
Abstract
Depression and anxiety are common in persons with dementia (PWD) and associated with poor outcomes. We explored frequency, pharmacologic management and mental health service use in PWD and depression symptoms with/without coexisting anxiety symptoms. The sample comprised 160 community-dwelling PWD in a trial to prevent development of aggression. Baseline data on depression and anxiety symptoms, psychotropic medications and mental health service use were examined. Regarding participants, 65 (41%) lacked clinically significant depression or anxiety symptoms, 45 (28%) had depression symptoms, 43 (27%) had depression and anxiety symptoms, and 7 (4%) had anxiety symptoms. Comorbid anxiety was associated with more severe depression symptoms. One third with depression symptoms and one half with depression and anxiety symptoms were taking an antidepressant. Mental health service use was very low, regardless of depression symptom severity or coexisting anxiety. Research needs to evaluate therapies for depressed PWD, but treatment of those with comorbid anxiety and depression is more urgent. Clinical Trial Registration for Parent Trial: ClinicalTrials.gov (NCT02380703)
Introduction
Neuropsychiatric symptoms (NPS), also known as behavioral and psychological symptoms of dementia, are signs and symptoms of disturbed perception, thought content, mood or behavior. 1 Among the most frequent NPS are depression and anxiety, along with apathy, agitation and irritability 2 -4 Depression and anxiety in dementia have been associated with patient- and caregiver-reported poorer quality of life, 2,5 -7 greater impairment in activities of daily living, 8,9 increased rates of sleep disturbance and aggression, 10 -12 increased wandering, worsened cognitive impairment, 8,9 and higher rates of institutionalization. 13,14
Depression is common in PWD, with prevalence rates ranging from 30.3-42% in 2 recent meta-analyses. 15,16 Anxiety also occurs frequently in PWD, with rates of 5-21% for anxiety disorders and 8-71% for anxiety symptoms. 15,17 -19 Measurement of depression and anxiety in dementia is complicated by factors such as symptom overlap among dementia, depression and anxiety 17 and symptom instability and fluctuation over time. 20 Deficits in memory, language, judgment and executive functioning may cause difficulty in recognition and report of these symptoms. 21 Additionally, depression and anxiety in PWD may present differently than in cognitively intact older adults. 22 Several studies have shown that PWD with depression less frequently report feelings of worthlessness, excessive guilt or sad mood but higher rates of delusions, hallucinations, weight loss and decreased appetite. 22,23 Similarly, anxiety symptoms such as excessive worry are internally expressed and may be underreported due to expressive or receptive language impairment. 17 Differences in definition, instruments and source of information may also explain the variability in prevalence rates of depression and anxiety in PWD. 24
Guidelines on the evaluation and treatment of depression and anxiety in dementia are heterogeneous, yet some recommendations are universal. Multiple guidelines recommend that PWD be evaluated and reevaluated over time for depression and other NPS. 20,25 -27 If depression or anxiety symptoms are present, treatment is warranted. 20,27 -29 Consensus remains that mild and moderate depression and anxiety should primarily be managed with psychosocial or environmental interventions when available, 20,25,30,31 with 1 aim being the avoidance of risks of psychotropic therapy in PWD. 32 Pharmacological treatment of depression in dementia has largely centered on selective serotonin reuptake inhibitors and other antidepressants; however, a recent Cochrane Review meta-analysis of 8 studies on the use of antidepressants in PWD with depression found no difference in scores on depression-symptom rating scales between antidepressant and placebo groups after 6-13 weeks. 33 Despite this finding, the study also found moderate-quality evidence that remission rates were higher in the antidepressant group than in the placebo group 33 ; and multiple guidelines continue to recommend a trial of antidepressants for the treatment of severe, persistent depressed mood in PWD. 20,27,30,31 In contrast to depression, there have been no randomized-controlled trials of pharmacotherapy for anxiety in PWD, and explicit guidelines are lacking, though some evidence supports the use of antidepressants 34 and the avoidance of benzodiazepines. 35
Compared to the literature on depression and anxiety in dementia, much less is known about the prevalence and treatment of depression with coexisting anxiety in PWD. Based on the limited available literature, prevalence rates of depression with anxiety in PWD range from 26-54%. 8,24 Specific guidelines are lacking for treating depression with coexisting anxiety in this population. This study was conducted with the goal of increasing knowledge about frequency and treatment of depression symptoms with and without coexisting anxiety symptoms in PWD living in the community.
