
Abstract
Keywords
Introduction
Pancreatic cancer is a highly malignant tumor, and only about 20% of patients are eligible for surgical resection. 1 The median postoperative survival time is 15 to 19 months, and the 5-year survival rate is 20%. 2 The survival time for advanced pancreatic cancer is only 5 to 7 months. 3 Traditional Chinese herbal medicine (TCHM) has certain effects in prolonging the survival time and improving the quality of life in patients with pancreatic cancer. This study was a retrospective matched case-control study on pancreatic cancer patients to assess the factors that affect the survival time of patients with pancreatic cancer.
Methods
Patient Characteristics
From April 1, 2004, to September 30, 2012, pancreatic cancer patients who underwent treatment at the Department of Oncology, Longhua Hospital, Shanghai University of Traditional Chinese Medicine; Department of Surgery, Renji Hospital, Shanghai Jiao Tong University School of Medicine; and Department of Interventional Therapy, Zhongshan Hospital, Shanghai Fudan University were recruited for the study.
Diagnoses were made by surgical pathology or cytology according to the Guidelines for Diagnosis and Treatment of Pancreatic Cancer developed by the Ministry of Health (2011) and Clinical Practice Guidelines for Pancreatic Cancer developed by National Comprehensive Cancer Network (2013), and TNM staging was performed according to the guidelines of American Joint Committee on Cancer (2010). The diagnosis of Chinese Medical Differentiation was splenic deficiency, according to the “National Standard Terminology/Chinese Medicine Clinical Diagnosis and Treatment Terminology GB/T16751.2-1997” and the Guidelines for Clinical Studies of New Chinese Medicine (Chinese Medical Science and Technology Press, 2002). The main manifestations were abdominal bloating and reduced dietary intake; aggravated abdominal bloating after meals; loose stools; fatigue; lassitude; weak breath; either emaciation, obesity, or edema accompanied by dull complexion, pale tongue, and coating on the tongue; and slow and weak pulse.
Major inclusion criteria were the following: 18 years or older; either gender; pathologically proven pancreatic cancer, with complete TNM staging information; Karnofsky Performance Scale (KPS) score ≥60; adequate hepatic, renal, and hematological function; estimated survival time of 3 months or more; and complete disease, treatment, and follow-up information. The patients also had to be TCHM group patients receiving consecutive TCHM treatment at our department for 3 months or more. Major exclusion criteria were the following: pathological classification as neuroendocrine tumor, incomplete TNM and clinical staging information, and 2 or more types of tumors. Pregnant and lactating women, children, and mentally ill patients and those who had severe acute and chronic diseases that could significantly affect treatment and prognosis, such as cardiovascular and cerebrovascular disease, severe liver and kidney dysfunction, and severe postoperative complications, were also excluded.
Treatment
In this retrospective study, patients received Western medicine treatment in any of the 3 hospitals and were self-selected to receive TCHM treatment in our department. Thus, patients were divided into combined traditional Chinese medicine group (TCHM group) and Western medicine only group (non-TCHM group, control group) based on whether they received TCHM compounds at our department or not.
In the primary study, we found that baseline radiotherapy and chemotherapy were significantly unequal between the 2 groups, so we made a further paired match of the recruited patients. The match was done based on the following: gender, age of onset (<65, ≥65 years), and consistency in radiotherapy and chemotherapy.
The TCHM group received the TCHM spleen-invigorating compound for 3 consecutive months or more. The basic prescription was: Radix pseudostellariae, 12 g; fried white atractylodes rhizome, 12 g; poria, 30 g; Rhizome pinelliae Preparata, 9 g; green dried tangerine peel, 4.5 g; pericarpium citri reticulatae viride, 4.5 g combined with raw oysters 30 g; Prunella, 9 g; Curcuma zedoaria, 9 g; Sargent gloryvine, 30 g; and black nightshade, 30 g, decocted, 2 to 4 times daily orally. This core formula remained in all treatment periods; additional changes were made once every 1 to 2 weeks according to patients’ symptoms of Chinese Medical Differentiation Treatment Standard. These herbs were purchased and decoction prepared by Traditional Chinese Medicine Herbal Pharmacy of Longhua Hospital, which is licensed by the Good Manufacturing Practice and has prepared the decoction in previous studies. 4
Both groups received Western medicine treatments, including the following: surgery (R0 resection, palliative resection, bypass surgery, biopsy), intravenous chemotherapy (gemcitabine, oxaliplatin, fluorouracil, capecitabine monotherapy or combination therapy), regional arterial infusion chemotherapy (delivered to the lesions via the superior mesenteric artery and/or the celiac artery), radiation therapy (3-dimensional conformal radiotherapy and γ-ray stereotactic radiation therapy), and other treatments (Chinese patent drug therapy, molecular targeted therapy, immune therapy).
