
Abstract
Background:
In a previous study, we found that traditional Chinese medicine (TCM) alleviated the clinical symptoms and improved the quality of life (QoL) in patients with hepatocellular carcinoma (HCC).
Objectives:
A cohort was continuously followed up to determine the impact of the TCM adjuvant therapies on the prognosis of HCC after conventional treatments.
Methods:
We did a retrospective monocentric cohort study including 175 eligible patients. The participants who received TCM adjuvant therapies were termed as TCM group. For the purpose of stratification analysis, the patients who received TCM adjuvant therapies over 3 months per year were further classified into the high frequency group, while the rest of the TCM users were classified into the low frequency group. Non-users were recorded as the control group. The primary outcome was overall survival (OS) and the secondary outcome was the mean progression-free survival (mPFS) primarily introduced in this study, referring to the time from initial diagnosis to the latest progression over the number of disease progressions. Analyses used Cox proportional hazards and Kaplan-Meier (K-M) methods, adjusted for stratification factors.
Results:
Until June 30, 2021, 56 patients survived, 21 patients were lost to follow-up, and 98 patients died from the disease. Each disease progression of every individual was recorded, and most of the PFS was within 1 year. The baseline data of the allocated groups were balanced, the result revealed that TCM adjuvant therapies might have little influence on OS (P = .129). However, the 1, 3, and 5-year progression-free survival rates of the patients in TCM and control group were 68.75%, 37.50%; 25.00%, 8.33% and 8.33%, 2.08%, respectively, indicating TCM use significantly extended the mPFS, and decreased the risk of disease progression by a factor of 0.676 (P = .006). In the patients with BCLC stage B HCC, compared with controls, a 37-month median OS advantage in the high frequency group was noted (P = .045); and the high frequency of TCM use significantly suppressed disease progression (P = .001).
Conclusions:
The present study revealed that TCM adjuvant therapies could postpone disease progression in HCC. Furthermore, using TCM over 3 months per year might extend OS in patients with intermediate HCC.
Keywords
Introduction
Hepatocellular carcinoma (HCC) remains threatening human health worldwide significantly. 1 Hepatic resection and liver transplantation were deemed to be the potential radical therapies. 2 Even if the demands for treatment were satisfied, the prognosis was still poor with a recurrence rate of up to 70% within 5 years after the curative therapies. 3
Traditional Chinese medicine (TCM) has a unique system info influenced by the theory of Yin-yang and 5 elements in ancient times. It’s reported that TCM use could diminish the adverse events of conventional therapies, 4 and improve the patients’ quality of life (QoL) in HCC. 5 Taking Chinese herbal medicine was observed to profoundly lower HCC risk in patients with chronic hepatitis B. 6
In the previous study, we found that the Huqi Formula could ameliorate the clinical symptoms and improve QoL in patients with HCC after trans-hepatic arterial chemotherapy embolization (TACE). 7 Some participants demanded to take the Huqi Formula or other Chinese patent medicines (CPMs) as alternative therapies after the study before and after conventional therapies. As the cohort was followed up over 5 years, we intended to dissect the role of TCM use in the prognosis of the candidates. The primary outcome was overall survival (OS), and the secondary outcome was the mean progression-free survival (mPFS), which was primarily introduced in this study, referring to the time from the initial diagnosis to the latest progression over the number of disease progression. It is well known that the Barcelona Clinical liver cancer (BCLC) staging system has crucial guiding significance on prognosis and options of treatment regimen in HCC. 8 Patients with intermediate HCC (BCLC B), whose outcomes are less disappointing than those with advanced HCC, whereas more challenging than the early ones, particularly attracted our attention. Given that the high frequency of TCM utilization might benefit this group, we did a stratification analysis to preliminarily locate how to apply TCM to this potentially suitable audience. In this study, we simply verified the positive significance of the TCM adjuvant therapies in HCC, while the underlying molecular mechanism still needs to be exploited; therefore, we listed the representative drugs used to provide a reference for potential further research.
Materials and Methods
Participants
The patients were enrolled from 2013 to 2016 at Beijing YouAn Hospital, Capital Medical University. And the cohort was established to prospectively determine the influence of the Huqi Formula, a traditional Chinese medicine decoction, on QoL in HCC in the National Science and Technology Support Program (2013BAll3804). During the observation, all the conventional treatments were strictly conducted according to the guidelines.9-11 We kept following up with the participants, tracing their disease progression, conventional therapeutic approaches and the medication administration of TCM. To further illustrate the effect of the TCM drugs on prognosis in the patients, we retrospectively collected the data on the course of the disease and therapeutic methods by searching the attendance system of the hospital and checking back on patients by phone. The starting point of this research was the time of initial diagnosis instead of the time of enrollment, and the deadline was June 30, 2021, or death, or loss of contact.
Inclusion and Exclusion Criteria
The inclusion criteria were: (1) The patients were diagnosed with HCC through pathology or imaging methods based on multiphasic CT or dynamic contrast-enhanced MRI. The classification of the disease endorsed the BCLC staging system. (2) The range of age should be 18 to 85.
The exclusion criteria were: (1) Patients with severe cardiovascular or cerebrovascular diseases, kidney diseases, hematological diseases, endocrine diseases, pulmonary diseases, neuropsychiatric disorders, or other serious diseases significantly affecting survival; (2) Secondary HCC; (3) Pregnant or lactating women; (4) Patients who are prone to allergic reactions or allergic diseases should not be incorporated to avoid Chinese medicine allergic reactions.
Selection Process
A total of 299 patients were enrolled in this study initially. After eliminating the individuals without complete information about the initial diagnosis, 175 participants were incorporated into the analyses. The patients who received TCM as adjuvant therapy were termed as the TCM group, while the non-users were recorded as the control group. The distribution of baseline data was uneven between the 2 groups. Propensity score matching (PSM) was performed with the nearest neighboring method in a 1:1 ratio according to age, sex, BCLC staging, Child-Pugh score, level of AFP, and conventional therapy. A subgroup of 96 matched subjects was formed to investigate the effect of TCM use on patients’ survival. Additionally, to determine the influence of different frequency of TCM use on survival in intermediate-stage HCC (BCLC B) (n = 100) (Figure 1), the patients who received TCM adjuvant therapies for over 3 months per year were further classified into the high frequency group, while the rest of the TCM users were classified into the low frequency group in accordance with their actual TCM consumption. Stratification analysis was performed.

