
Abstract
Objective:
This study was conducted to elucidate the distribution characteristics of predominant unbalanced constitutions and TCM syndrome elements in patients with recurrent and metastatic gastric cancer. This study was also undertaken to analyze the potential relationship between the body constitutions of patients, syndrome elements, and biological indicators, as well as to investigate the effect of Yiqi Wenyang Jiedu prescription (YWJP) on symptoms and biological indicators before and after treatment.
Result:
Yang-deficiency and Qi-deficiency were identified as prevalent imbalanced constitutions among patients with recurrent and metastatic gastric cancer. The primary syndrome factors associated with disease localization included the spleen-stomach and liver, with the main syndrome elements being Qi-deficiency, Yang-deficiency, and Qi-stagnation. Patients with Qi-deficiency and Yang-deficiency constitutions exhibited lower BMI and higher monocyte-to-lymphocyte ratio (MLR). A notable positive correlation was observed between cold (Yang-deficiency) and BMI, as well as between Qi-deficiency constitution and neutrophil-to-lymphocyte ratio (NLR). Furthermore, YWJP demonstrated efficacy in alleviating symptoms associated with Qi-deficiency and Yang-deficiency in patients with recurrent and metastatic gastric cancer, including dyspnea, fatigue, diaphoresis, cold intolerance, abdominal sounds, postural changes, and abdominal distension.
Discussion:
Yang-deficiency and Qi-deficiency emerged as prevalent constitutional patterns in patients with recurrent and metastatic gastric cancer. Notably, BMI, MLR, and NLR may serve as physiological indicators of these conditions. Furthermore, YWJP treatment demonstrated potential efficacy in alleviating symptoms associated with Qi-deficiency and Yang-deficiency in this patient population.
Clinical Trial Registration: Chinese Clinical Trial Registry: ChiCTR2200055826.
Introduction
According to data from the International Agency for Research on Cancer, global cancer statistics for 2020 estimated approximately 1,089,000 new cases and 373,000 deaths attributable to gastric cancer worldwide. In China, the crude incidence rate of gastric cancer was reported to increase from 30.5 per 100,000 in 2000 to 43.1 per 100,000 in 2019. Moreover, gastric cancer constituted 44.21% of the global cancer burden1 -3 in terms of disability-adjusted life years. Notably, surgical intervention remains the preferred treatment modality for gastric cancer, with research indicating a median recurrence interval of approximately 16.8 months. 4 The postoperative recurrence rate for patients with early gastric cancer is approximately 12.56%, whereas that for patients with locally advanced disease can reach 50–80%.5,6 Consequently, the proactive administration of adjuvant therapies, such as radiotherapy and chemotherapy, following gastric cancer surgery is essential for mitigating the risk of recurrence and metastasis, thereby extending patient survival. 7 However, despite the use of these adjuvant therapies, up to 50% of patients may still experience recurrence and metastasis within 2–3 years. 8 In cases of recurrence and metastasis after surgical intervention, palliative chemotherapy may yield a median survival duration of 7 to 15 months, with a 5 year survival rate of approximately 2%.9 -12 Therefore, investigating biological markers associated with the recurrence and metastasis of gastric cancer holds significant clinical importance.
Traditional Chinese Medicine (TCM) is classified as a form of complementary and alternative medicine that employs personalized therapeutic approaches based on the theory of body constitution.13 -15 The concept of TCM body constitution encompasses the unique morphological characteristics, physiological functions, and psychological state of an individual, which are influenced by both innate and acquired factors throughout their lifespan. These constitutions not only affect the susceptibility of individuals to diseases but also significantly influence the development and prognosis of various health conditions.16,17 According to the “Classification and Determination of Constitution in TCM,” published by the China Association of Chinese Medicine (CACM) in April 2009, the constitutional types in individuals can be categorized into 9 distinct types: balanced constitution (BC), Qi-deficiency constitution (QDC), Yang-deficiency constitution (YADC), Yin-deficiency constitution (YIDC), phlegm-damp constitution (PDC), damp-heat constitution (DHC), blood-stasis constitution (BSC), Qi-stagnation constitution (QSC), and inherited-special constitution (ISC). 18 Qi-deficiency and Yang-deficiency are important factors in the occurrence and development of gastric cancer. Prior research has indicated that individuals with YADC and QDC are more susceptible to recurrence and metastasis after gastric cancer surgery than those with other constitutions. 19 Qi-deficiency and Yang-deficiency are characterized by a low metabolic state. The tumor microenvironment can stimulate an increase in the number of IL22+ cells, and the overactivation of IL22+ cells can regulate the intestinal microbiota, reduce the expression of the key lipid transporter CD36, and decrease the levels of serum triglycerides and free fatty acids, thereby promoting the development of hypometabolism.20 -22 Therefore, based on clinical practice and previous studies, it is posited that Yang-deficiency toxicity is a central pathogenic factor in gastric cancer recurrence and metastasis.
The Fuzheng Jiedu prescription (FJP), an empirical prescription formulated by the Oncology Department of Guang’anmen Hospital, comprises Codonopsis pilosula, Astragalus membranaceus, Atractylodes macrocephala, Polygonum multiflorum, Rhizoma smilacis glabrae, Radix Actinidiae chinensis, Lycium chinense Miller, and Paris polyphylla Sm. In a previous study, Sun et al used this prescription in the postsurgical treatment of patients with stage III gastric cancer, leading to a notable 9.1% increase in the 5 year survival rate. 23 Moreover, following intervention with adjusted FJP, the 2 year recurrence and metastasis rates among patients who underwent gastric cancer surgery decreased to 18.60%, reflecting a reduction of approximately 25% compared with that in the control group. The intervention also improved clinical symptoms such as fatigue, pain, nausea, insomnia, and abnormal bowel movements.
The Yiqi Wenyang Jiedu prescription (YWJP) is a principal treatment for gastric cancer characterized by Yang-deficiency toxin-induced core pathogenesis after surgery. Developed by Professor Li from Guang ’anmen Hospital, YWJP is based on FJP and reflects extensive clinical experience. YWJP was designed to reinforce healthy Qi to eliminate pathogenic factors, supplement Qi, and warm Yang. 24 However, there is a limited understanding of the distribution patterns of common TCM body constitutions and syndrome elements in patients with recurrent and metastatic gastric cancer, as well as their associations with biological indicators. Furthermore, the effects of YWJP on symptoms related to prevalent imbalanced constitutions and clinical biological indicators require further investigation. The effectiveness of YWJP in addressing Qi-deficiency and Yang-deficiency in patients also is yet to be fully elucidated. Therefore, this study was conducted to elucidate the distribution of predominant unbalanced constitutions and TCM syndrome elements in patients with recurrent and metastatic gastric cancer. This study was also undertaken to analyze the relationships between body constitutions, syndrome elements, and biological indicators and to assess the effect of YWJP on symptoms and biological indicators before and after treatment.
Methods
Study Subjects
A prospective, single-arm study was conducted at the Oncology Department of Guang ’anmen Hospital, China Academy of Chinese Medical Sciences, between April 1, 2021, and February 1, 2022. This study included 55 individuals diagnosed with recurrent and metastatic gastric cancer, with an average age of 61 ± 12.38 years, comprising 34 males and 21 females. During the follow-up period, 9 patients died, and 6 were lost to follow-up, resulting in a total of 40 patients who completed the follow-up survey.
Selection Criteria
Diagnostic Criteria
(1) The diagnostic criteria for gastric cancer were based on the “Gastric Cancer Diagnostic and Treatment Guidelines (2018 Edition)” issued by the National Health Commission of the People’s Republic of China in 2018. 25
(2) Pathological staging, recurrence, and metastasis criteria for gastric cancer were determined using the definitions provided by the American Joint Committee on Cancer (AJCC) and the Union for International Cancer Control Tumor, Node, Metastasis staging system for gastric cancer, as outlined in the eighth edition of the AJCC guidelines.
Inclusion Criteria
(1) Confirmed diagnosis of gastric cancer.
(2) Recurrence or metastasis of gastric cancer after curative gastrectomy (including endoscopic mucosal and submucosal resection, open surgery, and laparoscopic surgery); or metastasis diagnosed at initial presentation without prior surgery (metastasis confirmed by histopathology, imaging, or clear clinical symptoms and signs).
(3) Participation in the questionnaire survey, with good compliance.
(4) Age ≥18 years old.
(5) Karnofsky Performance Status (KPS) score ≥60 points.
Exclusion Criteria
(1) Receipt of Western medical treatment within the last month (≤1 month).
(2) Presence of concurrent malignant tumors or significant primary diseases affecting the cardiovascular, cerebrovascular, hepatic, renal, or hematopoietic systems.
(3) Presence of psychiatric disorders or intellectual and language impairments.
(4) Pregnancy, pre-pregnancy, or lactating status in females.
(5) Known allergic reactions or predisposition to the drugs used in the study.
Study Methods
Constitutional Types in TCM
The constitutional types are delineated in the “TCM Constitution” 16 and the “Classification and Diagnostic Expression Basis of 9 TCM Constitution Types” 26 authored by Wang et al, alongside the “Classification and Determination Scale of TCM Constitution” 27 published by the China Association of Chinese Medicine in 2009 (Supplemental Table 1).
The main symptoms for each constitutional type are as follows:
(1) BC: Fatigue, low voice, low mood, insomnia, and forgetfulness.
(2) QDC: Fatigue, shortness of breath, palpitations, dizziness, susceptibility to colds, and tendency to sweat easily.
(3) YADC: Fear of cold, wearing more layers than others, and discomfort from consuming cold food or drinks.
(4) YIDC: Heat sensation, dry skin, and tendency toward constipation.
(5) PDC: Abdominal fullness, heaviness, full and soft abdomen, and forehead fat secretion.
(6) DHC: Greasy facial skin, tendency to develop acne, and bitter and malodorous mouth taste.
(7) BSC: Subcutaneous bleeding, body pain, dull complexion, and dark eye circles.
(8) QSC: Low mood, anxiety, sentimentality, and frequent sighing.
(9) ISC: Tendency to sneeze and runny nose owing to seasonal changes or odors, with a predisposition to allergies and hives (details are provided in Supplemental Table 1).
Diagnostic Criteria for TCM Syndromes
Based on the criteria for identifying syndrome elements outlined by Zhu in “Syndrome element differentiation,” 28 individual syndrome elements were assigned weights and calculated independently. A diagnostic threshold of 100 was established, and a syndrome element was diagnosed if the sum of its contributions exceeded this threshold.
Intervention and Follow-Up
Following enrollment, patients received modified treatment based on YWJP for 8 weeks, employing an integrated methodology that considered the constitution of “disease, syndromes, symptoms.” (Supplemental Table 2) The key herbs in YWJP include Astragalus membranaceus (30 g), Codonopsis pilosula (15 g), Angelica dahurica (10 g), Curcuma zedoary (9 g), Rhizoma nardostachyos (10 g), Polygonum cuspidatum (10 g), Radix Actinidiae chinensis (15 g), Paris polyphylla (9 g). 24 The herbs were decocted with water, resulting in a 100 to 150 ml solution each time, which was divided and administered twice daily, in the morning and evening. The patient took the medication at home after collecting it from the hospital.
Regulations for the Administration of Combined Medications
Patients were prohibited from using additional TCM drugs throughout the study duration.
Observation Index
(1) General information: Age, sex, weight, height, smoking history, drinking history, family history, medical history, and history of gastric cancer recurrence and metastasis.
(2) Diagnostic index: Pathological diagnosis, disease stage, degree of differentiation, clinical symptoms and signs, imaging examinations (computed tomography, magnetic resonance imaging, B-ultrasound, bone scan), and laboratory tests, including routine blood tests and liver and kidney function assessments.
(3) Efficacy evaluation indicators
1) Primary efficacy outcomes
① Grading scale for assessing the severity of symptoms related to Qi-deficiency
The grading scale comprises 5 symptoms, each of which was categorized into 4 grades based on clinical manifestations: none, mild, moderate, and severe 29 (Supplemental Table 3).
② Quantitative standard scale for identifying factors in deficiency-cold syndrome
The quantitative standard scale comprises 33 symptoms, each categorized into 5 grades based on clinical presentation: none, mild, moderate, severe, and extremely severe. Evaluations were conducted both prior to and following treatment. This scale was developed by the project team of the National Natural Science Foundation of China, “study of gene expression profile of kidney-Yang deficiency by gene chip” 30 (Supplemental Table 4).
2) Secondary efficacy outcomes
① KPS scores were determined using the standardized international KPS scoring system.
② Safety indicators such as routine blood tests, liver function (including alanine aminotransferase [ALT] and aspartate aminotransferase [AST] measurements), and renal function (including urea and creatinine measurements) were assessed before and after intervention. Any adverse reactions that occurred during treatment were documented.
Observation Node
Upon enrollment, patients were required to complete several assessments, including a general data sheet, a TCM syndrome element questionnaire, a TCM constitution classification and evaluation table, and scales for Qi-deficiency, Yang-deficiency, and KPS. Additionally, participants were required to undergo routine blood tests and evaluations of liver and kidney function. Following an 8 week intervention period, participants were instructed to readminister the Qi-deficiency, Yang-deficiency, and KPS scoring scales and repeat the blood tests and liver and kidney function assessments.
Statistical Analysis
Data was input into Excel and analyzed using a descriptive statistical analysis method to determine the number of cases, frequency, and percentage for each variable, with the results visually represented. Statistical analysis was performed using SPSS 25.0 software. A paired t-test was used for normally distributed data, whereas non-parametric tests were used for non-normally distributed data. Relationships among indicators were examined using various statistical methods, including paired rank-sum tests, multinomial logistic regression, and Pearson correlation analysis. Statistical analyses were conducted using a 2-tailed test of significance, with a probability value of P < 0.05 indicating statistical significance.
Result
Baseline Data
This clinical study enrolled 55 patients with recurrent and metastatic gastric cancer who met the inclusion and exclusion criteria between April 1, 2021, and February 1, 2022. A total of 55 patients completed the enrollment survey. During the follow-up period, 9 patients died, and 6 patients dropped out, leaving a total of 40 patients who completed the follow-up survey.
General Demographic Data
Sex distribution: The participant population comprised 34 males (61.82%) and 21 females (38.18%), resulting in a sex ratio of 1.62:1.
Age distribution: The mean age was 61 ± 12.38 years, with a median age of 64 years. The age distribution was as follows:
5 cases (9.09%) had an age range of 30 to 39 years.
3 cases (5.45%) had an age range of 40 to 49 years.
15 cases (27.27%) had an age range of 50 to 59 years.
17 cases (30.91%) had an age range of 60 to 69 years.
11 cases (20.00%) had an age range of 70 to 79 years.
4 cases (7.27%) had an age range of 80 to 89 years.
Tobacco and alcohol history distribution: 23 patients (41.38%) had a history of smoking, whereas 32 patients had no history of smoking (58.18%). Additionally, 21 patients (38.18%) had a history of alcohol consumption, whereas 34 patients (61.82%) had no history of alcohol consumption.
Family history distribution: 21 (38.18%) patients had a family history of gastric cancer, whereas 34 patients (61.82%) had no family history of gastric cancer.
Distribution of gastric cancer-related data: 30 patients (54.55%) with gastric cancer recurrence and metastasis received surgical treatment after diagnosis, whereas 25 patients (45.45%) did not. The distribution of primary lesion sites for gastric cancer was as follows: the cardia was the most common site, with 16 cases (29.09%), followed by the stomach body and antrum pylorus, each with 13 cases (23.64% each), the lesser curvature of the stomach, with 6 cases (10.91%), and other parts, with 7 cases (12.73%; Table 1).
General Personal Data of Patients With Recurrence and Metastasis of Gastric Cancer.

