
Abstract
Alzheimer’s disease and related dementias are more prevalent in rural areas than in urban areas in China. This study aims to examine the role of dementia beliefs and knowledge in influencing dementia worry among rural adults in China. Data were generated in a cross-sectional survey of 577 participants. Hierarchical regression analyses found that both the beliefs and knowledge of dementia contributed to higher levels of dementia worry. The propensity score matching method affirmed the robustness of regression results. In addition, those aged 45-64 reported higher worry about dementia than those aged 65 or older, while being married was related to lower dementia worry. As one of the first kind studies that examined dementia worry in rural Chinese population, our findings suggest that policy and practice efforts should address cultural beliefs of dementia as they contributed to higher worry about dementia in rural areas.
Keywords
Introduction
Alzheimer’s Disease International estimated that more than 55 million people worldwide live with dementia and that this number will increase to 78 million by 2030, lack of access to trained clinicians, fear of diagnosis and cost are key barriers to identifying a diagnosis for people with dementia. 1 Dementia refers to a series of symptoms characterized by problems with short-term memory and other cognitive deficits, resulting from progressive neurological diseases or other causes. 2 The progressive cognitive impairment due to dementia leads to the eventual loss of independence.
Alzheimer’s disease and related dementias (ADRD) is the most common neurodegenerative form of dementia. 3 Incidences of ADRD increases substantially due to advanced age. Symptoms of the disease occur when neurons involved with cognitive functions are damaged or destroyed. As ADRD continue to progress, nerve cells that are responsible for basic motor functions, such as swallowing and walking are negatively impacted, in the final stage of the disease, patients become incapacitated and bedridden needing round-the-clock care until the end of their life. 4
Because of the close association between ADRD and older age, ADRD has become a growing concern for Chinese older adults, a rapid increasing population. By the end of 2019, the number of older people aged 65 and above in China was 176.03 million, which accounted for 12.6% of the total population. 5 Over the past 30 years, the prevalence of dementia in China has increased dramatically. A recent published study estimated that China will have the world’s largest dementia population by 2050, reaching almost 35.97 million. 6 The projected huge number and rapid growth of older people with dementia in China can bring significant care challenges to families and communities.
More than half of the total Chinese population lives in rural areas. 7 Investigating the influence of dementia beliefs and knowledge on perceived dementia worry in both rural and urban areas will be of great importance for providing information used in developing appropriate dementia education policies. However, it is especially essential to understand the perception of dementia among Chinese rural residents, as the prevalence of dementia was more than twice higher in rural areas (11.98%) than in urban areas (5.19%) among people aged ≥65 years in China. 8
Given the wide urban-rural disparities in socioeconomic development and access to health and services in China. Rural residents tend to have relatively low educational attainment, poor socioeconomic conditions, poor health literacy, and limited access to social and health services, all of which contribute to an increased risk of developing dementia.9-11 Furthermore, sociocultural (eg, traditional beliefs with emphasis on intergenerational support) and environmental factors (eg, availability of specialty care) in rural areas can affect rural adults’ dementia beliefs, knowledge, and worry.12,13 Therefore, research efforts are urgently needed to shed light on the perception of dementia among rural population who can be more vulnerable to dementia.
Beliefs of dementia in Chinese culture are influenced by 2 long-standing beliefs: fatalism and stigmatization of mental illness. 14 Because of fatalism, people tend to view dementia as normal aging and delay or reject formal diagnosis and treatment. Since the stigma associated with dementia, families tend to hide a relative’s dementia condition from others, which affects the timely access to appropriate treatment and care for the patients. 15 People with dementia may face misunderstanding, isolation, and even abuse. 16 Such stigma not only contributes to the poor quality of life of patients with dementia, but also reinforces a horrifying belief of dementia among family caregivers and the general public.
Knowledge of dementia refers to an individual’s accurate understanding of dementia from medical or scientific perspectives, such as its causes, symptoms, risk factors, progression, consequences, treatment, and impact.17,18 Solid knowledge of dementia, including its initial symptoms, progression, and management, is essential for timely detection of dementia, early medical treatment, development of a clear treatment plan, and the provision of appropriate care. 19 Therefore, improving the knowledge of dementia among rural residents of China is imperative to potentially eliminate their dementia worry and prejudice.