Flow diagram of study selection process.
The Drugs of TCM Therapies
The TCM therapies applied in this study included 2 parts: the Huqi formula and CPMs. The Huqi formula was an experiential prescription created by a prestigious Chinese physician, which contains 8 herbs, Viscum coloratum (Kom.) Nakai, Astragalus membranaceus, Salviae miltiorrhizae, Hedyotis diffusa, Rhizoma Curcumae, Curcuma aromatica, fruits of Polygonum orientale, and Sophora flavescens. The herbs were all high-quality products selected by professional herbalists, then processed by the manufacturing laboratory in Beijing YouAn Hospital, Capital Medical University. The CPMs prescribed for the patients were all approved by the national medical products administration. It should be noted that the latest guidelines (China) proposed that TCM treatment could be used in HCC if necessary. The Jinlong capsule, Huaier granule, Ganfule capsule, Fufang Banmao capsule, Brucea javanica oil soft capsule, Cidan capsule, and Huachinopadin capsule were recommended, 12 which were the CPMs used in this study.
Statistical Analysis
Statistical analyses applied SPSS (version 23.0; IBM, NY, USA) and GraphPad (GraphPad Software Inc., San Diego, CA, USA). The variables were expressed as means ± SD for continuous data and as frequencies (percentages) for categorical data. Kaplan-Meier (K-M) method was performed to reflect survival and mortality of the patients, and the difference was examined by log-rank test. Cox proportional hazards method was used to recognize the prognostic factors and calculate the hazard ratio (HR). To compare the distribution of variables among multiple samples, t-test, one-way ANOVA, chi-square test, and Kruskal-Wallis (H) test were applied. Statistical significance was set at P < .05.
Ethical Considerations
The study was approved by the Ethics Committee of Beijing YouAn Hospital, Capital Medical University (京佑字2014 [13]号). All the patients provided written informed consent to participate in the study and publication of the data.
Results
Clinical Characteristics
The number of the patients at BCLC stages A, B, C, and D were 46, 100, 27, and 2, respectively. There were 104 patients diagnosed through histopathology, and the rest of the patients were diagnosed based on imaging. And 39 patients received hepatectomy or hepatectomy combined with other therapies, such as TACE, radiofrequency ablation (RFA), and sorafenib; 31 patients received single non-hepatectomy therapy, including TACE, RFA, Ar He cryoablation; the rest ones received combined non-hepatectomy therapies, for instance TACE incorporated with RFA. Among all the participants, 123 (70.29%) patients received TCM as adjuvant therapy. The general data are presented in Table 1.
Clinical Characteristics.

