
Abstract
Background
To examine the effect of combination exercise program on cognitive function of older adults with mild cognitive impairment (MCI), and identify biomarkers associated with improvement of cognitive functions.
Methods
Subjects were 42 older adults (ages, 60-80 years) with MCI. The subjects were randomly classified to traditional Chinese exercise combined with rhythm training group (TCE + RTG, n = 14), walking group (WG, n = 14), and control group (CG, n = 14), according to their level of MMSE scores. These groups exercised for 60 minutes at 1 session, 3 sessions a week for 12 weeks. The intervention program was conducted under multitask conditions to stimulate attention and memory, and the control group attended 3 education classes. Measurements were administered before, after the 6-week, and after the 12-week intervention period; Measurements: The Mini-mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), Symbol Digit Modalities Test (SDMT), Activities of Daily Living Scale (ADL), and the 17-item Hamilton Depression Scale (HAMD-17), along with the brain-derived neurotrophic factor (BDNF). A repeated-measures analysis of variance was used to examine differences among the 3 groups and between the 3 testing times (pre-test vs middle-test vs post-test).
Results
(1) The TCE + RTG showed significant improvement in the MMSE, MoCA, SDMT, and ADL scale test results (P < .01) and HAMD-17 scale test results (P < .05). The WG also showed significant improvement in the MMSE, MoCA, and HAMD-17 scale test results (P < .05) and the ADL scale test results (P < .01). While there was no significant change in the CG after the intervention. (2) The TCE + RTG and WG showed positive improvement in peripheral blood BDNF levels, while the CG showed a decrease in these test results. There were significant differences between the TCE + RTG and CG before and after the intervention.
Conclusion
The results suggested that a TCE + RT is beneficial for improving memory and maintaining general cognitive function and peripheral blood BDNF levels in older adults with MCI. Peripheral blood BDNF levels may predict improvement of cognitive functions in older adults with MCI. Further studies are required to determine the positive effects of TCE + RT on cognitive function in older adults with MCI. Trial Registration: ChiCTR2200058545, Registered 10 April 2022.
Keywords
Introduction
Cognitive impairment (CI) is a syndrome characterized by progressive degeneration of memory, learning, execution, attention, calculation, understanding, or judgment. 1 The elderly population is at high risk of developing cognitive impairment, with approximately 10% to 15% of the population over the age of 65 developing CI, and more than half of these individuals further progressing to dementia within 5 years. 2 As of 2018, there were 50 million people with CI worldwide, and this is expected to reach 82 million by 2030 and 152 million by 2050. CI not only has a serious impact on the quality of life of older adults, but also places a significant financial burden on the health care system.3,4 However, medication has not led to important breakthroughs in the treatment of CI, and can even be ineffective, cause side effects, or result in medication tolerance,5–7 which leads a preference for non-pharmacological approaches to slow the progression of CI.
