
Abstract
Family caregivers face ongoing, formidable stress and burden. Caregivers need sustainable support to maintain resilience. We aim to identify challenges, possible solutions that are resources for resilience, and expected consequences from the perspective of 39 family caregivers of hospice patients with dementia. The resilience framework was used to guide the coding and synthesis of the qualitative data. Identified challenges included difficulties in communication, providing care and decision-making, lack of knowledge, emotional challenges, concern about care facility selection, death with dignity, and lack of public awareness. Resilience resources for caregiving challenges were identified at the individual, community, and societal levels. Anticipated benefits of using these resources included the ability to provide better care and have a better quality of life for both patients and caregivers. The findings of this study can guide the design and implementation of supportive interventions designed for family caregivers of hospice patients with dementia to bolster available resilience resources.
Keywords
Introduction
Alzheimer’s disease is the sixth leading cause of death in the United States, and its mortality rate has dramatically increased from 1980 to 2014. 1 Alzheimer’s disease is the most common type of dementia. The number of persons with Alzheimer’s disease and related dementias (ADRD) is projected to reach 65.7 million in 2030 and rise to 115.4 million in 2050. 2 This increase is expected to lead to a proportionate rise in the use and costs of hospice care for persons with ADRD. 3 In 2016, dementia was among the top 3 primary diagnoses for hospice patients. 4 Among hospice patients, those with dementia account for the most days of care and the largest amount of Medicare spending. 4 The health-care costs for persons with dementia including hospice services are projected to increase from US$259 billion in 2017 to US$1.1 trillion in 2050. 5
Dementia Caregiving in Hospice Care
Hospice provides the gold standard of care for patients with ADRD at the end of life, facilitating much-needed assistance to family caregivers who have long provided care often in the absence of tailored support. 6 In this study, we focus on the US definition of hospice, which is compassionate care delivered to patients with a prognosis of 6 months or less, and their families, mostly in outpatient settings such as private residences or nursing homes. The role of family caregivers can be fulfilling, but burdening on caregivers themselves. 7 Stress and caregiving burden can negatively impact caregivers’ morbidity and mortality. 8 Caregivers of persons with ADRD face particularly stressful demands associated with the extended length of care, potential behavioral problems common in late-stage dementia, and the extreme impairment and debilitation of patients with end-stage disease. 9 Caregivers of a hospice patient with dementia have to grapple with continuous, stressful situations while assisting with basic and higher order activities of daily living of their patients such as personal hygiene, medication management, household chores, and transportation. 10 This has the potential to lead to chronic stress, depression, deteriorating physical health, tenuous financial conditions, and premature death because of caregiving burden and stress. 11 -13 Support for meeting caregivers’ health and emotional needs to mitigate health risks should be provided to avoid such catastrophic consequences of stressful hospice dementia caregiving. Compared to patients with other kinds of conditions, patients with dementia demonstrate unique needs and require substantial support. 11
Caregivers experience dementia grief associated with the disruption in communication and memory, which is perceived as many small and large losses throughout the disease progression before physical death. 14 -16 Toward the end of the patient’s life, caregivers may face difficulties and need specific resources at various points in the disease trajectory. They may have to cope with intense intellectual and emotional conflicts because caregivers reckon with uncertainty about continued unpredictable losses and when to expect the death of their patient. 9,17 It is imperative that hospice care develops support services for caregivers tailored to those who care for patients with ADRD. 18
Resilience Resources for the Challenges of Hospice Dementia Caregiving
In response to persistent caregiving stress, health-care professionals are called upon to provide sustainable, steady, and continuous support throughout the entirety of the disease trajectory and even after. Family caregivers should be able to restore balance and harmony when they encounter negative circumstances, which may be achieved by enhancing inherent adaptation, also known as caregiving resilience. 19,20 Caregivers are more likely to be resilient when they are knowledgeable, supported by family members, and able to have access to support services such as respite care. 21 In addition, personal mastery, self-efficacy, and coping strategies are considered resilience domains that have a protective effect on health outcomes. 22 Caregivers’ responses to their hospice dementia caregiving challenges and possible solutions for improving their resilience have yet to be fully understood due to the paucity of research studies in hospice adopting the resilience lens. Identifying resources that enhance resilience among family caregivers can inform family-centered, supportive interventions. Health-care professionals, administrators, and policymakers can contribute toward an infrastructure and appropriate policies to facilitate access to supportive resources for the patient–caregiver dyad. Thus, it is necessary to fill knowledge gaps in meeting family caregivers’ unique needs to foster and facilitate their resilience in the context of hospice dementia caregiving. The aim of this study was to identify challenges, possible resources for resilience, and associated benefits for family caregivers of hospice patients with dementia.
Methods
A theory-driven, deductive content analysis of secondary data obtained from a clinical trial (NIH/NINR, R01NR012213, PI: Demiris) was carried out to explore family caregivers’ experience in taking care of hospice patients with ADRD. The parent study was designed to test the efficacy of a problem-solving therapy intervention for hospice caregivers with the goal to improve their capacity to handle challenges. The parent study recruited 514 hospice caregivers who were 18 years or older, completed a 6-grade education at least, could speak and read English, and received home hospice services for their patient. Trained interventionists engaged the hospice caregivers in behavioral intervention sessions by using problem-solving skills, and intervention questions were structured according to the problem-solving therapy intervention manual. A more detailed description of the parent study can be found elsewhere. 23 Out of a total of 514 hospice caregivers from the parent study, we only included the 39 caregivers whose care–recipient’ primary hospice diagnosis was reported as ADRD given the focus on hospice dementia caregiving experiences for this study who were assigned to the problem-solving therapy intervention and completed study procedures.
