
Abstract
Despite substantial staffing and cost implications, the use of constant observation (CO) has been poorly described in the acute care setting. The purpose of this cross-sectional, multicenter, survey study was to assess hospital provider practices regarding the use of CO. Of the 543 surveys distributed, 231 were completed across 5 sites. Most respondents worked on medical units (67.5%), as nurses (49.1%); 44.8% were white; and 75.6% were female. The majority (84.2%) reported at least 1 patient/wk requiring CO. Most frequent indication for CO was dementia with agitation (60.7%), in patients older than 70 (62.3%) and predominantly by nurse assistants (93.9%). Almost half (47.3%) stated they felt pressured to discontinue CO, despite a strong perceived benefit (76%). Enhanced observation (92.6%) was most frequently used to decrease CO. Finally, 77.9% perceived that those performing CO lacked training. Our study highlights the widespread use of CO for hospitalized older adults with dementia.
Keywords
Background
Constant observation (CO) is defined as “an increased level of observation and supervision in which continuous one-to-one monitoring techniques are utilized to assure the safety and well-being of an individual patient…in the patient care environment.” 1 In 2009, The Joint Commission published The National Patient Safety Goals, indicating the use of one-to-one observation (CO) for patients at risk of harm, while advocating for the elimination of restraint use. 2
Individuals who provide CO have been referred to in the literature by numerous terms, including “constant observers,” “sitters,” “one-on-one observers,” “patient care attendants,” “patient safety attendants,” “activity companions,” and “therapeutic companions.” 3 –5 Sitters may include a variety of personnel, such as registered nurses (RNs), certified nurse assistants (CNAs), and other nonlicensed paid employees as well as family members and volunteers. Regardless of their title, the observation is predominantly delivered by hospital personnel not trained specifically for this task. 4,6 There are no national guidelines with regard to sitter qualifications, specific components of a required education and training curriculum, nor job descriptions and roles. 6 Furthermore, hospitals continue to struggle with the challenge of maintaining staffing and cost to provide CO. 1,5,7 –10 Previous studies exploring strategies to decrease the use of sitters in order to reduce high cost and disruption of staff responsibilities are numerous. 7 –9,11,12 –14
The concept of CO, which originated in patients with psychiatric disorders who are at risk to themselves or others, has been empirically expanded to address other clinical challenges such as fall prevention, delirium, and dementia. 5,10,11,15 Persons with Alzheimer’s disease and related dementias (ADRD) now account for 3.2 million hospital admissions per year. 16,17 For older adults with cognitive impairment, the unfamiliar, stressful, and complex hospital environment may result in exacerbation of behavioral and psychological symptoms of dementia (BPSD; ie, aggression, anxiety, apathy, depression, agitation, and wandering). 18 –23 In addition, up to half of all hospitalized older patients develop delirium, which may also lead to behavioral symptoms that require a higher level of care. 24
A 2018 scoping review on CO found a lack of clarity in the terms used to describe CO, who provides CO, variability in what the care entails, and the needs of patients requiring this care. 6 Furthermore, few studies have explored CO practices for patients with cognitive impairment. As the number of older adults and persons with dementia in the hospital setting continues to increase, further research is needed in order to understand the use and quality of CO for this population. Our study aimed to assess hospital provider practices and perceptions with regard to the use of CO for older adults with cognitive impairment.
