
Abstract
Background and Objectives
To assess gender differences in prevalence of neuropsychiatric symptoms (NPS) among community-dwelling Mexican Americans ≥80 years.
Research Design and Methods
Using data from Wave 7 (2010–2011) of the Hispanic Established Population for the Epidemiological Study of the Elderly, we analyzed the NPS of 914 participants as determined by the Neuropsychiatric Inventory (NPI) with assessments conducted by their caregivers. Multivariate logistic regression models were used to test the association of individual NPS with gender, adjusting for relevant characteristics.
Results
The average age of our sample was 86.1 years, and 65.3% were women. Over 60% of participants had at least one informant/caregiver reported NPS. After adjustment, women had lower odds than men of agitation/aggression but higher odds of dysphoria/depression and anxiety.
Discussion
Recognizing gender differences in NPS phenotype could help guide development of culturally appropriate NPS screening and treatment programs.
Significance Statement
Gender differences in neuropsychiatric symptoms (NPS) have not been studied among the very old from Hispanic backgrounds. Over 60% of participants in our sample of very old Mexican Americans had at least 1 NPS. Women had lower odds of agitation/aggression, but higher odds of dysphoria/depression or anxiety.
Introduction
Neuropsychiatric symptoms (NPS) are especially important to examine in the very old, those ≥80 years, 1 as NPS may be an early indication of dementia2–5 or a reflection of other underlying yet undiagnosed mental health conditions, such as major depressive disorder, schizophrenia, or substance use disorder. NPS commonly reported in neurodegenerative disorders include delusions, hallucinations, depression, anxiety, apathy, irritability, elation, disinhibition, agitation, aberrant motor behavior, appetite and eating disturbance, and nighttime behavior disturbance. 6 The Neuropsychiatric Inventory (NPI) is a widely used tool to assess behavioral symptoms commonly observed in individuals with dementia. 7
Among the very old, emergence of NPS is usually a leading indicator of underlying AD, Lewy body disease, or other related dementias. The term mild behavioral impairment was coined to reflect this phenomenology, akin to mild cognitive impairment (MCI). 8 In a study of 1998 cognitively normal AD Centers volunteers, over 59% had NPS before developing either MCI or AD. 5 Depression and irritability were the most common NPS to precede diagnosis of a cognitive disorder. 5 Among >12,000 cognitively normal participants aged 60 and older from AD Centers throughout the United States who subsequently developed dementia, 8.1% had affective (depression, anxiety, apathy) symptoms, 8.6% had agitation (disinhibition, agitation, irritability) symptoms, and 18.7% had psychotic symptoms (hallucinations, delusions). 4 While the majority of participants in population-based or clinical studies of NPS phenomenology in older adults are women, very little is known of the extent to which NPS phenotypes might differ between men and women, especially among the very old and among persons of Hispanic ethnicity, two of the fastest growing segments of the US population.
Gender differences in the prevalence of NPS have been more well documented among the young–old population than in the very old. One study of patients with AD (mean age for men: 77.2 years, mean age for women: 79.8 years) found that women had higher odds of irritability/lability compared to men. 9 Among individuals with cognitive impairment in geriatric care settings, men were more likely to exhibit aggressive and regressive behaviors, while women were more likely to exhibit depression behaviors. 10 Another study of patients (mean age for men: 79.0 years, mean age for women: 82.0 years) hospitalized with behavioral and psychosocial symptoms of dementia found that men more often exhibited aggression and women more often had delusions, hallucinations, affective disturbances, and anxieties/phobias. 11 Gender differences have not been widely studied among very old community-dwelling older adults, as most studies focus on individuals who are cognitively impaired or in clinical care settings. Given the implications of NPS for future disease and health outcomes, as well as the consequences for caregiving, a study of gender differences in NPS phenotypes in very old community-dwelling adults, both cognitively intact and impaired, is important for generating actionable data to guide caregivers and clinicians who care for the growing population of Americans aged 80 and older.