Traditional Chinese exercise (TCE) is widely used to improve CI in older adults due to its excellent health benefits, high level of safety, lack of special requirements, and ease of learning.8,9 Previous studies have mainly focused on Tai Chi (TC), Baduanjin, Qigong,10–12 and acupoint massage. 13 Studies on the efficiency of TC on patients with CI have indicated that TC improves their function significantly, including overall cognitive function, memory and learning, visuospatial ability, executive functions, and physical activity.14–16 Baduanjin training also has been shown to have positive benefits on global cognitive function, attention, executive function, and processing speed in older adults with mild cognitive impairment (MCI).10,17,18 Liu et al. performed a meta-analysis to evaluate the usefulness of acupoint massage in preventing cognitive decline in older adults and suggested that acupoint massage is an effective intervention for maintaining their cognitive function. 13
Some studies have shown that TCE is more beneficial to cognitive function improvement in older adults than other forms of exercise. Specifically, in a pair-wise meta-analysis, traditional Chinese medicine (TCM) exercise therapies (Baduanjin exercise, Tai Chi, Liuzijue exercise and finger exercise) were superior to non-TCM exercise therapies (stretching and toning exercise, usual care, health education, and routine daily activities) in terms of the Mini-mental State Examination(MMSE), Montreal Cognitive Assessment (MoCA), and Activities of Daily Living Scale (ADL) outcomes. 19 Yue et al. performed resting-state functional magnetic resonance imaging (rsfMRI) scans on TC practitioners and walking participants and showed that regular TC training is more conducive to optimizing the brain functioning and networking of the elderly. 20 Lam et al. also found that the TC group had better preservation of the Clinical Dementia Rating (CDR) sum of boxes scores than the stretching and toning exercise group; the TC group also had greater improvement in delay recall and Cornell Scale for Depression in Dementia scores. 21 Moreover, Xia et al. demonstrated that Baduanjin significantly increased the selective attention of patients with MCI and the dorsal attention network (DAN) compared with brisk walking (BWK) exercise or usual physical activity (UAP). 22 Moreover, Jin et al. found that Qigong practice was significantly superior to stretching exercise not only for the prevention of cognitive decline progression, but also for the improvement of several cognitive functions among older adults at risk of cognitive decline. 11 Qigong was found to cause significant improvement in processing speed and sustained attention, increased hippocampal volume, and reduced peripheral interleukin-6 (IL-6) levels, resulting in an increase and improvement in processing speed performance and sustained attention. 23
Recent studies have proved that rhythm training (RT) is also helpful to improve CI.24,25 RT is based on both music and movement elements of the exercise form, focusing on exercises driven by the rhythm of music. 26 Music intervention is a noninvasive and inexpensive therapy that appears to reduce depression among the elderly; it also delays the deterioration of cognitive functions, particularly short-term recall. 27 Some studies suggest that nursing facilities for older adults with dementia should incorporate group music intervention into routine activities in order to enhance emotional relaxation, create inter-personal interactions, and reduce future agitated behaviors. 28 Studies have found that RT promotes intellectual development in young children and is beneficial for motor skill development in children and adolescents,24,25 but whether RT is beneficial for cognitive function in older adults with MCI has not been studied.
Although TCE has been recommended as an effective and safe exercise for older adults aged 60 and over, no conclusion has been reached about whether TCE + RT can show more benefits than a single intervention for the elderly with MCI. Studies have confirmed that a combination of training with multiple modalities can be more effective at improving cognitive performance in older adults with MCI.29–31 Therefore, this study aimed to assess the effects of TCE + RT on older adults with MCI through a randomized controlled trial.
Materials and Methods
Participants
We recruited 88 subjects in the Dongcheng District community of Beijing through media advertising and community outreach between March and July 2022.
The inclusion criteria were: (1) Subjects aged 60 to 80 years old who had been diagnosed with MCI; (2) Subjects who signed an informed consent form, agreed to be assigned to any group to participate in the experiment, were willing to complete all parts of the study, and were capable of doing so alone or with the help of a caregiver; (3) Subjects had not undergone any adjustment in drug type or drug dose within 6 months prior to enrollment and their condition remained relatively stable; (4) Subjects educated to primary education literacy level or higher, with the ability to read, write, and communicate effectively prior to the onset of illness; (5) Subjects took part in an entry group self-test (Simple memory test > 13). The following exclusion criteria applied: (1) Weight < 40 kg; (2) Blood pressure <90/60 mmHg or >160/100 mmHg, systolic or diastolic blood pressure fluctuation >30 mmHg 2 weeks before enrollment; (3) Subjects were participating in other pharmacology studies or coach-directed exercise programs; (4) Physical weakness or impaired vision, unable to understand the test; (5) Metal foreign bodies in the skull and eyes, artificial cardiac pacemakers, and nerve stimulators. Five participants were unable to complete the follow-up assessment due to lack of time. 57 participants completed baseline neuropsychological assessments, with 42 meeting the inclusion criteria (Figure 1). The purpose of the study, duration, intervention plan, and assessment test schedule were explained to the subjects at the beginning of the study and before they were enrolled. Each participant was assured that their participation in the study was on a voluntary basis, and they had the right to be informed of their test scores and the right to withdraw from the study at any time. Outline of the flow of participants from first contact to study completion.
