
Abstract
This study investigated a dose-response relationship between Leisure-Time Physical Activity participation (LTPA) and the risk of diabetes and a comparison of the risk across different cognitive function groups among older adults. The Health and Retirement Study data were used from 2012 to 2020 (n = 18 746). This study conducted a Cox Proportional Hazard Regression to investigate the Dose-Response Curve between the prevalence of diabetes and the covariates following a level of LTPA participation. The result presented that the Odds Ratio continuously decreased as the level of LTPA participation increased. Among the three cognitive function groups, the high group (OR = .43, P < .05) and the mid group (OR = .71, P < .05) had a larger negative slope coefficient than the low group. This study found that LTPA participation reduces the risk of diabetes and gives evidence for the importance of cognitive function in reducing the prevalence of diabetes.
Introduction
Diabetes has emerged as a prominent chronic condition affecting older adults that results in significant health complications including heart disease, nerve damage, and risk for dementia and significant expenses related to medical treatment.1,2 The American Diabetes Association (ADA) has reported that over 26% of older adults suffer from diabetes mellitus and that 1.4 million Americans are diagnosed with diabetes every year.3–7 Older adults who are diagnosed with diabetes typically experience a reduction in their life expectancy of approximately 5 years, which highlights the severity of the impact of this chronic disease on mortality rates in this vulnerable population.8–11
Diabetes in older adults has been associated with a heightened risk of several complications and comorbidities including cardiovascular disease, renal disorders, infections, cancers, and an increased mortality rate.12–15 Thus, based on the statistical data and the observed health challenges and concerns associated with diabetes, researchers have stressed the importance of investigating the prevalence and mortality rates of diabetes and its impact on older adults.16–19 This finding of this investigation will provide researchers with critically needed data that can be used to design effective preventive strategies that can mitigate the growing burden of this disease.
Recently, a growing body of literature has reported findings related to the epidemiological association between diabetes mellitus and cognitive decline that provided conclusive evidence that diabetes is significantly associated with cognitive decline.16–19 One extensively supported mechanism involves the escalation of insulin resistance that leads to persistent elevation of blood glucose levels and the risk of diabetes. 20 Insulin resistance impacts both cerebrovascular and noncerebrovascular pathways and contributes to cognitive impairment in individuals with diabetes. 21 Insulin resistance triggers chronic hyperinsulinemia in the brain that results in elevated levels of beta-amyloid peptide-42, the primary constituent of amyloid plaques.22,23 The presence of amyloid plaques is a defining feature of Alzheimer’s disease, Alzheimer’s Disease and Related Dementias (AD/ADRD), and amnestic cognitive impairment.24,25 Moran et al 26 reported extensive changes in brain metabolites and structures in patients with diabetes that firmly established the association between diabetes and cognitive impairment.
While several studies have demonstrated that worsening memory and attention-processing function is related to the increasing prevalence of diabetes in older adults, the pathogenetic link between declining cognitive function and the risk of diabetes has not yet been fully elucidated.17,27 It is important for researchers to identify the changes in the risk of diabetes being followed by cognitive decline and design and implement interventions that effectively prevent the onset of diabetes among older adults.
It is well established that Leisure-Time Physical Activity (LTPA) is one of the most effective chronic disease prevention strategies for diabetes and the most important factor in promoting the health and wellbeing of older adults with diabetes.28,29 Previous findings presented evidence that LTPA contributes to increased cardiorespiratory fitness, enhanced vigor, improved glycemic control, reduced insulin resistance, optimized lipid profile, blood pressure reduction, and the sustainability of weight loss.30–32 Clinical studies have reported positive effects of LTPA on glycated h Hemoglobin A1C (HbA1C),33,34 triglycerides (TG), and cholesterol levels in individuals with diabetes compared to non-exercise comparison groups. 35 In addition, research has provided evidence that LTPA such as aerobic and exercise activities is associated with a 26% reduction in the prevalence of diabetes 36 and a 33% reduction in HbA1C levels, which are leading indicators of diabetes in older adults. For example, cohort studies have demonstrated an association between regular physical activity, moderate to high cardiorespiratory fitness, and reduced risk of diabetes and mortality in both type 1 and type 2 diabetes populations.37–39 Some studies have investigated the relationship between the level of LTPA participation and the risk of diabetes and found that older adults who frequently participated in LTPA were more likely to reduce the risk of diabetes onset.34,38,39 For example, engaging in a minimum of 150 minutes per week of aerobic physical activity, such as walking or jogging, and incorporating resistance exercises like weight training has been proven to be effective in reducing HbA1C levels and lowering the risk of diabetes. Moreover, moderate to vigorous levels of LTPA have a more significant impact on decreasing HbA1C and the risk of diabetes than lower-intensity LTPA.33,34
While a substantial number of clinical studies have reported that LTPA participation provides benefits that reduce the risk of diabetes and related diabetic symptoms,37–40 there is currently no longitudinal evidence of the relationship between different levels of LTPA participation and the prevalence of diabetes in older adults. Though prior studies investigated how diabetes is associated with cognitive function and have provided evidence that individuals with diabetes are likely to experience cognitive decline,16–19 little research has been conducted to examine the reverse relationship between different levels of cognitive function and the prevalence of diabetes.
