
Abstract
Resources for Enhancing All Caregivers Health (REACH VA) is a behavioral intervention for caregivers of individuals with dementia disseminated in the VA. Although shown to improve caregiver and care recipient outcomes, some caregivers continue to experience depression or caregiver burden following the intervention. Factors that predict symptom remission following REACH VA are unknown. The present study investigated attachment, social support, and psychopathology as predictors of symptom remission for family caregivers who completed REACH VA. Caregivers who do not remit perceive lower levels of social support from loved ones, endorse poorer attachment quality, and have more personality disorder characteristics, particularly affective instability. These factors that impair caregivers’ abilities to be effectively attuned to the needs of their care recipients and to reap benefits from a brief and focused behavioral intervention such as REACH VA. Interventions that target caregiver interpersonal functioning and emotion regulation skills may be helpful to those who do not respond to REACH VA.
Introduction
Over the last 40 years attempts have been made to develop psychosocial interventions tailored to the needs of families caring for individuals with dementia. Resources for Enhancing All Caregivers Health (REACH VA; based on the REACH II intervention model) was one of the Veterans Health Administration Caregiver Assistance Pilot Programs and the first national clinical translation of an empirically supported behavioral intervention for caregivers. 1,2 The intervention includes education, support, and skills building to help caregivers better manage stress and patient behaviors. The REACH VA has effected significant decreases in caregiver burden, depression, anxiety, number of troubling patient behaviors reported, caregiver frustrations, stress symptoms, and health-care costs for the care recipient. 3,4 However, the presence of patient nonresponse or partial response is inevitable for even the most effective psychosocial interventions. Few intervention studies publish data on nonresponse; however, for caregiver interventions generally, one found the average caregiver remained moderately depressed postintervention 5 and another indicated that rates of clinically significant depression and anxiety postintervention were nearly 50%. 6 No known literature exists on caregiver nonresponse to REACH VA.
Although few studies examine predictors of response to caregiver interventions at all, across populations, the most common predictors of nonresponse are severe psychopathology and measures of interpersonal functioning such as attachment status. 7 –9 The current study attempts to understand factors associated with symptom remission among those receiving REACH VA. We specifically tested variables associated with psychotherapy response in other populations (eg, attachment, social support, and psychopathology) and attempted to determine their generalizability for family caregivers of individuals with dementia.
Methods
Participants
Participants were referred by Veterans Affairs Medical Center (VAMC) staff in the geriatric, mental health, and primary care clinics, as well as by other participants and self-referral from flyers posted throughout the VAMC. To be eligible to participate, caregivers must be a family member of the individual with dementia devoting at least 4 hours per day to caregiving and report elevated burden (Zarit ≥ 9) or depressive symptoms (Patient Health Questionnaire [PHQ-9] ≥5). Caregivers were excluded from the study if the PWD was bedbound, or had a Mini-Mental State Examination or a St Louis University Mental Status score of 0 based on a review of the medical record.
Procedure
Participants were assessed via phone for exclusion criteria. Eligible participants were seen for an intake session, which consisted of assessments including the PHQ-9, Zarit Burden Scale (Zarit), Personality Assessment Inventory (PAI), Adult Attachment Scale, SCID-II, and Multidimensional Scale of Perceived Social Support (MSPSS) prior to their first intervention session.
Caregivers received REACH VA, a behavioral intervention focused on psychoeducation, problem-solving around typical caregiver challenges, and stress management strategies. 1,2 The intervention consisted of between 5 and 12 weekly individual sessions in person at the VAMC and/or by telephone based on caregiver preference. Interventionists for the study were either doctoral-level psychologists, postdoctoral fellows in geropsychology, or master-level psychology students under the supervision of a licensed doctoral-level psychologist. All sessions were video or audiotaped and periodically reviewed in supervision for fidelity to the protocol. All interventionists completed training and certification in the REACH VA protocol provided by the Memphis VA Medical Center where REACH VA was developed. All caregivers received a “caregiver notebook” that includes strategies to address a range of challenges faced by caregivers including wandering, agitation, sleep difficulties, depression, and so on. The content of the REACH VA intervention sessions cover the following topics: education about dementia, safety, caregiver health and stress, stress management techniques, mood management techniques, and problem-solving strategies utilizing the caregiver notebook. Upon completion of the intervention, participants were contacted by research staff either in person or by phone and given the PHQ-9, Zarit, and MSPSS.