Dementia worry is an emotional response to the perceived threat of developing dementia. 20 Cutler and Hodgson (1996) 21 coined the term “anticipatory dementia” to explain the fears of middle-aged adults and their cognitive changes as a potential precursor to dementia. 22 Conceptually, this can be thought of as a specific type of health worry that represents an important but underexplored health problem of an aging population, also known as the anxiety or fear associated with dementia. This is an emotional response to an anticipatory worry. As there is no known cure or recovery from dementia, worry about dementia is widespread in the general population, 20 and may affect not only older people who perceive memory changes or declines, but also other age groups with or without cognitive impairment.
A moderate level of concern can serve as a warning signal to help people notice potential dementia threats and promote effective preparedness to respond to these threats. 20 Frequent and intense worry about dementia may lead to lower life satisfaction, a worse outlook on the future, avoidance of medical support, limited medical consultations, and forced cognitive assessments, and may even lead to objective cognitive impairment in some cases.23-25 So it is important to understand the factors that influence dementia worry.
Health behavior models (HBM) as a conceptual formulation for understanding the determinants of health related actions. 26 The model assumption that an individual’s decision to obtain a dementia evaluation, depends on the individual on the susceptibility of dementia, the severity of dementia, and take action to reduce disease susceptibility and severity of benefits and barriers, in addition, according to HBM, other modify variables, such as demography, also may have a significant impact on health related behavior. Socio-Cultural Health Belief Model (SHBM) provides an empirically based conceptual framework, which is derived from the HBM. SHBM posits that cultural beliefs affects beliefs and knowledge of dementia, which in turn affects perceptions of susceptibility and severity of dementia, and that dementia worry is associated with not seeking care. 18 Based on SHBM, we hypothesize that knowledge and beliefs of dementia directly influence dementia worry.
Existing research demonstrates that sociodemographic characteristics such as age and gender can explain some variation in worry about dementia.27-29 As risk of dementia increases with age, worry about dementia is conflated with the broader aging process itself.20,30 According to previous studies reports, the effect of age on dementia worry remains controversial. Some studies have revealed that higher age is positively associated with worry about dementia. 31 Further research has shown that perceived worry about dementia was significantly higher for those aged 50 to 64 and 65 to 74 than older people. 32 However, another study reported no difference in dementia worry levels regarding age. 27 Some studies have reported that increased worry about dementia was associated with being female.21,31
Adult children of parents with a history of dementia are more likely to worry about dementia than adult children of parents with no history of dementia. 33 The closer the contact with patients with dementia, the higher the degree of anxiety about dementia. 34 In addition, losing independence and dignity, being a burden to others, potential suffering from a mental problem, and the daunting financial cost of long-term care are all worries related to dementia.35,36
Although there is a large amount of literature examining the factors influencing dementia worry and the relationship between dementia beliefs, knowledge, and worry,37-39 among the existing studies, there are researchs on dementia beliefs, knowledge, and worry in urban settings, but little research specifically focused on dementia beliefs, knowledge, and worry among rural adults. And most studies are based on convenience samples or specific at-risk populations, making it difficult to generalize the findings to residents of rural areas. 40 In addition, previous findings have not been consistent or comprehensive, and more research is needed to confirm these findings in different social and cultural contexts. To fill these research gaps, we conducted a study on a sample of adult residents of rural areas in Shaanxi Province, China. Shaanxi province, located in the western part of China, is an underdeveloped state with underdeveloped health service infrastructure in its vast rural counties. 41 The cost of dementia treatment and care poses psychological stress for older adults in rural Shaanxi province than for those who live in other regions. In the present study, we aimed to examine the beliefs and knowledge of dementia in influencing the worry about dementia in a sample of adult residents from rural areas of Shaanxi province, China.
Methods
Sampling and Participants
The data was collected from a cross-sectional study conducted between November 2014 to December 2014 on adults (aged 18 or above) in rural areas of Shaanxi province, China. Self-administered questionnaires were distributed in 3 counties in Shaanxi province: Dali county in Weinan City on the east of the Guanzhong Plain, Fengxiang county in Baoji City on the west of the Guanzhong Plain, and Yichuan county in Yan’an City in the north of Shaanxi province. A county was defined as an administrative unit one level below a city and consists of several townships. The choice of these 3 counties is largely because of their geographic locations. They are located in 3 directions in Shaanxi Province, and inclusion of this geographic diversity can be more representative of the overall situation of the province. Moreover, the 3 counties share similarities in population composition, labor structure and economic development. After the counties were determined, 6 to 9 townships were randomly selected from each county, and farmers were randomly selected from these townships.
