
Abstract
Purpose:
To study the effect of undiagnosed diabetes on the relationship between self-reported diabetes and cognitive impairment.
Methods:
Data were from 1033 participants aged
Results:
Self-reported diabetes was associated with significantly higher odds for severe, but not moderate, cognitive impairment (odds ratio [OR] = 2.70, 95% confidence interval [CI] = 1.39-5.32). The association between self-reported diabetes and severe cognitive impairment decreased by 6.3% when undiagnosed diabetics were included in the nondiabetic category and by 30.4% when undiagnosed diabetics were included in the self-reported diabetes category.
Discussion:
The association between self-reported diabetes and severe cognitive impairment is underestimated when undiagnosed diabetics are not differentiated from self-reported diabetics and nondiabetics.
Introduction
Consistent evidence indicates type 2 diabetes is a risk factor for cognitive impairment among older adults. A Delphi Consensus study identified 19 studies that examined the relationship between diabetes and Alzheimer disease (AD), of which 17 reported a positive association between diabetes and AD. 1 Furthermore, a meta-analysis of 20 longitudinal studies reported that diabetes was associated with a 21% higher risk for mild cognitive impairment, 54% higher risk for AD, and 148% higher risk for vascular dementia. 2 Epidemiological research has focused largely on nonhispanic white older adults, but diabetes has also been identified as a risk factor for cognitive impairment among older Mexican adults. Older Mexican adults who reported being diagnosed with diabetes by a physician have been observed to have 2 times higher odds for dementia compared to nondiabetic older adults. 3 These findings are consistent with those reported by studies of older Mexican Americans. A study of 1617 nondemented Mexican Americans revealed that older adults with treated and untreated diabetes had 2 and 1.5 times higher risk, respectively, for cognitive impairment compared to nondiabetic older Mexican Americans. 4
While type 2 diabetes has been consistently associated with cognitive impairment among older adults, the impact that older adults with elevated blood glucose levels who have not been diagnosed with diabetes (ie, undiagnosed diabetics) may have on this relationship is not known. This is particularly important to study in older Mexican adults because prior research has relied primarily upon self-reported data to determine if a participant has diabetes. 3 A limitation of this approach is cases of undiagnosed diabetes are included in the nondiabetic reference group, which may underestimate the association between self-reported diabetes and cognition. This limitation is concerning, given the high prevalence of undiagnosed diabetes among older Mexican adults. 5,6 Thus, the purpose of this study is to examine the effect that undiagnosed diabetes has on the relationship between self-reported diabetes and severity of cognitive impairment among Mexican adults aged 60 and older. We hypothesize that undiagnosed diabetes will be associated with cognitive impairment and not excluding older adults with undiagnosed diabetes from those who are nondiabetic will result in an underestimation of the relationship between self-reported diabetes and cognitive impairment.
Methods
Data Source and Study Design
This study used a cross-sectional design and used data from a subset of the 2012 Wave of the Mexican Health and Aging Study (MHAS). The MHAS is an ongoing nationally representative longitudinal cohort study of Mexican adults aged 50 and older in 2001. 7 The MHAS was initiated in 2001 and follow-up observations were conducted in 2003 and 2012. A total of 18 465 individuals were interviewed during the 2012 Wave, of which 2086 participants underwent a capillary blood draw for measures of hemoglobin and glycosylated hemoglobin (HbA1c).
A visual representation for the selection of the final sample is presented in Figure 1. Participants who were selected to provide anthropometric or biomarker data; were aged 60 or older; had data for HbA1c concentration; and had data for demographic, health, and behavioral characteristics were included in the final sample. In order to maximize the final sample size, participants who had completed 2 or more cognitive assessments were included in the final sample. Of the 1041 participants who had data for sociodemographic, health, behavioral, and cognitive data, 8 participants who reported being diagnosed with diabetes during the 2003 observation but reported never being diagnosed with diabetes during the 2012 observation were excluded from the final sample (n = 1033). Participants who were excluded from the final sample were significantly older; were less likely to be married; were more likely to have had a stroke and to be depressed; and had lower scores for orientation, verbal learning, verbal memory, verbal fluency, and attention compared to participants included in the final sample (P < .05).