Specifically, the aims of this study were 3-fold: To examine the frequency of depression symptoms with and without anxiety symptoms in a sample of community-dwelling PWD. To investigate pharmacologic management of depression symptoms with or without anxiety symptoms in this sample. To explore the degree of mental health service use in the clinical care of PWD with depression symptoms with or without anxiety.
Materials and Methods
This cross-sectional study (N = 160) is a subsample of baseline data for PWD enrolled in a longitudinal, randomized, controlled trial of a behavioral intervention designed to prevent the onset of aggression in PWD by addressing the management of depression, pain, and communication with their caregivers. 36 The research was approved by the Baylor College of Medicine Institutional Review Board (IRB Protocol #H-33720).
Recruitment
Participants were recruited by direct referral and by searching an administrative database of medical records of patients with a documented diagnosis of dementia, based on International Classification of Diseases, Ninth and Tenth Editions codes from 1 of 3 partner clinics (Baylor College of Medicine Geriatric Medicine Associates, Baylor College of Medicine Alzheimer’s Disease and Memory Disorders Center or Kelsey-Seybold Clinics). Potential participants underwent telephone screening to describe the study to the PWD and to obtain permission to speak to his/her caregiver. To be eligible for inclusion in the study, the PWD needed to be residing in the community (either private residence or retirement home) and to be receiving care from a family member or close friend (caregiver) at least 2 days a week for at least 8 hours per week. At screening, the PWD had to be identified as being without aggression but experiencing pain, depression symptoms or communication challenges and relationship strain between him-/herself and his/her caregiver. The PWD was also required to have mild-to-moderate dementia, based on the Functional Assessment Screening Tool (FAST) score of 6e or lower. 37,38 Patient and caregiver participants provided written informed consent.
Measures
Geriatric Depression Scale
Depression symptoms were measured using the Geriatric Depression Scale (GDS) 39 administered to the caregiver. The GDS was designed specifically to assess depression symptom severity in older adults and has been used extensively in research with seniors. 40,41 It includes 30 items with yes and no response options, with a total score ranging from 0 to 30. Scores of 10 to 19 indicate mild-to-moderate depression symptoms, and scores above 20 suggest severe depression symptoms. The measure has demonstrated good validity and reliability in participants with mild-to-moderate dementia by self-report 42 -45 and by caregiver report. 43,46 For this study, GDS scores of ≥ 10 were considered to be clinically signficant depression symptoms, with the above-mentioned score cut points defining “mild-to-moderate” and “severe” depression symptoms.
Geriatric Anxiety Inventory-Short Form
Anxiety symptoms were measured using the Geriatric Anxiety Inventory-Short Form (GAI-SF) 47 administered to the caregiver. The GAI-SF is a 5-item instrument that was created from the 20-item Geriatric Anxiety Inventory (GAI). 48 It has a response format of agree or disagree and total score range from 0 to 5, with a cut-off of 3 or higher consistent with significant anxiety symptoms. The GAI has demonstrated good validity and reliability in participants with mild-to-moderate dementia by self-report and by caregiver report. 49 The GAI-SF also has demonstrated acceptable psychometric properties in clinical older-adult groups 50 and among nursing-home residents. 51 For this study, GAI-SF scores of ≥3 (i.e. scores of 3-5) were considered to be clinically significant anxiety symptoms.
Medication use
Medication use was documented by asking the caregiver to collect the PWD’s medication bottles or a medication list. Medication names, routes, frequencies and doses were collected for psychotropic medications. All classes of psychotropic medications with the exception of anti-dementia medications were included since depression and anxiety are treated with a variety of medication classes for both Food and Drug Administration-indicated and off-label indications. Medications were classified as antipsychotics, antidepressants, anxiolytics, stimulants, or sleep medications.
Mental health services
At baseline assessment, participants and their caregivers were asked how many outpatient visits were made to mental healthcare providers, including social workers, psychiatrists, therapists and counselors in the 3 months prior to assessment. This question was designed to assess the use of available mental health services in the community.
