
Abstract
Introduction
The objective of this study was to examine the relationship between dementia severity and early discharge from home health.
Methods
This was a retrospective study of 100% national Medicare home health da ta files (2016-2017). Multilevel logistic regression was used to study the relationship of dementia severity, caregiver support, and medication assistance with early discharge from home health.
Results
The final cohort consisted of 91 302 Medicare beneficiaries with an ADRD diagnosis. A pattern of early discharge rates across dementia severity levels was not demonstrated. The relative risk for early discharge was lower for individuals who needed assistance with medication and for those with unmet caregiver needs.
Discussion
The findings of this study do not support the hypothesis that dementia severity contributes to early discharge from home health. Further research is needed to fully understand key factors contributing to early discharge from home health.
Significance Statement
• There was not a pattern of early discharge rates across Alzheimer’s Disease and Related Dementia (ADRD) levels. • People with ADRD who had unmet caregiver needs had lower risks of early discharge from home health. • People with ADRD requiring assistance with medication had lower risks of early discharge from home health.
Introduction
Most older adults prefer to receive health care services at home 1 and a growing body of evidence suggests that home health care is more cost efficient than institutional care for both patients and the health care system.2-4 Home health care offers a unique opportunity to directly assess a patient’s home environment, socioeconomic status, and need for caregiver or community support while providing rehabilitation services (physical, occupational, and speech therapy). In 2020, a total of 3.3 million Medicare fee-for-service beneficiaries received home health care 5 and nearly one-third of these individuals had a diagnosis of Alzheimer’s Disease or a related dementia (ADRD). 6 Familiar environments and routines have been shown to decrease neuropsychiatric symptoms (NPS) and improve health outcomes for people with ADRD.7-9
Prior to the implementation of the Patient Driven Groupings Model in January 2020, 10 it was required that the combined number of visits planned for physical therapy, occupational therapy, and speech-language pathology for the upcoming 60-day period be documented at the start or resumptions of care. Each discipline determines the reasonable and necessary number of visits based on a review of referral notes and orders, the plan of care, the patient’s medical history and current status, and any other relevant information. 11 Early discharge occurs when a patient is discharged from home health before the patient has received the prescribed number of rehabilitation sessions. An early discharge may occur if the home health team determines that the patient has met their goals quicker than expected or that the patient is no longer benefiting from therapy services. It is important to patients and their caregivers that the patient has sufficient independence in self-care tasks, that comorbid conditions are being properly managed, and that the caregiver has access to resources and support before the patient is discharged from home health. 12
Older adults with ADRD have been shown to be more vulnerable to early discharge from home health than their peers without ADRD. 13 Health care providers often doubt the rehab potential of people with ADRD and incorrectly think that these individuals will not benefit from rehabilitation services.14-17 Recent studies have established the efficacy of home health and rehabilitation services in meeting the health care needs of people with ADRD.18-22 However, clinicians often report feeling ill-prepared to work with individuals who have ADRD, especially in the later stages of the disease.14,15,23,24 Clinicians report that neuropsychiatric symptoms experienced by people with ADRD can be difficulty to manage and disruptive to rehabilitation sessions. 14 Thus, clinicians may underestimate the rehabilitation potential of patients with ADRD and terminate services early. 15
Early discharge from rehabilitation services may result in negative patient outcomes such as failure to achieve maximal functional gains, readmissions, or adverse events that endanger the patients’ health and quality of life. 25 Conversely, longer home health episodes of care and more visits has been associated with lower odds for rehospitalization. 26 The relationship between early discharge and ADRD severity has not been described. The primary objective of this study was to examine the association between dementia severity and risk of early discharge from home health care. We hypothesized that rates of early discharge would increase as dementia severity increases.