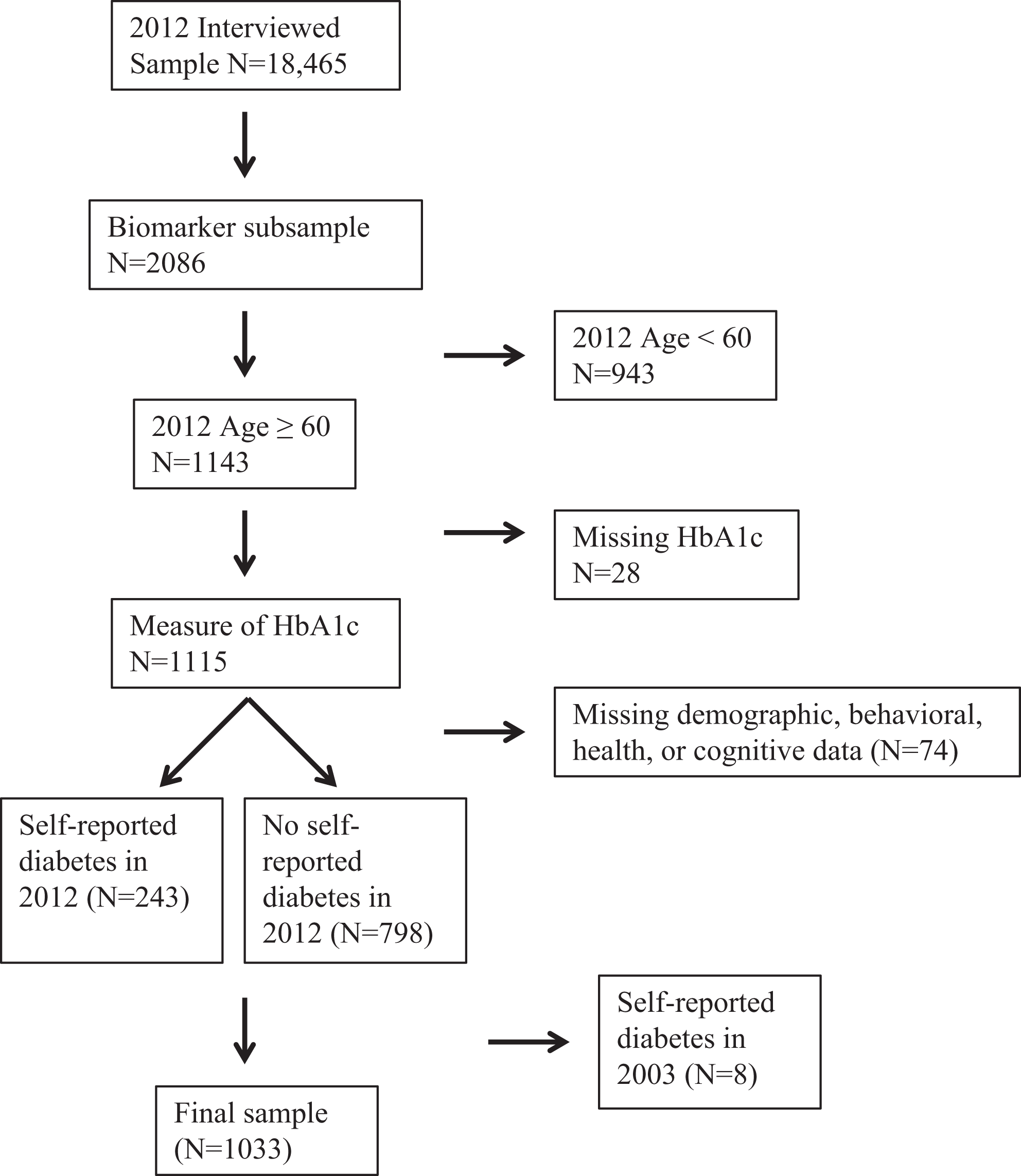
Selection of final sample from the Mexican Health and Aging Study.