Data Analysis Plan
Microsoft Excel and SPSS version 25.0 (SPSS Statistics, IBM, Armonk, NY) were used for all statistical analyses. Two analyses were planned. The first analysis compared participants without depression or anxiety symptoms (GDS < 10 and GAI-SF < 3), participants with depression symptoms alone (GDS ≥ 10 and GAI-SF < 3), and participants with depression and anxiety symptoms (GDS ≥ 10 and GAI-SF ≥ 3). Differences in GDS scores were evaluated using Welch’s 1-way ANOVA because the data violated the assumption of variance, as assessed by Levene’s test for equality of variance (p < 0.001). Games-Howell post hoc analyses were performed for the 3 groups. Differences in GAI score, number of medications, medication classes and number of mental health service visits were also examined. Categorical variable comparisons were made by chi-square tests for independence when appropriate. Bonferroni correction was applied due to multiple comparisons. Fisher’s exact test was used in calculations that did not meet the assumptions of the chi-square test. The second analysis involved the subsample of participants with depression symptoms (GDS ≥ 10) and compared participants with mild-to-moderate depression (GDS 10 to 19) to participants with severe depression (GDS 20 to 30). Differences in GAI-SF score, number of medications, medication classes and number of mental health services visits were also examined as in the first analysis.
Results
At the time of this cross-sectional study, 1536 persons had been screened for the longitudinal study; and 1354 persons had been excluded because they declined to participate or did not meet study enrollment criteria. Reasons for exclusion were varied and included PWD death; residence in long-term care; residence greater than 30 miles from the Texas Medical Center; FAST score > 6e; aggression at baseline; lack of pain, depression or relationship strain; status as non-English speaking; and lack of available caregiver. The study’s full inclusion and exclusion criteria can be found in the trial’s protocol at ClinicalTrials.gov (NCT02380703). There were 182 positive screens; however, 12 refused to sign a consent, and 10 dropped out of the longitudinal study. This left 160 participants with baseline data available to analyze.
Overall, the sample comprised 86 (54%) men, and included 111 (69%) Caucasians, 29 (18%) African Americans, 14 (9%) Hispanic Americans, 4 (3%) Asian Americans and 2 (1%) people of mixed ethnicity. Mean participant age was 78.5 years (SD = 9.0). Mean GDS score was 11.22 (SD = 6.16), and median GAI-SF score was 1 (IQR = 0-3). Sixty-five participants (41%) had no clinically significant depression or anxiety symptoms. Forty-five participants (28%) had depression symptoms alone, 43 participants (27%) had depression and anxiety symptoms, and 7 (4%) participants had anxiety symptoms alone. Ten (6%) participants reported at least 1 mental health service visit in the 3 months prior to study enrollment.
With respect to the first analysis, mean GDS score statistically differed for the 3 groups, Welch’s F ((2,78.96) = 146.03, p = 2.96E-27). There was an increase in mean GDS score from 6.00 ± 2.42 in participants without depression or anxiety symptoms to 12.71 ± 3.06 in participants with depression symptoms alone, and this further increased to 18.16 ± 5.30 in participants with depression and anxiety symptoms. These increases from participants without anxiety or depression symptoms to participants with depression symptoms alone (6.71, 95% CI (5.41, 8.01), p = 5.1E-9) and from participants with depression symptoms alone to participants with depression and anxiety symptoms (5.45, 95% CI (3.23, 7.67), p = 4.41E-7) were both statistically significant. Please see Table 1 for sample demographic and clinical characteristics for the first analysis.
Demographics and Clinical Characteristics (N = 160).

a Anxiety alone group shown for comparison; MHS = mental health services; IQR = interquartile range, SD = standard deviation; GDS = Geriatric Depression Scale; GAI = Geriatric Anxiety Inventory.
b GDS significantly higher in participants with depression alone than in participants without depression or anxiety (p = 5.1E-9).
c GDS significantly higher in participants with depression and anxiety than in participants with depression alone (p = 4.41E-7).
d Significantly more participants with depression and anxiety were taking antidepressant medications than in participants without depression or anxiety (p = 0.011).