Materials and Methods
Data Sources
Data were derived from 4 administrative and clinical assessment data files obtained from the Centers for Medicare and Medicaid Services that contained 100% cohorts of beneficiaries receiving home health services between October 1, 2016, and September 30, 2017: (1) Home Health Base file, (2) Outcome and Assessment Information Set (OASIS), (3) Medicare Provider Analysis and Review, and (4) Beneficiary Summary file. The Home Health Base file was used to identify the cohort and to confirm the start and end of care dates. Data from the OASIS file was used in the development of a dementia severity categorization based on the Functional Assessment Staging Tool (FAST) (see Primary Predictors). The Medicare Provider Analysis and Review file was used to identify patients with an International Classification of Diseases, Clinical Modification Codes, 10th Revision (ICD-10) code for dementia. The Beneficiary Summary file was used to verify Medicare Fee-for-Service enrollment and to obtain sociodemographic information. This study was approved by our university’s institutional review board (#13-0549). A Data Use Agreement was reviewed and approved by the Centers for Medicare and Medicaid Services.
Patient Cohort
Criteria from the Home Health Quality Reporting Program specification models27,28 were modified to identify our cohort from 2 086 755 Medicare beneficiaries admitted to home health between October 12 016 and September 30, 2017 (Figure 1). The cohort was limited to those individuals who had an index hospitalization prior to home health admission. Consistent with the Home Health Quality Reporting Program specification models, we excluded individuals for the following reasons: (1) admitted to home health more than 30 days after discharge from an acute or psychiatric hospitalization; (2) under the age of 66 years; (3) transferred between home health agencies; (4) non-continuous Medicare Fee-for-Service coverage for 12 months prior to the index hospitalization and 31 days after the hospital discharge; (5) discharged from the acute care hospitalization against medical advice; (6) missing items of interest in the Outcome Assessment Information Set; (7) having a discharge status that the Centers for Medicare and Medicaid Services excludes from the specification model (hospice, federal hospitals, law enforcement, etc.); and (8) hospital stay was for non-surgical treatment of cancer. Flow chart depicting cohort selection at each step as exclusion criteria were applied. Percentages represent percent remaining from the previous step.
Three additional exclusion criteria were applied consistent with the aims of this study. First, patients who did not have an ADRD diagnosis were excluded. Second, those patients not assigned at least 2 therapy visits were excluded from the study to better define our outcome of interest, early discharge. Third, in addition to removing patients with a discharge status excluded by CMS (see above), we also removed patients who were admitted to the hospital, rehabilitation facilities, nursing home facilities, or whose discharge status was unknown. This exclusion criterion was used as we were interested in examining the amount of therapy visits provided within completed home health episodes. The final sample included 91 302 home health patients with ADRD who were discharged to the community (with or without formal assistive services).
Dementia Diagnosis
Beneficiaries with dementia were identified using 19 ICD-10 codes included in the Chronic Conditions Data Warehouse algorithm for Alzheimer’s disease, related disorders, or senile dementia (Supplemental Table 1).29,30 Beneficiaries with 1 or more of these ICD-10 codes for dementia in Medicare Part A, home health, skilled nursing, or inpatient rehabilitation claims in the year prior to hospitalization were classified as having ADRD.
Outcome
Early discharge from therapy services was defined as missing more than 2 of the planned therapy visits. Early discharge was determined by comparing the difference between the total number of planned rehabilitation visits (physical therapy, occupational therapy, speech therapy) on the start of care OASIS (item M2200) to the total number of rehabilitation visits billed. The total number of therapy visits billed was determined by using Revenue Unit Count variables from the Revenue Center File. Revenue Unit Count is a quantitative measure of the number of times a service was provided. Revenue Unit Counts for physical therapy, occupational therapy, and speech therapy were summed to determine the total number of therapy visits provided. It is common for patients in home care to miss 1 or 2 scheduled visits for a variety of reasons such as medical appointments or religious observances. Setting the bar at 2 instead of zero accounts for this usual occurrence.