Design
The study used a randomized block group experimental design. And the sample size was calculated using G*Power Software, Considering a power of 80%, an effect size of .25, α of .05, number of groups is 3, number of measurements is also 3, and nonsphericity correction is 1, twelve subjects were required at least. All subjects were divided into 3 groups according to their level of MMSE scores: TCE + RTG (n = 14), WG (n = 14), and CG (n = 14). Each subject was informed of the risks associated with the training and measurements and gave written consent to participate in the study, which was approved by the Ethics Committee of the Beijing Sport University. Testing was conducted before the initiation of training (pre), at the mid-point of training (middle), and after 12 weeks of training (post). During the study, an ActiGraph GY3X + accelerometer (ActiGraph, Ft. Walton Beach, USA) measured the subject’s physical activity level, counting as an average acceleration per minute (vector magnitude counts/min) as an evaluation index. 32 And all subjects had set dietary plans that were consistent across the training blocks and were designed to meet their body weight and activity needs. Subjects were encouraged to ensure they got a minimum of 8 hours of sleep, and a self-reported log suggested they achieved this regularly.
Intervention
The Main Content of the TCE + RTG.

WG: After finishing the same warm-up as the TCE + RTG, the subjects performed a 10-minute relaxation phase. They went on a 60-minute 3 km walk with 3 sessions a week for 12 weeks. The intensity of the exercise in the WG was similar to that of the TCE + RTG.
In addition, all participants in the intervention and CG participated in monthly health science knowledge dissemination activities, which included knowledge on diseases related to CI in older adults, memory care, seasonal disease prevention, and prevention of common chronic diseases in older adults.
Neuropsychological Assessment
Cognitive assessments were performed by neuropsychologists according to standardized methods. These included the Mini-mental State Examination (MMSE), the Montreal Cognitive Assessment (MoCA), the Symbol Digit Modalities Test (SDMT), the Activities of Daily Living Scale (ADL), and the 17-item Hamilton Depression Scale (HAMD-17). (1) MMSE, Mini-mental State Examination: 33 It assesses patients’ cognitive function orientation, memory, calculation, language ability, visuospatial and utilization ability, etc. It is more sensitive and specific for dementia diagnosis, but not sensitive enough to identify MCI. (2) MoCA-BJ, The Beijing version of the Montreal Cognitive Assessment: 34 a scale that assesses 8 cognitive domains (including attention and concentration, executive functioning, memory, language, visual structure skills, abstract thinking, computation, and orientation) from alternating connective tests, visuospatial and executive functions (cubes, clocks), naming, memory, attention, sentence repetition word fluency, abstraction, delayed recall, and orientation. (3) SDMT, Symbol Digit Modalities Test: 35 This is mainly used to assess subjects’ attention, working memory, visual perceptual ability, information-processing speed, and motor speed; it is sensitive to frontal and parietal lobe damage. The SDMT is widely used in the assessment of cognitive function in patients with various neurological disorders. (4) ADL, Activity of Daily Living Scale: 36 developed by Lawton and Brody in 1969, it assesses the ability of subjects to perform daily activities. The ADL consists of 20 items, including 6 areas related to physical self-care (toileting, eating, dressing, grooming, walking, and bathing) and 8 areas related to the ability to use tools (telephone, shopping, strolling, housework, laundry, using transportation, taking medication, and taking care of one’s own finances). If the total score of the scale results is less than or equal to 26, then the assessment returns a normal result; if it is greater than 26, then the subject is assessed as having different degrees of functional decline. If a single item is scored 1, then this is assessed as normal; 2 to 4 signifies functional decline. Two or more scores greater than or equal to 3, or a total score greater than or equal to 22 are indicative of significant functional impairment. (5) HAMD-17, 17-item Hamilton Depression Scale: 37 used with adult patients with depressive symptoms and has a total score that reflects the severity of the condition. The problems associated with depression are grouped into 7 subcategories: anxiety or somatization, weight, CI, day–night variation, blockage, sleep disturbance, and feelings of hopelessness. It is generally considered that a total score of less than or equal to 7 is normal, 7 to 17 means that the subject is likely to have depression, depression can be diagnosed when the total score is 17 to 24, and severe depression is indicated when the total score is greater than or equal to 24.