Assessment of Diabetes Status
Participants who reported having been diagnosed with diabetes by a physician or a medical professional were classified as having self-reported diabetes. Undiagnosed diabetes was determined according to HbA1c concentration. HbA1c provides a reliable measure of circulating glucose in the blood over a 1- to 3-month period.
8
The American Diabetes Association defines diabetes, prediabetes, and normal according to the following HbA1c categories: (1) diabetes: HbA1c
Defining Moderate and Severe Cognitive Impairment
Cognitive functioning was measured using the Cross-Cultural Cognitive Examination (CCCE). 10 The CCCE includes eight cognitive tasks that each assess a different cognitive domain: (1) verbal memory immediate recall (verbal learning), (2) verbal memory delayed recall (verbal memory), (3) visuospatial (construction), (4) visual memory (visual recall), (5) visual scanning (attention), (6) date naming (orientation), (7) animal naming (verbal fluency), and (8) backward counting (working memory).
The criteria used to classify cognitive impairment were based on the diagnostic criteria for mild cognitive impairment and dementia proposed by the National Institute on Aging-Alzheimer’s Association workgroups.
11,12
Cognitive impairment was defined as performance on 1 or more cognitive assessments that was
Participants who were defined as cognitively impaired were further classified as moderate or severely impaired based on their ability to perform activities of daily living (ADLs; difficulty walking, bathing or showering, eating, getting out of bed, or using the toilet) and instrumental ADLs (IADLs; difficulty preparing a hot meal, shopping, taking medications, or managing money). Since Mexican culture contributes to gender differences in IADLs (eg, men do not typically shop for groceries or prepare a meal and women do not typically manage money), participants who had difficulty performing 1 or more ADLs and/or 2 or more IADLs were classified as being functionally impaired. 3 Participants who were not cognitively or functionally impaired were classified as having normal cognition. Participants who were cognitively impaired and had no functional impairment were classified as having moderate cognitive impairment. Participants who were cognitively and functionally impaired were classified as having severe cognitive impairment.
Covariates
Covariates were selected based on previous research on the relationship between cognition and diabetes. 4,13,14 Participants were asked to report their age, sex, years of education completed, and marital status (single, married, in a consensual union, divorced, separated from a union, separated from a marriage, widowed from a union, and widowed from a marriage). Education was recoded as 0 years, 1 to 6 years, and 7 or more years and marital status was recoded as married or in a consensual union, not married, and widowed.
Participants were also asked if they engaged in exercise or hard physical work 3 or more times a week and if they had ever experienced a heart attack, stroke, possible stroke, or transient ischemic attack. Depressive symptoms were assessed using 9 questions from the Center for Epidemiological Studies Depression Scale that asked if a participant felt depressed, if everything they did was effort, had restless sleep, felt happy, felt lonely, felt that they enjoyed life, felt sad, felt tired, and felt they had a lot of energy. Participants who had 6 or more symptoms were classified as having high depressive symptoms. 15 Alcohol consumption was defined according to 3 categories: (1) abstainer, (2) former drinker: has consumed alcohol in the past but is not currently drinking alcohol, and (3) current drinker: reported consuming alcohol in the past 3 months. Smoking status was defined as never, former, and current smoker. Body mass index (BMI) was calculated using measured values for height (in meters square) and weight (in kilograms).