Conceptual framework
This study used the resilience framework for caregivers developed by Windle and Bennett, 24 which has been used in several studies 21,25,26 in order to capture caregiving challenges, solutions (resilience resources), and expected consequences (see Figure 1). We categorized various resources into the individual, community, and societal levels. 26 First, resources at the individual level include psychological resources, such as mastery, personal control, competence, self-esteem, and appraisal. Examples of individual-level resources are: caregivers’ own abilities to maintain normal functioning, manage stress, stay positive, and have a sense of humor; biological factors such as gender and age; material factors such as income and financial capacity; and internal traits and personal characteristics such as health behavior. Second, resources at the community level include geographically immediate community resources which are located in or near the caregivers’ neighborhood areas. Formal and informal social support from friends and other family members are considered resources at the community level. Social participation and cohesion (eg, dementia support groups or religious groups) and housing are also included. Finally, resources at the societal level are associated with laws, policies, national associations, and government organizations. Social policies, welfare and respite services, including home help, day and respite care, innovative services (eg DVDs), culture, and religion can be intertwined with these structures. Medicare hotline service can be an example of the resources at the societal level.
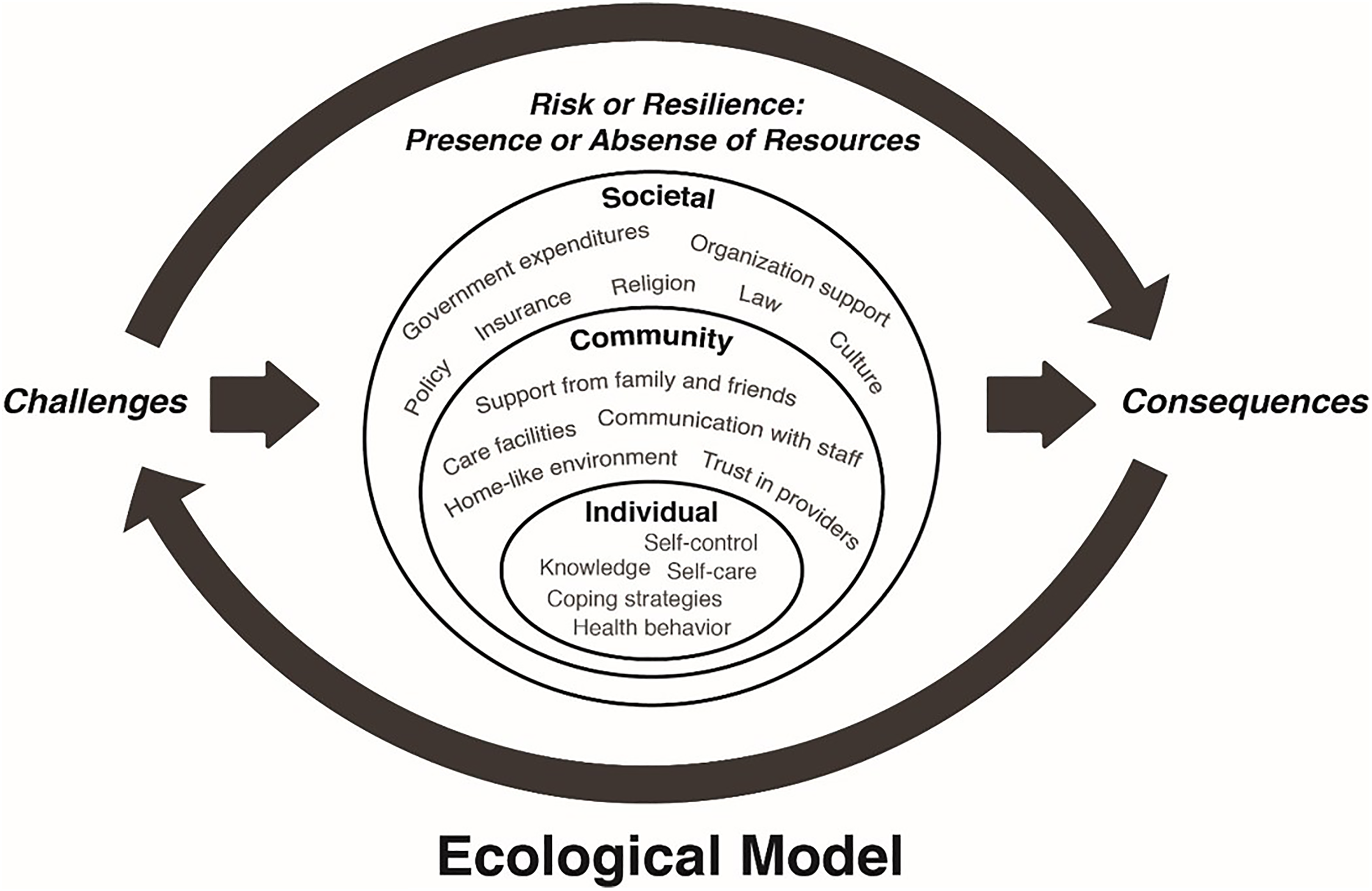
Conceptual framework of resilience resources (adapted from Windle and Bennett 24 and reproduced with permission of Bennett et al26) for hospice dementia family caregivers.