Primary Predictors
The primary predictor was dementia severity. We used a previously developed dementia severity categorization based on items from the Functional Assessment Staging Tool (FAST) and the OASIS (Supplemental Table 2). 31 Both the FAST and the OASIS are clinical assessments of a patient’s functional status. The FAST is a sequential assessment that categorizes a patient’s dementia severity based on their functional abilities.32-34 The dementia severity categorization used for this study divides dementia severity into 6 categories based on the 7 stages of the FAST.33,34 As has been previously described, 31 each category was identified through an iterative process that created a crosswalk between items on the FAST and items on the OASIS. Items included in the crosswalk were cognitive status, instrumental activities of daily living, activities of daily living, incontinence, verbal expression, and mobility. These items were selected based on their face validity with the description of each FAST stage. The first (i.e., lowest) dementia severity category represented FAST stages 1 and 2. At stages 1 and 2, symptoms are not clinically observable or reported by patients making it appropriate to group these stages together. The remaining 5 dementia severity categories aligned directly with the remaining 5 stages of the FAST.
Covariates
Sociodemographic characteristics included age, sex, race/ethnicity, Medicare original entitlement, and Medicare – Medicaid dual eligibility status. Health care utilization characteristics included length of index hospitalization, days in the intensive care unit/critical care unit, primary diagnosis and procedure categories from index hospitalization (based on the Centers for Medicare and Medicaid Services multilevel clinical classification software), receipt of dialysis during the index hospitalization, and the number of hospitalizations in the previous year. Two additional control variables were included (1) a composite measure of caregiver assistance need and availability, and (2) need for assistance with oral medications. The variable for caregiver support was based on an OASIS item that addresses the need for assistance in the following areas: (1) activities of daily living; (2) instrumental activities of daily living; (3) medication administration (4) medical procedures/treatments; (5) management of medical equipment; (6) supervision or safety; and (7) advocacy or facilitation. Each item is rated on a 6-point scale that was rescaled as a 4-point scale: no assistance needed (1-points), caregiver provides assistance (2-points), caregiver needs training to give assistance (3-points), and patient needs assistance, but a caregiver is not available (4-points). A summary score was then calculated (range 0-28) with higher scores reflecting greater unmet caregiver needs. Based on the distribution, summary scores were broken into quartiles. The OASIS item for oral medication management rates patients on a 4-point scale: independent (0-points), needs assistance with dosages or making a medication schedule (1-point), needs reminders to take medication at correct times (2-points) and medication must be administered by another person (3-points). A value of “not applicable” indicates that the patient has no prescribed oral medications. This item was not modified. Additional OASIS items related to function and mobility were not included in the model due to high correlation with the items used to develop the dementia severity scale described above.
Data Analysis
For each patient characteristic, we calculated early discharge rates and 95% confidence intervals (CIs). We used multilevel logistic regression to study the relationship of ADRD severity, caregiver support, and medication management with early discharge from home health, adjusting for patient demographics, patient comorbidities (using the Centers for Medicare and Medicaid Services Hierarchical Condition Categories based on diagnoses from the past year of acute care stays and the non-primary diagnoses from the index hospitalization), and clinical characteristics. Risk Ratios were calculated by adjusting the odds ratios as described by Zhang and Yu. 35 A second level random effect was used to account for the clustering of patients within home health agencies. All data analyses were performed using SAS software version 9.4. 36
Results
Cohort Characteristics and Observed Rates of Early Discharge.