In summary, the aim of this study is to: (a) investigate the longitudinal dose-response relationship between LTPA participation and the risk of diabetes, and (b) compare the risk of diabetes in three different cognitive function groups (i.e., low, mid, and high). The hypotheses that guided this investigation included:
Higher levels of LTPA participation reduces the risk of diabetes.
Higher levels of cognitive function reduces the risk of diabetes.
Methods
Data
This study used the Health and Retirement Study (HRS) data from 2012 to 2020 that has been biannually released since 1992 by the University of Michigan. The data includes a wide range of information about the health status of older adults and the demographic characteristics, pension, housing, and job history of individuals over 45 years old. The HRS uses not only a paper-based survey but also interviews (e.g., telephone, in-person) to gain proxy-measured and biofeedback data. While a similar survey format has been used since initial data collection, the HRS has modified the instruments, questionnaires, and domains they have used over time. We employed data from 2012 to 2020 as each dataset in that timeframe is comprised of identical domains and instruments.
The HRS has used their own data collection protocol to follow up with study respondents. The respondents in the survey participant pool have been identified with Person Identification Numbers (PN) and a Household Number (HH). Changes in family structure such as births, deaths, or divorces are recorded in the HH. For instance, if PN1 and PN2 in HH-1 experience a divorce, they are redesignated as PN1 in HH-1 and PN2 in HH-2. Similarly, if an PN1 in HH-1 has a second marriage, the HH-1 has PN1, PN2.
Study Sample
This study tracked participant samples from 2012 to 2020. Figure 1 shows the overview of the longitudinal follow-up of the study sample populations. The study samples were extracted using the following protocol: (a) the year 2012 as the baseline, (b) track from 2012 to 2020, (c) participants must be over 50 years old, and (d) exclude respondents who had null values in a dependent variable during the period. The total study sample of this study following this protocol was 18 746. Flow Chart of the Longitudinal Follow-up of Study Participants.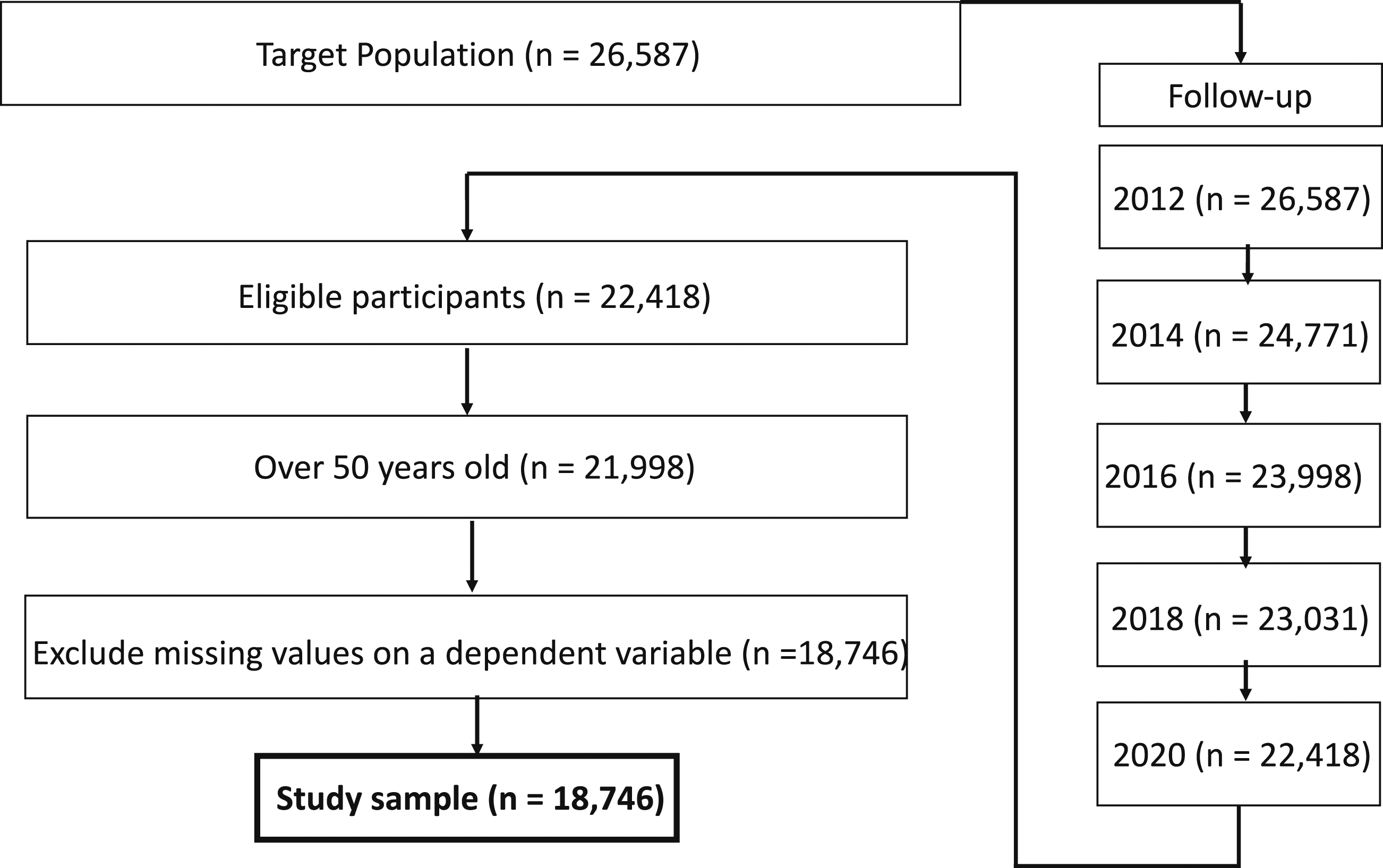
Measurements
Dependent Variables
Diabetes
The onset of diabetes was screened by a questionnaire item: “Has a doctor told you that you have diabetes?” to which respondents answered either “Yes” or “No.” Each answer was coded as 1 = ‘Yes’ and 0 = ‘No’. The HRS provides information about the time of diabetes onset using an item: “In what year was your diabetes first diagnosed?”
This study encompassed samples that consistently provided the same answers on the diabetes diagnosis questionnaire between 2012 and 2020. For instance, if a study participant indicated that they were diagnosed with diabetes in 2014, they were required to report having diabetes in 2016, 2018, and 2020 to be included in the study sample. We only included respondents who were diagnosed with diabetes after 2012 and used the 2020 data to investigate whether the study participants had diabetes. However, this study did not consider the timing of when participants were diagnosed with diabetes between 2012 and 2020, nor did it include information about whether the diabetes diagnosis was type 1 or type 2.