Disease Progression
By the end of the study, 56 patients survived, 21 patients were lost to follow-up, and 98 patients died from HCC. We recorded each disease progression, including local recurrence, new intrahepatic lesions and distant metastasis recognized by abdominal MRI or enhanced CT, calculating PFS. This revealed that most of the PFS were within 1 year (Figure 2). Among the patients died from HCC, 40 participants suffered progression more than once, and of these, 26 patients were diagnosed with intermediate HCC.

The distribution of recurrence according to PFS. The colors indicate the sequence of progression, and the height indicates the number of the patients.
TCM Adjuvant Therapies Improved the mPFS in HCC
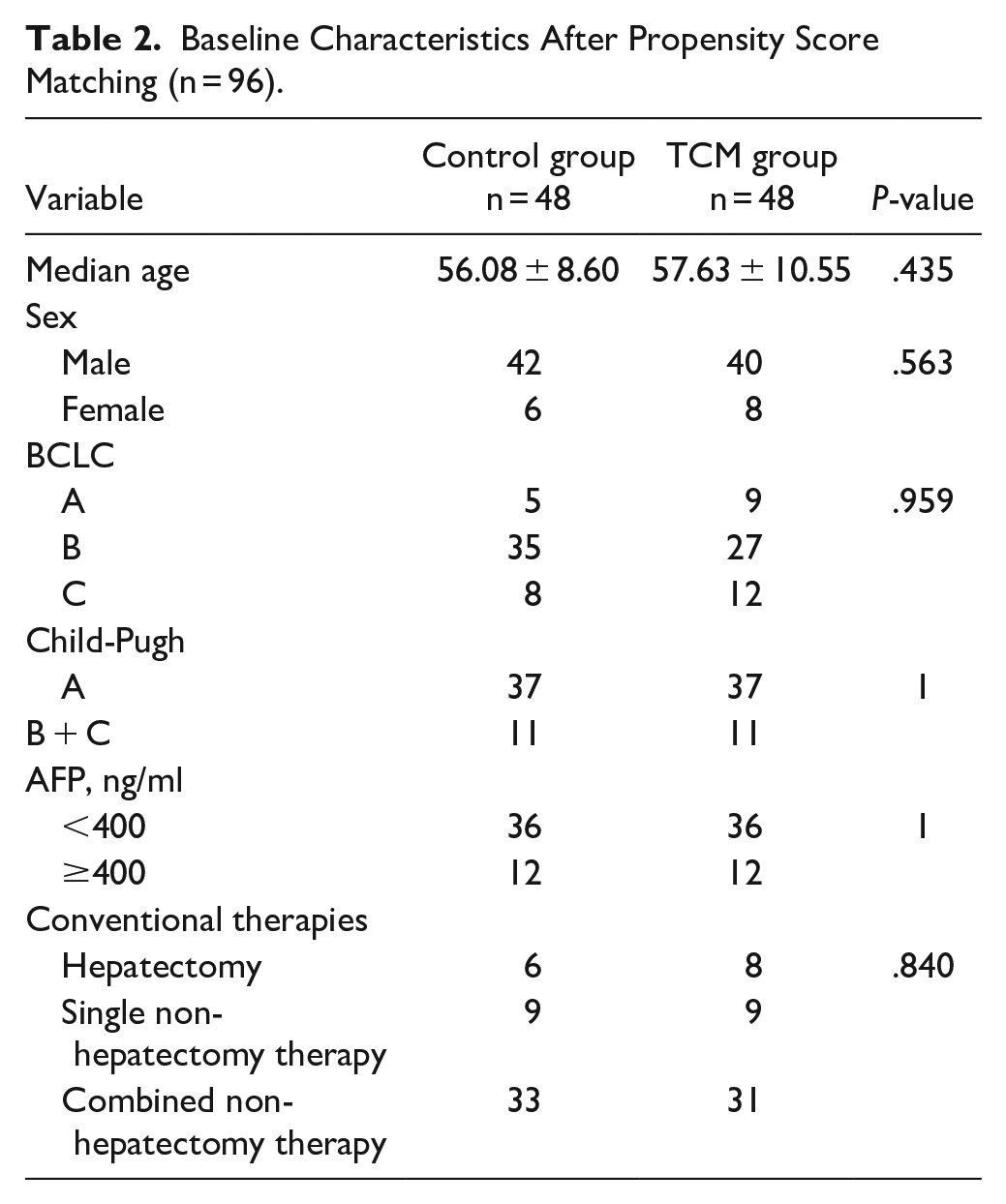
The matched baseline data showed no statistical difference between the 2 groups (Table 2). Since most of the patients experienced repeated disease progressions, the mean PFS (mPFS) was introduced for the first time in this study. This refers to the time from the initial diagnosis to the latest progression over the number of progressions for the purpose of reflecting PFS more logically during the long course of the illness.
Baseline Characteristics After Propensity Score Matching (n = 96).
The 1, 3, and 5-year survival rates of the patients in the TCM and control groups were 87.50% versus 81.25%; 68.75% versus 37.50%; and 39.58% versus 25.00%; which showed no statistically significant difference (P = .129) (Figure 3A). The 1, 3, and 5-year progression-free survival rates of the patients in the TCM and control groups were 68.75% versus 37.50%; 25.00% versus 8.33%; and 8.33% versus 2.08%, respectively. The results confirmed that TCM use significantly extended the mPFS, decreasing the risk of disease progression by a factor of 0.676 compared to the control group (P = .006) (Figure 3B).