Methods
We conducted an institutional review board (IRB)–approved (IRB# 17-0020-NH), multicenter, cross-sectional, anonymous survey with RNs, advanced practitioners, and physicians in the Greater New York metropolitan area. We used a purposive sampling strategy to obtain maximal diversity in responses from providers across the 5 hospitals. The survey was provided to a diverse array of nurses and nurse practitioners/physician assistants from different units across 5 different hospitals. We also provided the survey to hospitalists during meetings (not unit specific). To preserve anonymity and ensure valid and reliable responses, we did not monitor who completed surveys. Surveys were left on hospital units for participants to anonymously complete. Data collection occurred from July 2017 to December 2017. Surveys were collected by the principal investigator and research coordinator from each unit across the 5 hospitals. Survey data were entered into REDCap. 19 The survey instrument was investigator-developed in the absence of existing validated tools. We developed the instrument in REDCap for formatting purposes, printed it on paper, and administered it in person. To ensure face and content validity, the following process was used to iteratively develop the instrument: completing a comprehensive literature review; interviews with subject matter experts to ensure the topic of the survey was relevant to the population of interest; iterative item development/modification with feedback from psychometrics, biostatistics, geriatrics, and survey experts; assessment of item clarity; and cognitive interviews to ensure items were interpreted as intended and a small pilot with a convenience sample to assess survey logistics and data capture. We tested the survey on 10 participants, including 5 nurses and 5 hospitalists, and had 5 different iterations before reaching consensus on the final version. The major topics of the survey included number of patients on average who require CO, what conditions most frequently necessitate CO, duration of CO, who requests and who performs CO, age of patients requiring CO, policies and practices regarding CO, training/protocol for CO, perceptions and beliefs regarding CO, and demographic characteristics.
Statistical Analysis