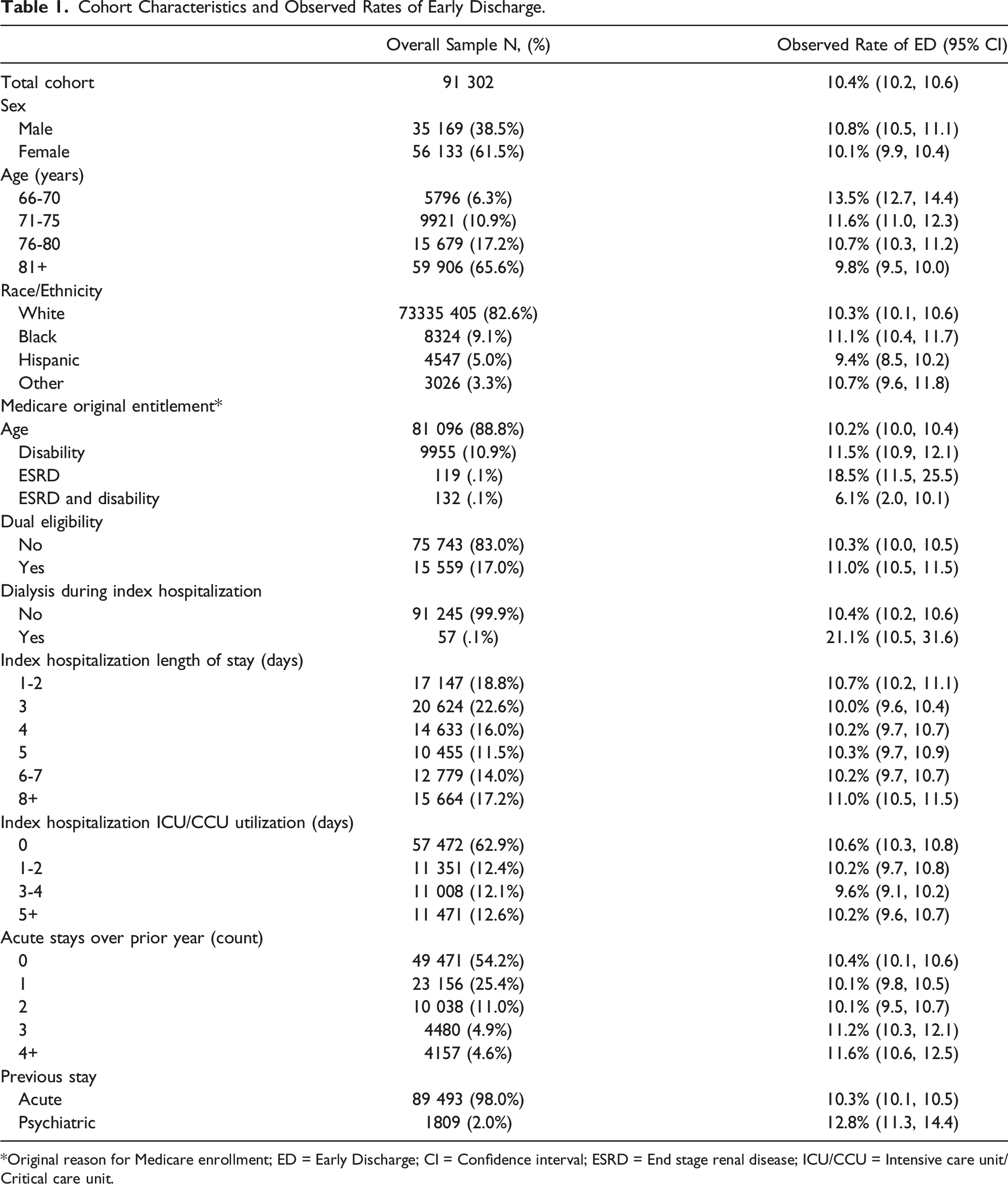
*Original reason for Medicare enrollment; ED = Early Discharge; CI = Confidence interval; ESRD = End stage renal disease; ICU/CCU = Intensive care unit/Critical care unit.
Observed Rates of Early Discharge from Home Health for ADRD Severity, Caregiver Support, and Medication Management.