Independent Variable
Leisure-Time Physical Activity
The Psychosocial domain (i.e., LB) was comprised of information about 21 types of leisure activities. This study extracted two items to construct the LTPA variable: “Play sports or exercise” and “Walk 20 minutes or more”.41,42 A seven point Likert scale was used to assess the level of LTPA participation (1 = ‘Daily’ and 7 = ‘Never relevant’). The scale was reverse coded to use a high score to represent a high level of LTPA participation. We summed LTPA participation each year from 2012 to 2020 to calculate total participation.
Covariates
Cognitive Function The HRS cognition section elicits comprehensive information regarding the cognitive function of older adults via in-person and/or telephone interviews. The HRS has consistently used the telephone Interview for Cognitive Status-27 (TICS-27) for cognitive assessment and collects two types of cognition data using the same instrument: Patient-Reported Outcome (PRO) and Proxy-Measured Outcome (PMO). The HRS interviewer decides whether to use PRO or PMO method based on the responsiveness of the interviewee. If the interviewee can respond reliably to the questionnaire, the interviewer collected data from the interviewee using the PRO method. However, if the interviewee was not reliable and responsive to the questions, the interviewer would use the PMO method that requires support from caregivers. Therefore, PRO data indicates that the respondents are able to answer to the questions independently, and data users can expect PRO data to be reliable. This study employed the PRO method to collect cognitive function data with respondents who were able to engage in the tests without support. These respondents were not considered cognitively impaired, even if they had a low score on each test or had been diagnosed with dementia.
The TICS-27 is comprised of cognitive tests assessing three domains of cognitive function: memory, working memory, and attention and processing speed. The total cognitive function score was derived by adding the results of the three cognitive function tests, with a scoring range of 0 to 27.43–45 The memory domain was assessed using both recall and delayed recall tests. The interviewer presented 10 random words to the interviewees and asked them to recall as many words as possible immediately in the recall test and then asked them to recall the same 10 words again five minutes later in the delayed recall test (e.g., car, tree, cloud). Each correctly answered word had a one-point value and the total memory score ranged from 0 to 20. The seven-subtraction test was used to measure working memory that requires processing and storing information simultaneously. The respondents were asked to subtract 7 from 100 five times (e.g., 100-7 = 93, 93-7 = 86, 86-7 = 79). Each correct answer was given one point resulting in a total score that ranged from 0 to 5. Attention and processing speed were measured using a counting backward test.44,45 The respondents were asked to count backward 10 continuous numbers from 20 in two trials (e.g., 20, 19, 18, 17). Each correct trial has one point value and score ranged from 0 to 2.