Paper questionnaires were distributed to each participant. Well-trained research assistants were on spot to provide assistance when participants were not clear about questions or how to fill it out. The assistants did not discuss the question contents with participants, and their role is to ensure participants completed the questionnaire within 40 minutes and check, so as to ensure the validity of the questionnaire. It should be noted that the investigators’ guidance has not been involved the discussion of the questionnaire contents, but only for the filling in instructions, such as explaining the reserved time and indicating where to fill in the answers. After removing the invalid data, the valid sample size was 577, including 198 farmers from Dali County, 198 from Fengxiang County, and 181 from Yichuan County. The study protocol was approved by Biomedical Ethics Committee of Xi’an Jiaotong University. Verbal informed consent was obtained from participants before the data collection. Participants were told that their participation was entirely voluntary and that they could terminate at any time.
Measures
Dependent variable
Worry about dementia.
Independent variable
Beliefs of dementia.
Knowledge of dementia.
Covariates
Survey Sample Demographics (N = 577).
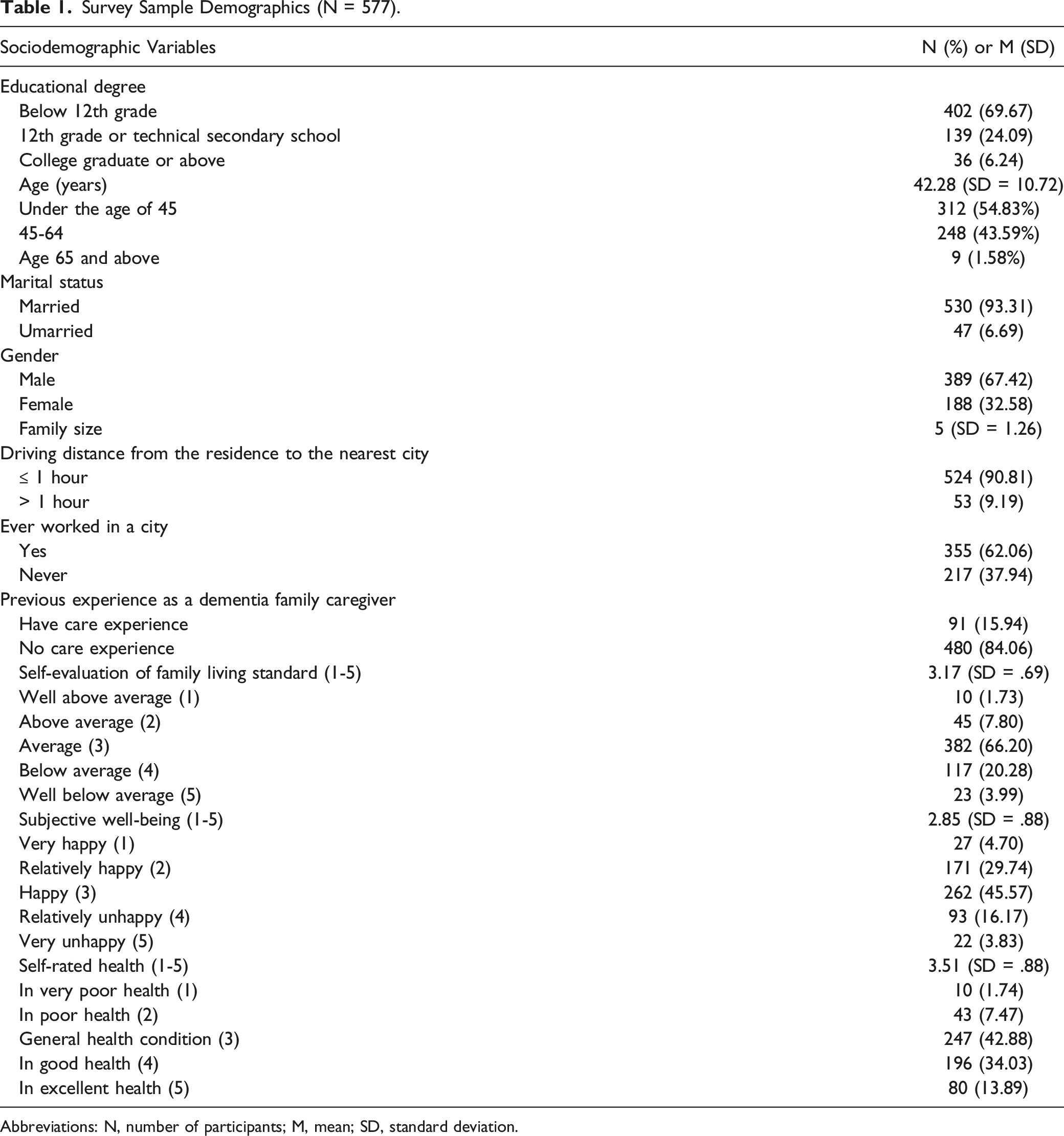
Abbreviations: N, number of participants; M, mean; SD, standard deviation.