Data Analysis
Using the resilience framework, a deductive content analysis was conducted. 27 Four members of the team served as coders and had either in-person meetings or e-mail communications to match each coder’s coding results, discuss inconsistencies to find agreements, and develop the comprehensive coding framework. Professional transcriptionists transcribed interviews verbatim. Thirty-nine transcripts were independently analyzed by 3 authors (S.H., N.-C.C., and C.H.). Initially, they coded line by line for content that fit the components and dimensions of the resilience framework and categorized resilience resources into 3 levels. The first 3 transcripts were coded individually and compared. For any cases where there were differences in coding, a consensus was reached after discussion with 4 members (S.H., N.-C.C., C.H., and G.D.) and the rest of the transcripts were coded. The intercoder agreement was 89.23% and the Cohen κ value was 0.78, indicating solid agreement between coders. 28 To enhance the trustworthiness of our results, we used peer debriefing on a regular basis to discuss the process. 29
Results
Characteristics of the Study Participants
Descriptive statistics are described in Table 1. We studied 39 caregivers (30 females; 9 males with a mean age of 62 years [standard deviation, SD: 7.4]). The relationships of caregivers to hospice patients were: adult child (82.1%), spouse/partner (7.7%), niece (5.1%), and friend (5.1%). Hospice patients consisted of 31 (79.5%) women and 8 (20.5%) men. The 39 patients had an average age of 90.2 years (SD: 7.3).
Characteristics of Caregivers and Patients.a
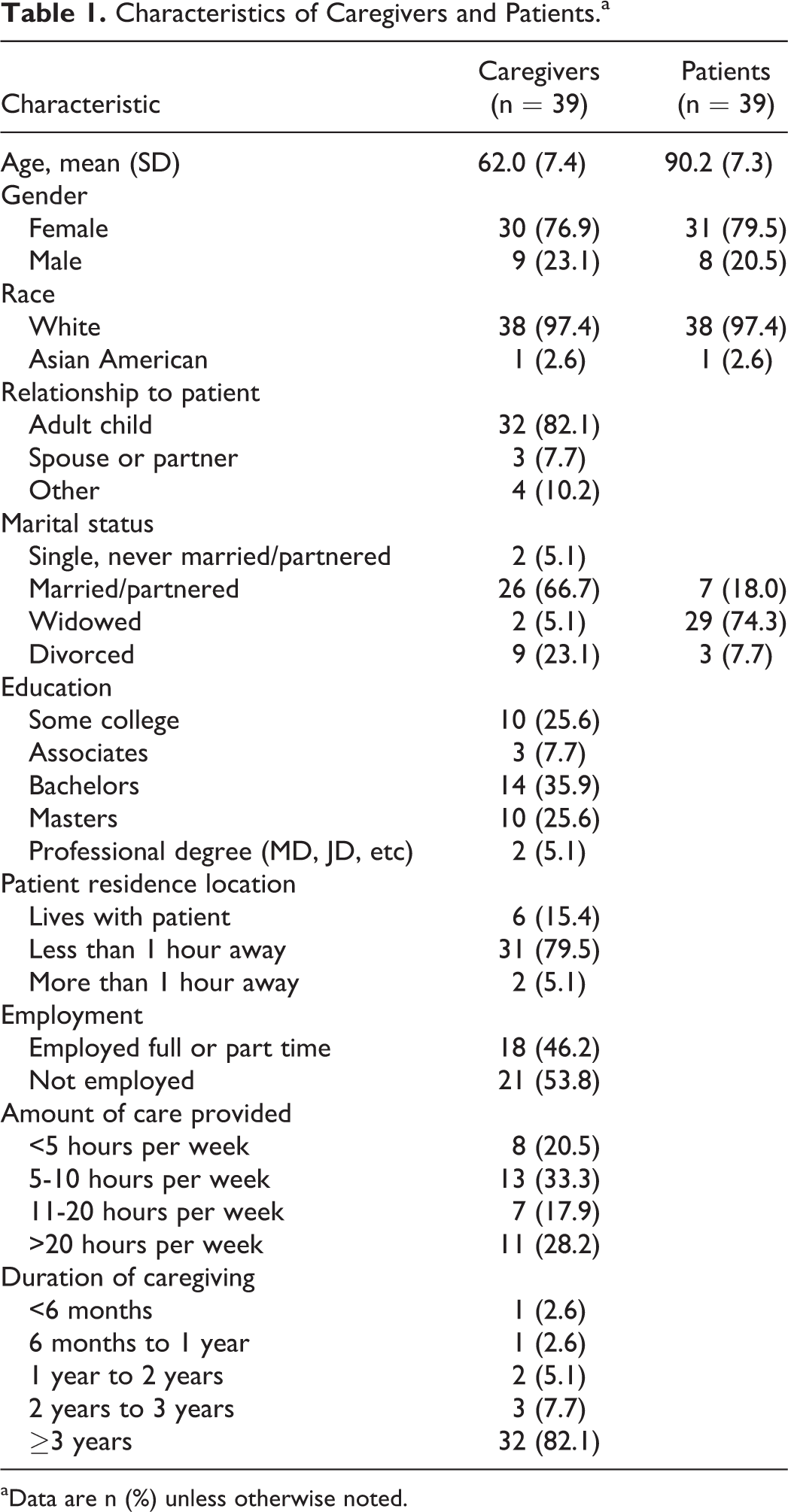
aData are n (%) unless otherwise noted.