Categorical and ordinal survey items were summarized for the overall sample of respondents using percentages. We compared the frequency (never, rarely, sometimes, often, very often) of CO use for several conditions across provider types using the Mann-Whitney U test, and hospitals using the Kruskal-Wallis test. Agreement with various statements regarding the use of CO (strongly disagree, disagree, neither agree nor disagree, agree, and strongly agree) was compared across provider types using the Mann-Whitney U test, and hospitals using the Kruskal-Wallis test. We assessed differences in responses to nominal survey items across provider types and hospitals using the χ2 test, or Fisher exact test when frequencies were <5.
A nominal P value of .05 was used to determine statistical significance. No adjustments were made for multiple comparisons. All statistical analyses were performed using SAS software version 9.4 (SAS Institute Inc, Cary, North Carolina) and R version 3.3.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Characteristics of Survey Respondents
Of the 543 surveys distributed, 231 were completed (42.5% response rate) across 5 sites in the Greater New York metropolitan area. The majority of respondents (82.4%) worked in 1 of 2 tertiary centers while 17.6% were from community hospitals. Nurses constituted the largest group of participants (49.1%), followed by physicians (35.6%). Among physicians, 22.2% had completed medical training requirements (attending physicians) and 12% were residents. Most respondents were female (75.6%); 44.8% were white, 25.9% Asian, and 14.2% black. Almost half (47%) of respondents were between 26 and 35 years old and 82.8% had 10 years or less of experience. Respondents worked primarily on medical units (67.5%), followed by telemetry (16.0%) and surgery (6.5%; Table 1).
Characteristics of Survey Respondents.
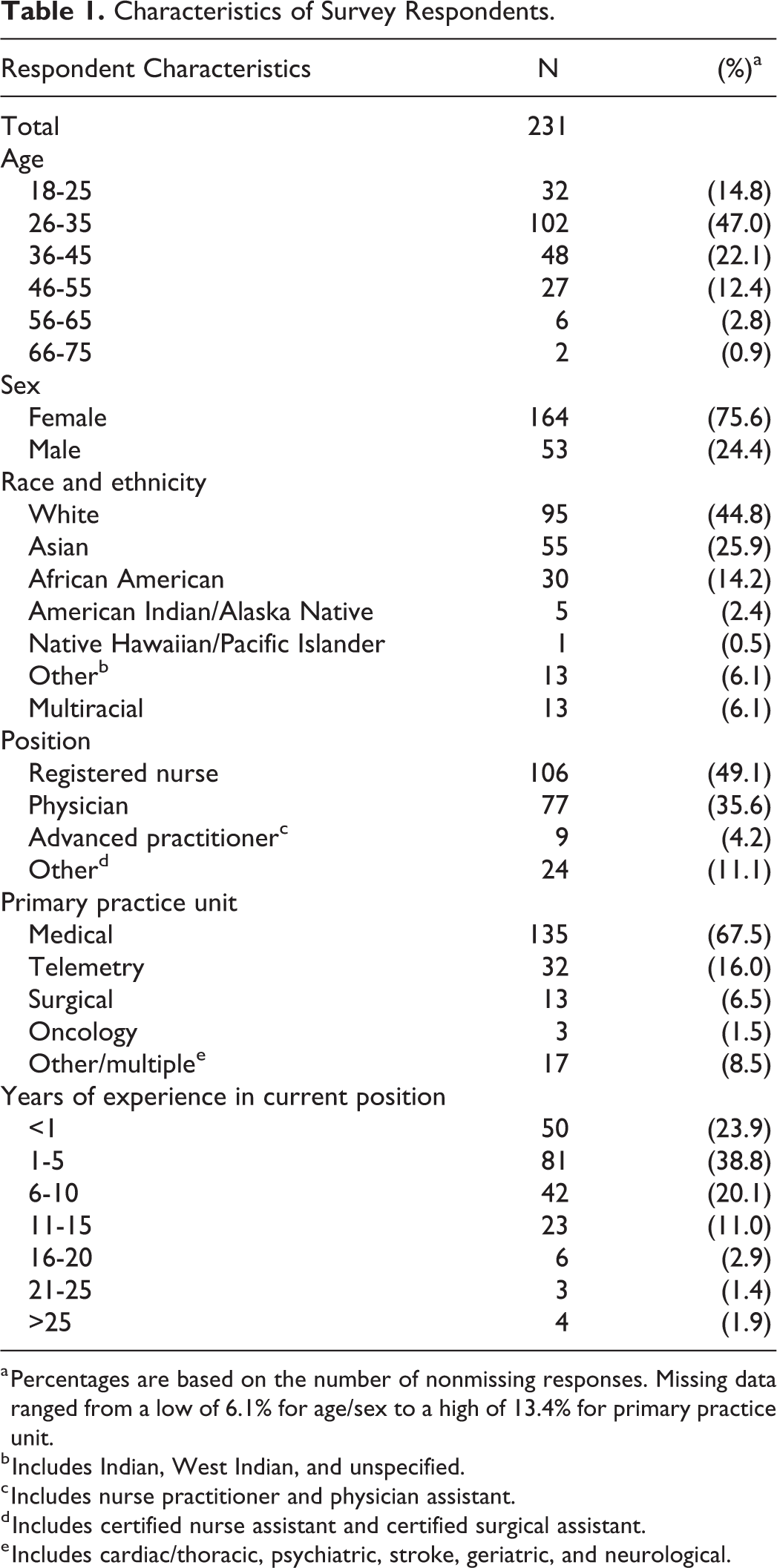
a Percentages are based on the number of nonmissing responses. Missing data ranged from a low of 6.1% for age/sex to a high of 13.4% for primary practice unit.
b Includes Indian, West Indian, and unspecified.
c Includes nurse practitioner and physician assistant.
d Includes certified nurse assistant and certified surgical assistant.
e Includes cardiac/thoracic, psychiatric, stroke, geriatric, and neurological.
Constant Observation Practices
The vast majority (84.2%) reported that at least 1 patient/wk required CO on their unit and 24.4% indicated at least 2 COs per week. Once used, most (59.9%) continued CO for “over a few days” (Table 2). The most frequent conditions that necessitated the use of CO (sometimes/often/very often) were dementia with agitation (90.2%), suicidal ideation (82.3%), and delirium (78.8%). Over three-quarters (77.2%) reported that patients most frequently requiring CO were older than 60 years and 62.3% reported most frequent CO use in patients older than 70 years (Figure 1).
Constant Observation Practices.