A TICS-27 score of 6 or below indicates cognitive impairment, whereas a score falling between 7 and 11 suggests cognitive impairment without meeting the dementia threshold, commonly referred to as MCI. Scores ranging from 12 to 27 are deemed to be within the normal cognitive status range as established by previous studies. Therefore, we classified study samples into three cognitive groups (i.e., low, mid, and high) according to their TICS-27 scores. The low group included scores from 0 to 6, the mid group from 7 to 11, and the high group from 12 to 27. The high group was comprised of participants with higher cognitive function than the mid and low groups.
Age and Sex
Effective coefficient estimation with covariates requires predictable outcomes and low correlation with the study variables to avoid multicollinearity risks. 46 Previous diabetes studies considered covariates such as age, sex, weight, and height.47–49 Thus, we confirmed a correlation with study variables and put age and sex in 2012 as covariates as they were available in the HRS data.
Analysis
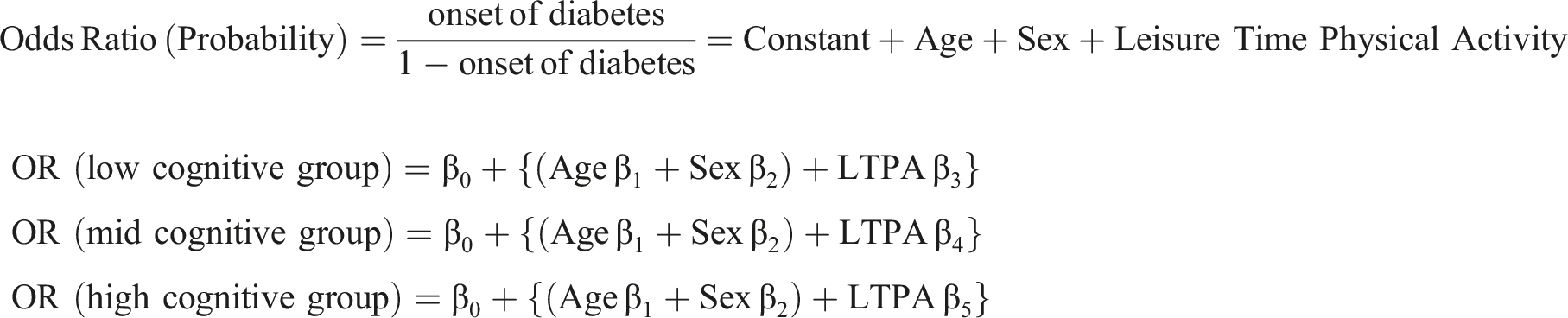
This study employed a Cox Proportional Hazard Regression to investigate the Dose-Response Curve (DRC) between the prevalence of diabetes and the covariates (i.e., age, sex, cognitive function) based on varying levels of LTPA participation. The Odds Ratio (OR) indicates the probability that the study sample is diagnosed with diabetes. An OR of 1.0 means that the individual has a 100% risk of diabetes and an OR of .70 indicates that, after a specific intervention, the intervention has reduced the risk of diabetes by 30%, indicating a 70% risk of diabetes. The DRC presents the OR as changing coefficients of covariates. The aim of this study was to calculate each covariate coefficient and describe the OR changes as LTPA participation increases. This study not only visualized the changes of the OR as LTPA levels increased, but also compared the OR in three different levels of cognitive function (i.e., low, mid, and high). All statistical analyses were conducted using the SPSS version 29.0 statistical package. The regression equation was as follows:
Results
Demographic variables.