Clinical Data Related to Recurrence and Metastasis
Distribution of Recurrence and Metastasis Sites
Among patients with recurrence and metastasis, the distribution of recurrent sites was as follows: 3 cases (30.00%) occurred at the anastomosis, 2 cases (20.00%) at the cardia, 1 case (10.00%) at the gastroesophageal junction, 1 case (10.00%) at the greater curvature of the middle stomach body, and 1 case (10.00%) at the stomach body involving input and output loops.
The most prevalent site of distant metastasis was the peritoneum (19 cases, 28.36%), followed by the liver (16 cases, 23.88%), lymph node (8 cases, 11.94%), lung (5 cases, 7.46%), ovary (5 cases, 7.46%), kidney (4 cases, 5.97%), colon (3 cases, 4.48%), bone (2 cases, 2.99%), and pelvic cavity (2 cases, 2.99%). Additionally, there was 1 case each of metastasis to the bladder, rectum, and psoas major muscle, each accounting for 1.49% .
Treatment After Recurrence and Metastasis
Chemotherapy was the predominant treatment modality for patients with recurrent and metastatic gastric cancer. Among a total of 33 patients, 18 (32.73%) underwent chemotherapy alone. Six patients (10.91%) underwent chemotherapy combined with targeted therapy. Four patients (7.27%) received chemotherapy combined with immunotherapy, and 3 patients (5.45%) were treated with chemotherapy combined with radiotherapy. There was 1 case (1.82%) of chemotherapy combined with radiotherapy and targeted therapy and 1 case (1.82%) of chemotherapy combined with immunotherapy and targeted therapy. Additionally, 14 patients (25.45%) received TCM therapy alone, 7 patients (12.73%) received targeted therapy, and 1 patient (1.82%) underwent endoscopic surgery.
Constitutional Types in TCM
Among the cohort of 55 patients with recurrent and metastatic gastric cancer, the predominant constitution type identified was YADC, followed by BC, QDC, PDC, YIDC, DHC, and QSC, and BSC. Notably, no patients were classified under the ISC category. Additionally, the constitutions of 4 patients could not be accurately assessed. Based on the frequency of occurrences, the unbalanced constitution was categorized as follows: Yang-deficiency > Qi-deficiency > phlegm-damp > Qi-stagnation = damp-heat = Yin-deficiency > blood-stasis > inherited-special constitution.
Among patients exhibiting concurrent constitutional types, the predominant constitution was QDC, followed by QSC, YADC, PDC, YIDC, and DHC. BSC, and ISC. The hierarchical order of concurrent constitutional types, ranging from most to least prevalent, is Qi-deficiency, Qi-stagnation, Yang-deficiency, phlegm-damp, Yin-deficiency and damp-heat, blood-stasis and inherited-special constitution (Tables 2 and 3).
Distribution of Main Constitution Types in Patients With Recurrence and Metastasis of Gastric Cancer.