Peripheral Blood Index Test
Brain-derived neurotrophic factor (BDNF) is mainly found in the hippocampus, cerebral cortex, hypothalamus, and cerebellum brain regions. It is closely related to central and peripheral energy metabolism and homeostatic molecular processes, and is a key molecule involved in changes in learning memory plasticity. 38 Therefore, memory function can be assessed by examining BDNF in cognitively impaired older adults. In this study, community health service center nurses assisted in blood collection, each drawing 5 mL of venous blood. The drawn venous blood was first placed at room temperature, and after all the blood was drawn (after about 30 minutes) the blood samples were transferred to the Institute of Sports Science of the State General Administration of Sports for serum centrifugation in an incubator at low temperature, and the centrifuged serum was divided and stored in a freezer at −80° for testing. The blood centrifuge was a low-temperature centrifuge with a centrifugation speed of 3000 rpm for 20 minutes. The BDNF test used an enzyme-linked immunosorbent assay (ELISA); the kit included a 96-well Immunoway imported brand of human serum BDNF kit (Item No. KE1464), an ELISA test instrument using the Omega BMG Labtech fluorescent multifunctional enzyme labeling instrument, and a Bio-Tek plate washer in strict accordance with the kit instructions for the experiment.
Statistical Analysis
Statistical analysis was performed using SPSS v.26.0 (SPSS Inc., IBM, China). The data in tables and figures are presented as mean ± standard deviation. The Shapiro–Wilk, Levene, and Mauchly’s tests were used to verify the normality, homogeneity, and sphericity of the sample’s data variances, respectively. At pre-test, between-group comparisons were analyzed by univariate analysis of variance (ANOVA), and between-group comparisons under the influence of experimental treatment were analyzed by repeated ANOVA [group (TEC + RTG, WG vs CG) × time (pre-test, middle-test vs post-test-12 weeks)] was used. When a significant interaction or main effect was found, post hoc comparisons with Bonferroni adjustment were used to test the discrimination between means. Statistical significance was set at P < .05.
Results
Baseline Data
Baseline Demographic Information for the Intervention and CG.
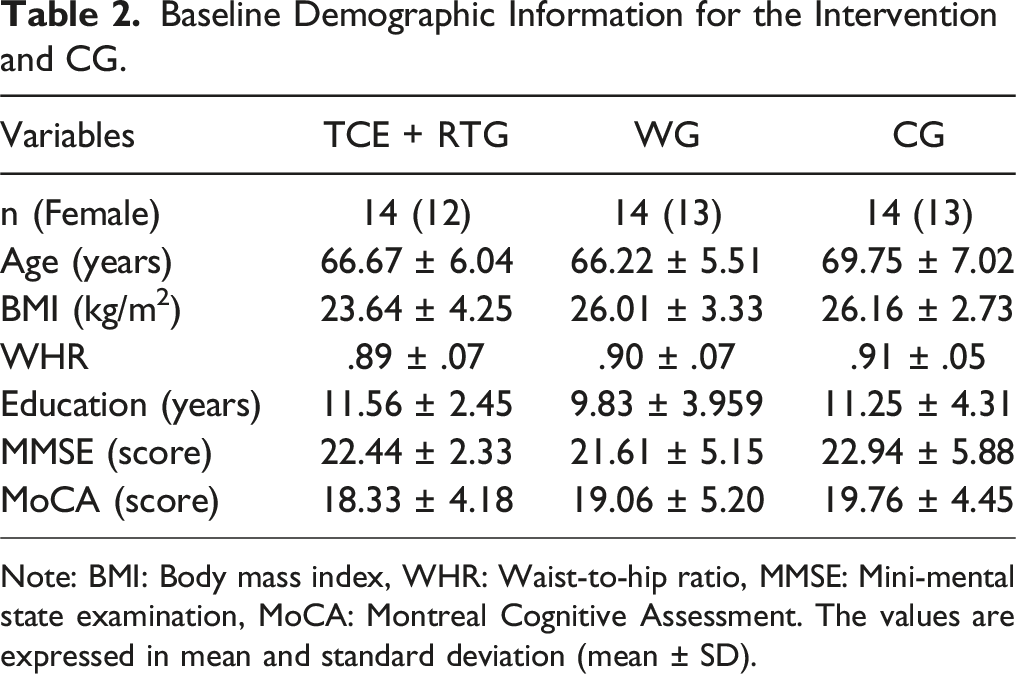
Note: BMI: Body mass index, WHR: Waist-to-hip ratio, MMSE: Mini-mental state examination, MoCA: Montreal Cognitive Assessment. The values are expressed in mean and standard deviation (mean ± SD).