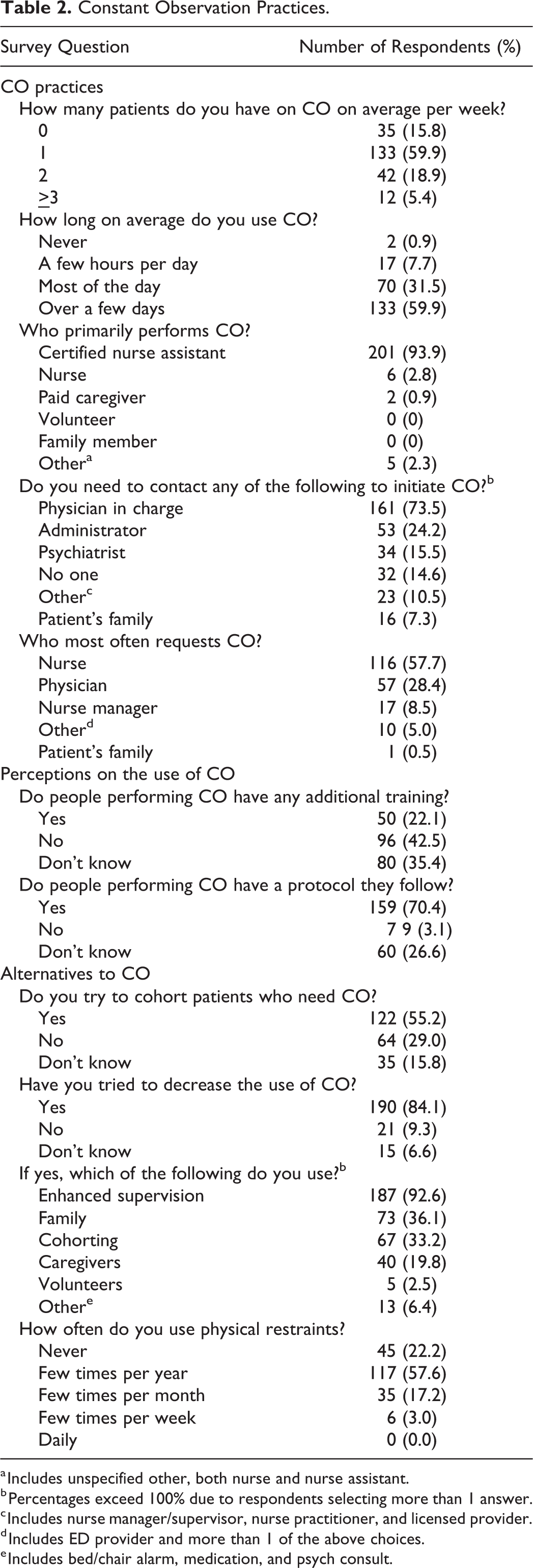
a Includes unspecified other, both nurse and nurse assistant.
b Percentages exceed 100% due to respondents selecting more than 1 answer.
c Includes nurse manager/supervisor, nurse practitioner, and licensed provider.
d Includes ED provider and more than 1 of the above choices.
e Includes bed/chair alarm, medication, and psych consult.
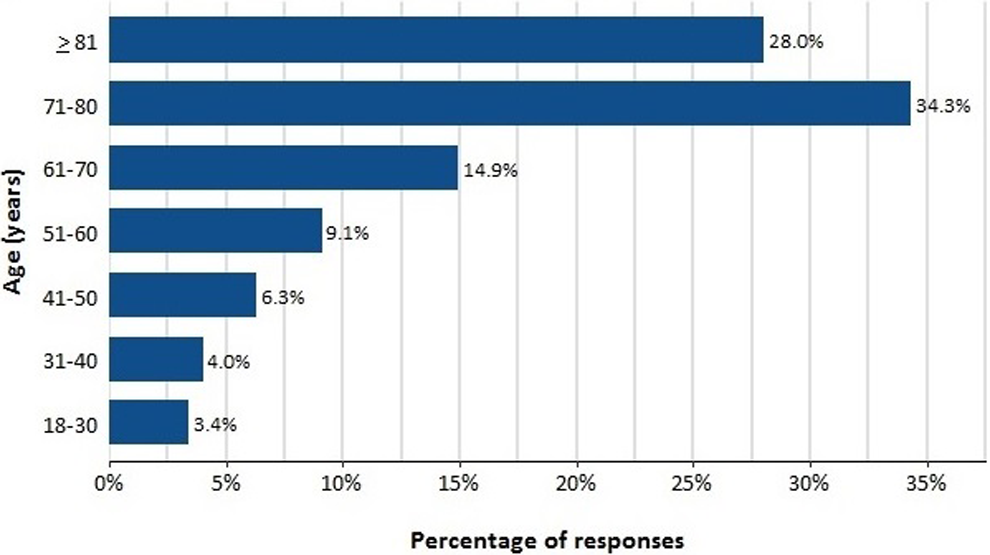
Survey question: Patients in what age category most frequently require constant observation?