Distribution of Concurrent Constitution Types in Patients with Recurrence and Metastasis of Gastric Cancer.

Distribution of Syndrome Elements
Disease Location of Syndrome Elements
Among the 55 patients included in this study, the spleen and liver were the most commonly affected organs, with each organ involved in 40 patients cases, followed by the stomach, kidney, large intestine, small intestine, heart, gallbladder, and lungs. The disease location could not be definitively determined for 4 patients. The primary disease locations associated with syndrome elements in gastric cancer were the spleen-stomach and liver. The relative frequency is ranked as follows: spleen = liver > stomach > kidney > large intestine > small intestine >heart > gallbladder > lung (Table 4).
Distribution of Syndrome Elements of Disease Location in Patients With Recurrence and Metastasis of Gastric Cancer.

Disease Characteristics of Syndrome Elements
Among the 55 patients included in this study, the most prevalent disease characteristics of syndrome elements were Qi-deficiency, followed by Qi-stagnation, Yang-deficiency, dampness, cold and Yin-deficiency, blood-deficiency, body fluid deficiency, dryness, phlegm, heat, dyspepsia, blood stasis, and fluid-retention. However, the distribution of syndrome factors could not be accurately determined for 6 patients.
The prevalence of disease characteristics associated with syndrome elements is ranked in descending order as follows: Qi-deficiency, Qi-stagnation, Yang-deficiency, dampness, cold, Yin-deficiency, blood-deficiency, fluid-deficiency, dryness, phlegm, heat, food-stasis, blood-stasis, and fluid-retention. Among these, the predominant syndrome elements in the solid syndromes were Qi-stagnation, dampness, and cold, whereas deficiency syndromes were characterized by Qi-deficiency, Yang-deficiency, and Yin-deficiency (Table 5).
Distribution of Disease Characteristics of Syndrome Elements in Patients with Recurrence and Metastasis of Gastric Cancer.

Relationship Between Constitutional Factors, Syndrome Elements, and Primary Outcomes and Secondary Outcomes
Relationship Between Constitutions and BMI, NLR, PLR, MLR, and PNI
Subsequently, patients with ISC, those with missing data on body mass index (BMI), neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), monocyte-to-lymphocyte ratio (MLR), and prognostic nutritional index (PNI), as well as patients with unbalanced constitution and PNI, were excluded, resulting in 45 patients. Multinomial logistic regression analysis revealed no significant relationship between unbalanced constitution and PNI (Table 6). Statistical analysis indicated that BMI, NLR, and MLR exhibited significant relationships with constitution types, whereas PLR did not demonstrate a discernible association with constitution. Compared to individuals with a balanced constitution, those with QDC and YADC exhibited lower BMI (P < 0.05, P < 0.01), higher MLR (P < 0.01), and lower NLR in the case of the QDC group (P < 0.05).
Relationship Between Constitution Types and BMI, NLR, PLR, and MLR.

b: System Missing Value; NLR, MLR, and PLR indices do not have units.
Abbreviations: BMI, body mass index; NLR, neutrophil to lymphocyte ratio; MLR, monocyte to lymphocyte ratio; PLR, platelet lymphocyte ratio.
Relationship Between Syndrome Elements and BMI, NLR, PLR, MLR, and PNI
Relationship Between Disease Location of Syndrome Elements and BMI, NLR, PLR, MLR, and PNI
Among the 55 patients enrolled in the study, disease location could not be determined for 4, data on BMI, NLR, PLR, and MLR were unavailable for 5, and information on PNI was unavailable for 2, resulting in their exclusion from the analysis. This exclusion resulted in a total of 41 patients. Owing to the presence of only one case of gallbladder disease, the data for this condition were deemed insufficient and excluded. The correlations between the disease location of syndrome elements and BMI, NLR, PLR, MLR, and PNI (Table 7) are illustrated in Table 6. The analysis revealed no statistically significant correlations between BMI, NLR, PLR, MLR, and PNI, and the specific disease locations associated with the syndrome elements.
Relationship Between Disease Location of Syndrome Elements and BMI, NLR, PLR, MLR, and PNI.

NLR, MLR, PLR, and PNI indices do not have units.
Abbreviations: BMI, body mass index; NLR, neutrophil to lymphocyte ratio; MLR, monocyte to lymphocyte ratio; PLR, platelet lymphocyte ratio; PNI, prognostic nutritional index.
Relationship Between Disease Characteristics of Syndrome Elements and BMI, NLR, PLR, MLR, and PNI
Among the 55 patients included in this study, disease characteristics of syndrome elements could not be determined for 6, data on BMI, NLR, PLR, and MLR were unavailable for 6, and data on PNI were unavailable for 2, resulting in their exclusion from the analysis. This exclusion resulted in a total of 41 patients. Given that most patients with recurrent and metastatic of gastric cancer exhibited concurrent disease characteristics, the highest disease factor score was selected as the primary syndrome factor. Additionally, data for phlegm (n = 1), dryness (n = 1), and fluid-deficiency (n = 1) were excluded from the analysis owing to insufficient valid data (Table 8). The analysis revealed a statistically significant positive association between BMI and cold symptoms (P < 0.05) and a significant positive correlation between NLR and Qi-deficiency (P < 0.05). Conversely, PLR, MLR, and PNI were not significantly correlated with syndrome elements. These results suggest that increased severity of cold symptoms is associated with higher BMI, whereas greater severity of Qi-deficiency symptoms is linked to higher NLR levels.
Relationship Between Disease Characteristics of Syndrome Elements and BMI, NLR, PLR, MLR, and PNI.

