
Abstract
This study reports on the first phase of an investigation aimed at adapting The Savvy Caregiver program, a successful family caregiving curriculum developed in the United States, for application in South India. Thirty family members caring for a person with dementia were interviewed regarding their experiences as caregivers (CGs). Qualitative interviews were conducted with the family member at a geriatric clinic, while other diagnostic procedures were being carried out with the person with dementia. Findings from the study revealed that although family members understood the term CG, none could identify a word for CG in his or her language. There was little understanding of dementia as an illness. Family CGs reported feeling distressed, overwhelmed, and frustrated with caregiving. Caregivers were interested in an educational program, but many had unrealistic expectations for what they wanted to learn. The findings provide directions for adapting The Savvy Caregiver curriculum for Indian family CGs.
Over the past 20 years, a compelling picture has emerged regarding the role family members in North America, Europe, and East Asia play (and the price they pay) in providing care for their community-dwelling elders affected with dementing disorders such as Alzheimer’s disease. An equally robust literature portrays a wide variety of interventions that have been demonstrated to support the work and ameliorate the distress of these family members, these caregivers (CGs), as they have come to be known. Much less has been written—or is known—about the care that families from low- and middle-income countries (LMICs) provide for relatives affected with dementing disorders. However, about two-thirds of all cases of dementing disorders occur in these LMICs. Moreover, as development continues in these countries and their populations age, dementing disorders will become more prevalent. 1,2 This article reports on the preliminary activities of a collaborative effort to identify and attend to the needs of dementia family CGs in a setting—South India—where demography has not produced widespread knowledge and awareness about dementing diseases in the general population.
Introduction
India, one of the fastest developing countries in the world, is the second most populous country (approximately 1.2 billion people) with the fourth largest economy in the world in terms of purchasing power parity gross domestic product. 3 According to the United Nations Population Division of the Department of Economic and Social Affairs, the number of people aged 60 and older in India is approaching 104 million. 4 This age-group represented only 8.3% of the population in 2013, but with improved health and increased longevity, the proportion of elderly individuals in India is expected to rise dramatically in the coming decades. The aging of the population is associated with an upsurge in dementia. For each increment of 5 years of age, the number of persons with dementia doubles. As a result, India will face one of the largest populations of elderly individuals with dementia. Currently, it is estimated that 3.7 million Indian persons aged older than 60 will have dementia (2.1 million women and 1.5 million men). 5 By 2050 that number is predicted to increase to14.3 million. 5 Despite impressive economic gains, India faces basic health care problems such as access to health care services and information, including an absence of supportive health and welfare services for people afflicted with Alzheimer’s disease. 6 The public health sector in India has focused on preventive and curative child and maternal health issues, so this projected growth in the aged population and population with dementia threatens to overwhelm the resources of governments, service providers, and CGs. 7 -9 The family remains the principal source of care for the frail elderly individuals in India, despite several trends weakening India’s historic safety net, the joint family system. 5,10
Family caregiving for dementia is a well-recognized health and social issue in the United States. Extensive research has been done on caregiving and its impact within Western populations. The extent and magnitude of community-based dementia family caregiving in the United States is well known as is the physical, emotional, social, familial, and economic toll this work exacts from CGs. 11 -17
Likewise, over the past decade, a number of interventions have been shown, in clinical trials, to be effective in reducing or ameliorating dementia family CG distress. These interventions have employed diverse strategies. Several interventions involved home-based components including in-home, one-on-one assessment, consultation, and coaching by nurses 18 ; in-home family therapy sessions 19 ; and a home-and community-based educational and support program. 20 Other interventions consisted of combined group and individual counseling with education, 21 group-based psychoeducation, 22,23 classes on cognitive behavioral therapy, 24 and a self-care skill building, self-efficacy enhancing, community-based program. 25 A number strategies have been translated into effective interventions. In one instance, The Savvy Caregiver program 23 was transformed into a transportable, manualized psychoeducational program able to be offered by a wide variety of sponsoring organizations 26 ; this program has been shown (in a controlled trial) to reduce CG distress. 27 The project on which this article reports represents an effort to transform this successful transportable program into a curriculum that would be useful to and suitable for dementia family CGs in South India. The Savvy Caregiver program was chosen, in part, because the Fogarty International Research Collaboration Award (FIRCA), the project funding source, stipulated that the lead US researcher (KH) must be a principal investigator on an National Institutes of Health research grant and that the proposed research should be an extension or a new direction of the parent grant. The Savvy Caregiver program was a product of the research funded by the parent grant.