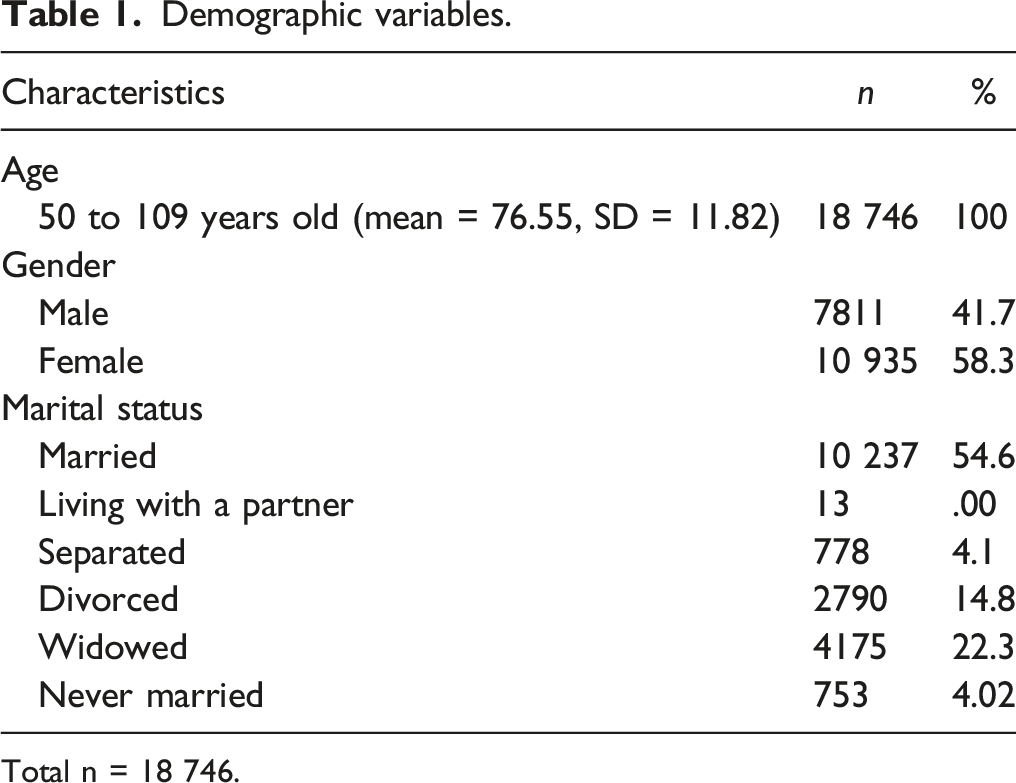
Total n = 18 746.
Descriptive Statistics.
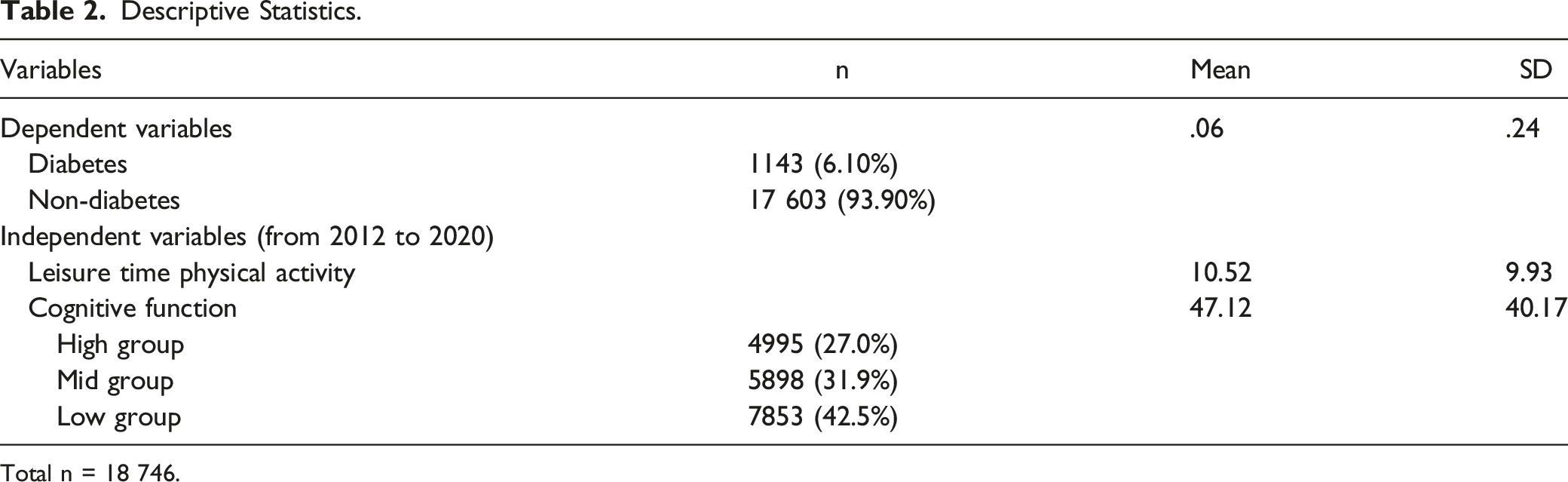
Total n = 18 746.
Omnibus Tests of Model Coefficients.