NLR, MLR, PLR, and PNI indices do not have units.
Abbreviations: BMI, Body mass index; NLR, neutrophil to lymphocyte ratio; MLR, monocyte to lymphocyte ratio; PLR, platelet lymphocyte ratio; PNI, prognostic nutritional index.
YWJP for Patients With Recurrent and Metastatic Gastric Cancer and Unbalanced Constitution
Building upon previous research on constitutional and syndromic elements in patients with recurrent and metastatic gastric cancer, Qi-deficiency and Yang-deficiency have been established as prevalent imbalances. Consequently, the Qi-deficiency scale and Yang-deficiency scales were employed to assess the efficacy of YWJP supplemented with Qi-tonifying and Yang-warming medications in alleviating symptoms associated with Qi-deficiency and Yang-deficiency in this patient population.
Changes in Qi-Deficiency Scale Scores Pre- and Post-Treatment
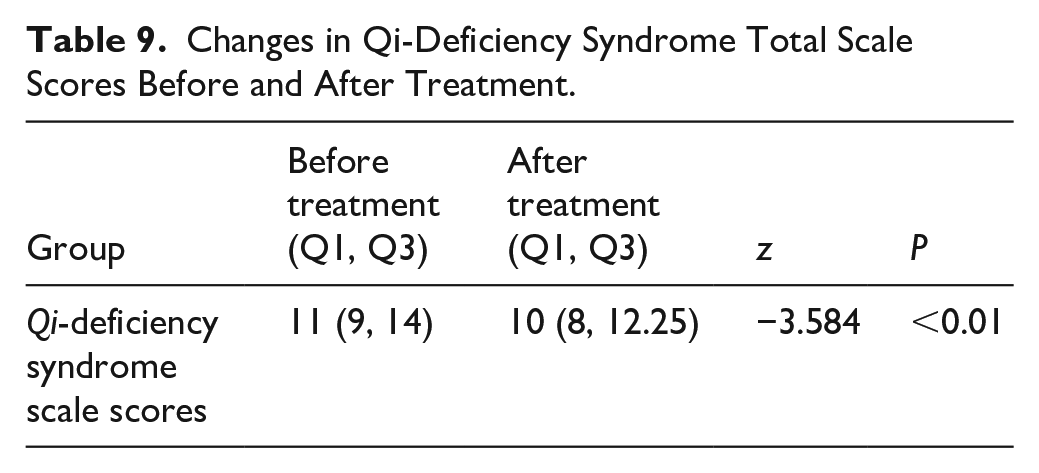
Among the 55 patients with recurrent or metastatic gastric cancer included in this study, 9 patients died during follow-up, and 6 patients withdrew from the study, resulting in a total of 40 patients who completed the follow-up. The median Qi-deficiency syndrome scale score was 11 pre-treatment (upper quartile: 9, lower quartile: 14), which decreased to 10 post-treatment (upper quartile: 8, lower quartile: 12.25). A statistically significant difference was observed in the Qi-deficiency scale scores before and after treatment (P < 0.01). The findings indicated that the administration of YWJP, combined with Qi-enhancing and Yang-warming medications, led to significant improvement in the Qi-deficiency scale measurements among patients with recurrent and metastatic gastric cancer (Table 9).
Changes in Qi-Deficiency Syndrome Total Scale Scores Before and After Treatment.
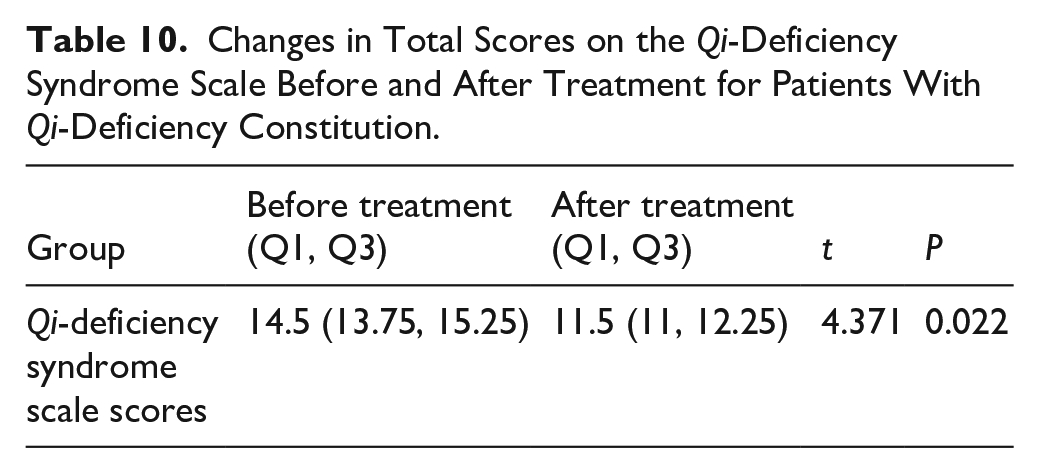
Furthermore, based on the differences in patients’ constitution distributions, we investigated changes in the Qi-deficiency scale scores before and after YWJP treatment among patients with Qi-deficiency constitution, and Yang-deficiency constitution. A total of 35 patients completed follow-up before and after treatment and had their constitution types effectively determined, including 13 cases of Yang-deficiency constitution, and 4 cases of Qi-deficiency constitution. The following sections present the Qi-deficiency scale scores, including the median and upper and lower quartiles, for patients with Qi-deficiency constitution, and Yang-deficiency constitution, respectively. There was a statistically significant difference in the change of total scores on the Qi-deficiency scale before and after YWJP treatment between patients with Qi-deficiency constitution (P < 0.05; Table 10), however, due to the small sample size, the clinical significance should be carefully evaluated. While patients with Yang-deficiency constitution showed a trend of improvement, no statistical difference was observed (Supplemental Table 5) .
Changes in Total Scores on the Qi-Deficiency Syndrome Scale Before and After Treatment for Patients With Qi-Deficiency Constitution.
Symptoms associated with Qi-deficiency syndrome were assessed using a grading scale before and after YWJP administration. Following the intervention, a significant improvement in fatigue symptoms was observed (P < 0.01). Additionally, statistically significant improvements in shortness of breath and spontaneous sweating were observed (P < 0.05). Although improvements were also observed in symptoms such as shortage of Qi, lack of desire to speak, and poor appetite, these changes were not statistically significant (Table 11).
Grading of Qi-Deficiency Symptoms Total Scale Before and After Treatment.

In addition, we separately analyzed the grading of symptoms related to the Qi-deficiency syndrome scale for patients with Qi-deficiency constitution, and Yang-deficiency constitution before and after YWJP intervention. Among patients with Qi-deficiency constitution, due to the small sample size (4 cases), no statistically significant improvement in symptoms was observed (Supplemental Table 6). However, among patients with Yang-deficiency constitution, significant improvement was noted in symptoms of fatigue (P <0 .05; Table 12).
Grading of Qi-Deficiency Symptoms Total Scale Before and After Treatment for Patients With Yang-Deficiency Constitution.

Changes in Yang-Deficiency Syndrome Scale Scores Pre- and Post-Treatment
The median score on the Yang-deficiency syndrome scale was 57 before treatment (upper quartile: 43.75, lower quartile: 70), and 53 after treatment (upper quartile: 44.25, lower quartile: 66). The observed change in scores was statistically significant (P < 0.05). These results indicate that the addition of Qi-enhancing and Yang-warming drugs to YWJP led to a notable improvement in recent Yang-deficiency symptoms among patients with recurrent and metastatic gastric cancer (Table 13). However, among patients with Qi-deficiency constitution, and Yang-deficiency constitution, no statistically significant differences were observed in the changes of Yang-deficiency syndrome scale scores (Supplemental Tables 7 and 8).
Changes in Yang-Deficiency Syndrome Scale Scores Before and After Treatment.

The symptoms associated with Yang-deficiency syndrome were assessed before and after YWJP administration, as detailed in Table 11. Following the intervention, Statistically significant improvements were observed in symptoms such as cold limbs, cold intolerance, and bowel sounds (P < 0.01). Statistically significant improvements were also observed in symptoms such as body curling, fatigue, and abdominal distension (P < 0.05; Table 14; Supplemental Table 9 as complete table). Based on the differences in patients’ constitution distributions, we explored the changes in Yang-deficiency syndrome scale scores among patients with Qi-deficiency constitution, and Yang-deficiency constitution before and after YWJP treatment. A total of 35 patients completed the follow-up before and after treatment and had their constitution types effectively determined (13 cases of Yang-deficiency constitution, and 4 cases of Qi-deficiency constitution). According to statistical analysis, there was no significant statistical difference in Yang-deficiency symptoms among patients with Qi-deficiency constitution (Supplemental Table 10). Patients with Yang-deficiency constitution showed significant improvement in symptoms of aversion to cold and chilliness(Table 15; Supplemental Table 11 as complete table).
Grading of Yang-Deficiency Symptoms Scale Before and After Treatment.

Grading of Yang-Deficiency Symptoms Scale Before and After Treatment With Yang-Deficiency Constitution.