Measures
Patient Health Questionnaire 10 consists of 9 questions based on the Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition) DSM-IV criteria for depression (range: 0-27). The PHQ-9 has been shown to correlate with the scores of the short-form BDI (r = .73; P < .0001). 7 The measure demonstrated good reliability in the current sample (α = .87).
Zarit Burden Interview 11 is a unidimensional scale of caregiver strain consisting of 12 items in which caregivers rate the degree to which they experience a statement such as “do you feel stressed between caring for your relative and trying to meet other responsibilities (work/family)?” (range: 0-48). The measure demonstrated good reliability in the current sample (α = .87).
Personality Assessment Inventory 12 is 344-item self-report inventory of adult psychopathology. The Borderline Affective Instability scale was used in our analyses that demonstrated acceptable reliability in the current sample (α = .75). The Borderline Identity Problems (BOR-I), Borderline Negative Relationships (BOR-N), and the combined Borderline Features (BOR) scales were also used in our analyses and demonstrated Cronbach α = .73, α = .62, and α = .90, respectively.
Adult Attachment Scale 13 is a 16-item measure of attachment quality. Caregivers rated their relationship on items such as the ability to seek comfort from or feelings of love or closeness to the care recipient prior to developing dementia on a 7-point Likert-type scale. The measure demonstrated excellent reliability in the current sample (α = .95).
Multidimensional Scale of Perceived Social Support 14 is a 12-item self-report measure with higher scores indicating greater perceived support. Three subscales assess support by relationship type: significant other, family, and friends. The measure demonstrated excellent reliability in the current sample (α = .94).
Structured Clinical Interview for the DSM-IV—Axis II Personality Disorders 15,16 is a clinician administered semistructured diagnostic interview that elicits information about the participant’s relationships, capacity for self-reflection, and the presence of personality disorders. Interrater reliability coefficients ranged from 0.90 to 0.98 for dimensional judgments. Internal consistency coefficients were satisfactory (0.71-0.94).
Statistical Analyses
Demographic characteristics were summarized in mean and standard deviation for continuous variables and proportions for categorical variables. Wilcoxon rank-sum test was used to assess the association between remission with continuous variables, in order to address the small sample size of this study and potential skewed distributions. Wilcoxon signed-rank test was applied to test whether a change variable was significantly different from zero. Fisher exact test was used to assess the association between categorical variables. All analyses were performed using SAS 9.4 (SAS Institute Inc, Cary, North Carolina). All P values reported were 2-sided; statistical significance was defined as P < .05.
Results
These analyses focused on the 28 caregivers who completed the intervention. Caregivers were evenly split between male and female, with a median age of 65. The majority of caregivers were a romantic partner (60.6%), followed by adult children (32.1%), and niece/nephew (7.1%). Most were Caucasian (60.7%), followed by African American (17.8%), and other (21.4%). All of the sample competed high school, 35.7% completed college, and 10.7% had a graduate degree.
In our sample, the effect sizes (Cohen d) for change in depression (PHQ-9) was −.44 (P = .03) and burden (Zarit) was −.75 (P = .004). Remission in caregiver burden was defined as Zarit <16. 17,18 Remission in depression was defined as PHQ-9 <5. 19 In our sample, 32% (n = 9) of caregivers continued to report clinically significant burden, and 43% (N = 12) reported sustained depressive symptoms following REACH VA.