The proportions of participants prescribed at least 1 psychotropic medication did not differ among the 3 groups, with 27 (42%) participants without depression or anxiety symptoms, 19 (42%) participants with depression symptoms alone, and 21 (49%) participants with depression and anxiety symptoms receiving at least 1 medication (x 2 [df = 2, N = 153] = 0.624, p = 0.732). The proportions of participants prescribed antidepressant medications did significantly differ among the 3 groups, with 15 (23%) participants without depression or anxiety symptoms, 15 (33%) participants with depression symptoms alone, and 21 (49%) participants with depression and anxiety symptoms receiving antidepressant medications (x 2 [df = 2, N = 153] = 6.473, p = 0.039). Significantly more participants with depression and anxiety symptoms were taking antidepressant medications than participants without depression or anxiety symptoms (x 2 [df = 1, N = 108] = 6.488, p = 0.011). The proportion of participants taking antipsychotics (x 2 [df = 2, N = 153] = 0.266, p = 0.875), anxiolytics (x 2 [df = 2, N = 153] = 1.538, p = 0.464) and sleep medications (x 2 [df = 2, N = 153] = 2.172, p = 0.338) did not significantly differ among the groups. There were no significant differences among numbers of mental health service visits among the 3 groups (x 2 [df = 2, N = 153] = 2.22, p = 0.33).
The second analysis compared participants with mild-to-moderate depression symptoms (n = 70) to participants with severe depression symptoms (n = 18). Of the 70 participants with mild-to-moderate depression symptoms, 44 (63%) participants reported depression symptoms alone, and 26 (37%) participants reported depression and anxiety symptoms. Of the 18 participants with severe depression symptoms, 1 (6%) participant had depression symptoms alone, and 17 (94%) participants had depression and anxiety symptoms. The proportion of participants with severe depression symptoms was significantly larger in participants with depression and anxiety symptoms than in those with depression symptoms alone (Fisher exact p = 8.8E-6). The proportion of participants that met criteria for clinically significant anxiety symptoms was significantly higher in participants with severe depression symptoms (94%) than in participants with mild-to-moderate