MMSE Scores
Comparison of MMSE Scores Before and After the Intervention.

Note: * significant difference compared to pre-intervention (P < .05). ** highly significant difference compared to pre-intervention (P < .01). aa highly significant difference compared with 6 weeks of intervention (P < .01). ˄ significant difference between groups at different time points (P < .05).
MoCA Scores
Comparison of MoCA Scores Before and After the Intervention.

Note: * significant difference compared to pre-intervention (P < .05). ** highly significant difference compared to pre-intervention (P < .01). aa highly significant difference compared with 6 weeks of intervention (P < .01). ˄ significant difference in intervention outcomes between groups at different time points (P < .05).
SDMT Scores
Comparison of SDMT Scores Before and After the Intervention.

Note: * significant difference compared to pre-intervention (P < .05). ** highly significant difference compared to pre-intervention (P < .01).
ADL Scores
Comparison of ADL Scores Before and After the Intervention.

Note: * significant difference compared to pre-intervention (P < .05). ** highly significant difference compared to pre-intervention (P < .01). ˄significant difference in intervention outcomes between groups at different time points (P < .05).
Compared to the pre-intervention period, TCE + RTG and WG subjects showed highly significant differences in the ADL Scores after 12 weeks of intervention (P < .01), while the WG also showed highly significant differences in that after 6 weeks of intervention (P < .01). There was only a significant difference in the ADL Scores between the WG and CG at 12 weeks after the intervention (P < .05), and no difference in test results between the 3 groups at the pre-intervention and 6-week tests.
HAMD-17 Scores
Comparison of HAMD-17 Scores Before and After the Intervention.

Note: * significant difference compared to pre-intervention (P < .05). ** highly significant difference compared to pre-intervention (P < .01). a significant difference compared with 6 weeks of intervention (P < .05).
Peripheral Blood Index Test
Results of BDNF Level Test Before and After the Intervention.

Note: * significant difference compared to pre-intervention (P < .05). ** highly significant difference compared to pre-intervention (P < .01).
Discussion
The results of our study demonstrated that both the TCE + RTG and WG interventions improved the cognitive function of the subjects. However, there was a more pronounced interventional effect in the TCE + RTG, while the CG showed no significant decrease in cognitive function. This further suggests that a combination of interventions in multiple modalities may offer more benefits in terms of improving cognitive and physical function for older people with MCI than a single-round intervention approach. 39
Our results showed significant improvement in the MMSE (P < .01), MoCA (P < .01), SDMT (P < .01), ADL (P < .01), and HAMD-17 (P < .05) in the TCE + RTG after 12 weeks of intervention. This indicates a significant increase in the overall cognitive function of the subjects in the MMSE and MoCA scales, in the areas of attention and working memory and information-processing speed of the subjects in the SDMT test, improvement in self-care and tool use of the subjects in the ADL test, and in the depression of the subjects in the HAMD-17 test.
