
Abstract
Background
The role of diastolic blood pressure (DBP) with cognitive functioning is under-explored in relation to levels of systolic blood pressure (SBP).
Methods
We studied 5466 participants from the National Health and Nutrition Examination Survey. Blood pressure was measured 3 times manually with a standardized sphygmomanometer and averaged. Cognitive functioning was measured using the digit symbol substitution test (DSST).
Results
Participants were 60 years or older, 55% female, and 81% non-Hispanic White. Most participants had a DBP between 70 to <80 mmHg (33.7%), between 60 to <70 mmHg (29.3%), or <60 mmHg (18.8%). From multivariable linear regression analyses, each 5 mmHg increment of DBP was associated with significantly higher DSST scores among individuals with SBP <120 only (ß: 0.56, 95% CI: 0.09, 1.03).
Conclusions
Among older US adults, at non-elevated levels of SBP, higher DBP is associated with better cognitive performance.
Introduction
Elevated blood pressure (BP) or hypertension is a major risk factor for brain pathologies including stroke
While such studies find a clear relationship between elevated SBP and adverse brain health, the relationship between diastolic BP (DBP) and cognition is not as defined, with mixed findings.7,8 For example, in the Reasons for Geographic and Racial Differences in Stroke (REGARDS) cohort, higher DBP is associated with increased odds of cognitive impairment. 7 On the other hand, higher DBP, particularly in older age 9 has also been shown to be associated with better cognitive outcomes. 8 It has been posited that such mixed findings can be attributed in part to differential associations by age and possibly sex. For example, higher DBP has been shown to be negatively associated with cognition during mid-life,10,11 but positively associated with cognition in the later decades of life. 12 Indeed, findings from the Atherosclerosis Risk in Communities (ARIC) Study 12 have showed that lower DBP from mid to late life are associated with cognitive decline later in life. Further, results from the Norwegian Tromsø study showed that the relationship between DBP and cognition differs by sex, with higher DBP associated with lower cognitive function in men aged 45-55 years, but greater cognitive functioning among men aged 65-74 and with no associations among women. 11
Most studies have focused on either SBP or DBP as distinct exposures. Seldom is the relationship between SBP and cognition contextualized according to DBP (or vice versa). Though pulse pressure (PP), or the difference between SBP and DBP, is inversely related to cognitive functioning,13,14 it does not account for clinically relevant thresholds of SBP and DBP. 15 Thus, we sought to address this knowledge gap. Specifically, the objectives of the current study are to: (1) determine whether the association between SBP and cognition remains constant across all levels of DBP, (2) determine whether the association between DBP and cognition remains constant across all levels of SBP, and (3) determine whether these associations are modified by age or sex. To do so we leveraged data from the National Health and Nutrition Examination Survey (NHANES).
Methods
Study Sample
NHANES is a nationally representative, cross-sectional survey designed to evaluate the health and nutritional status of adults and children within the United States (US). 16 This survey has operated on a continual basis since 1999, collecting data from household interviews and through physical examinations. The current analysis includes data from NHANES survey cycles (1999-2002 and 2011-2014) which consisted of a cognitive assessment in 5480 adults aged 60 or older. The National Center for Health Statistics approved all protocols and received informed consent from all participants prior to commencement.