depression symptoms (37%) (Fisher exact p = 8.8E-6). Thirty (43%) participants with mild-to-moderate depression symptoms and 10 (56%) participants with severe depression symptoms were taking at least 1 psychotropic medication. There was no significant difference in proportions between the 2 groups (x 2 [df = 1, N = 88] = 0.93, p = 0.33). The proportion of participants taking antidepressants (x 2 [df = 1, N = 88] = 2.35, p = 0.13), antipsychotics (Fisher exact p = 0.27), anxiolytics (Fisher exact p = 0.15) and sleep medications (Fisher exact p = 0.58) also did not significantly differ between groups. Participants with mild-to-moderate depression symptoms were similar to participants with severe depression symptoms with respect to mental health care service visits (Fisher exact p = 0.35). Please see Table 2 for sample demographic and clinical characteristics for the second analysis.
Comparison of Mild-to-Moderate Versus Severe Depression Symptoms (N = 88).
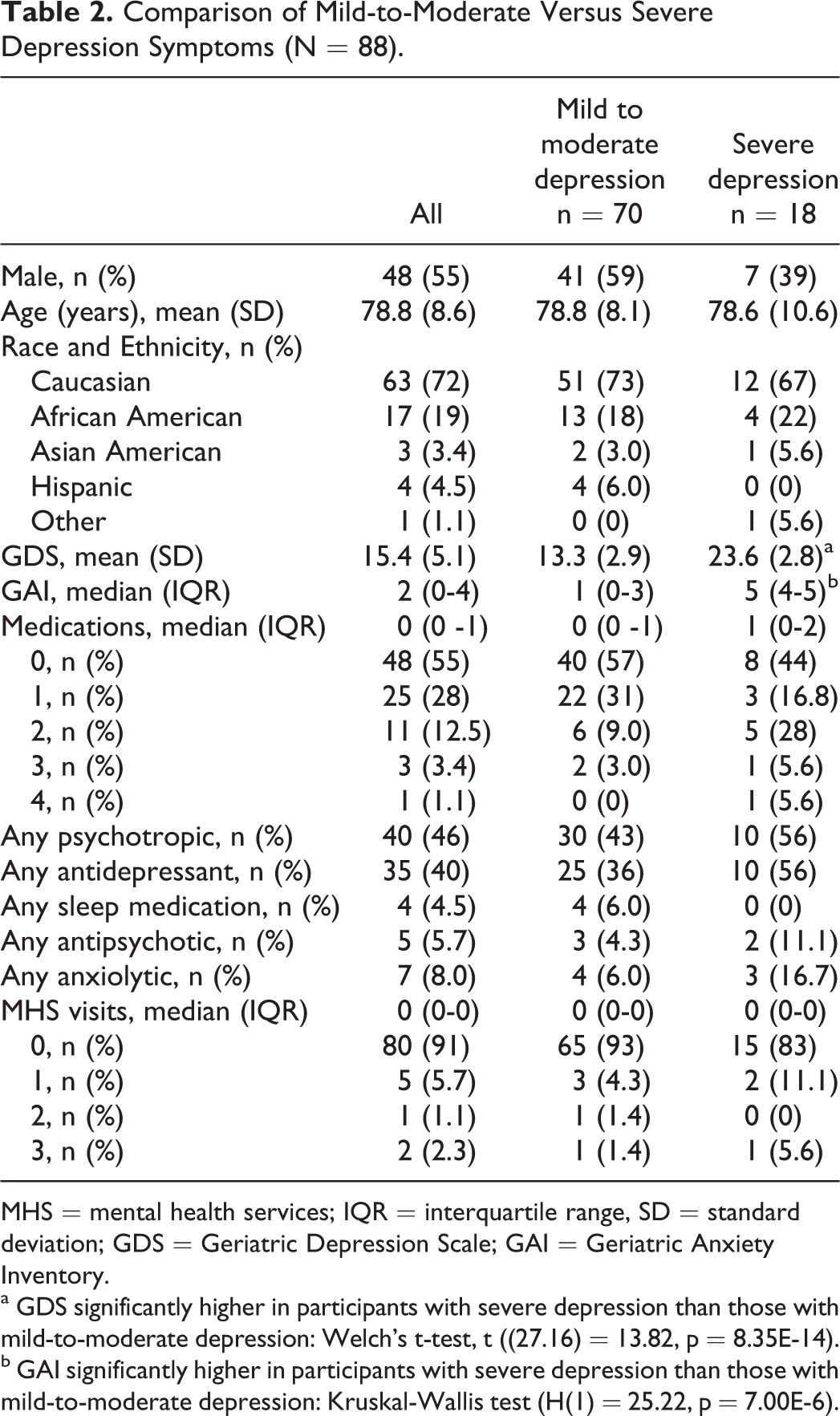
MHS = mental health services; IQR = interquartile range, SD = standard deviation; GDS = Geriatric Depression Scale; GAI = Geriatric Anxiety Inventory.
a GDS significantly higher in participants with severe depression than those with mild-to-moderate depression: Welch’s t-test, t ((27.16) = 13.82, p = 8.35E-14).
b GAI significantly higher in participants with severe depression than those with mild-to-moderate depression: Kruskal-Wallis test (H(1) = 25.22, p = 7.00E-6).
Discussion
Fifty-five percent of all participants experienced clinically significant depression symptoms in the current study. Depression symptoms were more common in this sample than in a recent systematic review and meta-analysis of 15 studies that reported 32.3% of community-dwelling older adults with dementia had coexisting depression. 16 Prior estimates of depression rates in PWD have varied extensively in studies due to different types of cognitive impairment, settings, populations and instruments used to measure depression. 9 This sample was drawn from baseline data from participants recruited on the basis of the presence of depression symptoms, pain or relationship problems. Hence, depression symptom rates would be expected to be higher in this population than in the general population of community-dwelling PWD.