The multidomain supervised intervention used in the present study was feasible and safe. The TCE + RTG performed aerobic exercise of moderate intensity or less. Studies have shown that increased blood flow in specific areas of the brain during aerobic exercise can cause changes in prefrontal cortex (PFC) activity, 40 with positive effects on the cognitive domain and vascular endothelial growth factor; brain-derived neurotrophic factor (BDNF) can enhance the plasticity of the cerebral motor cortex, and lactic acid can have a positive effect on BDNF. In addition, aerobic exercise can produce changes in the volume of human white matter, delay the shrinkage of white matter, and enhance the connectivity of the prefrontal cortex. 41 This is consistent with our findings, but the exercise content arranged in the TCE + RTG intervention differed from ordinary aerobic training by integrating the characteristics of drill training, traditional Chinese exercise movements, acupoint massage, and listening to music. The content was richer and had multiple points of cognitive stimulation for the subjects. In the 12-week intervention training program, subjects needed to learn and participate in changing motor movements, and the process of motor learning itself included the participation of various cognitive functions such as motor memory, visuospatial orientation, selective attention, and executive function. Leisman et al. argued that further support for the connection between movement and thought involves motor imagery. Motor imagery can alter the neuronal action in the primary sensorimotor areas in a comparable fashion to that observed with an actual performed movement; thus, 1 should be able to effect motor performance by cognitive imagery and cognitive performance by motor and movement exercise. Motor control and the attendant motor–cognitive processes can be readily evaluated through the use of motor imagery. 42 Repeated motor learning will inevitably promote the improvement of subjects’ cognitive function.
The design of the intervention for the TCE + RTG in this study integrated the traditional Chinese medicine (TCM) health concept, and acupoint massage was used throughout the intervention. According to the meridian theory of TCM, the meridians can pass qi and blood, connect with the organs of the gut organs. By stimulating the acupoints, the qi and blood of the meridians and the functions of the gut organs can be adjusted, the relative balance of yin and yang in the body can be restored, and the therapeutic purpose of promoting righteousness and exorcism can be achieved. 43 TCM research has proved that the stimulation of specific acupoints can help improve cognitive function in the elderly. 44 Traditional acupuncture at Baihui points is widely used to treat clinical diseases such as paralysis, dizziness, headache, poor memory, and stroke. In an animal experimental study, Claudia Di Giacomo et al found that laser acupuncture at Baihui points had a positive effect on hippocampal cognitive recovery, nerve cell loss, antioxidant enzyme activity, and IL-6 activity in an animal model of permanent ischemic stroke. Acupoint stimulation at Baihui ameliorates the low survival density caused by permanent occlusion of the right middle cerebral artery in the hippocampal CA1 and CA3 regions, which play an important role in information-processing nerve cells and associative memory. 45 The essence of this process is a learning process; following the TCM literature and expert advice, this study combined TCE movements and acupoint percussion, so that subjects could naturally perform acupoint percussion while practicing movements. In this way, the effect of acupoint massage and the intervention effect of TCE are superimposed, which is more beneficial to the cognitive function of the subjects.