Changes in KPS Scores Pre- and Post-Treatment
No statistically significant differences in KPS scores were observed among patients with recurrent and metastatic gastric cancer before and after YWJP administration. The median pre-treatment KPS score was 90 (upper quartile: 80, lower quartile: 90), whereas the median post-treatment KPS score was 90 (upper quartile: 80, lower quartile: 92.5; Table 16). Based on the differences in the distribution of patients’ constitutions, we explored the changes in KPS scores among patients with Qi-deficiency, and Yang-deficiency constitutions before and after YWJP treatment. A total of 35 patients completed the follow-up before and after treatment and had their constitution types effectively determined (13 cases of Yang-deficiency, and 4 cases of Qi-deficiency). After statistical analysis, no significant statistical differences were found in the KPS scores among patients with Qi-deficiency, and Yang-deficiency constitutions (Supplemental Tables 12 and 13).
Changes in KPS Scores Before and After Treatment.

Changes in BMI, NLR, MLR, and PNI Levels Pre- and Post-Treatment
Following YWJP treatment, a marginal decrease in BMI, NLR, and PNI was observed, whereas MLR exhibited a slight increase; however, these changes were not statistically significant (P > 0.05; Table 17). Furthermore, based on the constitution distribution of patients, we explored the differences in the changes of BMI, NLR, MLR, and PNI index levels before and after YWJP treatment among patients with Qi-deficiency, and Yang-deficiency, constitutions. A total of 31 patients completed the measurement of BMI, NLR, MLR, and PNI indices before and after treatment and had effective constitution type determinations. These included 11 cases of Yang-deficiency constitution, and 4 cases of Qi-deficiency constitution. Statistically, the BMI, NLR, and PNI of patients with Qi-deficiency, and Yang-deficiency constitutions decreased slightly after treatment, while MLR increased slightly. However, these changes were not statistically significant (P > 0.05; Supplemental Tables 14 and 15).
Changes in BMI, NLR, MLR, and PNI Levels Before and After Treatment.

Abbreviations: BMI, body mass index; NLR, neutrophil to lymphocyte ratio; MLR, monocyte to lymphocyte ratio; PNI, prognostic nutritional index.
Occurrence of Adverse Events During the Study
During treatment, a slight increase in ALT levels was observed in 1 patient (less than a onefold increase), which was considered abnormal but not clinically significant. This increase may be attributable to the elevation in aminotransferase levels caused by postoperative liver metastasis of gastric cancer. No significant abnormalities were observed in the safety indices related to the TCM administered. These findings indicate that YWJP was safe for clinical application and did not exhibit any apparent toxicity or side effects.
Overall Survival of Patients With Gastric Cancer Recurrence and Metastasis
Outcome visits for this clinical study were updated on July 20, 2024. Among the 55 patients included in this study, 27 patients were either unreachable or chose not to disclose their condition, 8 patients survived, and 20 patients experienced endpoint events. Among the surviving patients, the most prevalent constitutional type was balanced constitution (50%). Overall survival (OS) exceeded 730 days in 13 patients, ranged between 365 and 730 days in 5 patients, and was less than 365 days in 2 patients. The shortest, longest, and median OS recorded was 164, 2704 days, and 1002 days, respectively. The survival data of 20 patients with endpoint events classified by physical type are as follows:
Balanced constitution: Mean OS of 906.40 days.
QDC: Mean OS of 655.33 days
YADC: Mean OS of 933.83 days
PDC: Mean OS of 1439.50 days
Undefined constitution type: Mean OS of 1733.50 days (Table 18).
OS and Physical Status of Patients With Gastric Cancer Recurrence and Metastasis.