Almost all (93.9%) reported that CO was most commonly performed by a nurse assistant or patient care associate, while no respondents reported use of volunteers or family members and only 0.9% (n = 2) reported a paid caregiver. In order to initiate CO, most (73.5%) stated that the physician in charge needed to be contacted, followed by an administrator (24.2%) and psychiatry (15.5%). With regard to who most often requests CO, 58.3% reported nurses, 28.6% physicians, and only 0.5% (n = 1) indicated family members (Table 2).
Provider Perceptions on the Use of CO
While 76.0% of participants indicated that CO was beneficial for patient care, 84.1% reported that they have tried to decrease the use of CO, with almost half (47.3%) reporting that they “felt pressured” to decrease the use of CO. Only 28.2% disagreed with the statement “I feel pressure to decrease use of CO.” A small minority (7.7%) intended to increase the use of CO (Table 2 and Figure 2).
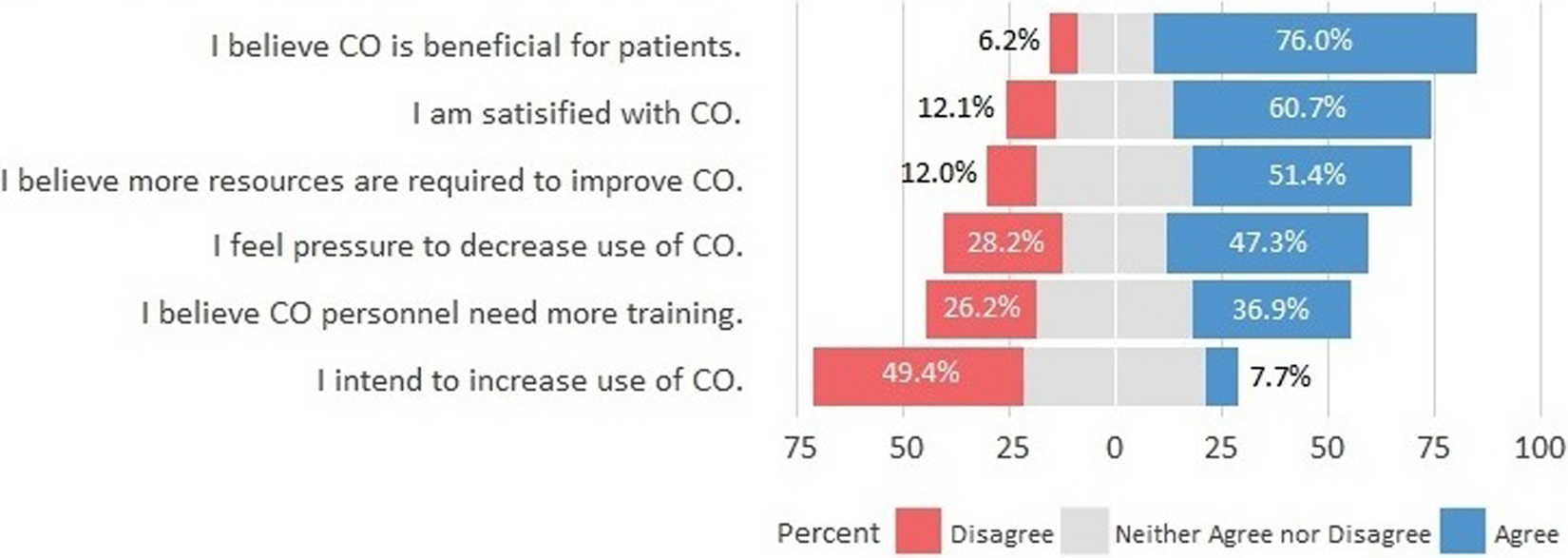
Provider perceptions on the use of constant observation.