Dementia-Related Challenges and Resilience Resources in Hospice Dementia Caregiving
We used the existing resilience framework to code themes in relation to caregivers’ challenges, resilience resources, and expected consequences from the interview data. We identified dementia-related challenges and related resilience resources as expressed by caregivers. We do not discuss all challenges in the main text but rather elaborate on the most frequently addressed ones; for a comprehensive set of challenges, please see Tables 2, 3, and 4. Resilience resources were classified at the ecological levels: individual, community, and societal.
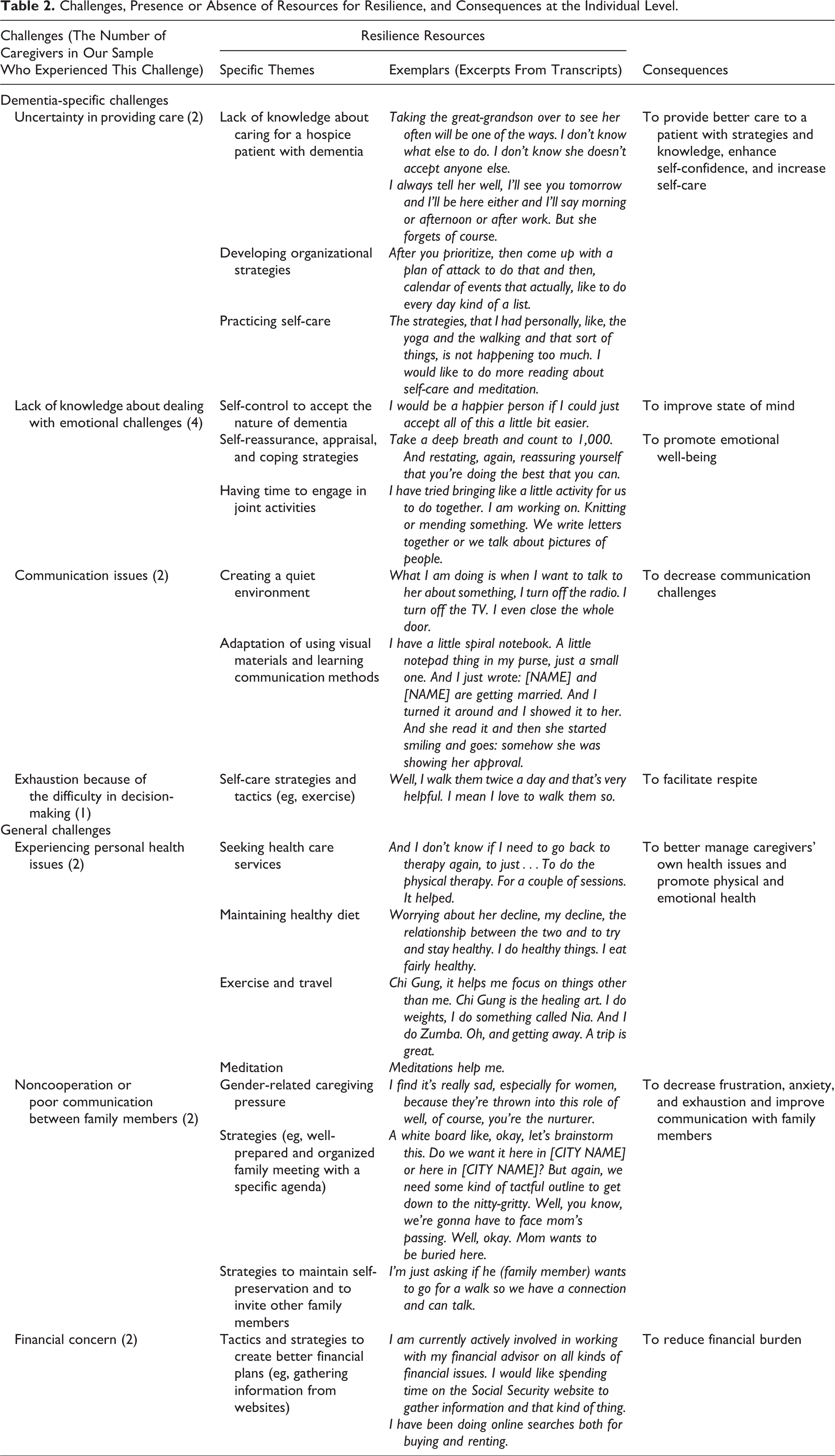
Challenges, Presence or Absence of Resources for Resilience, and Consequences at the Individual Level.