Study End Point and Assessment
The primary end point was overall survival (OS), defined as time from the date of definitive diagnosis to the date of death by any cause. Secondary end points were disease-free survival (DFS), defined as the date from definitive diagnosis to the date of disease recurrence or death caused by any cause, and 1-, 2-, 3-, and 5-year survival rates.
Before inclusion, general clinical tests, including routine blood, urine, and stool tests; occult blood tests; tests to determine liver and kidney function; electrocardiograms; and computed tomography/magnetic resonance imaging were performed. Tumor markers such as CA199 were tested once in 3 months, and abdominal computed tomography/magnetic resonance imaging and chest X ray were obtained every 3 to 6 months. Follow-ups were performed in the clinic, by mail, or by telephone and continued until April 30, 2014, or to the end-point event. For patients who were lost to follow-up, the end of the study was the date of the latest contact.
Statistical Analysis
Multivariate Cox regression analysis was performed to determine survival trends adjusted for clinical and demographic factors (gender, age of onset, primary tumor site, stages, KPS, radiotherapy, chemotherapy, TCHM). The baseline comparison was analyzed using the χ2 test between the TCHM and non-TCHM groups. The Kaplan-Meier method was used to estimate OS and DFS, and the log-rank test was used to make treatment comparisons. The life-table method was used to estimate the 1-, 2-, 3-, and 5- year survival rates. Statistical analyses were performed using SPSS 16.0 software (SPSS, Chicago, IL), and P <.05 was considered statistically significant.
Results
Patient Information
A total of 411 patients with pathologically confirmed stage I to IV pancreatic cancer were enrolled in the study. The primary study showed significant differences in baseline radiotherapy and chemotherapy between the 2 groups, so the patients were further matched according to the matching rules mentioned above, and 136 pairs (272 cases) of patients were included in this study. Among the 272 patients, all patients survived at least 3 months; study end points occurred in 229 cases (84.2%), and 8 were lost to follow-up (2.9%). The duration of follow-up was 3.1 to 119.6 months. The OS was 17.4 months and 11.3 months in the TCHM and non-TCHM groups, respectively (Figure 1). COX analysis revealed that KPS (P = .000), radiotherapy (P = .031), and TCHM (P = .000) were independent prognostic factors for the OS of pancreatic cancer patients. The hazard ratio (HR) of TCHM treatment was 0.458 (95% confidence interval [CI] = 0.349-0.601). The patients were divided into the advanced disease group and the post–radical surgery group for further analysis.

Median overall survival of all patients with pancreatic cancer.
Advanced Pancreatic Cancer
A total of 130 patients (65 pairs) with pathologically confirmed advanced pancreatic cancer were included in this part of the study. Study end points occurred in 53/65 (81.5%) patients in the TCHM group, and 3 (4.6%) were lost to follow-up. The median duration of follow-up was 11.5 months. In the non-TCHM group, study end points occurred in 63/65 (96.9%) patients, and 2 (3.0%) were lost to follow-up. The median duration of follow-up was 9.9 months. A χ2 test did not show significant differences in baseline values of the 2 groups (Table 1). COX analysis indicated that KPS (P = .000), radiotherapy (P = .003), and TCHM (P = .001) were independent prognostic factors for OS in advanced pancreatic cancer. The HR of TCHM treatment was 0.520 (95% CI = 0.353-0.766; Table 2).The OS was 12.7 and 9.9 months in the TCHM and non-TCHM groups, respectively (P = .033, log-rank test; Figure 2). The 1-, 2-, 3-, and 5-year survival rates were 47%, 21%, 18%, and 12%, respectively, in the TCHM group and 34%, 8%, 3%, and 2%, respectively, in the non-TCHM group.
Baseline Characteristics of Patients With Advanced Pancreatic Cancer. a

Abbreviations: TCHM, traditional Chinese herbal medicine; KPS, Karnofsky Performance Scale.