The increase of the OR LTPA participation levels is illustrated in Figure 2. The OR continuously decreased as the level of LTPA participation increased. In the next phase, the OR of diabetes was compared to the three different levels of cognitive function as the level of LTPA participation increased. The low cognitive function group was used as a baseline to compare the OR of diabetes with the mid and high LTPA groups. The equation consisted of three covariates (i.e., parameters): age, sex, and three different cognitive function levels. The OR of diabetes showed a negative slope with increasing age (OR = .99, Wald = 1.14, df = 1, P > .05) and sex (OR = .95, Wald = .40, df = 1, P > .05) but not at significant levels. Cox proportional Hazard regression: Diabetes.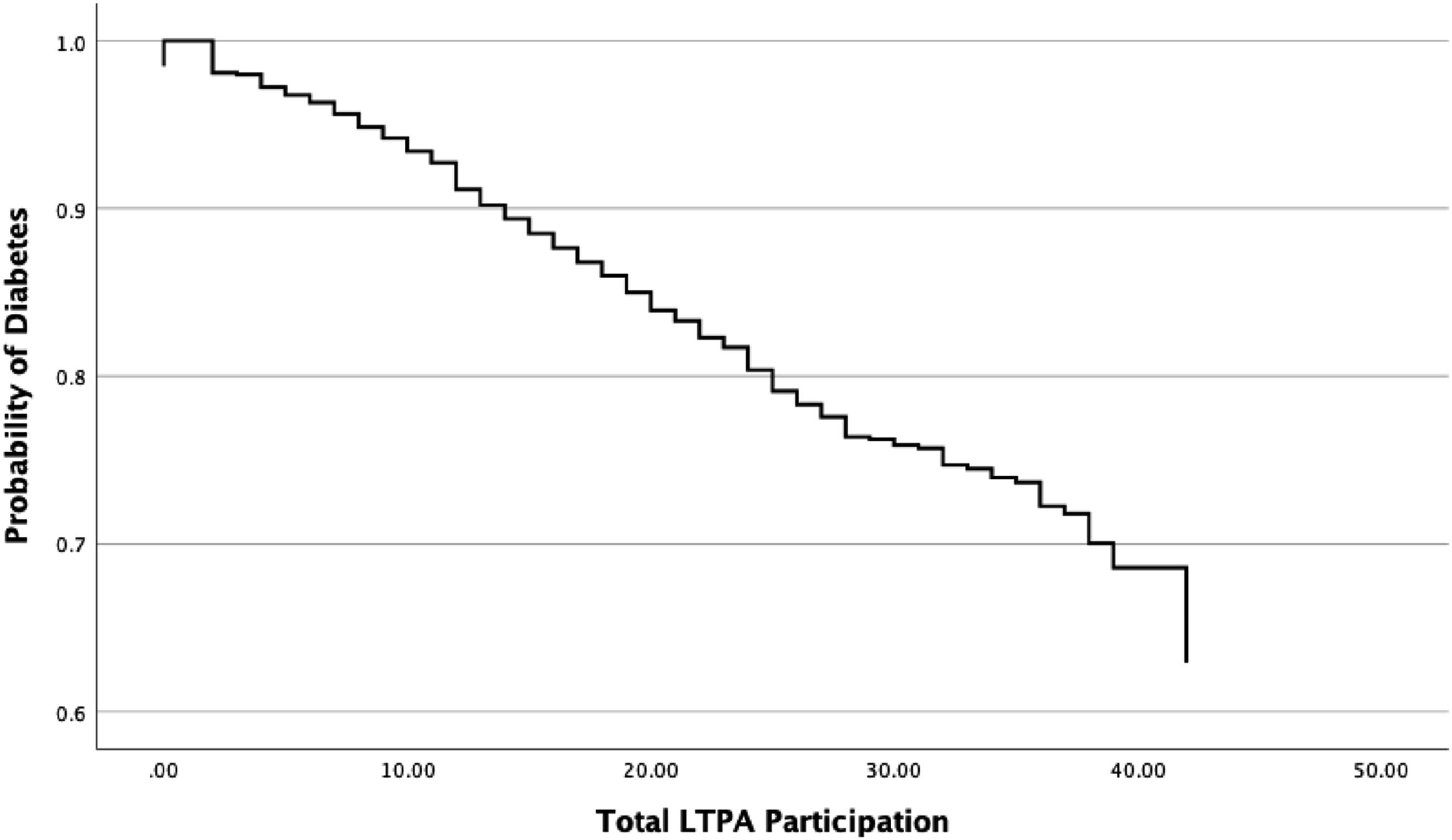
Variables in the Equation.