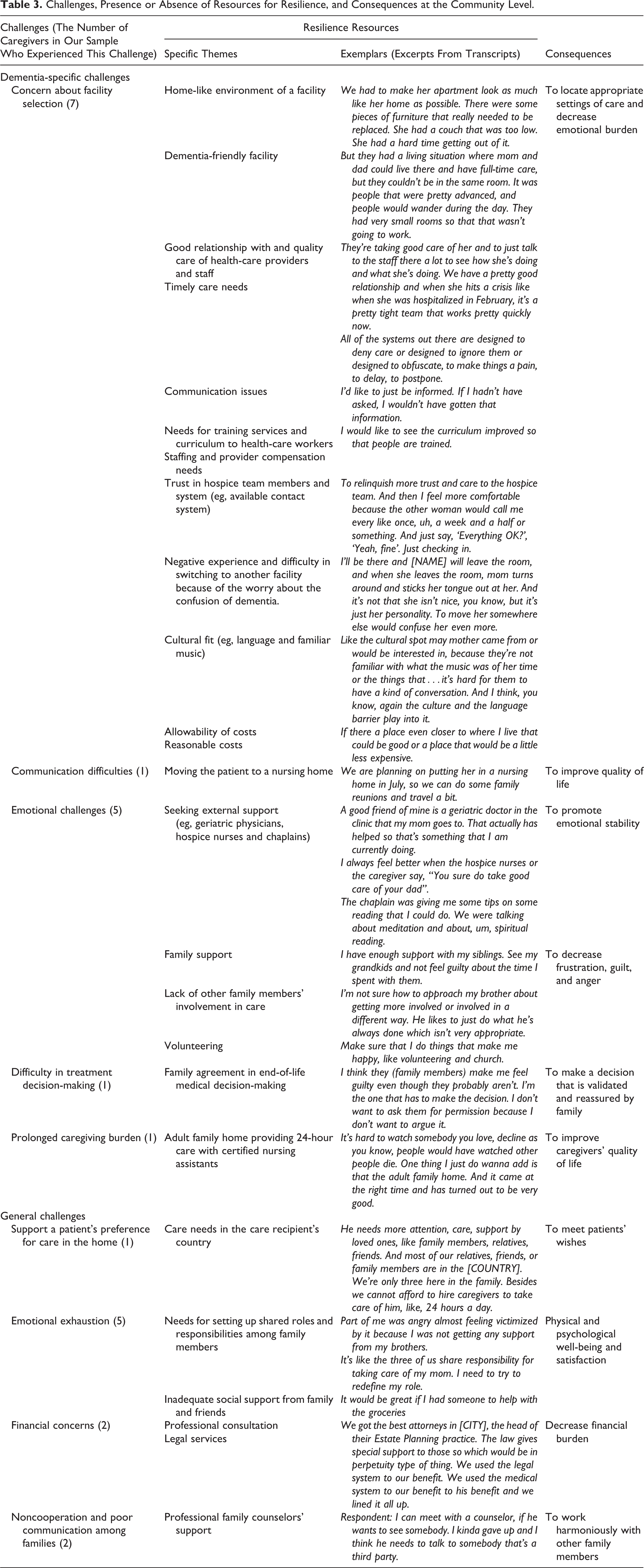
Challenges, Presence or Absence of Resources for Resilience, and Consequences at the Community Level.
Individual level
1. Knowledge support for contributing to self-appraisal
There were several dementia-related challenges that could be resolved by using resilience resources at the individual level (Table 2). First, 6 caregivers addressed lack of knowledge in how to manage their anxiety, cope with emotional stress, and provide appropriate care to their patient. Caregivers pointed out that assessing and managing the care needs of a hospice patient with dementia is challenging, as these needs change over time and assessment can be complex. Patients with ADRD may show confusion and mood instability, impeding communication. Additionally, feelings of guilt, irritability, agitation, anxiety, and fatigue exacerbate those difficulties. One caregiver mentioned feeling “tied down” because of continuous obligations that force the caregiver to visit the care–recipient every week. In spite of those particular dementia-related issues, caregivers were able to identify individual strategies and tactics such as recognizing limitations and accepting the unpredictable nature and symptoms of dementia as one of the examples of individual-level resilience resources. In addition, another caregiver stated that he/she made a point of reinforcing belief in himself/herself. This caregiver added that this self-appraisal was helpful in alleviating a feeling of guilt and in increasing self-confidence. Another caregiver also used self-appraisal strategies such as self-talk or writing mental preparation to manage frustration, guilt, and anger.
Two caregivers reported having communication issues with their patients because of the patients’ progressive deterioration along with pain, agitation, and hearing impairment, especially when the patients were reluctant to wear a hearing aid, uncooperative, or confused. Caregivers having such issues developed effective communication methods by using visual materials in a quiet environment as an individual resource to promote improved listening and comprehension. I tried twice. She just would look at me and it was just not getting in there. And so finally, I just took—I have a little, a little spiral notebook. A little notepad thing in my purse, just a small one. And I just wrote: [NAME] and [NAME] are getting married. And I turned it around, and I showed it to her. And she read it and then she started smiling…. somehow she was showing her approval.
2. Self-care management and activities
Caregivers highlighted a challenge to manage self-care and their routine activities and tried to find their own self-management strategies at individual levels. One caregiver expressed exhaustion related to pressure during the decision-making process and wished to maintain a normal, routine life. According to several caregivers, sometimes they wanted the patient to die and be free from suffering, yet still wanted to see and spend time with the patient. One caregiver developed self-care strategies such as exercising to boost his/her level of energy. Identifying strategies to overcome emotional challenges was also one of the important individual resilience resources. Another caregiver explicitly described that following good health practices and maintaining well-being were indispensable.
Community level
1. Utilizing the facility: Home-like environments
Next, we identified resilience resources at the community level (Table 3). Concerns about choosing the right facility were expressed by many caregivers. Some caregivers had positive experiences and others had negative experiences regarding the facility that they had selected. According to one caregiver, his/her patient said that she was very happy because the room in the facility reminded her of her own home. Some caregivers emphasized that the facility spaces should be equipped with home furniture that is more appropriate for people with ADRD.