Based on our preliminary discussions, we began with the premise that dementia caregiving is functionally equivalent between United States and India but that substantial cultural differences call into question the conceptual equivalence of caregiving. 28 -31 It seemed likely that persons who care for their demented family members in both cultures perform roughly the same kinds of caregiving work. What was less clear, however, was the extent to which the meaning and impact of caregiving are the same across cultures.
Methods
Supported by a FIRCA funded through the National Institute of Nursing Research, a team was formed between researchers in the United States and Bangalore, India. The US team involved nurses and a gerontologist from Metropolitan State University (St Paul, Minnesota), Emory University (Atlanta, Georgia), and The University at Buffalo (Buffalo, New York); the Bangalore team involved a psychiatrist, a psychologist, and a psychiatric social workers from the National Institute of Mental Health and Neurosciences (NIMHANS). The project is proceeding in 3 phases, namely, needs assessment and curriculum development, pilot testing and program revision, and field testing. All phases of the project are being conducted under the auspices of the institutional review board at Metropolitan State University and in collaboration with the human subjects review board at NIMHANS.
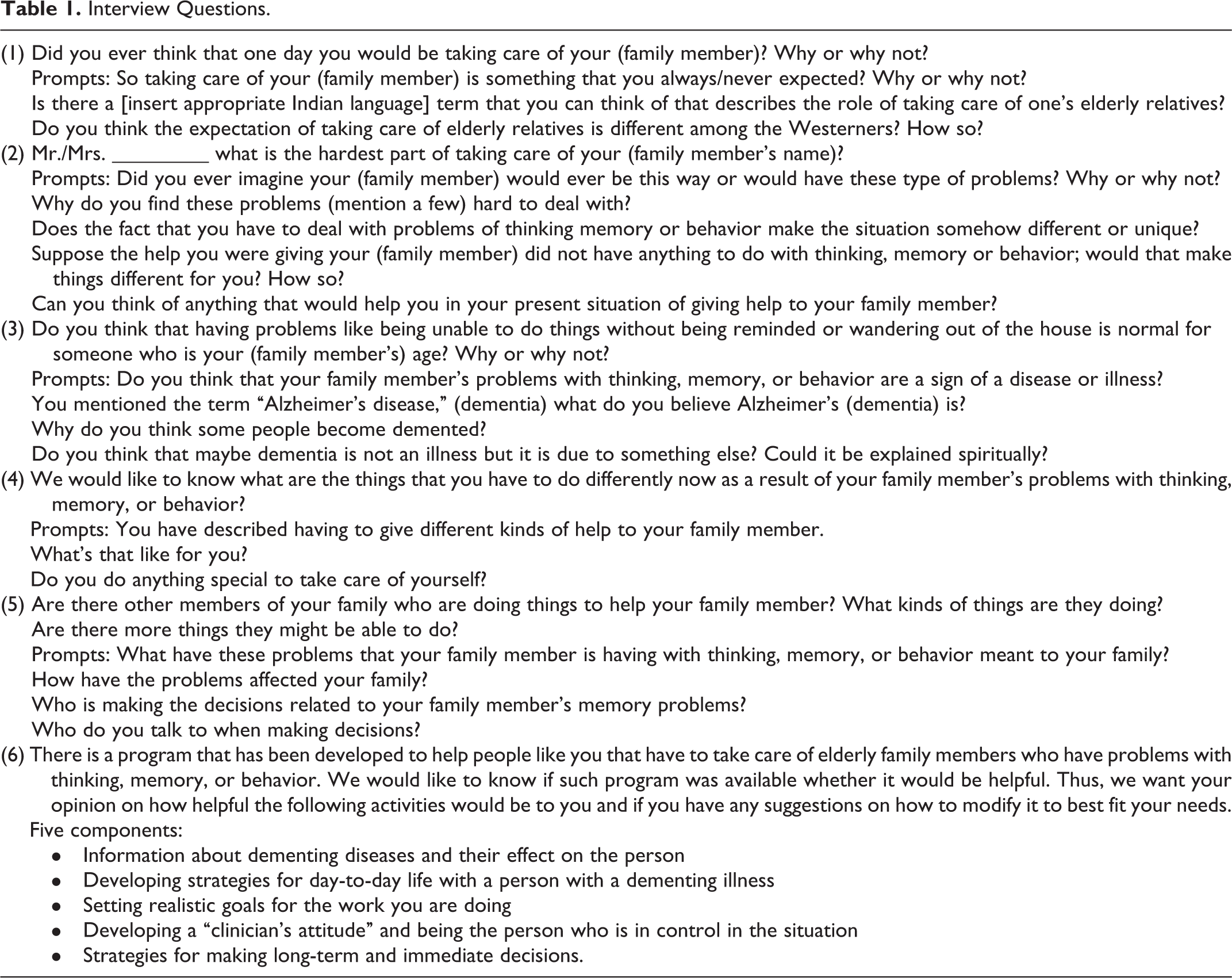
The first phase of the project—the subject of this report—centered on a series of semistructured interviews with dementia family CGs in Bangalore. The script for the interviews was developed by the partners in 2 ways. First, the content and curriculum of the Savvy Caregiver was reviewed by the Bangalore team to assess its face validity for Indian CGs. This assessment was conducted both through e-mail dialogue and during visits to Bangalore by 2 of the US collaborators (KH and SN). The Savvy Caregiver curriculum seeks to enhance the knowledge, skills, and attitude of family CGs to enable them to better perform the work of their caregiving roles. The curriculum provides information about the progressive effect of dementing disorders on the thinking, feeling, behaving, and performing abilities of the affected person. The program emphasizes the development of caregiving strategies that are tailored to the person and his or her disease stage and that are aimed at keeping the person comfortably occupied throughout the day. The program takes the tack that caregiving is an acquired role that includes a large clinical component and that the role skills can be learned and strengthened through the coaching that goes on in the program. Given the principles undergirding the Savvy program, one main interest of the interviews concerned the extent to which key principles (eg, caregiving as “role,” the clinical nature of caregiving, the need for and utility of caregiving strategies) would be comfortable for, endorsed by, and culturally appropriate for Indian family members. The second source of interview items was the e-mail and in-person dialogue of the partners: What did we feel we would want to know from CGs to help us design a program. As a result of this process, a 6-item semistructured interview guide was produced (see Table 1).