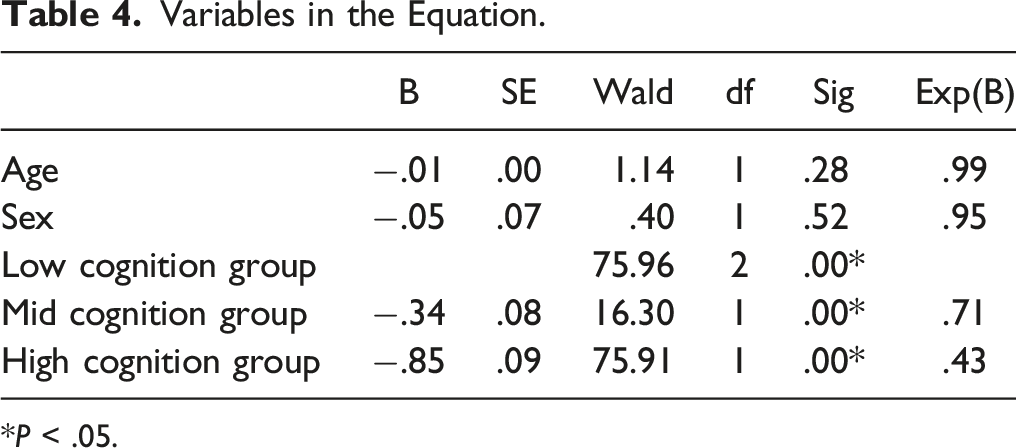
*P < .05.
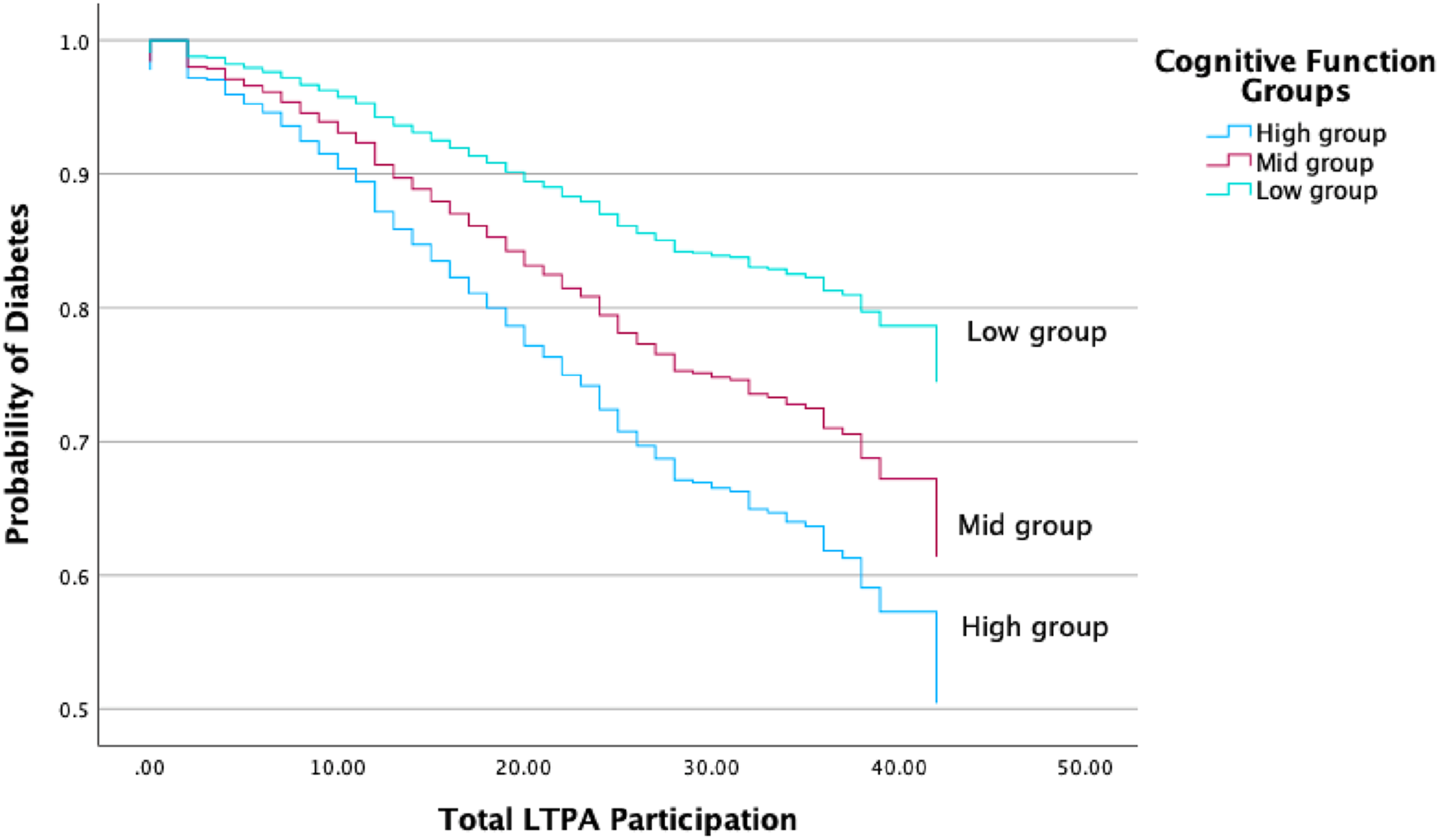
Dose-response curve in different cognitive function groups.