More than one quarter (27%) of PWD in the total sample and nearly half (49%) of PWD with depression symptoms had clinically significant coexisting anxiety symptoms. Although few studies have examined the prevalence of depression with anxiety in community-dwelling PWD, the rate of depression symptoms with anxiety symptoms in the current study was comparable to that in the study of Teri et al (54%) in this population. 8 The GDS score was significantly higher in participants with depression and anxiety symptoms than in participants with depression symptoms alone. Ninety-four percent of participants with severe depression symptoms also had significant anxiety symptoms. These results are consistent with literature reporting that PWD with coexisting depression and anxiety have clinically and statistically higher levels of depression than individuals with depression alone. 20,24 Several studies have shown that PWD with depression with coexisting anxiety have more severe psychiatric illness and that these patients may respond more poorly to treatment than those with depression alone. PWD with depression with anxiety have increased cognitive impairment, with lower scores on visual naming and verbal fluency, increased rates of problem behaviors and more significant limitations in activities of daily living than PWD with depression alone. 8,24 Still, there remains a dearth of research conducted in PWD with depression and coexisting anxiety, despite high rates of comorbid anxiety symptoms in this study and in the literature. Future research needs to optimize care and improve clinical and treatment outcomes in these individuals.
Antidepressants were the most commonly prescribed medication class in all groups. Interestingly, severe depression symptoms were not associated with increased antidepressant use compared with mild-to-moderate depression symptoms. The finding that more severe depression symptoms are not associated with increased antidepressant use recently has been reported. 52 Participants with severe depression symptoms had similar rates of other psychotropic medication use and low rates of mental health service visits compared to participants with mild-to-moderate depression symptoms. Forty-four percent of participants with severe depression symptoms did not receive any pharmacologic treatment or attend a mental health service visit. It is unclear whether this represents lack of detection or lack of treatment; however, both have been reported in the literature, with treatment rates of depression in dementia as low as 20% to 35%. 3,53
Almost half of participants with depression symptoms with coexisting anxiety symptoms were prescribed an antidepressant medication, which is considerably higher than the 11% rate reported in a study by Starkstein et al. 24 Benzodiazepine use was less common in this study (9%) than in previous studies in community-dwelling adults with dementia (13-20%). 24,54,55 Thus, this study’s higher rate of antidepressant use in PWD with anxiety symptoms may reflect a preferential shift away from benzodiazepine anxiolytics and toward antidepressants for the treatment of anxiety in this population.
Surprisingly, no difference was found in the proportion of participants without anxiety or depression symptoms taking antidepressants (23%) compared to participants with depression symptoms alone (33%). Almost one fourth of patients without depression or anxiety symptoms were receiving antidepressant medications, a finding that may be explained by several factors. Antidepressant medications have been used to treat multiple symptoms in PWD, including depression, anxiety, agitation and sleep. 32 Hence, it is probable that some patients without depression or anxiety who were prescribed antidepressant medications were using them for other indications, such as for pain or sleep. Alternatively, these participants may have had partial or full response to an antidepressant trial and were being continued on maintenance treatment to prevent relapse, which would explain normal depression and anxiety scores. There is also the possibility that antidepressant medications are being used improperly and without indication in this sample. Literature supports this idea, with 1 study reporting that PWD not taking antidepressants had similar scores on the Neuropsychiatric Inventory as PWD prescribed antidepressants. 52 Additionally, a recent Danish study found that only 10% of PWD were on fully appropriate psychotropic medications for the treatment of NPS. 56
In addition to pharmacologic therapy, very few patients in this study reported seeing mental health providers, regardless of depression symptom severity or presence of coexisting anxiety symptoms. This finding appears consistent with available literature. For example, a nationally representative study of US adults aged greater than 70 years found that only 6.7% of PWD in the community or in long-term care had ever seen a psychiatrist. 52 In the veteran population, a recent study of mental health treatment in veterans with neurological conditions revealed that veteran participants with dementia and depression with or without anxiety had, on average only 2.42 mental health service appointments per year. 57 Given the importance of treating depression and coexisting anxiety in dementia, there is a great need to make treatment by mental health providers more available to increase access to both pharmacologic and nonpharmacologic treatments.