Blood Pressure
BP was measured during the physical examination. After a five-minute rest period, using standardized sphygmomanometers, trained study staff obtained 3 to 4 BP measurements from each participant’s upper right arm while seated in an upright position. Cuff sizes were appropriately selected based on the arm circumference. The first 3 BP measurements were averaged. SBP was defined both continuously and categorized according to clinically relevant thresholds: <120 mmHg, 120 to 129 mmHg, 130 to 139 mmHg, 140 to 159 mmHg, and ≥160 mmHg. Similarly, DBP was also treated both as a continuous variable and categorized according to the following clinically relevant thresholds: <60, 60 to 69, 70 to 79, 80 to 89, and ≥90 mmHg. 17
Cognitive Functioning
Cognitive functioning was measured using the Digit Symbol Substitution Test (DSST), a measure of executive functioning and processing speed. 18 In this timed paper and pencil test, participants were tasked with correctly assigning symbols to their corresponding numbers based on a key that was provided. Scoring for DSST allows 1 point per correctly matched pair in the allotted time, with higher scores indicative of better cognitive function (range 0-133). 19
Other Variables
Demographic information was collected during the NHANES interview portion of the survey. Age, sex, race/ethnicity, marital status, health insurance status, education level (less than high school, high school graduate, some college, college graduate), and annual income range (less than $55,000, more than $55,000) were self-reported. Individuals also self-reported information regarding health behaviors such as alcohol consumption (number of days alcohol consumed in 1 month), overall health status (poor, fair, good, very good, excellent), level of physical activity (time spent in a given day and week, intensity of activity, type of activity), current smoking status, use of BP medication, self-reported diabetes diagnosis, and use of diabetic medication. 20 Total cholesterol (mg/dL) and plasma glucose (mg/dL) was measured from a fasting blood draw following standard procedures. 21 Consistent with guidelines in place at the time of data collection, hypertension was defined by the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure as: self-reported use of BP medication, average measured SBP ≥ 140 mmHg, or average measured DBP ≥ 90 mmHg. 22 Diabetes status was defined as meeting any of the following criteria: self-reported diabetes, diabetes medication use, or fasting plasma glucose levels ≥126 mg/dL. 23 Body mass index (BMI) was calculated from measured weight/measured height (kg/m2). Using BMI, individuals were categorized as: obese (BMI ≥30 kg/m2), overweight (BMI 25 to 29.9 kg/m2), normal weight (BMI 18.5 to 24.9 kg/m2), or underweight (BMI <18.5 kg/m2). 24
Statistical Analysis