NA: The constitution type could not be determined; Overall survival data of individual patients are shown under “OS”; mean survival times for constitution types are shown under “x¯ (days).”
Discussion
Advancements in medical, healthcare, and scientific technologies have underscored the importance of effective prevention and management of chronic diseases in public health. In 2006, the World Health Organization classified malignant tumors as chronic diseases owing to their protracted duration, prolonged treatment regimens, and lasting effects on individuals. This classification has led to an increased focus on tertiary prevention strategies for cancer among both healthcare providers and patients. 31 However, therapeutic options for recurrent and metastatic gastric cancer are limited and frequently associated with adverse reactions following the administration of modern medical treatments. 32 Therefore, it is imperative to investigate multimodal therapeutic approaches to ameliorate the clinical manifestations and improve survival rates. TCM, which focuses on balancing Yin and Yang, plays a crucial role in the management and prevention of recurrent and metastatic gastric cancer. 33 Accurate identification of constitutional types and syndromes in patients, alongside their association with biological markers, enables more targeted treatment based on the disease stage. The use of YWJP in managing gastric cancer recurrence and metastasis demonstrated promising results in alleviating symptoms of Qi-deficiency and Yang-deficiency, as well as improving KPS scores. These findings may provide valuable insights for refining clinical diagnosis and treatment strategies.
Among the 55 patients included in this study, there were 34 males, accounting for 61.82%, and 21 females, accounting for 38.18%. The male-to-female ratio was 1.62:1. The age distribution ranged from 32 to 84 years old, with a mean age of 61 ± 12.38 years and a median age of 64 years. The highest prevalence was observed in the age groups of 50 to 59 and 60 to 69 years old. Family history, smoking, drinking, high salt intake, low fruits and vegetables intake, and microbial factors are risk factors for gastric cancer.34 -37 In this study, the number of patients without a smoking history, without a drinking history, and without a family history of gastric cancer exceeded the number of those with these respective histories. This result suggests that although smoking, drinking, and family histories are risk factors for gastric cancer, they are not definitive factors, reflecting the complexity of the clinical scenario. In this study, 30 patients underwent surgical treatment following gastric cancer diagnosis. Surgical intervention is considered the preferred treatment approach for patients with gastric cancer post-diagnosis and is performed in accordance with surgical guidelines. 25 A previous study revealed that the recurrence rate of residual stomach and lymph nodes in the surgical field after a D1 operation was 72%, which decreased to 27% after a D2 operation (P < 0.05). 38 D2 surgery is recommended for patients without contraindications. In the present study, the primary sites of gastric cancer lesions were predominantly the cardiac region, stomach body, and antrum pylorus. These findings align with those of a previous clinical study and generally are consistent with the distribution of primary gastric cancer lesions in China. 39
In this study, the primary sites of recurrence in patients with gastric cancer were predominantly the anastomotic stoma, aligning with the principal local recurrence sites reported after radical gastrectomyin previous studies. 40 The main site of metastasis was the peritoneum, followed by the liver and lymph nodes, consistent with previous findings, which identified peritoneal implantation as the most common form of postoperative recurrence and metastasis in, 41 followed by lymph node and blood metastases. Following recurrence and metastasis, chemotherapy was the primary treatment modality; 33 patients received chemotherapy either as a sole treatment or in combination, in accordance with the established clinical diagnosis and treatment guidelines for gastric cancer.
The distribution of constitutions among patients with recurrent and metastatic gastric cancer is primarily characterized by Yang deficiency, followed by a balanced constitution, and then Qi deficiency. The order of biased constitutions, from most to least common, is Yang deficiency, Qi deficiency, phlegm-dampness, Qi stagnation, dampness-heat, Yin deficiency, blood stagnation, and special constitution. The order of combined constitutions, from most to least common, is Qi deficiency, Qi stagnation, Yang deficiency, phlegm-dampness, Yin deficiency and dampness-heat, blood stagnation, and special constitution. Evidently, the constitutions of patients with recurrent and metastatic gastric cancer are predominantly Yang deficiency and Qi deficiency, while the combined constitutions are mainly Qi deficiency, Qi stagnation, and Yang deficiency. This finding aligns with our team’s previous research 42 indicating that patients with Qi deficiency and Yang deficiency constitutions are more prone to recurrence and metastasis after gastric cancer surgery.
Furthermore, these results are consistent with Sun'’s 43 belief that Yang deficiency, Qi deficiency, and Qi stagnation are predisposing constitution types for gastric cancer patients. As recorded in “The Yellow Emperor’s Classic of Internal Medicine”(HDNJ), “Yang Qi is like the sky and the sun. Without it, life is shortened and vitality is diminished.” The Yang Qi in the human body is analogous to the sunshine of the universe, which should be warm and harmonious. If Yang Qi fails to circulate freely, pathologies may arise from its accumulation. The “HDNJ” states, “When there is disharmony of cold and warmth between the spleen and stomach . . . significant pathologies may emerge.” This suggests that Yang deficiency and internal coldness are crucial pathomechanisms in the development of gastric cancer. The findings of this study indicate that the pathological characteristics of patients with advanced gastric cancer are primarily Yang deficiency and Qi stagnation, aligning with our mentor’s proposal of the 5-phase evolution of tumors 44 : “deficiency, coldness, toxicity, stagnation, and decline,” where Yang deficiency is a core factor in tumor progression, Qi stagnation persists throughout, and in the terminal phase, both Qi and Yang decline. These findings lay a clinical foundation for the practical application of our team’s innovative theories in the diagnosis and treatment of gastric cancer.
In this study, the disease location syndrome elements of patients with recurrent and metastatic gastric cancer were primarily focused on the spleen-stomach and liver, with the order from most to least being spleen and liver, stomach, kidney, large intestine, small intestine, heart, gallbladder, and lung. The spleen-stomach and liver are involved in a mutual generative and inhibitory relationship. As stated in the “HDNJ,” “When the earth (spleen) is dredged and smooth, the verdant qi (of the liver) can be expressed.” This implies that when the spleen-stomach functions properly, the liver can flourish harmoniously, echoing the principle in the “Synopsis of Golden Chamber” that “when seeing a disease of the liver, one should know that it can transmit to the spleen, and therefore should strengthen the spleen first.” If the earth (spleen) becomes congested, the wood (liver) becomes stagnant, and vice versa. Additionally, when the wood (liver) loses its natural bending and stretching, emotional disharmony occurs, as stated in the “Ling Shu,” “When liver qi is excessive, there is anger; when it is deficient, there is fear.” Studies have shown that there is a bidirectional transmission of information between gastrointestinal function and central emotional cognition through the brain-gut axis. Moreover, dysfunction of the microbiota-gut-brain axis has a significant impact on depression, providing clinical evidence for the relationship between gastric cancer and adverse emotions such as depression.45,46 Patients with advanced gastric cancer often experience anxiety and depression. 47 Therefore, it is clinically evident that the disease location of patients with recurrent and metastatic gastric cancer is primarily in the spleen, stomach, and liver, which aligns with the current clinical situation.
In this study, the main pathological factors among patients with recurrent and metastatic gastric cancer were qi deficiency, followed by qi stagnation and yang deficiency. The frequency from high to low was qi deficiency, qi stagnation, yang deficiency, dampness, cold, yin deficiency, blood deficiency, fluid deficiency, dryness, phlegm, heat, food stagnation, blood stasis, and fluid retention. The main substantial pathological factors were qi stagnation, dampness, and cold, while the main deficiency pathological factors were qi deficiency, yang deficiency, and yin deficiency. It can be seen that patients with recurrent and metastatic gastric cancer have a mixture of deficiency and excess pathologies, but the main pathologies are yang and qi deficiency, as well as dampness-cold stagnation. Studies have demonstrated that patients with advanced gastric cancer often exhibit Yang-deficiency and Qi-deficiency in their constitution. 48 Depression is also prevalent among these patients, with Qi-stagnation and Qi-deficiency being the primary constitutional types observed in those experiencing depression. 49 Consequently, patients with recurrent and metastatic advanced gastric cancer may have a combination of Yang-deficiency, Qi-deficiency, and Qi-depression. Prolonged Qi Yang deficiency can lead to Yang damage affecting Yin, resulting in Yin deficiency. Additionally, some studies suggest that patients with gastric cancer post-chemotherapy commonly present with spleen deficiency, phlegm dampness, and spleen and kidney Yang deficiency as the main syndromes. 50 The cold dampness induced by chemotherapy acts as a toxin, harming human Yang and leading to its depletion within the body. Notably, Qi Yang deficiency can trigger endogenous cold and dampness, creating a cyclical relationship. Therefore, the distribution of the main pathogenic factors in patients with gastric cancer recurrence and metastasis aligns with the clinical understanding of gastric cancer recurrence and metastasis in TCM.
In this study, a significant association was observed between BMI, NLR, and MLR and constitutional types. Specifically, individuals with QDC exhibited lower BMI and NLR (P < 0.05), as well as higher MLR (P < 0.01) compared with those with a balanced constitution. Similarly, patients with YADC exhibited lower BMI and higher MLR (P < 0.01), suggesting that BMI and MLR could potentially serve as biomarkers for identifying Qi-deficiency and Yang-deficiency constitutional types. Previous studies have indicated that a low BMI 51 and a high MLR 52 are risk factors for the prognosis of gastric cancer. Additionally, patients with gastric cancer recurrence and metastasis who have Qi deficiency and Yang deficiency constitutions tend to have a poor prognosis. Therefore, it is hypothesized that low BMI and high MLR levels may serve as clinical biological indicators reflecting Qi deficiency and Yang deficiency in patients with gastric cancer recurrence and metastasis. According to the “Yellow Emperor’s Inner Canon of Medicine,” “Yang transforms into Qi, and Yin takes form.” Physiologically, when Yang fails to transform into Qi, it becomes difficult for Yin to take form. Qi is the gradual manifestation of Yang, while Yang represents the extreme state of Qi. Deficiency in Qi and Yang leads to difficulty in storing nutrients, resulting in weight loss and a tendency for BMI to decrease. MLR is an indicator that reflects inflammation in the peripheral blood and can be likened to the concept of “fiery pathogenic factors” in traditional Chinese medicine. As stated in the “Collection of Explanations on Treatise on Febrile Diseases,” “Under accumulated Yin, there must be hidden Yang.” In patients with gastric cancer recurrence and metastasis, deficiency in Qi and Yang leads to the accumulation of Yin, and tangible pathogenic factors obstruct Qi flow. The accumulation of Qi generates heat, and excessive heat consumes Qi, further depleting the body’s vital energy. When the body’s defenses are weak, fiery pathogenic factors combined with cancer toxins can exacerbate the disease, leading to a poor prognosis. NLR reflects the balance between the body’s anti-cancer immune system and pro-inflammatory responses that promote cancer. Previous studies have found that patients with a Qi deficiency constitution have lower levels of CD4+ immune cells compared to other constitutions (P < 0.05). 53 Weakened immune responses are observed in patients with deficient defensive Qi, and immune function shows a decreasing trend in mice with Qi deficiency. Constitution refers to the relatively stable physiological characteristics of the human body, which are inherent and influenced by environmental factors, shaping both morphology and function. Patients with a Qi deficiency constitution are chronically in a state of vital energy deficiency, 54 with suppressed immune function and an inability to effectively resist pathogenic factors. Consequently, these patients tend to have lower NLR levels.