According to respondents, only 22.1% of individuals performing CO have any formal training in managing behavioral symptoms, and 51.4% felt that more resources are required to improve CO performance in the hospital. Yet, only one-third of respondents (36.9%) reported that CO personnel do need more training.
Alternatives to CO
With regard to approaches to decrease the use of CO, almost all (92.6%) used enhanced supervision, followed by family/caregiver (55.9%) and cohorting (33.2%), while only 2.5% reported the use of volunteers. Other approaches included the use of medications and psychiatric consultation. Furthermore, the majority (77.8%) reported using physical restraints at least a few times a year and 20.2% indicated using restraints at least a few times per month or more (Table 2).
Group Comparisons
Nurses and physicians differed significantly in the frequency of CO use for several conditions, including dementia (P = .0004), delirium (P = .0132), fall prevention (P = .0089), and suicidal ideation (P = .0133); 35.7% (95% confidence interval, 26.2%-45.2%) of nurses reported CO use for dementia “often” or “very often” compared to 13.5% (5.7%-21.3%) of physicians. Nurses were also more likely than physicians to report higher frequency of CO use for fall prevention (36.3% [26.9%-45.8%] vs 20.1% [11.2%-28.8%]). Physicians were more likely to report that CO was used “often” or “very often” for delirium (47.4% [36.4%-58.5%] vs 29.3% [20.3%-39.3%] of nurses) and suicidal ideation (70.4% [60.4%-80.3%] vs 51.0% [41.3%-60.7%] of nurses; Figure 3). Nurses stated that they were more likely than physicians to request CO (73.6% vs 42.1%, respectively), while physicians reported that nurse managers (17.1% vs 1.1%) and physicians (35.5% vs 23.1%) most often request CO (P < .0001). In addition, nurses were more likely to report they believe CO is beneficial for patients (84.7% [77.7%-91.5%] vs 66.3% [56.3%-76.3%], P = .0027).
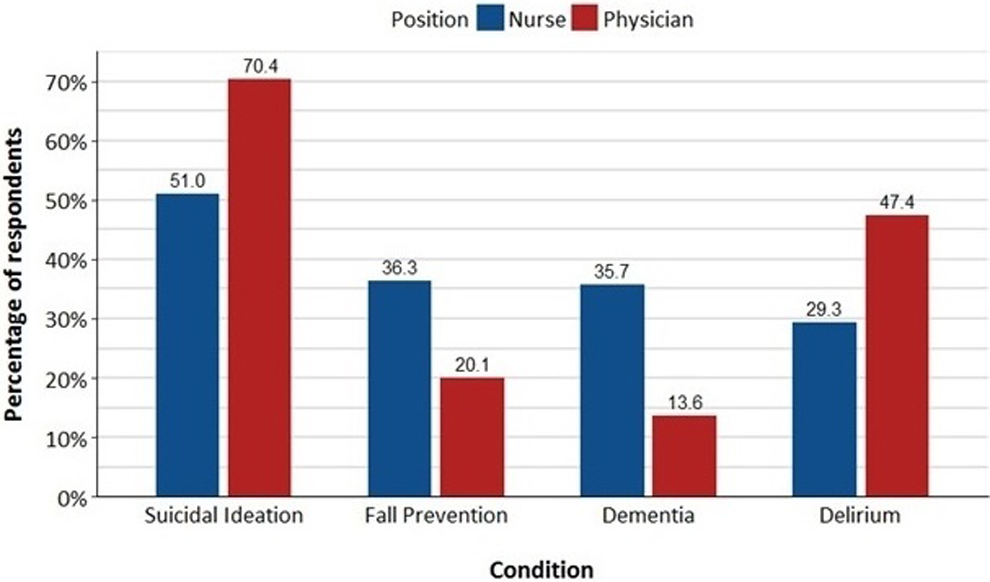
Frequency of constant observation use for selected conditions, percentage of respondents answering “often” or “very often” according to position.