We described demographic, clinical, and behavioral characteristics of the study population overall and according to categories of SBP. Then, we determined whether characteristics differed according to SBP category using means for continuous variables or chi-square tests for proportions. We also graphed the distribution of DBP category overall and according to category of SBP. To determine whether BP was associated with cognitive functioning, we used linear regression models. We tested the interaction between DBP and SBP categories and also between SBP and DBP categories with cognition. Interactions were significant (P < .05), leading to stratified models. We used a series of 4 linear regression models for each predictor of interest (DBP; modeling 5-unit increments and SBP; modeling 10mmHg increments) with DSST score. Model 1 was adjusted for sociodemographic characteristics (age, sex, and race). Model 2 included model 1 adjustments in addition to socio-economic factors (education, income, marital and insurance status). Model 3 included model 2 adjustments in addition to behavioral factors (alcohol use, health status, smoking status, and physical activity level). Model 4 included all model 3 adjustments in addition to clinical factors (BMI, diabetes, BP medication use, and total cholesterol). We also tested the three-way interaction of SBP and DBP with either sex, race, or education but, P values were all >.05. Finally, in a sensitivity analysis we repeated our main models among individuals with at least a high school education. All analyses were conducted using SUDAAN V11.0.3, utilized survey weights, and accounted for the complex survey design of NHANES.
Results
Characteristics of the Study Sample overall and according to Systolic Blood Pressure.
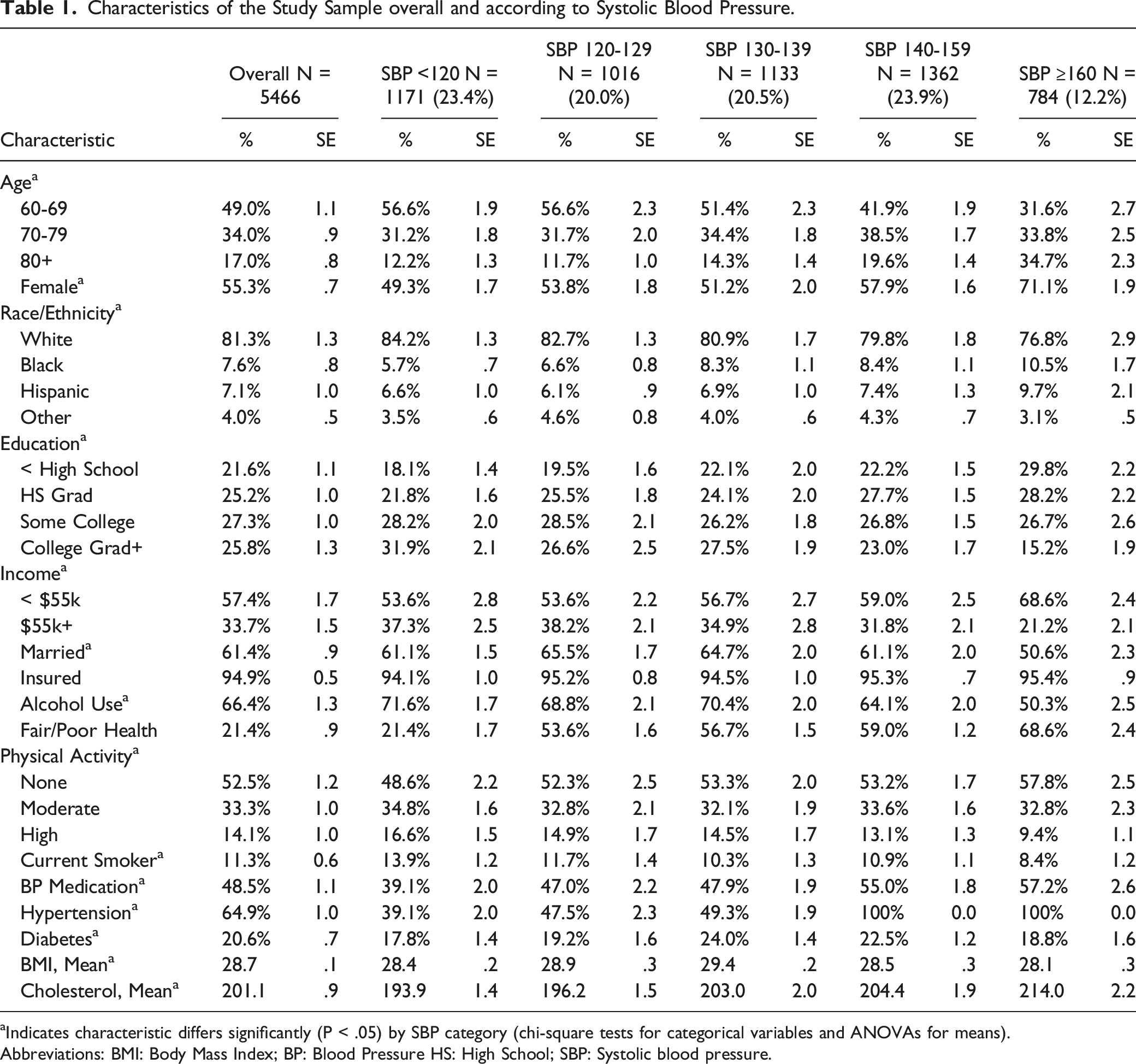
aIndicates characteristic differs significantly (P < .05) by SBP category (chi-square tests for categorical variables and ANOVAs for means).
Abbreviations: BMI: Body Mass Index; BP: Blood Pressure HS: High School; SBP: Systolic blood pressure.
The distribution of DBP category overall and according to categories of SBP are presented in Figure 1. Overall, 18.8% had DBP <60 mmHg (95% CI: 17.2% - 20.6%), 29.3% had DBP between 60-70 mmHg (95% CI: 27.7% - 31.1%), 33.7% had DBP between 70-79 mmHg (95% CI: 31.8% - 35.6%), 13.8% had DBP between 80-89 mmHg (95% CI: 12.6% - 15.2%), and 4.3% had DBP ≥90 mmHg (95% CI: 3.4% - 5.3%). The distribution of DBP differed according to SBP category (p for interaction <.05). For example, among individuals with SBP <120 mmHg, 30.6% (95% CI: 26.6% - 35.0%) had DBP <60 mmHg and 0% had DBP ≥90 mmHg. In contrast, among individuals with SBP >160 mmHg, 14.1% (95% CI: 11.1% - 17.8%) had DBP <60 mmHg and 18.1% (95% CI: 13.6% - 23.6%) had DBP ≥90 mmHg. Distribution of DBP among US adults age 60 and older, stratified by SBP. Abbreviations DBP: Diastolic blood pressure; SBP: Systolic blood pressure there are no individuals SBP <120 mmHg and DBP ≥90 mmHg.
Associations Between Diastolic Blood Pressure (DBP) and Digit Symbol Substitution Test (DSST), Overall and According to Categories Of Systolic Blood Pressure (SBP).

aIndicates estimate is significant (P < .05).