Older Hispanics represent the fastest growing segment of the older US population. The proportion of the population of US adults aged 65 and older of Hispanic ethnicity is projected grow from 8.4% in 2018 to 21.0% in 2060. 12 Mexican Americans are the largest group of Hispanic-origin adults, comprising 62% of the US Hispanic population. 13 Previous work using data from Wave 7 of the Hispanic Established Population for the Epidemiological Study of the Elderly (H-EPESE) found that a large proportion of community-dwelling Mexican Americans (mean age = 86 years) exhibit at least one NPS. 14 The most common symptoms reported were agitation/aggression, followed by dysphoria/depression and irritability/lability. 14 Another analysis, using data from Wave 9 of the H-EPESE found that among Mexican Americans aged 85 and older, most participants had at least one NPS and those with cognitive impairment more often had at least one NPS, compared to those without. 15
Hispanics may have different neuropsychiatric phenotypes compared to non-Hispanic White individuals. For example, non-Hispanic White and Hispanic populations present NPS differently prior to conversion to MCI. Among non-Hispanic White individuals, apathy was the most predictive NPS of conversion to MCI, while for Hispanic individuals, physical behaviors were most predictive. 16 Another study found that among individuals with Alzheimer’s disease, Hispanics more often exhibited apathy and anxiety, while non-Hispanic Whites more often exhibited apathy and depression. 17 Hispanics also had more NPS compared to non-Hispanic Whites. 17 Additionally, Hispanic caregivers are often unaware of NPS symptoms in their family members and are more likely to attribute such symptoms to factors other than dementia. 18 In a study of Latino caregivers, only 31% of caregivers attributed NPS to Alzheimer’s disease, with the remainder attributing them to medical, interpersonal, personality, mental, or other causes. 19 This difference is important because older Hispanics tend to receive delayed diagnosis and diagnosis at more advanced stages, compared to non-Hispanic Whites. 20
Gender differences in NPS have not been documented among Mexican Americans, especially among those aged 80 years and older. Given this gap in knowledge about community-dwelling populations and older adults of Mexican origin, the aim of this analysis was to assess gender differences in the prevalence of NPS among very old community-dwelling Mexican Americans. We hypothesize that a majority of Mexican Americans aged 80 + will have at least one NPS and participants will exhibit different NPS, by gender.
Research Design and Methods
Sample
The H-EPESE is a longitudinal study of older Mexicans aged 65 years and over who reside in the Southwestern United States. 21 The study began in 1993–1994 with 3050 individuals aged 65 and older interviewed, with follow-up interviews completed roughly every 2–3 years. At Wave 5 (2004–2005), an additional 902 Mexican American adults aged 75 years and over were added to the surviving sample. In addition to the interviews with older subjects, Wave 7 (2010–2011) included interviews with 925 caregivers/informants of the subjects, most of whom were family members. The longitudinal design of the H-EPESE has been previously described elsewhere. 22
As the presence of NPS was assessed in the informant interview, Wave 7 was used for these analyses, when the subjects were aged 80 and over. Our analytic sample included individuals who had complete data for all variables of interest (n = 914). Of these individuals, over half of both men and women had a child as their informant (63.4 and 70.5%). The remaining caregivers were spouses (men: 16.7%, women: 2.0%), other relatives (men: 13.9%, women: 18.1%), and non-relatives (men: 6.0%, women: 9.4%). Written or oral informed consent was obtained from all participants when they were interviewed, and study protocol was approved by the institutional review board at the University of Texas Medical Branch (IRB # 92-85).
Measures
Gender was our independent variable, categorized as male or female. Our dependent variable was NPS, measured with the NPI. 7 The NPI was administered to informants who were asked to assess the presence, severity, and frequency of 12 NPS in the older subjects during the past month: delusions, hallucinations, agitation/aggression, dysphoria/depression, anxiety, euphoria/elation, apathy/indifference, disinhibition, irritability/lability, aberrant motor behavior, nighttime behavioral disturbance, and appetite/eating disorders. Symptom severity was rated on a 3-point scale (1, mild; 2, moderate; and 3, severe). 7 While the NPI includes frequency, severity, and caregiver burden, we focused on frequency and severity, as we were interested in the manifestation of behavioral symptoms among older community dwelling Mexican Americans, rather than caregiver burden. Therefore, we did not use the total NPI score and instead used 1) frequency of each NPS (yes/no) regardless of severity and 2) severity (1-3) of each NPS among those who reported each symptom.