Hospital comparisons revealed that there was a statistically significant difference in the conditions that more frequently required the use of CO. While the majority of respondents across all hospitals reported that CO was most frequently required for older patients (aged 71-80 or >80), 24.4% of respondents from hospital 2 reported that CO was most frequently required in 18- to 40-year-old patients, compared to 0% of respondents from the other hospitals. Hospital 2, a large tertiary hospital with a specialized medical and behavioral health unit for patients with cognitive impairment and located next to an inpatient psychiatric hospital, was less likely to report that CO was used “often” or “very often” for each of the conditions (dementia, dementia with agitation, delirium, hallucinations, and alcohol withdrawal), other than suicidal ideation, compared to the other hospitals. Lastly, respondents from hospital 3 (community hospital) were more likely to agree that additional resources are required to improve CO, as compared to the 2 tertiary hospitals. 27.3% (5.1%-15.9%) of respondents from hospital 3 agreed strongly with the statement, compared to 10.5% (5.1%-15.9%) and 8.8% (1.4%-16.1%) from the 2 tertiary hospitals.
Discussion
The frequent use of CO has major staffing and cost implications for the health-care industry, yet CO practices for older adults with cognitive impairment have been poorly described in the acute care setting. 20, 21 The present study aimed to elucidate physician and nursing practices and perceptions regarding the use of CO for older adults with cognitive impairment in the acute care setting.
In a multicenter health system, we found that the use of CO in the hospital setting is common and most frequently used for older adults with cognitive impairment who display behavioral symptoms. These findings are similar to studies from the United Kingdom that reported 25% of hospital beds are used by persons living with dementia, rising to a higher proportion on some units. 25 Another UK study found that three-quarters of hospitalized patients with dementia exhibit BPSDs and almost half (43%) had symptoms that were considered challenging by hospital staff. 22 A longitudinal cohort study, also from the United Kingdom, demonstrated that increased staffing, including the use of close supervision or one-to-one staffing, was one of the most commonly used (17%) nonpharmacological techniques for the management of patients with BPSD. 20 In addition, up to half of hospitalized older adults will develop delirium, which can often result in behavioral symptoms such as agitation, combativeness, and restlessness that require CO.
With regard to the hospital personnel who are assigned to CO, almost all nurses and physicians indicated that CO is performed by CNAs. Although CNAs receive basic training in dementia/delirium as part of the general patient care curriculum, they do not receive additional training for the management of behavioral symptoms that are commonly encountered while performing CO. This is in line with previous findings that demonstrated that only 5% of hospital personnel receive dementia training. 26 Moyle et al demonstrated that the use of staff performing CO without training in dementia care, without clear understanding of their role, and without prioritization of risk management over addressing psychosocial needs, ultimately resulted in poor outcomes for patients. 27 Indeed, 2 literature reviews on CO have emphasized the importance of role clarification and adequate staff training to optimize therapeutic potential. 6,28 Therefore, the sitter role necessitates national standardization and institutional support.
Although the use of volunteers has been well established (Hospital Elder Life Program) in the management of delirium, it was rarely reported in our study. 29 Programs using trained volunteers appear to be cost-effective; however, their national implementation rate remains low. 29,30 Our findings indicate that hospitals bear the vast responsibility for the personnel and financial aspects of providing CO.