Interview Questions.
The sample for the study comprised family CGs of patients attending the NIMHANS Geropsychiatry Clinic led by the principal Indian partner (MV). The clinic is a major dementia diagnostic center in South India and beyond; it also provides ongoing care consultation for patients and education for family members. This outpatient clinic meets for about 4 hours every Saturday, and at present, approximately 5 to 7 new patients are seen for a comprehensive evaluation and 40 to 50 patients are seen for follow-up. In addition, the clinic also runs daily outpatient department screening for about 10 to 20 elders for geropsychiatric problems.
All interviews were conducted by a clinical psychologist (IP) under the supervision of MV. The interviews lasted 30 to 40 minutes and were conducted with individual family members, while other diagnostic procedures were being done with the person having dementia. Usually, these involved just 1 family member, but occasionally 2 members of the same family took part at the same time. The majority of the interviews were conducted in either Kannada or English and the remainder in other Indian languages. The interviews were audio-tape recorded and transcribed and then the interviewer translated them into English for review by the US and Indian partners.
For this report, the transcripts were read repeatedly by the members of the US team (RB, KH, ML, and SN), using the method of constant comparative analysis. 32 In this method, themes are identified from the discourse of the interviewees. As similarities are discovered among statements by those interviewed, the team’s understanding of the statements is expressed by a developing set of terms used to code the statements. Likewise, as the coding of themes continues, linkages among certain themes or codes begin to be understood in terms of broader categories. Independent reading of the interviews—and the subsequent independent development of codes and categories by the individual readers—provides the basis for team dialogue about themes and categories. Through this dialogue, consensus emerges in the form of a code book that defines codes (and provides examples from the transcripts) and categories. The final step of the process entails a second independent rereading of a sample of the interviews, a comparison of coding results, and an adjudication of any coding disputes by the larger team. The second reading of the transcripts was conducted by 2 team members (RB and KH) to enhance trustworthiness. Only a very small number of divergent codings were noted and were readily resolved either by discussion or by consultation with the other team members.