The results of this study indicate a significant positive correlation between BMI and the pathogenic factor of cold (P < 0.05), as well as a strong positive correlation between NLR and qi deficiency (P < 0.05). This suggests that higher levels of cold in syndromes are associated with higher BMI, and greater qi deficiency is linked to higher NLR. The significant positive correlation between BMI and the pathogenic factor of cold is further supported by the finding that as BMI decreases, the level of cold also decreases (P < 0.05). Research has showed 55 that warm acupuncture intervention in patients with Yang deficiency constitution and obesity led to a decrease in BMI and improvement in Yang deficiency scores. This suggests a positive correlation between the degree of internal cold due to Yang deficiency and BMI, which aligns with the findings of this study. Yang deficiency leads to internal cold, which impairs the warming and dispersing functions of qi. Additionally, the presence of a tumor blocks the internal passageways, resulting in the accumulation of metabolic products such as dampness and phlegm due to impaired qi transformation. This accumulation leads to a pathological increase in BMI. As stated in the HDNJ, “Cold injures the body.” Both internal and external cold consume yang qi, leading to impairment of spleen and stomach functions and a lack of Yang qi generation. Coupled with the consumption of Yuan yang by gastric cancer lesions and recurrent metastases, as well as the overflow of dampness and phlegm, an increase in BMI is observed. Therefore, there is a positive correlation between the pathogenic factor of cold and BMI.
The results of this study indicate a significant positive correlation between NLR and the syndrome element of Qi deficiency. As NLR increases, the syndrome of Qi deficiency gradually worsens. Previous research has found that gastric cancer patients with high NLR levels are more prone to distant metastasis, and as the tumor stage increases, NLR levels rise, leading to a poorer prognosis. 56 As stated in the book of “Huofa Jiyao,” “Strong people do not accumulate illness, while weak people do.” Patients with recurrent or metastatic gastric cancer already have a deficiency of healthy qi. Coupled with the internal obstruction caused by cancerous tumors, impedance of qi flow, and consumption of qi and yang, the weakness of healthy qi cannot be stabilized, leading to the overflow of pathogenic factors. Furthermore, studies have shown 57 that qi deficiency syndrome is a common syndrome type in patients with advanced gastric cancer. Evidently, patients with qi deficiency syndrome have a poor prognosis, and patients with high NLR levels also have a poor prognosis, indicating a positive correlation between the two. In this study, “syndrome” refers to a summation of the pathogenesis at a certain stage of the disease process in the body. The NLR of patients with qi deficiency constitution tends to be low, while the NLR of patients with qi deficiency syndrome tends to be high. This may be because patients with qi deficiency constitution are chronically in a state of qi deficiency, with weak healthy qi and inability to resist pathogenic factors, resulting in a low NLR, an indicator of immune inflammation. On the other hand, patients with qi deficiency syndrome experience qi deficiency at a certain stage of the disease, but their healthy qi has not yet been exhausted, and the body is still compensating, fighting against pathogenic factors, leading to an elevated NLR.
By analyzing the efficacy of YWJP in the treatment of patients with recurrent and metastatic gastric cancer, we found that YWJP significantly improved the symptoms of Qi deficiency and Yang deficiency in these patients (P < 0.01). Specifically, patients experienced marked improvement in symptoms of fatigue (P < 0.01), with some improvement also noted in shortness of breath and spontaneous sweating (P < 0.05). While symptoms of lack of energy and poor appetite showed some improvement, these changes were not statistically significant. In patients with Qi deficiency constitution, there was a statistically significant difference in the total score of the Qi deficiency scale before and after YWJP treatment (P <0 .05). However, due to the small sample size (4 cases), no significant statistical difference was observed in the improvement of Qi deficiency symptoms. In patients with Yang deficiency constitution, there was a trend of improvement in the total score of the Qi deficiency scale before and after treatment, but this difference was not statistically significant. Notably, these patients showed significant improvement in symptoms of fatigue (P <0 .05). The median total score of the Yang deficiency syndrome scale decreased from 57 before treatment to 53 after treatment with YWJP (P < 0.05). Patients also experienced significant improvement in symptoms such as cold extremities, aversion to cold, and bowel sounds (P < 0.01), as well as improvement in symptoms of curling up, fatigue, and abdominal distension, with statistically significant differences (P < 0.05). However, no significant statistical difference was observed in the total score of the Yang deficiency syndrome scale in patients with Qi deficiency or Yang deficiency constitution. Patients with Yang deficiency constitution showed significant improvement in symptoms of aversion to cold (P < 0.05), while no significant statistical difference was noted in the improvement of Yang deficiency symptoms in patients with Qi deficiency constitution. Additionally, there was no significant statistical difference in the KPS scores of patients before and after YWJP treatment. Similarly, no significant statistical differences were observed in the KPS scores of patients with Qi deficiency or Yang deficiency constitution. Due to the small sample size in this part of the study, although some results are statistically significant, they can only suggest potential trends. This is because a small sample size may lead to insufficient statistical power, increasing the risk of false positives and false negatives. Therefore, even if the results are statistically significant (P < 0.05), they may not be robust enough, limiting the reliability of the conclusions. In the future, we plan to conduct a large-sample, multi-center randomized controlled study to further validate its clinical significance.
In patients with advanced gastric cancer, cancerous toxins overflow and block internal mechanisms, leading to deficiency and stagnation of Yang qi, which gradually depletes. As the disease deepens, it affects the root of the body’s constitution. Medications that benefit Qi and warm Yang have the effect of strengthening the body’s resistance and detoxifying, nourishing Qi and supporting Yang. These medications significantly improve symptoms of Qi deficiency and Yang deficiency, alleviating the Qi deficiency state in patients with Qi-deficient and Yang-deficient constitutions. They also markedly ameliorate symptoms such as fatigue and aversion to cold in patients with Yang-deficient constitutions. Yang is the extreme manifestation of Qi; when Qi is vigorous, Yang is abundant. In patients with advanced cancer, internal Yin toxins and pathogenic factors consume Yang qi. YWJP, with its mineral medications, aids in replenishing the internal consumption of Yang qi, slowing down or even reversing the depletion of inherent Yang qi. Consequently, symptoms of Qi deficiency and Yang deficiency, such as shortness of breath, fatigue, spontaneous sweating, cold limbs, aversion to cold, gurgling sounds in the intestines, curling up of the body, and abdominal distension, are significantly improved after intervention with Chinese medicine. This intervention has a universally beneficial effect on the Qi and Yang deficiency states of patients with different constitutions. It demonstrates notable efficacy in alleviating Qi deficiency in patients with Qi-deficient constitutions and fatigue and aversion to cold in patients with Yang-deficient constitutions. Additionally, there were no significant changes in patients’ KPS scores before and after treatment. Future studies could extend the observation period to explore the long-term efficacy of YWJP modifications in patients with recurrent or metastatic gastric cancer.
In this study, 55 patients were enrolled, and 40 patients completed the follow-up survey. The results showed that after treatment, there were slight decreases in BMI, NLR, and PNI, and a slight increase in MLR, but none of these changes were statistically significant. The same trends were observed in patients with Qi deficiency and Yang et al deficiency constitutions, also without statistical significance. Previous studies have identified high levels of NLR and MLR, as well as low levels of BMI and PNI, as poor prognostic factors for gastric cancer. After treatment with YWJP, patients showed a slight decrease in NLR, suggesting a marginal short-term improvement in immune-inflammatory status.51,52,56,58 However, the slight decreases in BMI and PNI, coupled with a slight increase in MLR, indicate that the overall prognosis remains poor. This result is presumed to be associated with the rapid progression and poor prognosis of patients with recurrent or metastatic gastric cancer. Although YWJP can improve some clinical symptoms of patients with recurrent or metastatic gastric cancer, there was no significant improvement in biological markers, suggesting that the prognosis remains unfavorable.
In the context of precision medicine, Professor Li et al has gradually evolved the TCM diagnosis and treatment model based on the “disease differentiation-syndrome differentiation-symptom differentiation” into a 5-in-one diagnosis and treatment approach that includes “disease differentiation-syndrome differentiation-symptom differentiation-constitution differentiation-stage differentiation.” Drawing from classical theories, he has proposed the 5-phase evolution law of “deficiency-cold-toxin-blockage-decay” and the 5-perspective system of diagnosis and treatment, namely, “spatiotemporal perspective, core perspective, symptomatic perspective, precision perspective, and preventive perspective.” According to this framework, Qi deficiency and loss of consolidation are the root causes of disease onset, while Yang deficiency and cold stagnation promote disease progression. The ultimate state is characterized by the decline of healthy Qi and the preponderance of pathogenic factors. In clinical practice, Professor Li emphasizes a dynamic and holistic approach, focusing on the core pathogenesis, concurrently regulating primary symptoms, precise targeting, and integrating prevention and treatment in the full-cycle management of Chinese medicine. This approach enhances the precision and targeting of clinical diagnosis and treatment.