Data Analysis
To determine the impact of different variables on worry about dementia, a three-step hierarchical linear regression analysis was used to examine the relation of covariates, dementia beliefs, dementia knowledge, and dementia worry. The 3 models were entered into the hierarchical linear regression analyses one at a time. The first model estimated the association between covariates and worry about dementia. The second model added dementia beliefs. The final model entered dementia knowledge.
The hierarchical regression analysis has inherent endogeneity problems such as sample selection bias and missing variables, as well as 3 kinds of risks including accumulative presupposition, average effect and collinearity. PSM was first proposed by Paul Rosenbaum and Donald Rubin in 1983. 48 It is a simulation of randomized experimental data, which matches the treatment group and the control group according to the propensity value to reduce the bias estimation of the treatment effect. Therefore, the treatment group and the control group have similar or balanced distributions on the included covariates. Its theoretical framework is the “counterfactual inference model”. This study adopted PSM to verify the robustness of regression results through reduction of the selection bias. STATA version 13.0 (Stata Corporation, TX, USA) was used for statistical analysis.
Results
The Results of the Three-Step Hierarchical Regression Analysis
Results of Hierarchical Multiple Regression Analysis.

AbbreviationsSE, Standard Error.
Notes: * P < .05 **P < .01 ***P < .001.
aReference group is those with an education level less than 12th grade.
bReference group is those under the age of 45.
cReference group is those who have never experience as a dementia family caregiver.
dReference group is those never worked in a city.
The Result of PSM
In the PSM model, the independent variables of dementia belief and dementia knowledge were divided into high and low groups. The score of dementia belief between 10 and 29 was defined as the low group and coded as 0. The score of dementia belief between 30 and 50 was defined as the high group and coded as 1. The score of dementia knowledge between 1 and 24 was defined as the low group and coded as 0. The score of dementia knowledge between 25 and 32 was defined as the high group, and coded as 1. Those coded as 0 were marked as the control group, and those coded as 1 were marked as the treatment group. Covariates affect the sample distribution of the treatment group and the control group during the matching process.
The Robustness Test of Different Matching Methods.

Notes: The nearest neighbor matching (k = 4), and the width of the radius matching is .01; * if B > 25%; R outside [.5; 2].
Average Treatment Effect on the Treated.

Abbreviations: ATT, average treatment effect on the treated; SE, Standard Error.
Notes: The nearest neighbor matching (k = 4), and the width of the radius matching is .01; *P < .05, **P < .01, ***P < .001.