Subject and informant characteristics were included as covariates in the analysis. Subject characteristics included age, years of education, marital status (married, not married), nativity (US born, non-US born), self-rated health (excellent/good, fair/poor), activity of daily living (ADL) limitations (none, 1 or more), and cognition. Participants were categorized as having an ADL if they were unable to perform or needed help to perform one or more of the seven activities from the Katz Activity of Daily Living scale (walking across a small room, bathing, grooming, dressing, eating, transferring from a bed to a chair, and using the toilet). 23 Cognition was assessed with the Mini-Mental State Examination (MMSE) 24 or informant-reported Alzheimer’s Disease and Related Dementias (ADRD) or mental incapacitation. Participants were categorized as cognitively impaired if they scored <21 on the MMSE and reported at least one instrumental activity of daily living limitation. This cutoff has been previously used with the H-EPESE population.25,26 Those missing an MMSE score were categorized as cognitively impaired if their informant reported that they had ADRD or were mentally incapacitated. Informant characteristics included age, gender (male, female), and relationship to respondent (child, spouse, other relative, non-relative).
Statistical Analysis
Chi-square tests of Independence and analysis of variance (ANOVA) tests were used to test differences in subject and informant characteristics. Chi-square tests of Independence were then used to test gender differences in the frequency, irrespective of severity, of each NPS. For symptoms that showed a bivariate association with gender, we used multivariate logistic regression models to test the association of the presence of each individual NPS with gender. Individual models were used for each NPS, adjusting for sociodemographic, health, and informant characteristics. We also conducted a sensitivity analysis for symptom severity, among those reporting each symptom, using ANOVA tests. Stata 15.1 (StataCorp, LLC, College Station, TX) was used for all analyses.
Results
Sample Characteristics
Characteristics of Subjects in the Analytical Sample From the Hispanic Established Population for the Epidemiological Study of the Elderly, Wave 7 (2010–2011), by gender (n = 914).
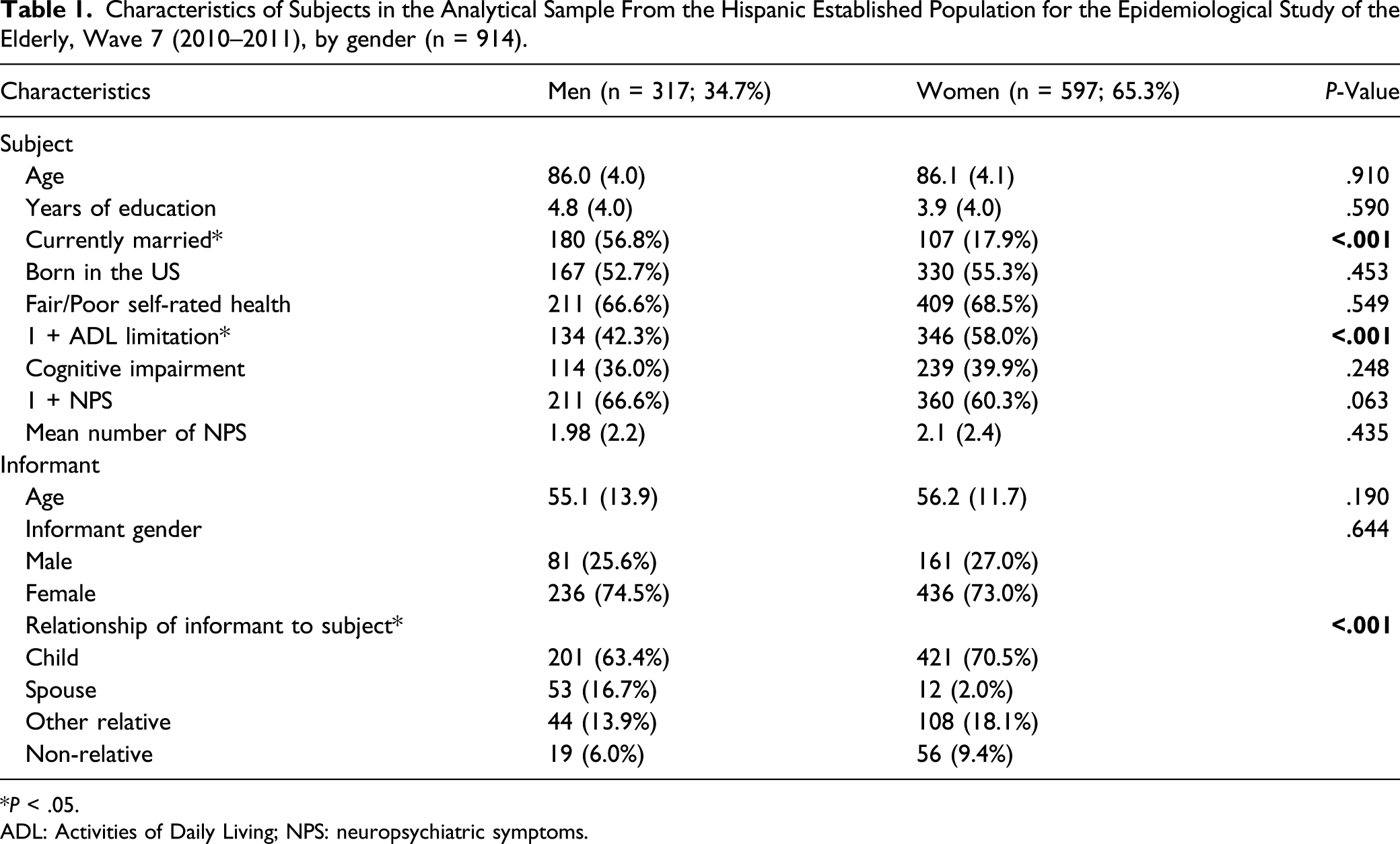
*P < .05.