Remission on the Zarit was significantly associated with total scores on the MSPSS with remitters reporting greater social support than nonremitters. Remitters reported significantly greater support on the friends and significant other scales than nonremitters. There were no significant differences by remission type on the family scale. Caregivers who remitted on the Zarit also reported significantly higher predementia attachment security to their care recipient and significantly lower PAI Borderline Affective Instability scores than nonremitters (see Table 1). The other PAI Borderline subscales and total score did not predict Zarit remission.
Differences by Caregiver Burden Remission Status.
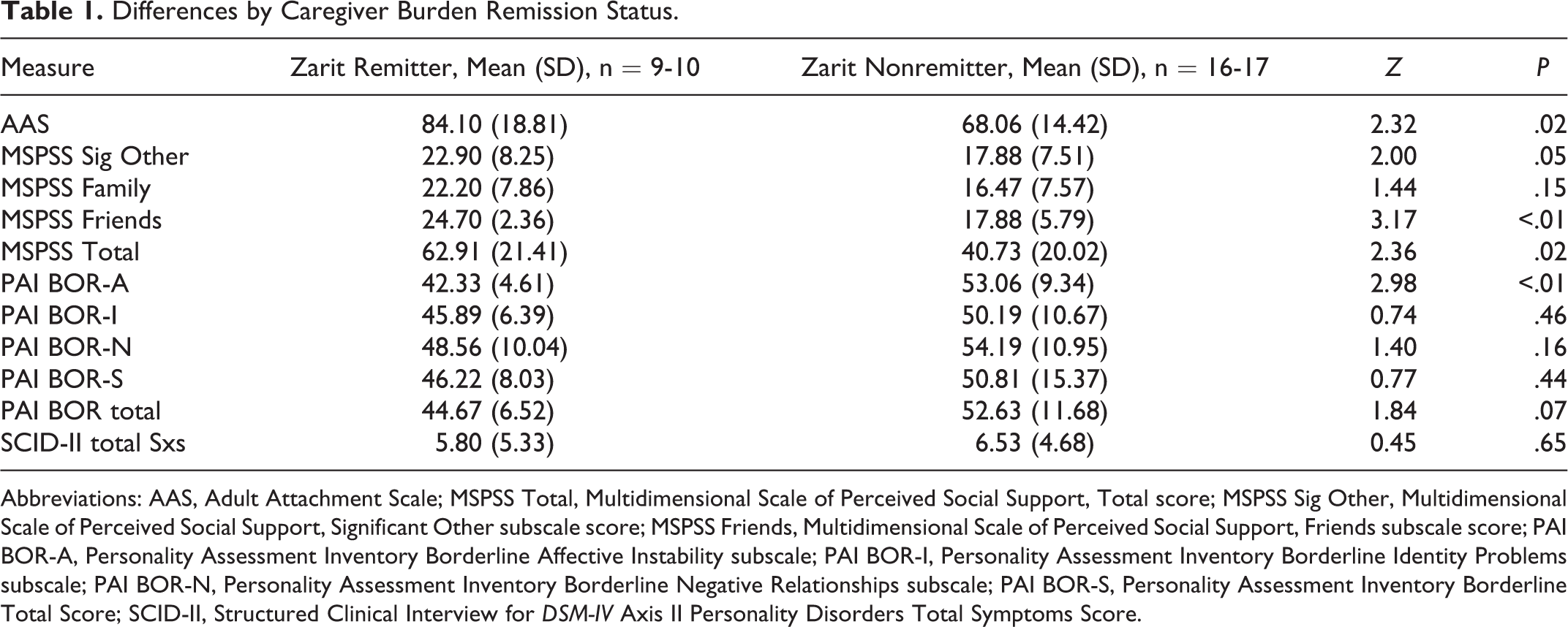
Abbreviations: AAS, Adult Attachment Scale; MSPSS Total, Multidimensional Scale of Perceived Social Support, Total score; MSPSS Sig Other, Multidimensional Scale of Perceived Social Support, Significant Other subscale score; MSPSS Friends, Multidimensional Scale of Perceived Social Support, Friends subscale score; PAI BOR-A, Personality Assessment Inventory Borderline Affective Instability subscale; PAI BOR-I, Personality Assessment Inventory Borderline Identity Problems subscale; PAI BOR-N, Personality Assessment Inventory Borderline Negative Relationships subscale; PAI BOR-S, Personality Assessment Inventory Borderline Total Score; SCID-II, Structured Clinical Interview for DSM-IV Axis II Personality Disorders Total Symptoms Score.