Discussion
This study demonstrates a longitudinal dose-response relationship between LTPA participation and the risk of diabetes, and a comparison of the risk of diabetes across different cognitive function groups. This study provides empirical evidence that LTPA participation reduces the risk of diabetes and gives evidence for the importance of cognitive function in reducing the prevalence of diabetes among older adults. This finding suggests that high levels of LTPA participation and cognitive function play an important role in reducing the risk of diabetes among older adults.
Substantial evidence has been presented in the literature that LTPA participation has been associated with reducing the risk of diabetes among older adults and increasing the health and wellbeing of people diagnosed with diabetes.33,34,40 Previous studies that were conducted using a cross-sectional methodology or in clinical settings reported that LTPA participation is effective in reducing the onset of diabetes among older adults.35,37–39 Our longitudinal study also indicates that 10 years of LTPA participation was a significant factor in the reduction of the prevalence of diabetes. This longitudinal study extends and supports previous findings.37–40 that LTPA participation is associated with a reduction in the risk of diabetes and the biomarkers related to diabetes. Our findings provide a cause-effect relationship between LTPA participation and the prevalence of diabetes, and it suggests that health professionals must continue to design and implement LTPA programs for older adults to reduce the onset of diabetes in this population.
As diabetes is recognized as a substantial risk factor for AD/ADRD, individuals diagnosed with diabetes face a 39% increased risk of AD and a 47% increased risk of dementia compared to nondiabetic patients.24,25 These studies demonstrate the negative effect of diabetes on cognitive function and indicate that older adults with diabetes are likely to experience cognitive decline and an increased risk of AD/ADRD. Prior studies have provided evidence that diabetes is negatively associated with cognitive function among older adults.16–19 Conversely, this study investigated the relationship between cognitive function and the onset of diabetes and found that the high cognitive function group exhibited a lower OR of diabetes compared to the mid and low cognitive function groups even though they had the same level of LTPA participation. This finding indicates that older adults who possess high levels of cognitive functioning are less likely to contract diabetes as it adds evidence to the literature that improving cognitive function among older adults can reduce the risk of diabetes in older adults that has heretofore been missing.
Overall, this study highlights the importance of LTPA participation as a strategy that can be used to reduce the risk of diabetes among older adults, and that improving cognitive function is essential to reducing the risk of diabetes for older adults. Based on these results, our study makes some practical suggestions on how to reduce the prevalence of diabetes among older adults. A recent systematic review and meta-analysis indicated that short-term (<1 year) multidomain (including two or more nonpharmacological components such as cognitive exercises and LTPA) intervention participation is associated with improvements in cognitive function in older adults when compared with single-domain interventions. 51 This study suggests that the design and implementation of a multidomain program that includes exercise programs and cognitive training (especially in a digital format) should be used to reduce the risk of diabetes in the older adult population.
Limitations
There are several limitations inherent to this study that can affect its application to future research. Considering the nature of the secondary data sets used, our research did not include the types of diabetes (e.g., type 1 or type 2) due to the lack of availability of this information. As different types of diabetes may affect the design and specific contents of an LTPA program, future studies are needed to investigate which type of diabetes are best addressed with LTPA and cognitive function training. Furthermore, this study did not consider the timing of participants' diabetes diagnoses between 2012 and 2020. As the time of diabetes diagnosis may affect the relationship between the prevalence of diabetes and LTPA, future researchers will be able to control the timeframe for how long the study samples have been diagnosed with diabetes. In addition, this study specified three cognitive function groups based on aggregate MoCA scores. Each category of cognitive function can be associated with LTPA participation and the onset of diabetes among older adults. Investigating the relationship between each cognitive category and LTPA participation provides more insightful information to researchers. Last, there are confounders that may affect the association between diabetes and LTPA participation such as comorbidities and other related factors (e.g., cardiovascular disease, heart function, and limitations to mobility and LTPA access). Future research is needed to investigate how these comorbidities and related factors are associated with the association between the onset of diabetes and LTPA participation.
Footnotes
Data Availability Statement
The datasets generated and analyzed during the current study are available at: https://hrs.isr.umich.edu/
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was carried out with the support of the ‘R&D Program for Forest Science Technology (Project No. 2021387D10-2323-0101),’ provided by the Korea Forest Service (Korea Forestry Promotion Institute).