Statistical Analysis
Analysis of variance and χ2 tests were used to assess the differences in demographic, behavioral, and health characteristics according to cognitive status. Separate logistic regression models for moderate and severe cognitive impairment were used to assess the association between diabetes and cognitive impairment. This is an appropriate approach when the proportional odds assumption, which is required for ordinal logistic regression, is not valid. 16 Three separate logistic regression models were constructed. Model 1 included 3 categories for diabetes: (1) nondiabetic (reference category), (2) undiagnosed diabetes, and (3) self-reported diabetes. Model 2 used self-report diabetes status as the primary independent variable. In this model, participants with undiagnosed diabetes were included in the same category as participants who did not have diabetes. Model 3 included participants with undiagnosed diabetes in the same category as participants with self-reported diabetes. All models were adjusted for the effects of age, gender, education, marital status, smoking, alcohol consumption, exercise, hypertension, heart attack, stroke, depression, and BMI.
The odds ratio (OR) obtained from model 1 and model 2 were used to calculate the percentage change in the association between self-report diabetes and severity of cognitive impairment when participants with undiagnosed diabetes are included in the same category as those who do not have diabetes. Percentage change was calculated using the following equation: (ORDM1 − ORDM2)/ORDM1, where ORDM1 is the OR of diabetes from model 1 and ORDM2 is the OR of diabetes from model 2. This calculation was also performed using the OR from model 1 and model 3 to calculate the percentage change when participants with undiagnosed diabetes are included in the same category as participants with self-reported diabetes.
Results
Characteristics of Final Sample
Table 1 presents a summary of the demographic, behavioral, and health characteristics of the final sample according to the severity of cognitive impairment. A total of 751 participants had normal cognition, 220 were moderately impaired, and 62 were severely impaired. Participants who were either moderately or severely impaired were older, had lower educational attainment, were more likely to be depressed, had lower BMI, and were less likely to engage in physical exercise compared to participants who were not cognitively impaired (all Ps < .05). Also, participants with self-reported diabetes were more likely to have severe cognitive impairment compared to participants who were nondiabetic (P < .05).