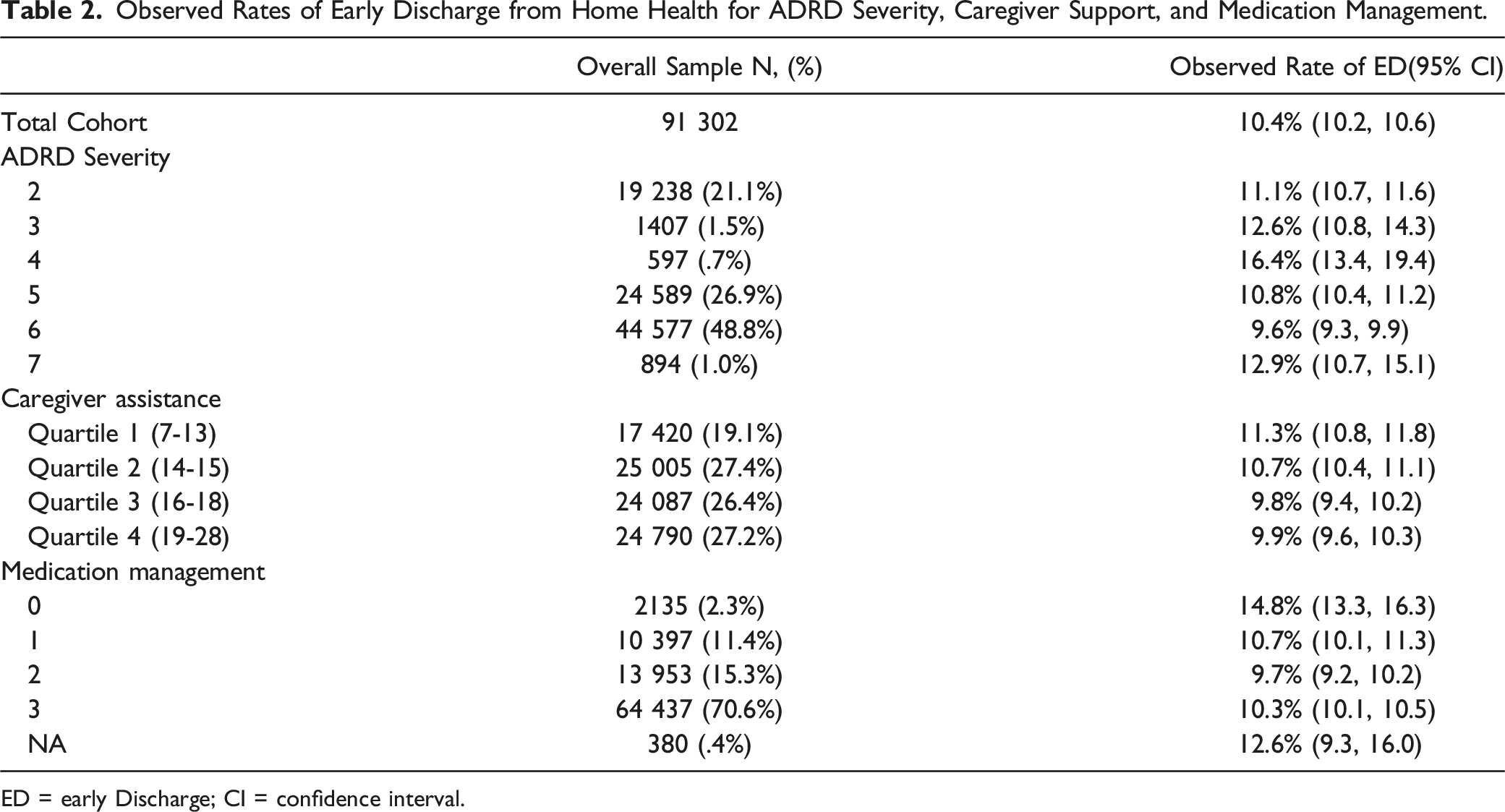
ED = early Discharge; CI = confidence interval.
Relative Risk of Early Discharge from Home Health.

ED = early discharge; CI = confidence interval.
Discussion
We hypothesized that rates of early discharge from home health services would increase in the later stages of ADRD. The findings of this study do not support this hypothesis. Rates of early discharge did not demonstrate a pattern across the ADRD stages. The highest rate of early discharge occurred in stage 4. Individuals in stage 4 of ADRD usually live independently, are oriented to time and place, and are able to navigate familiar locations. 37 However, individuals at this stage rely on denial as their primary defense mechanism and often withdraw from challenging situations. 37 It is possible that these coping mechanisms may contribute to their increased rates of early discharge as therapists may not see the benefit of continuing therapy. Another contributing factor to early discharge may be the presence and type of neuropsychiatric symptoms. Recent research has identified sub-syndromes of NPS that vary in frequency, intensity, and occurrence across ADRD and that present different levels of challenge to care providers. 38 It is possible that these sub-syndromes of NPS, and not ADRD severity, are a contributing factor to early discharge. Future research should explore the relationship between NPS subsyndromes and early discharge from home health for people with ADRD. Conversely, it is also possible that these individuals were discharged early because they exceeded expectations and met their rehabilitation goals quicker than expected.