2. Utilizing the facility: Dementia-friendly environments and building trusting relationships
One caregiver pointed out that patients with dementia need larger rooms because they often wander and talked about the residential environment needing to be adaptable to the symptoms of dementia. Another caregiver reported difficulty when attempting to have phone or in-person conversations with nurses in the facility about his/her family member, stating that shift changes and nurses’ busy schedules interfered with their availability. However, another caregiver felt that nurses in the facility where his/her loved one stays in provided constant quality care despite shift changes. Two caregivers addressed the critical components of good care, which includes staff members’ ability to deal with an impending crisis, ability to tightly coordinate in a timely manner, and ability to build a good, trusting relationship with patients and their family, through effective communication.
3. Utilizing the facility: Providers and staff members’ communication skills and attitudes
Communication impacts the quality of a facility. Almost 71% of the caregivers emphasized the importance of communication. Because the progression of dementia can be complicated, communication was perceived as critical to caregivers. Based on their experience, health-care providers sometimes did not provide specific information on a patient’s changing condition, which was important information to caregivers, even if not considered clinically important for providers. Our study participants also argued that providers should have opportunities to improve their communication skills through continuing education or increased compensation.
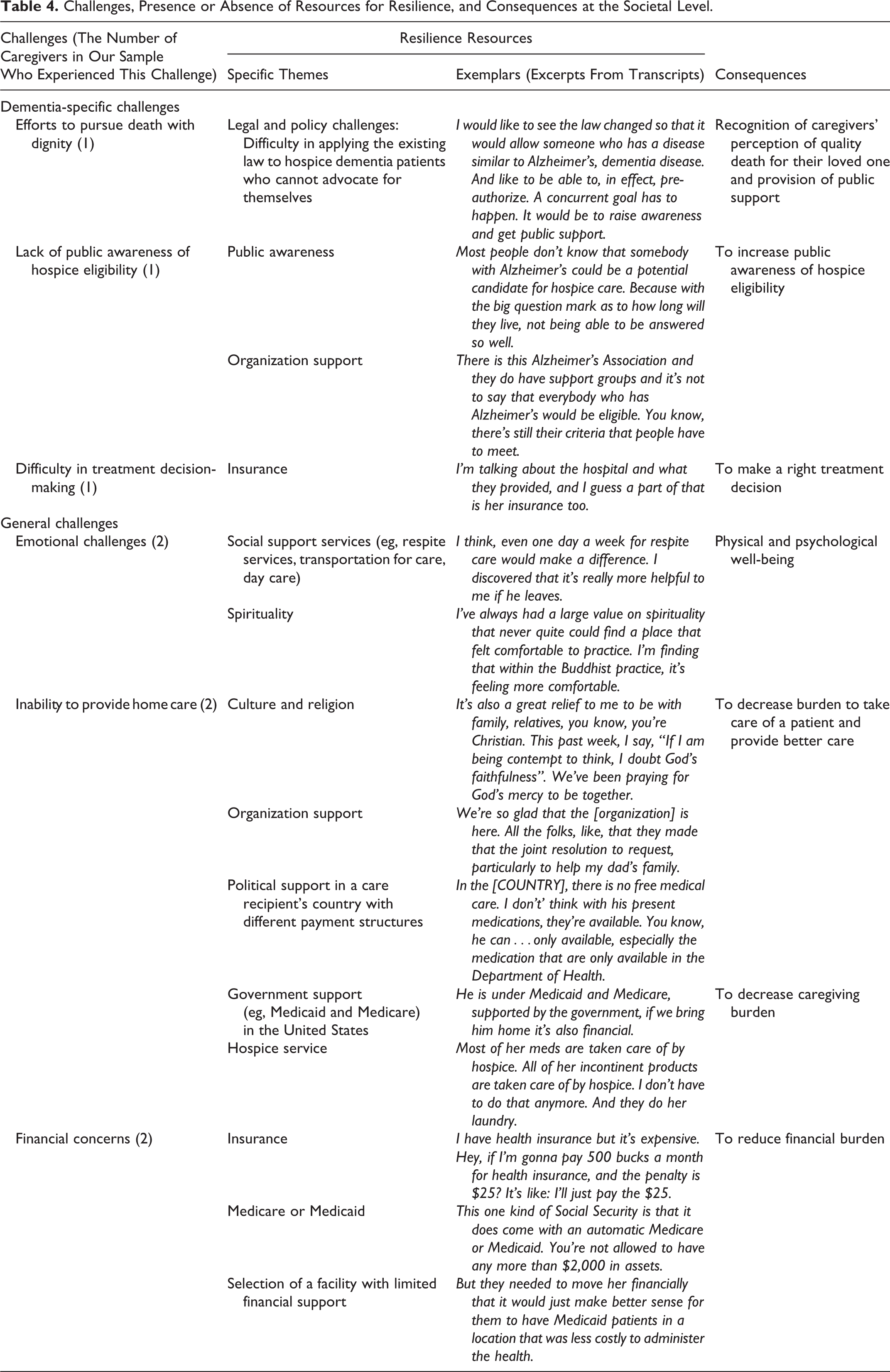
Societal level
Caregivers tried to resolve their challenges by using resilience resources at the societal level (Table 4). These resources were law, policy, or insurance related or provided by religious or cultural groups, state or federal organizations, or other entities. One caregiver emphasized legal challenges resulting from the fact that patients with ADRD cannot express themselves. The caregiver wished for the person with dementia to die with dignity through local policy by crafting laws and also pointed out that hospice eligibility for patients with dementia and treatment decision-making are tough topics due to prolonged caregiving. Another caregiver pointed out that having insurance makes it easier to make treatment decisions because insurance or financial status influences the direction or quality of care.