Results
A total of 30 interviews were analyzed. In 1 interview a son, the primary CG, and a daughter participated in answering the questions. Half (n = 15) of the interviews were conducted in Kannada, 43.3% (n = 13) in English, 1 in English and Bengali, and 1 in Malayalam. Table 2 provides demographic information about those interviewed. Two-thirds of the sample was female and 90% of the sample was married. Most CGs were either spouses (53.3%) or children (33.3%). The remaining CGs were daughters-in-law and a niece related to the care recipient (CR) by marriage. The majority of the CGs were older than 40 years of age with a mean age of 51.3 years (standard deviation = 14.6 years). Seventy percent of the CGs had attained a high school education. Half of the CGs were classified as middle income, a third as low income, and 16.7% as upper income. The vast majority (83.3%) of CGs resided with the CR. Two-thirds of the CGs lived in urban settings, while one-third lived in rural areas.
Caregiver and Care Recipient Demographic Information.
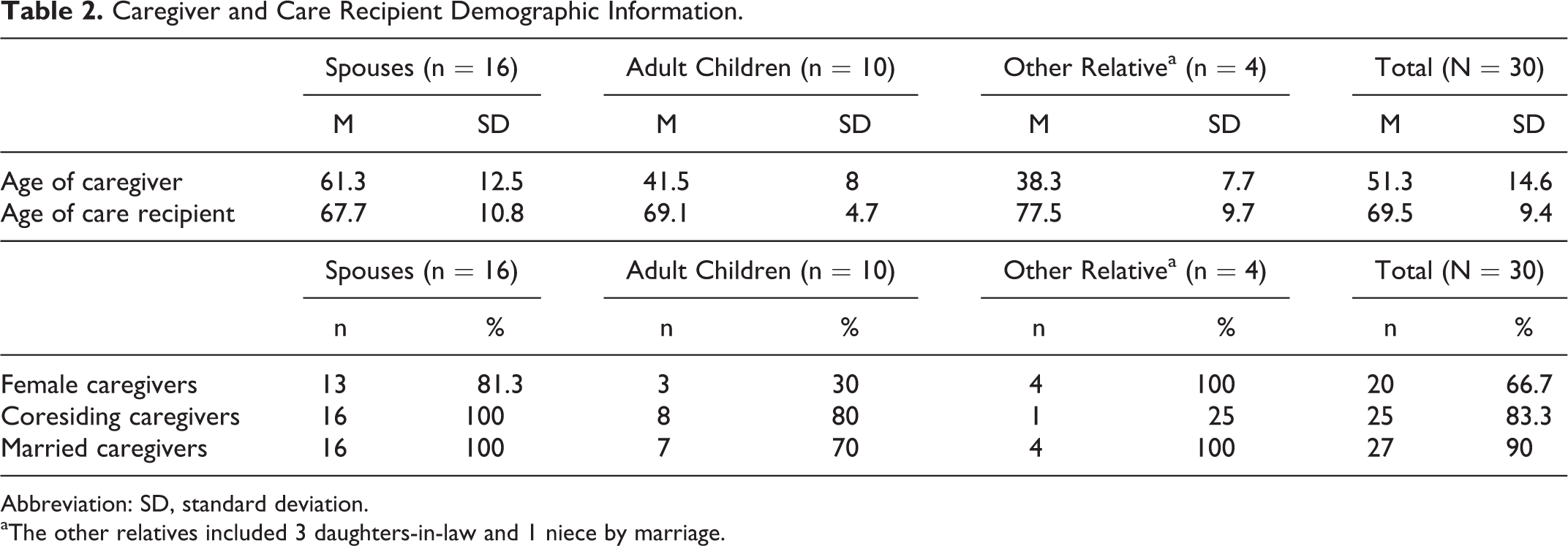
Abbreviation: SD, standard deviation.
aThe other relatives included 3 daughters-in-law and 1 niece by marriage.