ADL: Activities of Daily Living; NPS: neuropsychiatric symptoms.
Frequency of Neuropsychiatric Symptoms
Among men, agitation/aggression was the most common symptom reported, while among women, dysphoria/depression was the most common (Figure 1). Women had anxiety and hallucinations more frequently than men. The remaining symptoms did not differ by gender. Both men and women often reported irritability, in addition to apathy/indifference, nighttime behavioral disturbance, and appetite disorders. Less frequent symptoms included disinhibition and delusions. For both genders, the least frequent symptom was euphoria/elation. In adjusted analyses, women had lower odds of agitation/aggression but higher odds of dysphoria/depression or anxiety, compared to men (Table 2). Odds of hallucinations did not differ by gender. Frequency of neuropsychiatric symptoms, by gender (n = 914). *P < .05. Odds of Informant-Reported Hallucinations, Agitation/Aggression, Dysphoria/Depression, and Anxiety, by Gender (ref: men), Adjusted for Sociodemographic and Informant Characteristics (n = 914). *P < .05. Depicts odds ratios from separate multivariate logistic models with gender as the independent variable and each neuropsychiatric symptom as the dependent variable. Individual models were used for neuropsychiatric symptoms, adjusting for subject’s age, education, marital status, nativity, self-rated health, ADL limitations, and cognition and informant’s age, gender, and relationship to respondent. OR: odds ratio; CI: Confidence Interval; ADL: Activities of Daily Living.

Sensitivity Analyses
Differences in Severity (1–3), by Gender, Among Participants with Each Informant-Reported Neuropsychiatric Symptom.

*P < .05.
SD: standard deviation.
Discussion and Implications
In this study of community-dwelling Mexican Americans aged 80 and older, we assessed gender differences in the prevalence of NPS. Men were much more likely to be currently married compared to very old women (56.8 vs 17.9%) and were considerably more likely than women to have a spouse as an informant/caregiver. Over half (60%) of our participants had at least one informant-reported NPS. Last, in our adjusted analyses, men had higher odds of informant-reported agitation and aggression, while women had higher odds of depression or anxiety.
The high frequency of NPS may be due to the advanced age of the sample, with an average age of about 86.1 years. About 38.6% of our sample had cognitive impairment; however, cognitive status was controlled for in-adjusted analyses of the presence of NPS symptoms. The rate of NPS is fairly high compared to previous work. One study, among adults aged 70 and older, found that 25% of participants with normal cognition and 50% of those with MCI had at least one NPS; 27 however, this study did not report on race or ethnicity of subjects. Additionally, their sample had more years of education than our sample, with a median of 13 years for those with normal cognition and 12 years for those with MCI. 27 The prevalence of at least one NPS observed in our study may be higher than that of Geda et al., 27 but it is also lower than past studies of NPS among diverse older adults with dementia. Lyketsos and colleagues 28 noted a prevalence of at least one NPS ranging from 50% of participants with MCI participants to 80% of participants dementia. Their sample, aged 65 and older, was younger than our sample and was mostly White and female. The inclusion of individuals with both normal cognition and those with cognitive impairment may be why we noted a prevalence between the prevalence’s documented for individuals with MCI and dementia reported in previous studies.
