (herbal formula for invigorating spleen) had positive and independent curative effectiveness for the combination therapy of advanced gastric cancer. We believe that the current study provides preliminary and powerful data to support future evaluation of TCHM in combination therapy for AGC in a large cohort, randomized clinical trial study.
Conclusions
Traditional Chinese herbal medicine (a herbal formula for invigorating spleen) has an important value for improving the prognosis of patients with AGC. It shows survival benefit for AGC. The herbal formula for invigorating spleen in this study is safe and well tolerated.
Footnotes
Acknowledgements
Many individuals from 2 institutions participated to complete this study. The representative authors are grateful for everyone’s effort.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Natural Science Foundation of Shanghai (10ZR1430400) and Ministry of Civil Affairs Foundation ((2007) 18-2-15).