Descriptive Characteristics of 1033 Participants Included in Final Sample According to Severity of Cognitive Impairment.
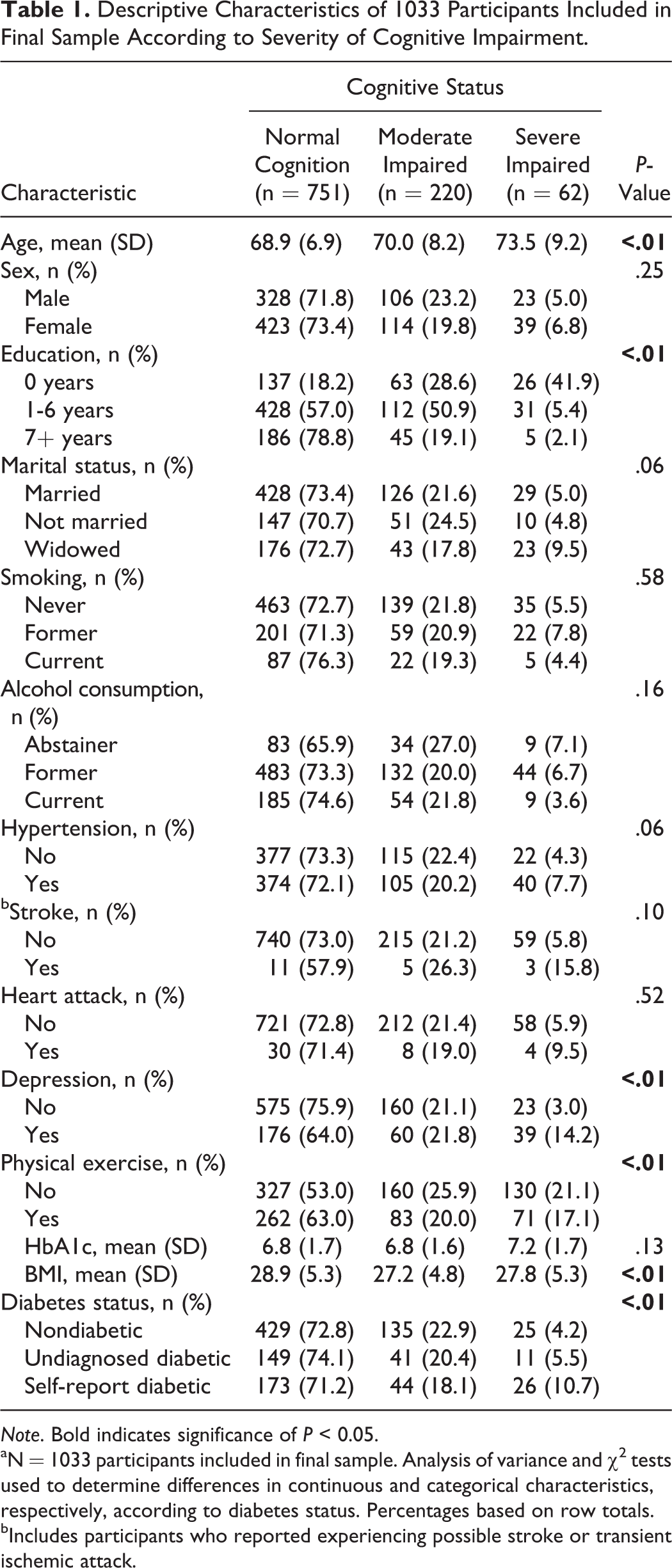
Note. Bold indicates significance of P < 0.05.
aN = 1033 participants included in final sample. Analysis of variance and χ2 tests used to determine differences in continuous and categorical characteristics, respectively, according to diabetes status. Percentages based on row totals.
bIncludes participants who reported experiencing possible stroke or transient ischemic attack.
Of the 1033 participants included in the final sample, 243 reported being diagnosed with diabetes, 201 were classified as undiagnosed diabetes, and 589 were classified as nondiabetic. Participants with self-reported diabetes were younger, were less likely to exercise, and were more likely to report having been diagnosed with hypertension or a heart attack, to be a former alcohol consumer, and had lower BMI compared to participants with undiagnosed diabetes or nondiabetics (all Ps < .05). Also, participants with self-reported diabetes had higher HbA1c concentration compared to nondiabetics (P < .05) and undiagnosed diabetes (P < .05).
Diabetes Status and Cognitive Impairment
A summary of the results for the association between diabetes and severity of cognitive impairment is provided in Table 2. Significant differences in the odds for severe but not moderate cognitive impairment according to diabetes status were detected in all 3 of the models. In model 1, participants with self-reported diabetes had 2.70 (95% confidence interval [CI] = 1.39-5.32) times higher odds for severe cognitive impairment compared to nondiabetics, whereas participants with undiagnosed diabetes did not have significantly higher odds for severe cognitive impairment compared to nondiabetics (OR = 1.24, 95% CI = 0.53-2.76). The association between self-reported diabetes and severe cognitive impairment decreased when participants with undiagnosed diabetes were included in the nondiabetic category (model 2). Compared to nondiabetics, participants with self-reported diabetes had 2.53 times higher odds (95% CI = 1.37-4.66) when participants with undiagnosed diabetes were included in the nondiabetic category. When participants with undiagnosed or self-reported diabetes were included in the same category (model 3), diabetic participants had 1.88 times higher odds (95% CI = 1.04-3.46) for severe cognitive impairment compared to nondiabetics.