TCHM group versus non-TCHM, χ2 test.
Multivariate Analysis of OS in Patients With Advanced Pancreatic Cancer.

Abbreviations: OS, overall survival; SE, standard error; CI, confidence interval; KPS, Karnofsky Performance Scale; TCHM, traditional Chinese herbal medicine.

Median OS of patients with advanced pancreatic cancer.
Pancreatic Cancer After Radical Surgery
A total of 142 patients (71 pairs) with pancreatic cancer who underwent radical resection were included in this part of the study. Study end points occurred in 45/71 (63.4%) patients in the TCHM group, and 2 (2.8%) were lost to follow-up. The median duration of follow-up was 22.5 months. Study end points occurred in 68/71 (95.7%) of the non-TCHM group; 1 (1.4%) was lost to follow-up; and the median duration of follow-up was 12.4 months (Table 3).
Baseline Characteristics of Patients With Pancreatic Cancer Post–Radical Surgery. a
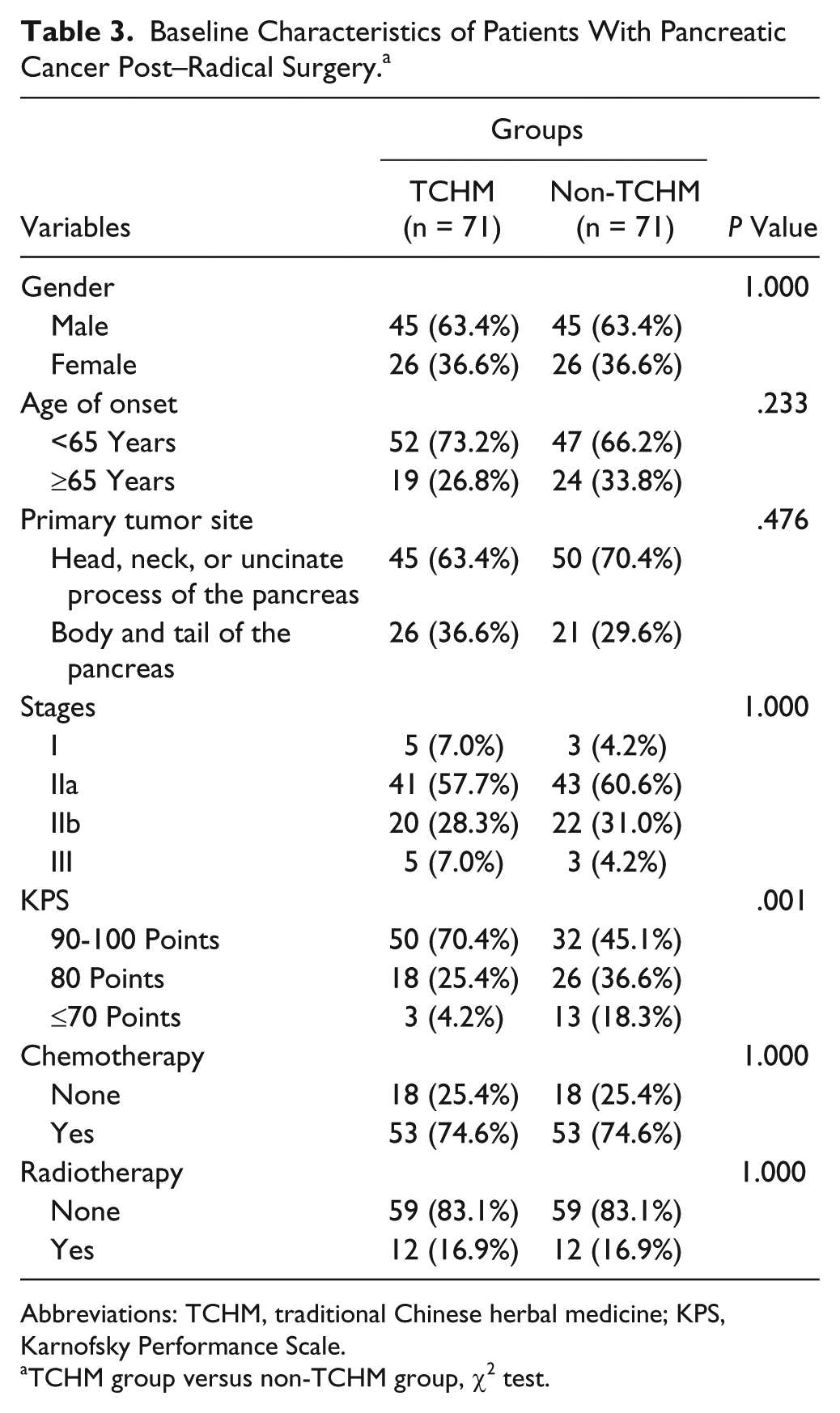
Abbreviations: TCHM, traditional Chinese herbal medicine; KPS, Karnofsky Performance Scale.