Limitations
Several limitations to the current study should be acknowledged. Presence of depression and anxiety symptoms were not based on structured clinical interviews but instead on GDS and GAI-SF scores, as rated by the participants’ caregivers. Utilization of a structured clinical interview would have been ideal; however, both GDS and GAI-SF have been validated in PWD and exhibit acceptable psychometric properties. 43,46,49 -51 Although validity of the GDS in participants with severe dementia has been found to be decreased, 58 this study’s enrollment criteria excluded participants with severe dementia, based on FAST score. While the GAI and GAI-SF have been found to correlate with the GDS in several studies, 49,59,60 there remains debate in the literature as to the interpretation of this finding. Several studies have felt that this correlation is evidence of low divergent validity of the measures 59 (i.e., whether the scales measure independent constructs of anxiety and depression). Indeed, with the introduction of the anxious distress specifier for major depressive disorder in DSM-5, it may be possible that only one construct is being measured. 61 Other studies have posited that the correlation is evidence of adequate convergent validity of the measures, given the high rates of comorbidity of anxiety and depression symptoms in PWD. 59,62 This correlation between anxiety and depression measures has also been reported between the CSDD and the RAID 63 and is not unique to the GDS and GAI; however, the difficulty in interpreting this correlation (i.e. decreased divergent validity versus acceptable convergent validity) can be considered a limitation of the present study.
Additionally, the sample size for the first analysis using 3 comparison groups may not have been large enough to detect small effects. Also, as previously mentioned, this study’s sample was drawn from community-dwelling older adults with dementia and either depression, pain or relationship problems. Although depression, 15,16 pain, 64 and relationship problems related to communication difficulties 65 are quite common in PWD, these findings may not generalize to the general population of community-dwelling PWDs.
Psychotropic medications have been used to treat a wide range of different NPS in PWD. Although psychotropic medications were sorted by general classes in this study, data were not collected concerning comorbid psychiatric diagnoses of the participants. Thus, exact indications for medicines reported in this study cannot be determined in this sample. Also, only 6% of participants reported seeing a mental health care provider such as psychiatrist in the 3 months prior to study enrollment; yet 44% of participants were taking psychotropic medications. Participants were recruited from 3 practices with providers trained in internal medicine, family medicine, geriatric medicine or neurology; and it is probable that these physicians were providing psychotropic prescriptions for study participants; however, no data were collected concerning name and specialty of the physicians prescribing psychotropic medications to participants in this study. Future studies would benefit from collecting these data, as it is possible that psychotropic prescribing patterns may exist, depending on provider training and specialty.
Lastly, participants were recruited based on International Classification of Diseases, Ninth and Tenth Editions codes for dementia, permitting the inclusion of individuals with a variety of neurocognitive disorders. Dementia type was not collected and, thus, did not allow comparison between frequency and severity of depressive and anxiety symptoms based on type of dementia. Previous literature has reported a higher prevalence of depressive symptoms in vascular dementia and Lewy body dementia compared to Alzheimer’s dementia. 66,67 In contrast, less data are available about the differences in prevalence rates and severity of anxiety symptoms among the different types of dementia. Future studies may benefit by examining patterns of anxiety symptomatology by dementia diagnoses (e.g. Alzheimer’s dementia, Lewy Body Dementia).
Conclusions
This study adds to the literature on the frequency, pharmacologic management and mental health service use in community-dwelling PWD with depression symptoms with and without coexisting anxiety symptoms. Additional studies need to explore the relationship between dementia with depression with coexisting anxiety and short- and long-term patient outcomes, as the literature is lacking in this area. Depression with and without anxiety is very common in PWD, but there is variable adherence to treatment guidelines. This study found potential issues both with the lack of detection and/or treatment in participants with severe depression, as well as potentially inappropriate treatment in participants prescribed antidepressants in the absence of depression and anxiety symptoms. Mental health service use is low; and there is a need for patient-, provider- and system-level interventions to facilitate access to mental health providers.
Footnotes
Abbreviations
Authors’ Note
This work was partly the result of use of resources and facilities at the Houston VA HSR&D Center for Innovations in Quality, Effectiveness and Safety (CIN13-413). The opinions expressed reflect those of the authors and not necessarily those of the Department of Veterans Affairs, the U.S. government or Baylor College of Medicine.
Acknowledgments
The authors would like to acknowledge Tracey Evans, RN, MPH; Sonora Hudson, MA; Lynn Snow, PhD; Amy Amspoker, PhD; Melinda Stanley, PhD; Jessica Freshour, PhD; and Sheila Richey, PhD; for their contributions to this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Significance Statement
Little is known about prevalence and treatment of depression with coexisting anxiety in dementia. Clinically significant anxiety symptoms occur in about half of depressed persons with dementia. One third with depression symptoms and one half with depression and anxiety symptoms were taking an antidepressant.