Remission on the PHQ-9 was significantly associated with PAI Borderline Affective Instability with remitters reporting significantly less affective instability than nonremitters. The other PAI Borderline subscales and total PAI Borderline scores did not predict remission status. The MSPSS Friends scale differed by remission status with remitters reporting greater support from friends. The MSPSS Significant Other scale also differed by remission status with remitters reporting greater support (trend level, P = .05) from a significant other than nonremitters. Finally, on the SCID-II, remission status differed by personality disorder symptoms with remitters meeting fewer criteria (trend level, P = .05) for personality disorder diagnoses than nonremitters (see Table 2).
Differences by Caregiver Depression Remission Status.
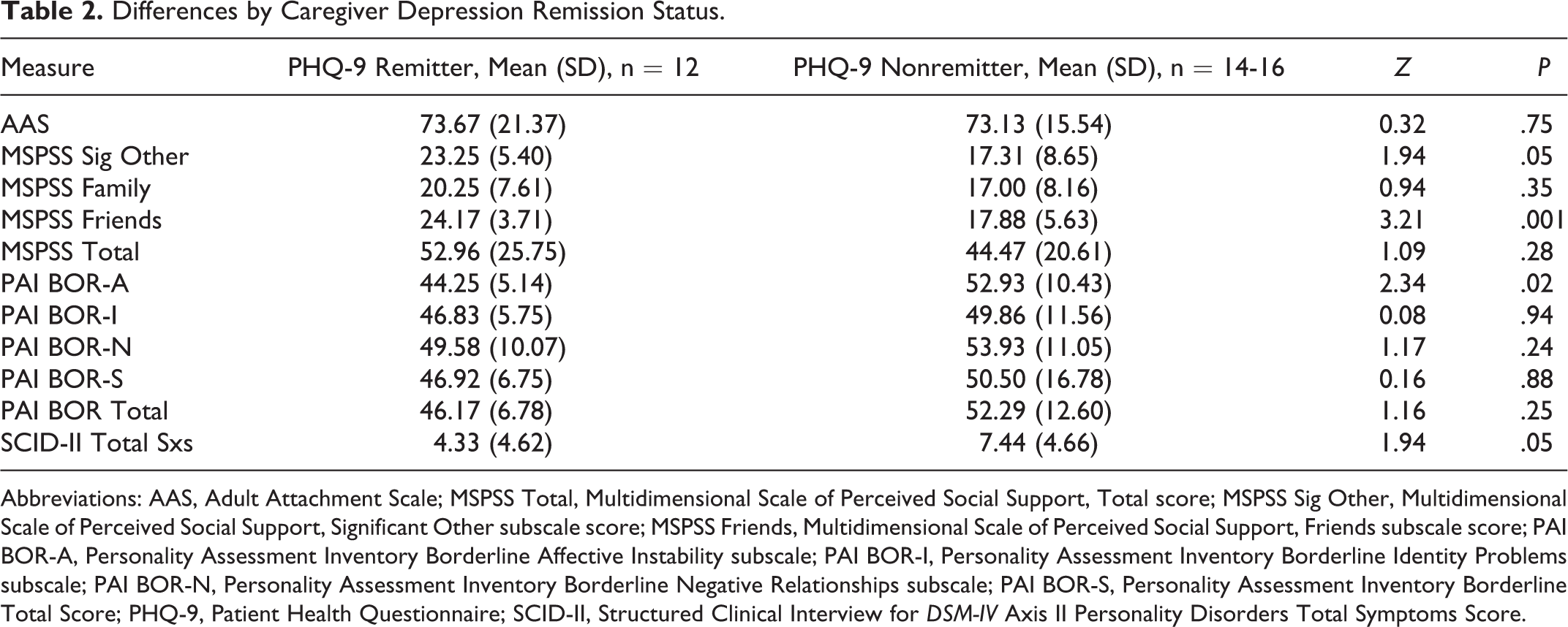
Abbreviations: AAS, Adult Attachment Scale; MSPSS Total, Multidimensional Scale of Perceived Social Support, Total score; MSPSS Sig Other, Multidimensional Scale of Perceived Social Support, Significant Other subscale score; MSPSS Friends, Multidimensional Scale of Perceived Social Support, Friends subscale score; PAI BOR-A, Personality Assessment Inventory Borderline Affective Instability subscale; PAI BOR-I, Personality Assessment Inventory Borderline Identity Problems subscale; PAI BOR-N, Personality Assessment Inventory Borderline Negative Relationships subscale; PAI BOR-S, Personality Assessment Inventory Borderline Total Score; PHQ-9, Patient Health Questionnaire; SCID-II, Structured Clinical Interview for DSM-IV Axis II Personality Disorders Total Symptoms Score.