TCHM group versus non-TCHM group, χ2 test.
COX analysis indicated that KPS (P = .000) and TCHM (P = .000) were independent prognostic factors for OS in post–radical surgery pancreatic cancer patients. The HR of TCHM treatment was 0.373 (95% CI = 0.251-0.554, Table 4). The OS was 23.8 months and 12.4 months in the TCHM and non-TCHM groups, respectively (P = .000, log-rank test; Figure 3). The 1-, 2-, 3-, and 5-year survival rates were 81%, 50%, 34%, and 28%, respectively, in the TCHM group and 46%, 14%, 10%, and 2%, respectively, in the non-TCHM group.
Multivariate Analysis of OS and DFS in Patients With Pancreatic Cancer Post–Radical Surgery.

Abbreviations: OS, overall survival; DFS, disease-free survival; SE, standard error; CI, confidence interval; KPS, Karnofsky Performance Scale; TCHM, traditional Chinese herbal medicine.

Median overall survival of patients with pancreatic cancer post–radical surgery.
COX analysis indicated KPS (P = .000) and TCHM (P = .000) were independent prognostic factors for DFS in post–radical surgery pancreatic cancer patients. The HR of taking the TCHM was 0.352 (95% CI = 0.237-0.522; Table 4). The DFS was 21.5 months and 10.2 months in the TCHM and non-TCHM groups, respectively (P = .000, log-rank test; Figure 4).

Median DFS of patients with pancreatic cancer post-radical surgery.
Discussion
Pancreatic cancer has a high degree of malignancy, rapid progression, and high mortality. Progress has been made in the diagnosis and treatment of pancreatic cancer in recent years, and available treatment options have increased. However, the improvement of OS is not significant. Seeking multidisciplinary treatment is the trend for the treatment of pancreatic cancer. This study retrospectively analyzed 272 pathologically confirmed pancreatic cancer cases from 2004 to 2012 and assessed the effects of spleen-invigorating compounds on the survival time of pancreatic cancer patients.
In the present study, the KPS score was an independent prognostic factor of OS in both post–radical surgery and advanced pancreatic cancer. Physical conditions have an important impact on the survival of pancreatic cancer patients. Storniolo et al 5 reported that KPS was an important prognostic factor in pancreatic cancer patients receiving gemcitabine. Other studies also showed that low KPS scores and poor overall condition indicated a bad prognosis.6,7 A number of chemotherapy regimens have specific requirements for patients’ physical condition, especially 3-drug regimens such as FOLFIRINOX, which have a higher requirement for physical conditions.
Meanwhile, the study showed that in post–radical surgery patients, the OS of the non-TCHM group was slightly shorter than the average level reported in other studies, and on the basis of relevant postsurgery stage, radiotherapy, and chemotherapy in the 2 groups, the OS of the TCHM group was significantly longer than that of the non-TCHM group. One possible reason might be that the overall KPS status of the non-TCHM group was poor (45.1%, 36.6%, and 18.3%, respectively), whereas the TCHM group had more patients with KPS scores of 90 to 100 and 80 and fewer with KPS ≤70 points (70.4%, 25.4%, and 4.2%, respectively), a difference that was statistically significant (P = .001).
Radiotherapy was also an independent prognostic factor for OS in advanced pancreatic cancer in the present study. A British multicenter, single-arm study suggested that gemcitabine in combination with oxaliplatin and 3-dimensional stereotactic radiotherapy induced by safe doses of fluorouracil was feasible in patients with locally advanced pancreatic cancer and could be tolerated, gaining a median OS of 15.7 months. 8 A systematic analysis by Huguet et al 9 suggested that gemcitabine-based chemotherapy and radiotherapy could be selected for locally advanced pancreatic cancer and that induction chemotherapy followed by sequential radiochemotherapy is a promising strategy for patients without early metastasis or progression.