The propensity score fitting of dementia beliefs and dementia knowledge before and after matching is shown in Figures 1 and 2. After PSM, the range of common value of kernel density functions of the control group and the treatment group was enlarged, and further superposition and coverage appeared. The results showed that the characteristic distribution of each covariate was consistent between the control group and the treatment group. Balance test of dementia beliefs before and after k-Nearest neighbors matching. Balance test of dementia knowledge before and after k-Nearest neighbors matching.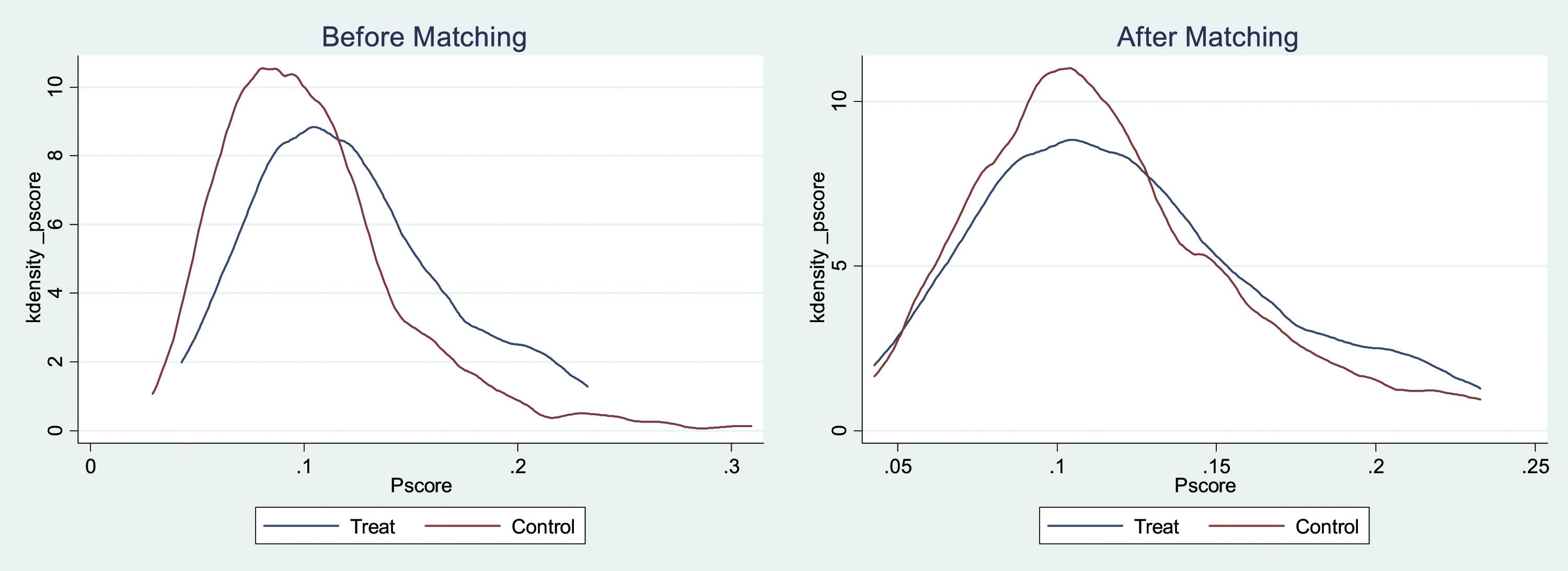

Discussion
According to our findings, higher levels of beliefs about dementia were positively associated with increased worry about dementia. This result is consistent with our hypothesis based on the SHBM. Many respondents do not know how to utilize available resources and strategies to help prevent or respond to the onset of dementia. People with biases and stereotypes about dementia tend to avoid interactions with patients with dementia, assuming them all live a miserable life. 22 This study found that participants with more misperception and stigma associated with dementia had greater the worry about developing it. In rural areas of Shaanxi province, China, knowledge of dementia is not widely available, and many rural adults’ knowledge of dementia is formed through negative experiences of visiting relatives and friends with dementia in long-term care. People with high levels of worry about dementia may tend to avoid reminders of dementia, including interactions with people living with dementia. This may reinforce the stereotype that dementia is associated with loss of memory, health, dignity, and identity. This further deepens the worry about developing dementia.
Our results show that higher levels of knowledge about dementia are positively associated with greater worry about dementia. This result is not surprising, as a similar finding was found among older Chinese Americans. 14 This result was opposite conclusion of our hypothesis. The positive relation may be due to the fact that people who know more about dementia are more likely to be alert to dementia signs and symptoms, and when there are some behaviors suspected of dementia in daily lives, they are more likely to develop a worry about dementia. It has been shown that there is a correlation between risk perception and worry about dementia. 31 Obtaining more knowledge of dementia can help develop a clear perception of risk. In addition, currently, there is no access to dementia care specialists in China’s rural areas, and a number of dementia screening instruments are not suitable for use due to the context of rural primary care. 16 When people suspect they have symptoms of dementia, the delay in obtaining a professional medical and scientific diagnosis can exacerbate the worry about dementia. Therefore, educational opportunities related to dementia are important for rural primary health care professionals due to the lack of specialized resources. 49 However, it is not sufficient just to provide dementia education, but more important to provide supportive services, such as counseling. Provide education and support services for people with dementia and to ensure that these support are sustainable. This may help rural residents to feel more secure and thus less worried about the uncertain situation they or their family members may face if they develop dementia.