Overall survival and progression-free survival in the TCM and control group. (A) Overall survival in the 2 groups. (B) Progression-free survival in the 2 groups.
The results of the univariate Cox proportional hazards method showed that neither age nor sex had a statistical influence on OS or mPFS. In consideration of the clinical application, BCLC staging, Child-Pugh score, the level of AFP, conventional therapy, and TCM adjuvant therapy were incorporated into the following multivariate Cox proportional hazards method to detect the factors affecting survival. This analysis indicated that advanced BCLC staging shortened OS and mPFS notably, and that the patients who received hepatectomy had the lowest mortality risk. Furthermore, the result likewise supported that TCM adjuvant therapies dramatically delayed disease progression in HCC (Table 3).
Cox Proportional Hazards Analysis for OS and mPFS (n = 96).

High Frequency of TCM Use Improved OS and the mPFS in Intermediate HCC
The K-M method revealed that TCM therapies significantly prolonged mPFS (P = .004) (Figure 4B), whereas they had little influence on OS (P = .099) (Figure 4A) in the patients with BCLC stage B HCC. The frequency of TCM use was then stratified into 4 levels based on the actual use of TCM medications, from 1 to 4 quarters of a year. The numbers of patients in each level were 33, 12, 4, and 8. We further separated the TCM users into low and high frequency groups demarcated at 3 months per year, while the non-users were recorded as the control group. It was determined that distribution of the baseline data was balanced among the 3 groups (Table 4).

Overall survival and progression-free survival in the TCM and control group in intermediate HCC. (A) Overall survival in the 2 groups. (B) Progression-free survival in the 2 groups.
Baseline Characteristics Among the 3 Groups.

The 1, 3, and 5-year survival rates of the patients in the high frequency group, low frequency group, and control group were 92.59%, 86.11%, and 83.78%; 81.48%, 52.78%, and 35.14%; and 55.56%, 36.11%, and 27.03%, respectively. Compared with controls, a 37-month median OS advantage in the high frequency group was noted (P = .045) (Figure 5A).

Overall survival and progression-free survival in the high, low frequency and control group in intermediate HCC. (A) Overall survival in the 3 groups. (B) Progression-free survival in the 3 groups.
The 1, 3, and 5-year progression-free survival rates of the patients in the high frequency group, low frequency group and control group were 70.37%, 55.56%, and 32.43%; 29.63%, 22.22%, and 8.11%; and 18.52%, 13.89%, and 2.70%, respectively. Analyses found the median mPFS of the patients in the high, low frequency and control groups were 18, 12, and 9 months, indicating the high frequency of TCM use significantly suppressed disease progression in the patients with intermediate HCC (P = .001) (Figure 5B).
The Composition of the TCM Therapies
Among these 175 patients, 13 received the Huqi Formula alone, 48 received CPMs alone and 62 received TCMD combined with CPMs. Almost every individual was prescribed no less than 1 CPM during the long term of therapies. The top 5 CPMs administered in this study were Jinlong capsule, Ganfule capsule, Demethylcantharidin Tablets, Huaier granule, and Fufang Banmao capsule (Figure 6). The Huqi formula and the CPMs used in this study shared several drugs, as demonstrated in Table 5, and the prime effective ingredient was also listed. The CAS (Chemical Abstracts Service) number was collected from PubChem (https://pubchem.ncbi.nlm.nih.gov/).

The top 5 CPMs used in this study. Jinlong Capsule was the most widely used one with 58 consumers.
The Representative Drugs Used in This Study.