Odds Ratios for Moderate and Severe Cognitive Impairment According to Diabetes Status.a
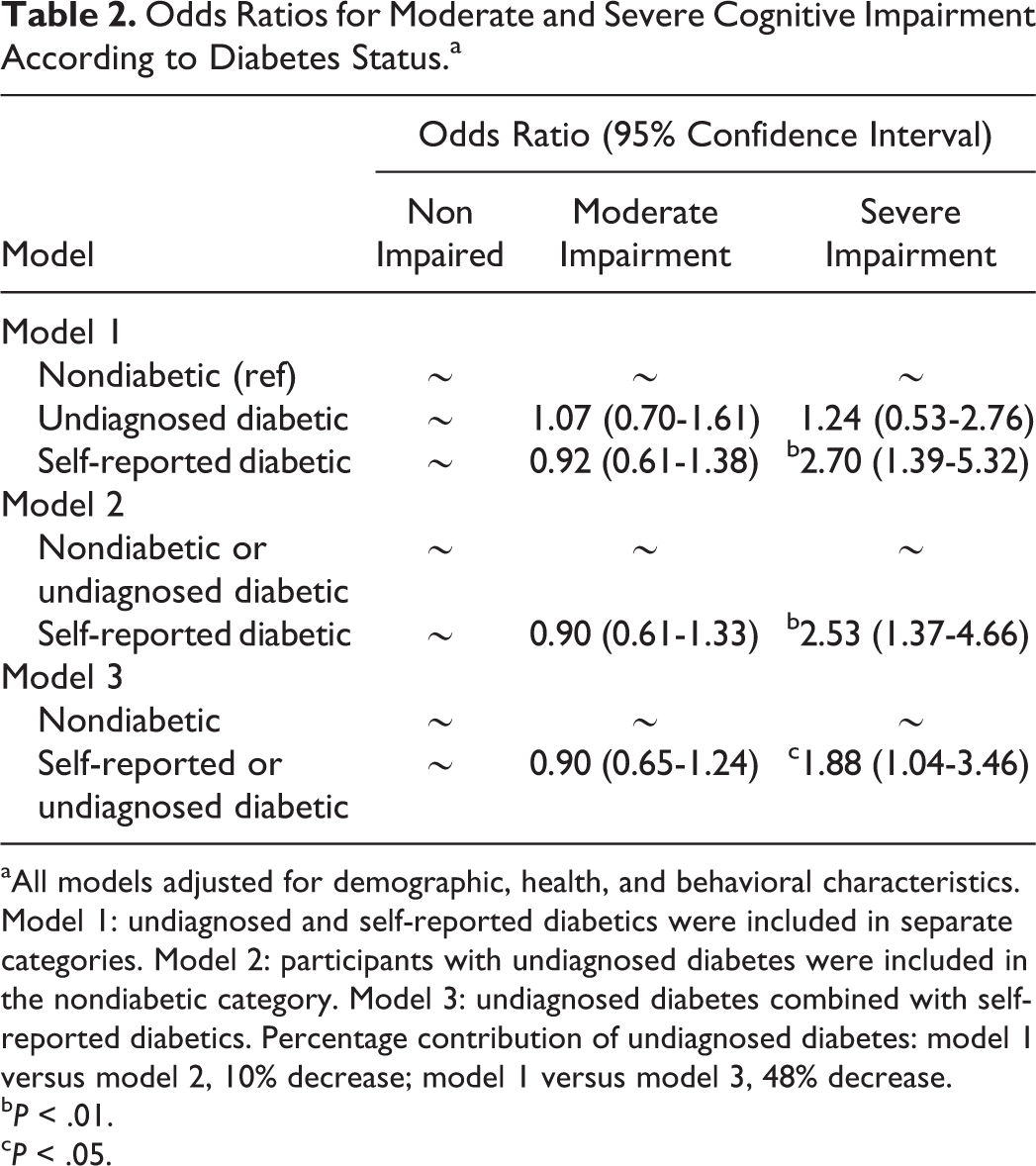
aAll models adjusted for demographic, health, and behavioral characteristics. Model 1: undiagnosed and self-reported diabetics were included in separate categories. Model 2: participants with undiagnosed diabetes were included in the nondiabetic category. Model 3: undiagnosed diabetes combined with self-reported diabetics. Percentage contribution of undiagnosed diabetes: model 1 versus model 2, 10% decrease; model 1 versus model 3, 48% decrease.
b P < .01.
c P < .05.
Using the OR from model 1 and model 2 indicate that including cases of undiagnosed diabetes in the nondiabetic category contributed to a 6.3% decrease ([2.53-2.70]/2.70) in the association between self-reported diabetes and severe cognitive impairment. The OR from model 1 and model 3 indicate that including participants with undiagnosed diabetes in the same category as those with self-reported diabetes contributed to a 30.4% decrease ([1.88-2.70]/2.70) in the association between diabetes and severe cognitive impairment.