The present study showed that the TCHM spleen-invigorating compound was an independent prognostic factor for OS in patients with both advanced and post–radical surgery pancreatic cancer. TCHM prolonged the OS of advanced pancreatic cancer patients from 9.9 to 12.7 months (P = .033; HR = 0.520; 95.0% CI = 0.353-0.766). It also contributed to a longer OS and DFS in post–radical surgery pancreatic cancer patients. OS was 23.8 and 12.4 months in the TCHM and non-TCHM groups, respectively (P = .000; HR = 0.373; 95.0% CI = 0.251-0.554), and DFS was 21.5 and 10.2 months in the TCHM and non-TCHM groups, respectively (P = .000; HR = 0.352; 95% CI = 0.237-0.52).
In traditional Chinese Medicine theory, the spleen is believed to be responsible for transporting water and grain essence and liquid distribution as well as the original source of human vital energy and blood. Symptoms of pancreatic cancer, including loss of appetite, nausea, vomiting, loose stools, diarrhea, weight loss, epigastric mass, and jaundice, are consistent with those caused by “insufficiency of the spleen” according to Chinese medicine theory. On one hand, TCHM spleen-invigorating compounds focus on the pathogenesis of pancreatic cancer, support positive vital energy, and fight against unhealthy environmental influences that cause disease; on the other hand, restoring spleen health and function may enhance the vital energy and blood function and improve physical conditions to allow patients to tolerate more antitumor treatments. Previous laboratory studies have shown that the TCHM spleen-invigorating compound adopted in this study has effects on multiple digestive tract malignancies, including pancreatic cancer, stomach cancer, colon cancer and others. It can resist mutagenic effects and induce apoptosis of human gastric cancer cells, inhibit cell proliferation, and affect the expression of certain cancer-related genes. 10 Furthermore, it can inhibit mutation of P53 during the growth process of Lovo transplantable tumor 11 and significantly inhibit the growth of human pancreatic cancer BxPC-3 cell line subcutaneous xenografts in nude mice. In addition, it is effective in improving the survival rate and quality of life of pancreatic cancer patients. 12
In the present study, the TCHM spleen-invigorating compound had a positive effect on pancreatic cancer patients, as seen in former studies, and the mechanism suggests that it could be further researched in the laboratory. Radiotherapy and the TCHM spleen-invigoration compound were both independent prognostic factors for advanced pancreatic cancer patients, suggesting that the TCHM spleen-invigorating compound could prolong OS in advanced pancreatic cancer and enhance toleration of anticancer treatments. The combination may result in longer survival time.
Systemic adjuvant chemotherapy has been proven to improve the survival rate of pancreatic cancer patients after surgery,13,14 and palliative chemotherapy could prolong the OS of advanced pancreatic cancer patients by 8.5 to 11.1 months.15-18 In the present study, chemotherapy failed to be an independent prognostic factor for OS in pancreatic cancer patients. This may result from our having grouped local interventional chemotherapy treatment and systemic chemotherapy treatment together for purposes of statistical analysis, which might obscure the effects of either type of treatment.
In summary, multidisciplinary and comprehensive treatments of pancreatic cancer are recommended. KPS was an important prognostic factor of pancreatic cancer, and TCHM spleen-invigorating compounds could improve the prognosis of pancreatic cancer patients. Combined with appropriate systemic radiotherapy and/or chemotherapy, it might further prolong the survival time. Randomized controlled trials are considered the best evidence. This retrospective, matched case-control study had equal baseline values on most variables between the 2 groups. However, it still had some bias. The fact that patients were self-selected to take TCHM treatment and that some patients with higher KPS were in the TCHM group limited the ability of this study to provide more robust evidence. Our results showed that TCHM spleen-invigorating compounds may be a positive option for pancreatic cancer patients, and we have planned to carry out well-designed, prospective clinical and randomized controlled studies in the near future.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by Shanghai Municipal Hospital New Developing and Leading Edge Technology Project (SHDC12010120) and Shanghai Health System Excellent Subject Leader Developing Plan (Shanghai Municipal Commission of Health and Family Planning, XBR2013103).