Challenges, Presence or Absence of Resources for Resilience, and Consequences at the Societal Level.
General Challenges and Resilience Resources
We identified general challenges that caregivers emphasized but are not exclusive to dementia care. Challenges that can be supported by resources at the individual level include (Table 2): (1) personal health issues, (2) communication with other family members or health-care providers, and (3) financial problems. Those 3 general challenges can be alleviated by using individual resources. Methods and strategies to improve their own health problems such as physical therapy, healthy diet, exercise, travel, and the use of medications were identified. One caregiver prepared for a family meeting with a specific goal and suggested sharable activities to other family members to have a more effective communication. There is an absence of resources for gender-related pressures when it comes to the difficulty in communicating with family members. Female caregivers in many cases were expected to serve as the primary caregiver, and they perceived the caregiving burden to be heavier for women. To solve financial concerns, the caregivers gathered information that was helpful for them in choosing the best option, which was one of their personal strategies.
For services provided at the community level, caregivers experienced various challenges (Table 3). In 1 case, a patient had moved to the United States from another country and was expressing the wish to die in his country among his close family members. This posed several challenges including the fact that the primary caregiver was residing in the United States. Furthermore, the patient received both Medicaid and Medicare in the United States, and the caregiver expressed concerns about the cost of care in the patient’s country where supportive systems for end-of-life care did not exist. The caregiver felt isolated because all other family members resided in the patient’s country increasing her perceived emotional burden.
There are general challenges that can be supported by resilience resources at the societal level (Table 4). Using social support services and drawing support from communities of faith can in some cases address emotional challenges, inability to provide home care, and financial problems. One caregiver had full support from family members, but the family support was not enough to support the primary caregiver and decrease the caregiver’s burden. The caregiver said she started relying on prayer even though her extended praying caused her internal conflict and doubts about her trust in God.
Absence of Resilience Resources
Capturing what resources caregivers wish to have access is one of the priorities in an aging society. We specifically identified the resilience resources that do not exist, but caregivers wish to receive, especially for caregivers of hospice patients with dementia. Caregivers stated that they do not know how to provide better care to their patient and deal with emotional challenges. Caregivers experienced frustrations because their patients used repeated phrases and were not able to remember previous conversations. Some caregivers developed self-strategies (eg, using communication tools and writing communication) and were engaged in joint activities with their patient.
Many caregivers addressed struggles when they needed to choose a facility for their loved one. They inevitably confront formidable challenges when they are not satisfied with the external support system. Identifying the appropriate facility was perceived as a challenging task. Caregivers wanted health-care providers at a facility to provide meaningful and detailed information about the continuously changing status of a hospice patient with ADRD by phone call or in-person follow-ups on a regular basis. They prioritized facilities that have an available contact system, enhancing trust in health-care providers, and provide 24/7 care. Caregivers also wanted to have an opportunity for a family meeting or a team meeting with providers. As one caregiver pointed out, facilities need to be culturally adapted and, more importantly, provide respectful care for multicultural populations. Caregivers stated that facilities should offer a culturally fit environment for patients with dementia with an understanding of what kind of music patients with dementia had enjoyed. Caregivers also complained about language barriers between patients and some health-care staff members in the facility.
Other support that caregivers desired to receive includes financial support, family or friend support, social support services such as respite care, and spiritual and political support. According to one caregiver, when family support is limited, one tends to “lean on spiritual power.”
Discussion
This study employed secondary analysis of data regarding caregivers of persons with dementia admitted to hospice care to explore their challenges and resilience resources as well as expected consequences. The unique challenges include uncertainty in providing care, lack of knowledge, emotional challenges, communication issues, difficulty in treatment decision-making, concern about care facility selection, prolonged caregiving burden, death with dignity, and lack of public awareness. Resilience resources include knowledge, self-control and appraisal, self-care, using visual materials, having options to choose a good care facility which is home-like and dementia-friendly with trustful, respectful providers and staff, family or friends’ support, involving in volunteer activities, legislative support, public awareness, and health insurance. Through these resilience resources, family caregivers can provide better care, have fewer communication issues and less caregiving burden, be harmonized with other family members, make a right treatment decision, and have a better quality of life. Our findings can inform the design of supportive interventions for families caring for their hospice patient with ADRD. This article provides insights into what resources are not present but can be supplied. Making up for the depletion of resources for resilience can contribute to high-quality hospice care for patients with dementia.