Discussion and Implications
Given the increasing number of individuals caring for a family member with dementia, it is critical to develop strategies to support caregivers who are not helped by existing caregiver interventions. The REACH VA is among the most studied and effective caregiver interventions; however, a proportion of individuals continue to experience depression and caregiver burden following the intervention. Thus, understanding factors that predict continued symptoms may guide the development of future interventions.
Our findings provide preliminary evidence that caregivers who do not remit are more likely to perceive lower levels of social support from loved ones, specifically significant others and friends, and endorse poorer attachment quality and personality disorder characteristics, particularly affective instability.
Attachment quality, interpersonal support, and personality disorder characteristics represent aspects of caregiver interpersonal functioning and impact a caregiver’s capacity to receive and provide interpersonal support effectively. Given the impairments associated with dementia, caregiving often demands interpersonal attunement and sensitivity to effectively respond to PWD who are confused, agitated, or may have limited capacity to express their needs. Caregivers with interpersonal difficulties may find it particularly challenging to implement REACH VA’s behavioral strategies to manage difficult situations with PWD and thus reap fewer benefits.
The REACH VA encourages caregivers to seek instrumental or emotional support, as a means of reducing caregiver burden. Caregivers with larger social networks may be better able to utilize the help-seeking skills encouraged by the intervention. Additionally, those with interpersonal difficulties may struggle to implement suggestions that elicit appropriate support or decline unwelcome assistance.
Finally, caregivers’ difficulties maintaining positive relationships may generalize to their relationships with interventionists. Prior research on psychotherapy outcome has found that a positive therapeutic relationship is predictive of improved outcomes. 15 Given its focus and brief nature, REACH VA requires caregivers to prioritize and communicate their needs quickly and recognize the boundaries and limitations of both the interventionist and the intervention. Caregivers with personality pathology and emotional dysregulation may have difficulty with these interpersonal demands.
Given the current results, there may be a need for an intervention that directly targets caregivers’ interpersonal functioning and emotional regulation skills. The REACH VA addresses certain aspects of interpersonal functioning, such as encouraging social engagement as a means of self-care, and caregivers can request to focus on social difficulties or emotional dysregulation as a target problem. However, improving interpersonal relations is not the focus of the intervention, unless specifically identified by the caregiver. An intervention that emphasizes caregivers’ abilities to develop positive relationships and tolerate distressing affect may improve their ability to utilize the skills and resources offered in REACH VA.
The small sample size of this study precludes more in-depth analyses that could explore mediators and moderators of the relationship between interpersonal functioning and response to the intervention. The sample was also comprised of caregiving dyads that included a Veteran; therefore, these results may not generalize to caregiving dyads in the civilian population. Despite these limitations, the current study presents important initial evidence for factors that impact caregivers’ response to the intervention and provides a potential focus for future interventions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by VA Health Services Research and Development [CDA-210-023].