The intervention provided to the TCE + RTG was a comprehensive exercise method with a musical background from the beginning to the end. At the beginning, the preparation activities were accompanied by stretching of the body joints and soft and cheerful music to guide the physical and psychological states of the subjects as they gradually entered the exercise. The rhythm of the background music of aerobic exercise is basically 100-104 BMP, and the change of the music rhythm can directly affect the adjustment of exercise intensity. After the training, the relaxation part involved listening to soothing music and relaxing the whole body under the instruction of the trainer, so that the body could transition from the exercise state to the quiet state faster, effectively relieving exercise fatigue and psychological anxiety. Depression and anxiety symptoms are common neuropsychiatric symptoms in patients with CI and risk factors for CI. 46 Therefore, relief of depressive symptoms helps to protect cognitive function and delay the decline of cognitive function. There is evidence that music induces physiological dopamine release, with substantial improvement in emotional responses. Improvement in physical function is further accentuated if exercise is accompanied by music. 47 There is an inverted U-shaped relationship between degree of syncopation in music and movement- and pleasure-ratings, indicating that intermediate degrees of syncopation elicit the most desire to move and pleasure in music associated with groove. 48 Music therapy appears to be the best treatment for MCI. 49 Many reports on the application of music therapy showed an improvement in memory, and our results are in line with these results. Hand–eye coordination guided by auditory stimuli improved the executive and visuospatial function as well as memory. The association between music and movement itself may be beneficial for cognitive functions, as reported by Vande Winckel, who showed that music-based exercise may improve general cognition and verbal fluency in dementia patients. 50 Hars et al. also found 6 months of once weekly music-based multitask training was associated with improved cognitive function and decreased anxiety in community-dwelling older adults, compared with non-exercising controls. 51 Other studies have reported consistently positive results after applying music activities to therapy designed to improve rigidity and motor ability (gait and balance), enhancing patient quality of life and emotional functions.52–54
In this study, compared with the CG, the participants in the WG showed significant improvement in MMSE and MoCA test results after 12 weeks of intervention, and a small improvement in the SDMT test results, suggesting that walking can effectively improve subjects’ cognitive function, but the effect on attention and working memory is not obvious. Walking plays a limited role in cognitive effects, mainly because the unique need to walk causes different areas of the brain to be active, and the dorsolateral cortex of the prefrontal lobe is not highly active during stable walking. 55 Previous studies have shown that insisting on long-term walking activities can improve cognitive function in older women. 56 Walking activities can effectively improve the memory and concentration of subjects. Another possible explanation for the possibility that bipedal walking can affect cognition is that the most important basis of human evolution is bipedal walking. In terms of development, children who achieve later developmental markers have a higher risk of CI, and human brain development is related to the development of bipedal movement. 42
The study also found that subjects in the WG had a significant improvement in ADL after 6 weeks, and there was a significant inter-group difference with the CG after 12 weeks, which was better than in the TCE + RTG. In the study, the walking intervention was conducted in a park, and subjects were required to walk, drive, or ride to and from the activity site. Compared with indoors, outdoor walking with a prolonged relaxation and meditative mental state increased vitality, decreased depression, anxiety, anger, depression, and regular exercise even increased well-being. The natural environment also contains less external stimuli and is beneficial for the performance of concentration. 57 It has beneficial effects on human health, and a greener environment is ideal for restoring attentional function. 58 During the intervention, walking, driving, riding, and finding a place to travel to and from the activity were not part of the intervention process, but were a necessary task to complete the walking activity. Therefore, walking activity also exercised participants’ ability to use transportation and tell location. In this study, there were significant differences between the pre- and post-test and the intermediate and post-test of HAMD-17 in the WG. Active social participation in the elderly can significantly improve their health and delay cognitive decline.46,59 Participation in a WG is also a good way for the elderly to socialize. For example, the team members gathered at the agreed time, chatted with each other during the walk, and reminded each other of the training time and precautions in the WeChat group, which also established a good social interaction environment for each walk.
After the 12-week intervention, the level of BDNF in the blood of subjects in the TCE + RTG and WG were significantly increased, but there was no significant difference between the groups, while the test results of the CG showed a decreasing trend. According to the change of each group before and after the intervention, there was a significant difference between the TCE + RTG and CG, and the increase of BDNF level in the blood of the TCE + RTG was more obvious after the intervention.
Animal experimental studies have shown that 6 weeks of aerobic exercise can up-regulate the expression level of BDNF during aging in the hippocampus of rats, which may be 1 of the neuromolecular mechanisms for the improvement of learning and memory ability in rats. 60 The results of this study showed that the TCE + RTG intervention 3 sessions a week for 12 weeks increased serum BDNF levels in the subjects. Compared with the CG, the magnitude of the increase in serum BDNF levels was significantly different in the TCE + RTG.