We found that while nurses and physicians reported CO to be of benefit, the majority reported feeling pressure to decrease the use of CO. In particular, community hospitals with greater limitations in personnel were more likely to report that more resources are required to improve CO. With regard to possible interventions to reduce the use of CO, almost all reported the use of enhanced supervision, which requires less stringent practices, defined as “patients who do not require continuous observation but have evidence that they are at increased risk for falls or other types of injury.” It is thus far unclear how these practices affect patient care. In addition, the use of family/caregivers and cohorting were used to decrease the use of CO. Unit-based models of care such as acute care for elder units have shown clear benefit for older adults, albeit not those specifically with dementia, who display behavioral symptoms. 31 Other programs have used cohorting as a method to decrease CO. The specialized adult-focused environment units and delirium rooms provide a different approach, based on patient proximity to allow monitoring by nursing staff. 7,31 Another technique that respondents suggested as “other” measures used to decrease the use of CO was the use of medications. Behavioral symptoms in the hospital setting are often treated pharmacologically with antipsychotics and benzodiazepines, which are associated with adverse events and increased mortality. 20,32 –35 The survey also revealed that the use of physical restraints is frequent. 36 The use of physical and chemical restraints has not only shown to be ineffective but may result in adverse events for patients, caregivers, and staff, as well as regulatory challenges. 37,38
Interestingly, 1 of the 2 tertiary hospitals in the study has a medical and behavioral health unit for patients with psychiatric disorders as well as patients with dementia and/or delirium who display behavioral symptoms. Consistent with the unit, the use of CO in this hospital was reported to be lower overall, with more frequent use in a younger cohort. The few previous studies evaluating specialized units for the care of patients with cognitive impairment have demonstrated some positive, albeit modest outcomes. These units utilized a combination of cohorting, joint staffing by medical and mental health professionals, enhanced staff training in dementia and delirium, patient-centered care, provision of organized purposeful activity, environmental modifications, delirium prevention, and proactive caregiver engagement. 39 –44 Their lower reliance on CO suggests the advisability of a multicomponent, ecological approach to behavioral symptoms, including staff approaches wherein sitters who act soley as “observers” become “doers” who translate observations into interventions that promote function, comfort, and a sense of well-being. Further research is necessary to examine nonpharmacological approaches to manage behavioral symptoms.
This study is not without limitations. Survey items were evaluated by a multidisciplinary panel of experts including geriatricians, hospitalists, biostatisticians, and researchers to establish face and content validity. However, we did not assess other psychometric properties, including test–retest reliability and interitem reliability. Respondents were recruited from multiple sites; however, all hospitals were part of the same health system operating in the New York metropolitan area, limiting generalizability. In addition, in order to keep the survey anonymous, we did not collect unit-specific data. The nature of the design of the study meant that respondents were self-reporting and thus provided a subjective account of the use of CO. Since we did not collect information on survey nonresponders, respondents may have been a self-selecting group; thus, it is possible that those who use CO are those who are likely to respond to the survey. Lastly, follow-up questions regarding protocols/policies/cohorting with regard to CO and approaches to decrease the use of CO should be explored in future studies.
Conclusion
Our study highlights the widespread use of CO for hospitalized older adults with ADRD who display BPSD. Given the high cost and lack of national guidelines, there is an urgent need to understand, improve, and standardize the use of CO. With the unprecedented number of older patients with ADRD being admitted to acute care settings, hospitals are increasingly challenged to identify and meet their specific care needs. The need to develop alternative cost-effective, sustainable models is imperative to prevent harmful outcomes and to ensure quality care, dignity, and respect for hospitalized persons who require a higher level of observation.
Footnotes
Authors’ Note
Liron Sinvani, MD, Vidhi Patel, MPH, Shalin Shah, MD, Marie Boltz, PhD, RN, and Gisele Wolf-Klein, MD, contributed to study concept and design, acquisition of participants and/or data, analysis and interpretation of data, preparation of manuscript, and final approval of the version to be published.
Andrew Strunk, MA, and Renee Pekmezaris, PhD, contributed to study concept and design, analysis and interpretation of data, preparation of manuscript, and final approval of the version to be published.
Colm Mulvany contributed to acquisition of participants and/or data, analysis and interpretation of data, preparation of manuscript, and final approval of the version to be published.
Andrzej Kozikowski, PhD, contributed to study concept and design, interpretation of data, preparation of manuscript, and final approval of the version to be published.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.