The application of the resilience framework helped us to comprehensively present a variety of resources for resilience at multiple levels. Several caregivers exhibited their capacity to identify available resources and predict positive consequences. Resilient families have the capacity to set goals and priorities. 30 Caregivers with a higher level of resilience may cope more effectively during stressful times. On the other hand, for caregivers who have a lower level of resilience and limited coping mechanisms to fulfill the caregiving duties, external resources need to be provided because the surrounding environment can affect the individual’s strength. As Borson and Chodosh 31 proposed, dementia-capable health-care systems require the consideration of the uniqueness of dementia, early invitation of partners, and accessible information that our participants addressed during the interview. Enrollment of a loved one with ADRD in hospice can offer substantial benefits to caregivers’ perception of the patient’s quality of life and death, greater satisfaction with management of terminal pain and shortness of breath, and a marked reduction in perceived unmet needs for knowledge about the dying process and what to do when death occurs, as well as substantial improvements in social support during the dying process. 32,33
Several caregivers in our study emphasized the need to support patients’ autonomy for their respectful death when it comes to the choice of place for care. Patients with dementia often prefer to stay in a home-like facility. Approximately, 70% of palliative care patients wish to be cared for at home at the end of life, although only 25% of them die at home. 34 Supporting the patient–caregiver dyads to avoid early, unnecessary transitions to a care facility is important to meet the patient’s desire to remain at home. Yet, if patients need to transfer to a facility, the place must be a dementia-friendly environment to make the transition as comfortable as possible. Cognitively impaired patients have particular characteristics, such as wandering, which require a certain environment to accommodate them. It is important to provide a familiar, home-like environment with a large space to walk around with environmental stimuli. 35 Caregivers had different opinions regarding the quality of care they received. Perceived quality of care may be impacted by staff shifting. Providing tools to improve clinicians’ ability to deal with unexpected health events and to develop communication skills may also have a positive influence on the quality of care. Literature highlights the lack of communication skills training for clinicians. 36 -38 It becomes essential that health-care providers and staff members strive to take care of patients with respect in a noncondescending manner to make the patients calm because patients’ personality and emotions remain even in the severe stages of dementia with cognitive loss. Health-care professionals need to consider strategies to improve communication with family caregivers. Providing a more supportive communication environment for patient–family caregiver dyads is crucial in dementia care. 39 In addition, religious and cultural considerations were also emphasized. Caregivers talked about culture as expanding to ways of life that can be reflected in language, material cultures such as clothing and food, religious forms, and cultural products such as music, literature, and art consistent with the broader definition of culture in the literature. 40 Moreover, several caregivers developed their own coping strategies and self-control. When caregivers properly use positive appraisal through self-monitoring, self-management, and self-evaluation, they can boost their confidence and caregiving skills. Possessing the ability to maintain positive emotions through these coping mechanisms, which is presented as a form of resilience, may mitigate and reduce stress.
Several limitations in our study have been accounted for. Our data were extracted from a parent larger study designed for another research question. For that reason, several parameters listed in the resilience framework (eg, health behavior or characteristics) were not present in our secondary data set. The differentiation between societal and community levels is obscure due to the ambiguity of the definitions of resources between each level. For example, having a support group can be interpreted as either societal level or community level, or both. We differentiate them based on geography and accessibility of the resource. If a resource can be obtained in their community or near it, we considered the resource as a community-level resource. If a resource can be provided by a state or federal entity or a religious organization, we considered the resource as a society-level resource. A few resources overlap. For example, we included trust in health-care providers and the health-care system under the category of resources at the community level in this study. This could be addressed at the societal level because culture is a broader concept and trust can be considered as one of the cultural elements. Mistrust in health-care providers can be created by cultural barriers. 37 Trust in health-care providers can be maximized by having effective communication and being assured that hospice team members are competent, communicative, and caring, which would be the way we pursue to support hospice patients with dementia and their caregivers. Nevertheless, the focus of this study was to comprehensively identify as many resources as possible based on the resilience framework at multiple levels, not to divide resources into each level, and not to differentiate them at each level. Another limitation is the use of a single data set in one geographic location with a sample of caregivers who had limited diversity. There is the possibility of sample bias. Notwithstanding these limitations, the findings of this study are important as they highlight caregivers’ unique challenges and a lack of resilience resources.
Future Research
Understanding caregivers’ experience lays the groundwork for future research. The next step would be to conduct prospective data collection using theoretical sampling through semi-structured interviews with family caregivers to produce richer and varied data. As indicated above, it will be important for researchers to ensure a more diverse sample of participants with different backgrounds and characteristics such as race, ethnicity, and educational level in future studies. Analysis of qualitative data by applying policy analysis may evaluate the impact of a policy, law, or regulation on communities regarding several resources at societal and community levels addressed by caregivers in this study. In addition, designing interventions to facilitate access to supportive resources may ultimately increase caregivers’ resilience to maintain a good quality of life and promote dignity and palliation for the patient. Additional studies can explore challenges to improving the quality of a facility and care by health-care providers and the design of educational interventions for clinicians in order to address challenges related to infrastructure and communication. Research is also needed in testing the efficacy and effectiveness of supportive behavioral and coping interventions, designed specifically for caregivers of patients with ADRD.
Conclusion
Despite the pursuit of a better quality of life and death, family caregivers taking care of hospice patients with dementia are facing various significant challenges. Our findings show that several resilient caregivers have found and used resources which can be informative and helpful for other caregivers. Their experience can inform interventions and raise awareness about the importance of providing resilience resources at multiple levels.
Footnotes
Authors’ Note
S.H. contributed to secondary analysis study design and manuscript write-up. S.H., N.-C.C., and C.H. analyzed and interpreted the data and provided advice. G.D. provided guidance in the qualitative data analysis; he led the clinical trial that generated the data for this study and contributed to the design of the study, data analysis, and interpretation of findings as well as manuscript preparation. D.O. and K.W. contributed to the design of the study, interpretation of findings, and manuscript preparation. All authors have read, reviewed, and approved the final version of the manuscript. The parent study was approved by the institutional review board of the University of Washington.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by the National Institutes of Health, National Institute of Nursing Research (grant number R01NR012213; Principal Investigator: G. Demiris).