Discussion
This study presents evidence that not separating participants with undiagnosed diabetes from participants with self-reported diabetes or who do not have diabetes underestimates the association between self-reported diabetes and severe cognitive impairment. Self-reported diabetes was associated with 2.70 times higher odds for severe cognitive impairment when cases of undiagnosed diabetes were excluded from the nondiabetic category (model 1). This association decreased but remained statistically significant when participants with undiagnosed diabetes were included in the same category as participants who did not have diabetes (model 2) or had self-reported diabetes (model 3). The 2.70 times higher odds for severe cognitive impairment among older adults with self-reported diabetes is higher compared to other studies that did not account for undiagnosed diabetes. 3,17 -19 While differences in sample population characteristics and study design make it difficult to directly compare our findings to those from prior studies, previous studies that used self-reported data for diabetes status may have underestimated the association between self-reported diabetes and cognitive impairment.
Contrary to previous research, 20,21 we did not observe that undiagnosed diabetes was associated with moderate or severe cognitive impairment. Our inability to detect a statistically significant association may be due to a small sample size. It should also be noted the association between diabetes and severe cognitive impairment decreased by 30.4% when undiagnosed diabetics were combined with self-reported diabetics (model 3). This may be due to older adults with undiagnosed diabetes having lower disease severity than participants who had received a diagnosis of diabetes by a physician. This is supported by the significantly lower HbA1c concentration for participants with undiagnosed diabetes compared to participants with self-reported diabetes. Also, it may be necessary for a person to be exposed to diabetes for a certain period of time before negative effects on cognition can be observed. Participants with undiagnosed diabetes likely have shorter exposure to diabetes compared to participants who reported being diagnosed with diabetes and may not have been exposed to diabetes for a sufficient amount of time for the disease to negatively impact cognition. However, peripheral hyperinsulinemia has been associated with reduced levels of insulin in the brain, which may contribute to altered brain functioning and lead to cognitive impairment. 22
The findings from the present study have important implications. Type 2 diabetes is an important risk factor for dementia, and reducing the prevalence of type 2 diabetes may be an effective strategy in preventing older adults from developing dementia. Previous research indicates a 10% reduction in the global prevalence of type 2 diabetes could potentially prevent approximately 81 000 AD cases and a 25% reduction would prevent approximately 203 000 cases. 23 However, these calculations may underestimate the number of AD cases that can be prevented based on our finding that including cases of undiagnosed diabetes in the nondiabetic or self-reported diabetes categories underestimate the relationship between diabetes and severe cognitive impairment.
This study was able to use self-reported and biomarker data to determine diabetes status and identify undiagnosed cases of diabetes, but important limitations need to be acknowledged. First, this study used a cross-sectional design because data for HbA1c concentration were collected only during the 2012 Wave. A cross-sectional study design cannot account for the relationship between diabetes and mortality.
24
Not accounting for the competing risk of mortality has been found to result in an underestimation of the relationship between diabetes and cognition.
25
Second, HbA1c concentration is the only test of blood glucose included in the MHAS. The American Diabetes Association recommends that a positive test for diabetes be confirmed by repeating the same test.
9
An HbA1c concentration
In summary, this study presents evidence that the relationship between self-reported diabetes and severe cognitive impairment is underestimated when older adults with undiagnosed diabetes are not differentiated from those with self-reported diabetes or who do not have diabetes. These findings indicate that future studies need to account for undiagnosed diabetes when examining the association between diabetes and cognition. Given the importance of diabetes and cognitive impairment to public health, these findings need to be replicated using data from other sample populations.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the US National Institutes of Health National Institute on Aging [5T32 AG000270-17 to BD, RW; 2P2C HD065702-06; 5R01 AG018016-10 to RW; and P30 AG024832-11 to SAS].