Agitation/aggression was one of the most frequent symptoms reported for both men (37.5%) and women (28.0%) older participants in our sample. Consistent with previous work, 10 in adjusted analyses, men had higher odds of agitation/aggression. Lövheim and colleagues included in their study individuals in geriatric care settings, while our analyses included only community-dwelling older adults. This high prevalence suggests that agitation may present early and before any cognitive decline occurs. This result is concerning, as agitation is the most distressing symptom for caregivers 29 and may potentially contribute to future poor outcomes for them. Additionally, agitation is one of the NPS which commonly precedes dementia. 4
Depression/dysphoria was the most common symptom among women (32.3%). Similar to Kitamura and colleagues, 11 who found that women were more likely than men to have affective disturbances, women in our sample more often had depression or anxiety, compared to men. Again, Kitamura and colleagues examined patients who were hospitalized with behavioral and psychological manifestations of dementia, 11 while we included individuals in the community, suggesting that these affective disorders may already be present prior to impairment, and might serve as an early marker for intervention. Additionally, we did not note any gender differences in severity of NPS, except for anxiety, with severity being higher among women. This was in contrast to previous work among individuals with amnestic MCI and mild Alzheimer’s disease, which found that women present more severe delusions, while men present more severe irritability; differences in anxiety severity were not noted. 30 This difference may be attributable to our inclusion of individuals with normal cognition in our analyses.
Previous research among Hispanics has shown that the presence of NPS is related to caregiver depressive symptoms. NPS are associated with higher levels of depression among caregivers of older Hispanics with cognitive impairment, as well as of those with dementia. 31 Likewise, caregivers of older Mexican American adults report higher levels of depressive symptoms when caring for older adults who have NPS. 32 Our research adds to this literature by revealing different potential sources of stress of caregivers of older Mexican Americans. While men are more likely to have informant-reported agitation, the most distressing symptom for caregivers, women were more likely to have informant-reported depression or anxiety. This knowledge can help clinicians better treat their older Mexican American patients by specifically asking for the presence of likely NPS, as well as inquiring about the presence of caregiver stress.
As previously stated, these findings may have clinical implications. NPS are an important and potentially modifiable contributor to caregiver stress, depression, and burnout, all factors known to increase the risk of institutionalization of their older care recipients. As NPS are a precursor to cognitive impairment, the high frequency in this population is concerning and underscores the need for clinicians to ask about the presence of NPS in their very old Mexican American patients.
Limitations
This analysis has a few limitations. There is the potential for survival selection bias, as our sample is composed of older adults who survived to 80 years and older. Additionally, we do not have information on clinical diagnosis. We were unable to assess time spent caregiving, which may affect the recognition of the presence and severity of NPS exhibited by the older participants, as caregivers who spend more time caregiving may have a better recognition of the presence and severity of NPS in the care recipient compared to those who spend less time with their care recipient. It is important to note that we use the word “gender” to capture both the biological construct of “sex” and the social construct of “gender,” 33 as the H-EPESE did not collect data on gender identities. Despite limitations, this analysis adds to the literature on gender differences in NPS, using a representative sample of community-dwelling very old Mexican Americans residing in the Southwestern United States, unlike prior studies which took place in clinical setting among patients already diagnosed with AD and other dementias.9–11,34
Conclusions
In our sample of community-dwelling very old Mexican Americans, over 60% of both men and women had at least NPS. Women had lower odds of agitation/aggression, but higher odds of dysphoria/depression or anxiety. Future studies are needed to understand how the presence of symptoms may influence future cognitive outcomes among older Mexican Americans and the effect of gender on these outcomes. Another important area of study is how gender, nativity, and age at migration interact to affect the presence of NPS and changes in cognition over time.
Footnotes
Acknowledgments
We thank Sarah Toombs Smith, PhD, Science Editor and Assistant Professor in the Sealy Center on Aging, University of Texas Medical Branch at Galveston, for providing editorial assistance in manuscript preparation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Milani is supported by a research career development award (K12HD052023: Building Interdisciplinary Research Careers in Women’s Health Program-BIRCWH; Berenson, PI) from the National Institutes of Health/Office of the Director (OD)/National Institute of Allergy and Infectious Diseases (NIAID), and Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD). Dr Cantu is supported by the training grant T32AG000270 (PI Wong, PI) from the National Institute on Aging/National Institutes of Health. The Hispanic Established Populations for Epidemiological Studies of the Elderly (H-EPESE) is funded by the National Institutes of Health, National Institute on Aging (R01AG10939; Markides, PI). Drs. Kuo and Raji are supported by the National Institute on Drug Abuse (R01‐DA039192; Kuo, Raji, MPI). This work was also supported by the Texas Resource Center on Minority Aging (P30AG059301, Markides, PI) and the Claude D. Pepper Older Americans Independence Center (P30AG024832, Volpi, PI). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.