Model 1 is adjusted for age, sex, and race/ethnicity. Model 2 is adjusted for model 1 covariates in addition to: education, income, marital status, and health insurance. Model 3 is adjusted for model 2 covariates in addition to: alcohol use, smoking, physical activity, and self-rated general health. Model 4 is adjusted for model 3 covariates in addition to blood pressure medication, body mass index, diabetes, and total cholesterol.
Figure 2 displays the associations between SBP and cognitive functioning stratified by categories of DBP. In fully adjusted models, every 10 mmHg increment in SBP was associated with lower DSST by: −.88 units (95% CI: −1.31, −.45) among participants with DBP 60-<70 mmHg, −.57 units (95% CI: −.93, −.21) among participants with DBP 70-<80 mmHg, and −.98 units (95% CI: −1.80, −.17) among participants with DBP 80-<90 mmHg. Results were not significant among individuals with DBP <60 mmHg (ß: −.45, 95% CI: −.91, .02) or DBP >90 mmHg (ß: −.67, 95% CI: −1.78, .44). Results from the sensitivity analysis restricted to individuals with at least a high school education (not shown) were consistent showing every 10 mmHg increment in SBP was associated with lower DSST score by: −1.01 (95% CI: −1.57, −.46) at DBP 60-<70 mmHg, −.59 (95% CI: −1.08, −.09) at DBP 70- <79 mmHg, and −1.04 (95% CI: −2.05, −.03) at DBP 70-<80 mmHg. Association between SBP and DSST, overall and according to categories of DBP. Abbreviations DBP: Diastolic blood pressure; DSST: Digit Symbol Substitution Test; SBP: Systolic blood pressure. *Indicates estimate is significant (P < .05) Models are adjusted for age, sex, race/ethnicity, education, income, marital status, health insurance, alcohol use, smoking, physical activity, self-rated general health, blood pressure medication, body mass index, diabetes, and total cholesterol.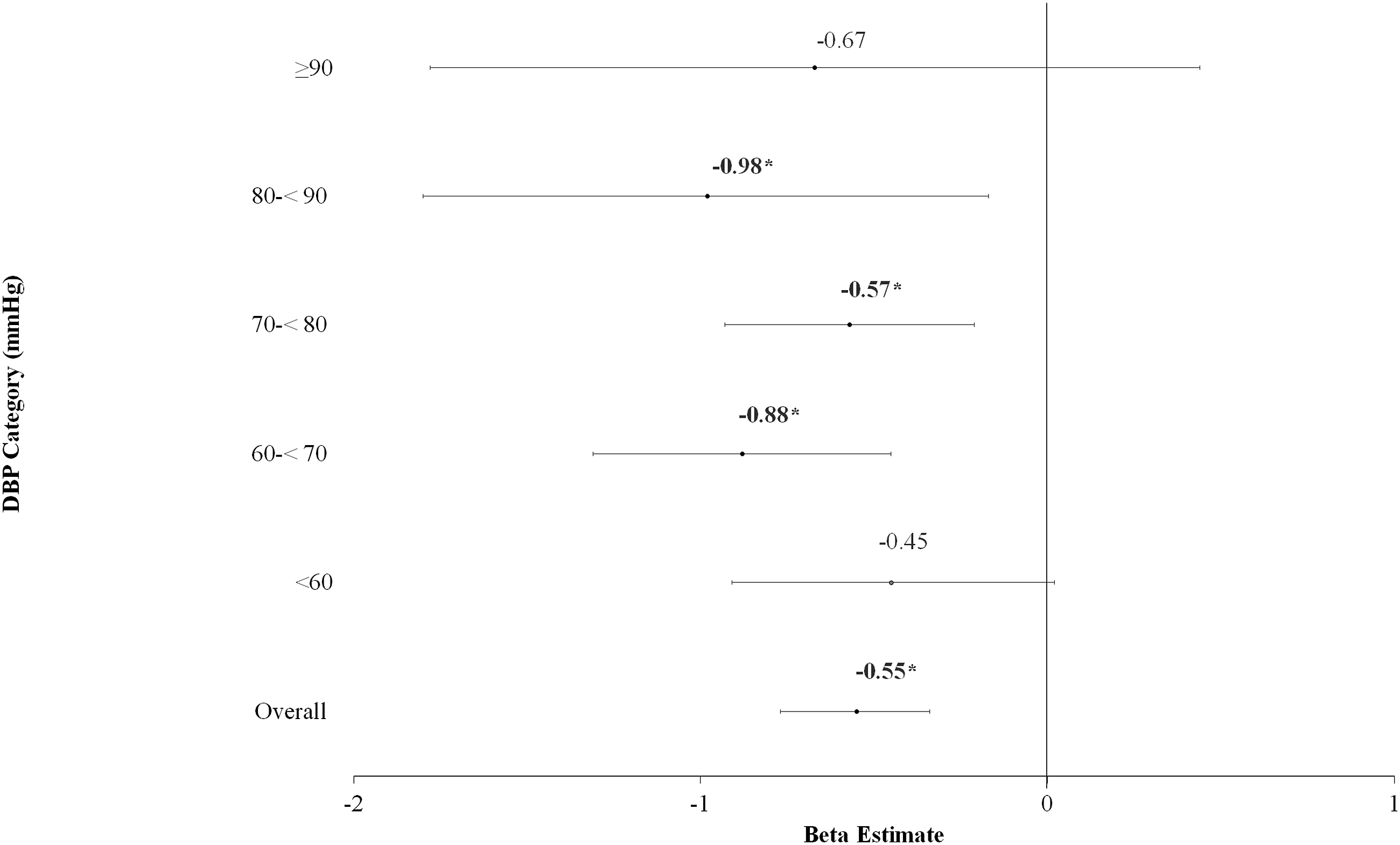
Discussion
In a population-based study representative of non-institutionalized US adults aged 60 and older, higher DBP was associated with better executive functioning at non-elevated levels of SBP (<120 mmHg). At elevated SBP, there was no association between DBP and cognitive functioning. On the other hand, higher SBP at any level of DBP was associated with lower executive functioning. These results highlight the importance of healthy SBP for brain health and emphasize the need for contextualization of SBP in consideration of DBP as a risk factor for cognitive functioning.
In US cohorts, the relationship between DBP and cognitive functioning has been mixed. Findings from the Coronary Artery Risk Development in Young Adults (CARDIA) study showed that higher cumulative DBP in young adulthood to mid-life are associated with lower cognitive performance in midlife. 25 Among participants of the Multi-Ethnic Study of Atherosclerosis (MESA) aged 45-84, higher baseline DBP was associated with lower scores on multiple domains of cognitive functioning. 26 Likewise, among diverse US Hispanics/Latino participants of the Hispanic Community Health Study/Study of Latinos (HCHS/SOL), aged 45-74, each 10 mmHg increment of DBP was associated with .04 standard deviation lower executive functioning. 14 These findings showing an inverse association between DBP and cognition have also been corroborated in international cohorts. In a prospective cohort of 12,281 older adults (median age 81) in China, every 10 mmHg increment of DBP was associated with a 6% increased risk of cognitive impairment measured from the Mini Mental State Exam. 27 In contrast, other research,12,13 including the current study, has shown positive associations between DBP and executive functioning. This is particularly true among older cohorts. 