Discussion
The effect of TCM on prognosis in HCC has attracted more attention in the past few years. A randomized controlled clinical trial involving 291 HCC patients found that TCM combined with TACE significantly prolonged PFS and OS. 13 A retrospective study including 3483 patients with HCC indicated that TCM therapy was an independent protective factor for 5-year survival. 14 The definition of HCC pertains to the scope of the ZhengJi in TCM, which refers to the chronic abdominal mass accompanying and resulting in the sthenia of pathogens and the asthenia of the vital Qi in patients. Therefore, the cardinal principle of the therapeutic approach was chiefly categorized into 2 types, strengthening the integrity and eliminating pathogens, which could be further divided into multiple methods minutely targeting the diverse specific syndromes. It has the same approach as the individualized treatments used in precision medicine. 15
The therapeutic principle of the Huqi Formula was benefiting Qi-blood, resolving toxin and removing blood stasis, which was proven effective in ameliorating liver injury and QoL in HCC. 7 The Jinlong capsule was the most commonly used CPM in our study. A meta-analysis showed that the Jinlong capsule could improve the patients’ liver function, quality of life and immune function, and decrease adverse events related to TACE, including leucopoenia, gastrointestinal side effects, hepatotoxicity, and myelosuppression. 16 A multi-center, randomized, controlled, phase IV trial, including 1044 patients, found that Huaier granule, another CPM used in this study, could prolong the recurrence-free survival and reduced extrahepatic recurrence in HCC after curative liver resection. 17 From the TCM perspective, the Jinlong capsule aims to eliminate pathogens, whereas the Huaier granule strengthens the integrity. This study confirmed that TCM remedies significantly postponed disease progression.
The TCM therapies lay emphasis not merely on the tumor but also the environment of the cirrhotic liver, gradually ameliorating liver condition through TCM administration. Hence, TCM doctors deem the treatment should be a long-term one. In this study, patients with BCLC stage B were the dominant population. The results validated that advanced BCLC staging was unfavorable for OS and mPFS (Table 3). As some patients experienced multiple recurrences during the observation, we proposed the definition of mPFS, attempting to describe the time free from disease progression better. Moreover, the outcomes indicated that high frequency TCM use might extend not only mPFS but also OS in intermediate HCC.
Generally speaking, our preliminary research verified the positive significance of TCM adjuvant therapies in HCC, whereas the underlying molecular mechanism remains obscure due to the complexity of the multifarious ingredients. At the same time, there is published research about the representative drugs used in this study. It is reported that Astragaloside IV, an active component of Astragalus membranaceus could inhibit the migration and viability of HCC cells via downregulating lncRNA-ATB. 18 Another research found that Astragaloside IV could delay the occurrence of primary HCC in C57BL/6J mice by regulating the pSmad3C/3L and Nrf2/HO-1 pathways. 19 β-Elemene is the efficient ingredient of Rhizoma Curcumae, and it is reported that β-Elemene could suppress HepG2 growth through downregulating LncRNA HOTAIR, SP1, and PDK1. 20 Tanshinone IIA, an extract of Salvia miltiorrhiza, could initiate HepG2 apoptosis and cell cycle arrest at the G1 checkpoint, and it may induce HCC cell death through the miR30b-p53-PTPN11/SHP2 pathway. 21 As for in vivo study, Tanshinone IIA could inhibit the HCC metastasis associated with palliative resection and the underlying mechanism might be promoting VEGFR1/PDGFR-related vascular normalization. 22 Cantharidin (CTD) is a terpenoid obtained from Mylabris phalerata, its derivative magnesium demethylcantharidate could significantly inhibit the invasion and metastasis of HCC cells by activating transcription factor FOXO1. 23 Amygdalin, an active component of Prunus persica 24 might promote apoptosis in HepG2 though the mitochondria-initiated pathway and cell cycle arrest at G/M. 25 Quercetin is an efficient ingredient of Scutellaria barbata, and it could induce EB-mediated lysosome activation and increase ferritin degradation, leading to ferroptosis and Bid-involved apoptosis in several kinds of tumor cells including HepG2. 26 Curcumin is an efficient ingredient of Curcuma aromatica, 27 which could repress proliferation, migration, and invasion of HCC cells by regulating miR-21-5p and SOX6. 28 We have just listed the tip of the iceberg of relevant studies, aspiring to provide a reference for potential further research.
Conclusion
This work revealed that the TCM adjuvant therapies could postpone disease progression in HCC. What’s more, using TCM over 3 months per year might prolong OS in patients with intermediate HCC.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Beijing Natural Science Foundation (7212171) and China Postdoctoral Science Foundation (2021M702312).