In this study, people with ADRD who were assessed to be independent with oral medication management or who reported that they did not take any oral medications had a greater risk of early discharge than those who required assistance with oral medication management. Cognitive deficits inherent to ADRD can impair an individual’s ability to understand and manage their medications appropriately. 39 The progressive nature of ADRD makes it imperative that an individual’s ability to manage medications is continually assessed. Inappropriate medication management can result in unintentional non-adherence, medication errors, and hospital readmissions.39,40 It is possible that the ability to manage one’s oral medications is a proxy indicator for the individual’s overall health. Individuals who can manage their own medications or who do not have oral medications may progress through therapy and meet goals quicker than expected and therefore be discharged early. An individual’s ability to manage their medications may change throughout the course of the home health episode. If evolving medication management needs are not met, they may contribute to early discharge. Future studies should examine if changes in medication management across the course of a home health episode are associated with risk of early discharge.
The critical role of caregivers in the care of people with ADRD is well recognized. In this study, individuals with ADRD who had unmet caregiver needs were less likely to experience early discharge than individuals whose caregiving needs were met. Unmet caregiving needs is associated with an increased risk of negative health outcomes including institutionalization, hospitalization, and mortality.41-44 Unmet caregiving needs commonly occurs in the realms of safety, medical care, meaningful activities, and legal assistance or advocacy.44,45 Prior research has identified that 90% of people with ADRD had unmet caregiving needs related to safety, including fall risk and wander risk. 44 Patient safety concerns may factor into discharge decisions for patients with ADRD who have unmet caregiver needs in a way that they do not for patients who have adequate caregiver support.
Limitations
Our study has limitations. First, our method of identifying people with ADRD was based only on an ICD-10 diagnosis which has been shown to have poor sensitivity for detecting older adults in the early to mild stages of ADRD. 46 There also is not a gold standard for ADRD severity by which to compare the dementia severity scale. Our measurements of ADRD severity, caregiver support and medication management were based on items in the OASIS and we are not able to account for differences in how the assessment is administered among clinicians and across home health agencies. While the Centers for Medicare and Medicaid Services publishes a detailed implementation manual describing best practice in the Outcome Assessment Information Set administration, it is likely that there is variability in how items are interpreted and recorded. Finally, there is not a standardized definition of early discharge from therapy services in home health care. So, there is not normative data on which to compare our early discharge findings.
Conclusion
The results of this study did not support the hypothesis that rates of early discharge would increase as ADRD severity levels increased. This finding may be limited by the ADRD severity scale and definition of early discharge used in this study. While it was identified that people with ADRD with unmet caregiver needs and those who required assistance with medication had lower risk of early discharge from home health, the reason for these findings needs to be further explored. Future research should examine additional factors that may contribute to early discharge from home health for people with ADRD.
Supplemental Material
Supplemental Material - Association of Dementia Severity and Caregiver Support With Early Discharge From Home Health
Supplemental Material for Association of Dementia Severity and Caregiver Support With Early Discharge From Home Health by Sara Knox, Allen Haas, Brian Downer, and Kenneth J. Ottenbacher in American Journal of Alzheimer's Disease & Other Dementias®
Abbreviations
Alzheimer’s Disease and Related Dementias
confidence interval
Functional Assessment Staging Tool
International Classification of Diseases, Clinical Modification Codes, Tenth Revision
neuropsychiatric symptoms
Outcome Assessment Information Set.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the National Institutes of Health [R01HD069443; P2CHD065702; K01AG058789; K01AG073538; P30AG024832; U54GM104941] and the National Institute on Aging [K01AG058789; P30AG024832]. Funding agencies were not involved in study design, the collection, analysis, or interpretation of data, or in the writing of the report.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.