28 In the ARIC Neurocognitive study, lower (<68 mmHg) vs higher (>76 mmHg) DBP from mid-life to later life was associated with cognitive decline later in life. 12 Similarly, findings from the US Health and Retirement Study (HRS) and U.K. English Longitudinal Study of Ageing (ELSA), also showed that among adults aged 50 and over, higher cumulative DBP exposure is associated with decelerated cognitive decline. 13
Though age at BP assessment (mid-life or late-life) may certainly account for the discrepant findings, we posit that other factors may be contributing to the mixed results. In our study we found a significant interaction between DBP and SBP with cognitive functioning. DBP was associated with better cognitive functioning only at non-elevated levels of SBP. These results may indicate that greater DBP protects against cerebral hypoperfusion 29 resulting in better cognitive performance. Had we considered only main effects (overall models), our associations would have been null. Our findings support the need for a more nuanced and thorough approach when examining DBP in relation to cognition. Indeed, most studies showing relationships between higher DBP and better cognitive performance are specific to sub-populations (i.e. older adults). 28 Yet, there is limited research which examines DBP in the context of SBP (or vice versa). While pulse pressure (PP), or the difference between SBP and DBP, is inversely associated with cognitive functioning, 30 it does not account for clinically relevant BP thresholds. A PP that is less than 25% SBP is considered to be narrowed and a PP that is greater than 100 mmHg is considered to be widened. 31 Thus, the current study may help to contextualize many of the findings with respect to PP: higher DBP at non-elevated SBP (consistent with low PP) is associated with better cognitive performance. High SBP and low DBP, indicative of high PP, can be mechanistically attributed to impaired cognitive functioning for various reasons. Aging is associated with a number of vascular changes. 32 As a result of enduring pulsation with arterial blood, the vasculature, particularly that of the large vessels including the aorta, undergo calcification, endothelial dysfunction, luminal enlargement, and thickening of the vessel wall. 33 These changes are characteristic of arterial stiffness and result in greater pulse wave velocity, higher SBP, and consequently, greater PP. 32 In addition to aging, another well-known determinant of arterial stiffness is longstanding hypertension. 34 Arterial stiffness and resultant lowered arterial compliance plays a pivotal role in the lowering of DBP after age 60, 35 further leading to greater PP. Persistently high PP of this nature would impair cerebral blood flow and thereby cognitive functioning, as seen in numerous studies.13,14,36 In turn, arterial stiffness has emerged as a recognized independent risk factor for cognitive decline, 37 dementia, 38 and stroke. 39