Ruschueyh et al found that after 6 months of aerobic exercise, the elderly showed an upward trend in quiescent BDNF levels. 61 Ferris et al noted that human BDNF levels increase significantly after exercise, and the magnitude of the increase is related to exercise intensity. At different exercise intensities, cognitive function scores improve, but do not always cause changes in BDNF. One-time acute aerobic exercise can temporarily increase peripheral blood BDNF concentrations. 62 Based on this, there was no significant increase in BDNF before and after the intervention in this study, which may be related to the lower exercise intensity.
The strengths of this controlled trial include the innovative design of clinical studies to elucidate the possibility of using a TCE + RTG to maximize cognitive benefits. The results of this trial can be generalized or applied to hospital clinics or regional dementia centers. The results of this experiment show that the effects of the TCE + RTG on cognitive function include direct and indirect parts. The direct effects include comprehensive training, such as action learning, acupoint recognition, calculation, positioning, memory, and attention training. The learning of new knowledge and new skills is essentially a comprehensive cognitive activity. Each subject needs to carry out cognitive activities such as feeling, perception, memory, imagination, and thinking during the learning process of the TCE + RTG, and the learning of motor skills and acupoint knowledge during the training process can exercise the subjects’ cognitive function. In addition, the integration of computing, positioning, attention and other training content into exercise targeted cognitive stimulation for the older adults with MCI, helping to improve their cognitive function. Indirect effects include traditional aerobic exercise, acupoint massage, listening to music, and social interaction. The social attributes of listening to music and group intervention reduced the anxiety and depressive symptoms of the subjects. While strengthening the body and protecting the health of the brain, aerobic exercise in older adults reduced the risk of CI and indirectly improved the cognitive function of the subjects. At the same time, exercise stimulated specific acupoints, regulated the subjects’ qi, blood, and viscera through the conduction of qi and the response of viscera, and can affect the physiological functions and pathological changes of multiple organs and systems at different levels. Practitioners of modern medicine hold the view that acupoint massage can improve the blood supply of the central nervous system, 63 increase the blood oxygen and nutrient supply of brain tissue, and improve certain immune abilities of the body through the regulation of nerve and body fluids, thereby improving brain function and improving the overall health of the body. 64
The present study had several limitations. The sample size was small and replication with a larger group with CI would be beneficial. The dose–response relationship between the TCE + RTG intervention and cognition is yet to be fully elucidated, which should be addressed in future studies.
Conclusions
In conclusion, this study suggests the 12-week TCE + RTG intervention significantly improved cognitive function in older adults with MCI. The intervention resulted in significant improvements in MMSE, MoCA, SDMT, ADL, and HAMD-17 scale results, as well as positive improvements in BDNF levels in the subjects’ blood. The TCE + RTG may be a promising and effective way to improve cognitive function in older adults with MCI. Further research is necessary to replicate these findings with a larger sample size and also to investigate TCE combined with other non-pharmacological interventions.
Footnotes
Acknowledgments
We gratefully acknowledge all the support given by the patients and the staff of Beijing Dongcheng district street community health center, the professionals who helped with tests, and the experts who provided guidance during the article revision process.
Author Contributions
Conceptualization, Q.Z., M.-L.Z., and P.Z.; methodology, Q.Z., M.Z., and L.-L.H.; formal analysis, Q.Z., L.-L.H., and P.Z.; data curation, Q.Z. and L.-L.H.; writing—original draft preparation, Q.Z., and P.Z; writing—review and editing, Q.Z., M.-L.Z., L.-L.H., M.Z., and T.M.; project administration, T.M.; funding acquisition, M.-L.Z. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Beijing Sport University (protocol code 2020062H and April 20th, 2020).
Informed Consent
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Clinical Trial Registration
The data underlying this article can be accessed on the Chinese Clinical Trial Registry website by the trial registration: ChiCTR2200058545. The link is as follow: https://www.chictr.org.cn/showproj.html?proj=165809.