According to the theory of traditional Chinese medicine, the spleen and stomach are considered the foundation of postnatal life and the source of qi and blood biochemistry. The spleen is responsible for transportation and transformation, while the stomach is responsible for reception and digestion. The absorption of nutrients from water and food as well as the metabolism of body fluids rely on the coordination of the spleen and stomach to complete, thus nourishing the entire body and limbs. If the spleen and stomach are inherently deficient or damaged by factors such as poor diet (irregular eating, consumption of cold foods), negative emotions, etc., the deficiency of Qi and Yang will occur due to the impairment of the spleen and stomach. The weakened function of Qi and Yang in promoting will lead to the disturbance of Qi movement, and the weakened defensive function of Qi and Yang will give rise to endogenous cancer toxins. Additionally, traditional Chinese medicine believes that the liver is responsible for regulating emotions. The liver belongs to the wood element, while the spleen and stomach belong to the earth element. In the 5 elements theory, wood restrains earth, so emotional factors such as anxiety and depression can affect the normal function of the spleen and stomach, leading to Qi stagnation in the body, obstruction of Qi, Yang, Yin, and blood, and ultimately the development of gastric cancer over time. Therefore, the spleen and stomach are closely related to the generation and distribution of Yang qi, and gastric cancer patients often exhibit a deficiency of Qi and Yang. From a microscopic perspective, the deficiency of Qi and Yang in the spleen and stomach results in the inability of Qi and blood to nourish the gastric mucosa, leading to thinning of the gastric mucosa, reduced blood flow, atrophy and damage of gastric folds, and weakened gastric motility. These changes are often accompanied by atypical hyperplasia or intestinal metaplasia, which can progress to gastric cancer over time. Therefore, as the key organs for generating and transporting Qi and blood in the human body, the spleen and stomach are more susceptible to factors such as cold diet and emotions compared to other types of cancer, leading to a deficiency of Qi and Yang. For patients with recurrent and metastatic gastric cancer, irregular diet and exposure to harmful foods or excessive consumption of cold foods can damage the middle warmer (spleen and stomach), resulting in insufficient generation of Qi and Yang. The deficiency of Qi and Yang, combined with the accumulation of cold toxins, leads to the formation of masses. Although the tangible Yin toxins are removed after surgery, the residual toxins remain hidden, and the instability of Qi and Yang allows cancer toxins to spread and block the Qi channels. The stagnation of Yang qi and the rampant spread of cancer toxins ultimately lead to recurrence and metastasis. Therefore, the core pathogenesis of patients with recurrent and metastatic gastric cancer is characterized by Qi and Yang deficiency and excessive pathogenic toxins. This study found that patients with recurrent and metastatic gastric cancer most commonly exhibit Yang deficiency and Qi deficiency constitution, and the disease is primarily characterized by Qi deficiency, Yang deficiency, and qi stagnation. These findings further support the clinical rationality of their core pathogenesis. Treatment with YWJP intervention has achieved certain clinical efficacy.
Due to the common clinical manifestations of Qi deficiency and Yang deficiency symptoms in patients with recurrent and metastatic gastric cancer, and the predominance of patients with Qi deficiency constitution, Yang deficiency constitution, Qi deficiency syndrome, and Yang deficiency syndrome in this study, clinical diagnosis and treatment often involve the adjustment of medications to tonify Qi and warm Yang. For patients with Qi deficiency, herbs such as Agrimonia pilosa (15 g), Rhizoma polygonati (10 g), and Rhizoma Dioscoreae (15 g) are commonly added to tonify the middle burner and replenish Qi. For those with Yang deficiency, herbs like Cassia twig (6 g), Galangal (6 g), and Epimedium (10 g) are selected to warm the middle burner and disperse cold. Additionally, wind-dispersing herbs, which can facilitate upward dispersion and circulation, are employed. As recorded in “Ben Jing Shu Zheng,” “Fangfeng (Saposhnikoviae Radix) is first pungent and then sweet, with the pungent taste predominating. Its action is based on its pungent taste to promote upward movement, combined with its sweet taste to harmonize the middle burner and enhance its dispersing effect.” Fangfeng, nourished by the Yang energy of heaven and earth, can enhance the efficacy of tonifying Qi and warming Yang medications when used together, as stated by Li dongyuan, “Huangqi (Astragali Radix) combined with Fangfeng enhances its efficacy.” For patients presenting with concomitant symptoms, flexible diagnosis and treatment should be applied according to the specific symptoms and syndromes, guided by the theory from “Jin Gui Yao Lue” which states, “For various diseases affecting the internal organs, treatment should be targeted according to the specific manifestations.”
This study had some limitations. Owing to the effect of the novel coronavirus epidemic, the sample size was small, and the geographical limitation of outpatient case collection may introduce statistical bias. The constraints of research time and funding prevented further investigation into the correlation between constitution, syndrome elements, and other objective indicators, such as tumor markers and immune indicators. Future studies would encompass a large-sample, multicenter, randomized controlled study on the treatment of gastric cancer recurrence and metastasis with TCM to optimize clinical evidence, explore the advantages of TCM, and enrich the clinical evidence of traditional TCM intervention.
Supplemental Material
sj-docx-1-ict-10.1177_15347354251331100 – Supplemental material for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study
Supplemental material, sj-docx-1-ict-10.1177_15347354251331100 for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study by Luchang Cao, Xinmiao Wang, Xinyi Ma, Guanghui Zhu and Jie Li in Integrative Cancer Therapies
Supplemental Material
sj-docx-10-ict-10.1177_15347354251331100 – Supplemental material for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study
Supplemental material, sj-docx-10-ict-10.1177_15347354251331100 for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study by Luchang Cao, Xinmiao Wang, Xinyi Ma, Guanghui Zhu and Jie Li in Integrative Cancer Therapies
Supplemental Material
sj-docx-11-ict-10.1177_15347354251331100 – Supplemental material for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study
Supplemental material, sj-docx-11-ict-10.1177_15347354251331100 for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study by Luchang Cao, Xinmiao Wang, Xinyi Ma, Guanghui Zhu and Jie Li in Integrative Cancer Therapies
Supplemental Material
sj-docx-12-ict-10.1177_15347354251331100 – Supplemental material for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study
Supplemental material, sj-docx-12-ict-10.1177_15347354251331100 for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study by Luchang Cao, Xinmiao Wang, Xinyi Ma, Guanghui Zhu and Jie Li in Integrative Cancer Therapies
Supplemental Material
sj-docx-13-ict-10.1177_15347354251331100 – Supplemental material for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study
Supplemental material, sj-docx-13-ict-10.1177_15347354251331100 for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study by Luchang Cao, Xinmiao Wang, Xinyi Ma, Guanghui Zhu and Jie Li in Integrative Cancer Therapies
Supplemental Material
sj-docx-14-ict-10.1177_15347354251331100 – Supplemental material for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study
Supplemental material, sj-docx-14-ict-10.1177_15347354251331100 for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study by Luchang Cao, Xinmiao Wang, Xinyi Ma, Guanghui Zhu and Jie Li in Integrative Cancer Therapies
Supplemental Material
sj-docx-15-ict-10.1177_15347354251331100 – Supplemental material for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study
Supplemental material, sj-docx-15-ict-10.1177_15347354251331100 for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study by Luchang Cao, Xinmiao Wang, Xinyi Ma, Guanghui Zhu and Jie Li in Integrative Cancer Therapies
Supplemental Material
sj-docx-2-ict-10.1177_15347354251331100 – Supplemental material for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study
Supplemental material, sj-docx-2-ict-10.1177_15347354251331100 for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study by Luchang Cao, Xinmiao Wang, Xinyi Ma, Guanghui Zhu and Jie Li in Integrative Cancer Therapies
Supplemental Material
sj-docx-3-ict-10.1177_15347354251331100 – Supplemental material for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study
Supplemental material, sj-docx-3-ict-10.1177_15347354251331100 for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study by Luchang Cao, Xinmiao Wang, Xinyi Ma, Guanghui Zhu and Jie Li in Integrative Cancer Therapies
Supplemental Material
sj-docx-4-ict-10.1177_15347354251331100 – Supplemental material for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study
Supplemental material, sj-docx-4-ict-10.1177_15347354251331100 for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study by Luchang Cao, Xinmiao Wang, Xinyi Ma, Guanghui Zhu and Jie Li in Integrative Cancer Therapies
Supplemental Material
sj-docx-5-ict-10.1177_15347354251331100 – Supplemental material for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study
Supplemental material, sj-docx-5-ict-10.1177_15347354251331100 for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study by Luchang Cao, Xinmiao Wang, Xinyi Ma, Guanghui Zhu and Jie Li in Integrative Cancer Therapies
Supplemental Material
sj-docx-6-ict-10.1177_15347354251331100 – Supplemental material for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study
Supplemental material, sj-docx-6-ict-10.1177_15347354251331100 for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study by Luchang Cao, Xinmiao Wang, Xinyi Ma, Guanghui Zhu and Jie Li in Integrative Cancer Therapies
Supplemental Material
sj-docx-7-ict-10.1177_15347354251331100 – Supplemental material for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study
Supplemental material, sj-docx-7-ict-10.1177_15347354251331100 for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study by Luchang Cao, Xinmiao Wang, Xinyi Ma, Guanghui Zhu and Jie Li in Integrative Cancer Therapies
Supplemental Material
sj-docx-8-ict-10.1177_15347354251331100 – Supplemental material for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study
Supplemental material, sj-docx-8-ict-10.1177_15347354251331100 for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study by Luchang Cao, Xinmiao Wang, Xinyi Ma, Guanghui Zhu and Jie Li in Integrative Cancer Therapies
Supplemental Material
sj-docx-9-ict-10.1177_15347354251331100 – Supplemental material for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study
Supplemental material, sj-docx-9-ict-10.1177_15347354251331100 for Exploration of Constitutional Bias and Associated Factors in Patients with Recurrent and Metastatic Gastric Cancer, and the Therapeutic Effect of Yiqi Wenyang Jiedu Prescription: A one-arm study by Luchang Cao, Xinmiao Wang, Xinyi Ma, Guanghui Zhu and Jie Li in Integrative Cancer Therapies
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.