Though the main focus of our study was on DBP, consistent with the literature, we also found SBP inversely associated with cognitive functioning. For example, data from ARIC, 12 CARDIA, 25 MESA, 26 the Northern Manhattan Study (NOMAS), 40 and HCHS/SOL 14 consistently show high SBP associated with lower cognitive functioning and cognitive decline. These findings are even supported by randomized controlled trial data. In the SPRINT-Memory and Cognition in Decreased Hypertension (MIND) study, intensive SBP control (to a goal of <120 mmHg) was associated with decreased cognitive impairment compared to those treated to a standard goal of <140 mmHg. 6 Our findings, though cross-sectional, corroborate these results, and show clear inverse associations between SBP and cognitive functioning at all levels of DBP.
The current study is not without limitations. First, our data are cross-sectional, limiting any causal inference. Further, our study utilized only one measure of cognitive function (DSST to measure executive functioning/processing speed). 18 Though we acknowledge that analysis of different cognitive domains may be warranted, we emphasize that the DSST has been shown to serve as a marker for cognitive ability in learning associations and to be predictive of future clinical as well as subclinical disorders of cognition.18,19 In addition, while the study sample size was large, we were underpowered to detect a 3 way interaction between SBP, DBP, with sex, education, or age. Given prior literature demonstrating the importance of both age and education as potential moderating factors, 41 we believe this is an important next step. Finally, given the design of our study, we could not adequately account for sub-clinical neuro-degenerative diseases which influence cognitive capabilities. Likewise, though DSST is a measure of executive functioning, 18 it can be sensitive to other impairments (e.g. non-essential tremors and arthritis). Therefore, it is important to consider that lower DSST results may be due to non-cognitive related deficits. Despite these limitations, our study has notable strengths. First, our study population is representative of US adults as a whole and includes diverse racial/ethnic groups. Standardized measures were utilized to obtain BP and cognitive functioning. While the role of hypertension in general and isolated systolic hypertension on cognition is clear, the relationship between DBP and cognition warrants more attention. This study employed a novel approach in elucidating the relationship between BP and cognition, focusing on the interaction between DBP and SBP. Our findings can help guide future research in this area and have implications for the clinical management of hypertension. Specifically, the efficacy of lowering DBP among older adults with isolated diastolic hypertension remains unknown as observational and clinical studies have reported mixed results. 42 Our findings suggest that isolated diastolic hypertension in older adults may not be associated with adverse cognitive outcomes.
In summary, in a representative study of older US adults, higher DBP was associated with better cognitive performance at non-elevated levels of SBP only. Higher SBP, at any level of DBP, was associated with worse cognitive performance. These findings emphasize that blood pressure is a potent vascular risk factor associated with cognitive functioning. To fully elucidate associations between BP with cognition, both SBP and DBP need to be considered in proper context in relation to one another. Further studies are warranted to corroborate these findings using longitudinal data.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Elfassy is supported by NIH/NIMHD (K01MD014158).