Our findings indicate that people aged 45-64 have a higher level of worry about dementia. This may be due to the influence of traditional family values and filial piety culture, in which supporting the older adults are a family responsibility. This tradition is protected and restricted by domestic law, and upheld in Chinese society. 50 The 45-64 age group is likely to be the main cohort providing care for older adults relatives with dementia. In the care process, caregivers in this age group may witness the whole process of dementia gradually worsening, thus increasing their worry about dementia. Concerns about the inheritance of dementia can also aggravate the worry about dementia in caregivers of this age group. Another possible explanation is that aging stereotypes are often internalized by older people, leading to negative self-image, and deep negative self-perception negatively affects physical functioning and health.51-53
Our research also found that married people had lower levels of worry about dementia than unmarried people. One possible explanation is that married people may feel secure and less anxious because their marriage can provide support, accompany and care for each other when one partner develops dementia. Another explanation is that most married families have children, who are likely to provide support and care for their older parents in rural China. Notwithstanding China’s developing urbanization, falling fertility rate, transformation of traditional female roles, improvement in healthcare among the older adults with chronic diseases, and/or cognitive impairment, and accompanying extension of life expectancy, China has yet to overhaul traditional family responsibility. Influenced by the traditional Chinese culture of filial piety, in which adult children care for older adult parents, most older adults in China are taken care of by families, including older adults with dementia. 54 Dementia care can be demanding in regards to meeting the patient’s needs for medication management, symptom monitoring, and assisting with activities of daily living. Intergenerational support could be crucial to reducing worry about developing dementia and the anticipated caregiver burden.
In China, public health problems with dementia, include low awareness, low screening rate, low treatment rate, and high morbidity. This study focused on dementia worry among adults in rural China. Although our study examined only a few key factors associated with dementia worry, the results highlight that reducing dementia stigma can help reduce dementia worry in rural areas of China. Dementia education should not just focus on increasing knowledge of dementia, as it would increase dementia worry, but also needs to address the emotional responses of rural adults to dementia information provided.
According to existing research, dementia, old age, and symptoms of mental illnesses are regularly co-depicted in popular media, and people with dementia may be additionally stigmatized because of this depiction of intersectionality. 55 Family stigma may prevent family caregivers from seeking services for dementia patients. The most important action that can be taken is to promote education on dementia in rural areas, to expand awareness of the prevention and treatment of dementia, to reduce discrimination against dementia among rural residents, and to enable rural residents to have a correct understanding of dementia. In addition, it has promoted the construction of a dementia friendly environment in hospitals, parks, and other major living places, and encouraged public welfare organizations to carry out activities to care for older adults with dementia, so as to help patients with dementia maintain social participation as much as possible, slow down the process of dementia. The dignity and basic rights of persons with dementia should be protected, and friendly community and social environment should be created. 56
Rural areas in Shaanxi province lack long-term care, social services and other supportive infrastructure, not to mention prevention programs aimed to increase dementia literacy and promote healthy life style. Rural residents also have limited access to dementia-related information and education. 11 Therefore, there is a need to (1) increase the prevalence of dementia knowledge among rural residents, (2) strengthen the education of health information of rural residents, and (3) adopt strategies to improve the effect of public health education.
For family members, placing relatives with dementia in elder care facilities can lead to feelings of guilt, loss, and failure, which leads older Chinese to view dementia as a burden on family members.57,58 On the other hand, care demands such as medication management, symptom monitoring, and assisting with activities of daily living can be overwhelming for families. Based on the characteristics of dementia and the limited formal resource in rural China that emphasize family responsibilities, we encourage home-based care by bringing care support provided by formal or informal networks in rural community to homes for older adults with dementia. In addition, it is also very important to improve the paid care leave system and supporting policies to relieve burden of employed caregivers. A community-level family support platform for dementia has been established to provide family caregivers with disease consultation, skill training, psychological counseling and other support, so as to improve the efficiency and quality of home care.
There are several limitations to this study. Firstly, participants of our survey are from the rural areas in northwest China, which may not be representative of all rural areas in China. This limits the generalizability of our results. Secondly, this study only included samples from rural counties and future studies need to examine the urban-rural differences in beliefs, knowledge, and worry about dementia. Thirdly, the cross-sectional design limits the ability to draw causal conclusions. Lastly, not all variables affecting worry about dementia were considered in this research, for example, the moderating factors between dementia knowledge and dementia worry. Future research should explore potential moderators between dementia knowledge and dementia worry among other rural areas in China.
Conclusion
This study represents one of the first research efforts that explored dementia worry among rural population in China. Our findings highlight that policy and practice attention should be directed to modifying cultural beliefs of dementia as they contributed to higher worry about dementia in rural areas. Dementia education cannot just provide mere scientific or medical facts or information without addressing the emotional distress that may arise from such information sharing as our findings found a positive association between dementia knowledge and dementia worry.
Footnotes
Acknowledgments
We would like to thank every person who accepted our invitation to participate in the survey.
Declarations of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study is funded by Xi’an Jiaotong University.
Ethical Approval
The study has been approved by Biomedical Ethics Committee of Xi’an Jiaotong University, China.
Informed Consent
Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.