Key Coding Categories and Codes
Seven categories emerged from analysis of the interview data, namely, (a) dementia knowledge, (b) caregiving activities, (c) caregiving difficulties, (d) CG as a concept, (e) caregiving roles, (f) what CGs want to know, and (g) feedback on program components. Refinement of the categories resulted in the identification of 2 or more codes for most of the categories. In particular, the codes within the category of dementia knowledge together with the demographic variables of gender and CG relationship were useful in elucidating patterns associated with CGs’ expressed caregiving difficulties. Verbatim excerpts from CG interviews are included under each category.
Dementia knowledge
Perhaps the most striking finding from the interviews was the very wide divergence of knowledge and understanding of dementia among the CGs. One interview question directly inquired “What do you think is happening to your family member?” Only 4 of the respondents described the situation in a way that reflected a clear understanding of the progression of dementia (“Alzheimer’s is an irreversible progressive brain disease”). Twelve described the situation solely in terms of memory and forgetfulness (“Dementia? Memory loss due to old age?”). They provided no indication that they understood the disorder to be a problem of global cognition that might be affecting either behavior or day-to-day functioning. The largest group (n = 14) provided a variety of explanations and descriptions, none of which indicated a disease as a basis for the person’s condition (“I think it is 90% natak (faking) and 10% illness. I think the illness part is due to her age”; “I do not know. It is some mental illness”; “I believe my husband developed it because of overwork in the office”; “It could be due to loneliness.”). There were other participants who wondered if this mysterious disease was black magic or punishment from God. Some participants wondered “If someone has done some black magic on him, but then what can I do?” Others said “It is sort of punishment from God. Why would such a thing happen to him?” With the exception of a few participants most did not understand Alzheimer’s disease and demonstrated need for more education and clarification of the disease process.
Caregiving activities
All of the CGs reported providing some degree of assistance to their family member. More than 80% reported providing help with 1 or more activities of daily living (ADL) including assistance with eating, toileting, hygiene, and dressing. One wife CG commented “[I] have to remind him to eat again and again. Sometimes he throws it away and I have to clean it. Sometimes he does not remember to wash his hands. I have to do it for him. Have to wash his face. Have to change his clothes when he passes urine in it.” Half of the sample stated that they assisted the family member with instrumental activities of daily living (IADL) such as handling the finances and banking, shopping, completing household tasks, or letter writing. For example, another wife CG observed that she is responsible for “handling all the finances, banking problems, shopping, running the family. Earlier I never had to do all this—make all the decisions.”
Caregiving difficulties
Most CGs verbalized feelings of being overwhelmed, depressed and frustrated with the role of being a CG. One participant said “Everything is new for us! We did not have to look after her before so everything is new. It is very difficult for us to manage.” Others reported changes in family role, “He’s become more like a child. He can’t put on his pants even if you give it to him.” A few also indicated a financial burden because of costs associated with buying medicine and inability to continue their job due to their caregiving role (“We do not have money and have difficulties. No one to help us.”). The CGs also expressed a profound sense of isolation and compromised feeling of well-being (“Sitting alone most of the time. I changed my life.” “There is no one else. It is a continuous illness, so we cannot ask others to stay and help us.”). Several CGs indicated that their social or personal activities had been constrained because of their caregiving responsibilities. Distress of CG has led to some violent behavior. One CG admitted to hitting his father with dementia out of frustration, while a female CG twice attempted to pour kerosene on herself to commit suicide.
The most frequently expressed difficulty (voiced by 22 CGs) was the negative emotional impact of caregiving (“He keeps asking questions. He cannot work. I am getting fed up.” “I know it’s not her fault, but there are times when I can’t control my anger and irritation.”). Twenty CGs mentioned the need for constant vigilance and supervision (“We have to keep an eye on him constantly.”). Closely related to this theme (and noted by 17 CGs) was the need to worry about the person’s physical safety (“He used to have weapons-hunting—we thought in this condition, it’s dangerous—we hid the bullets and told him he forgot where he kept it. He wants it and asks for it, tells us we have to buy them and we have difficulties with it still.”). Issues specifically related to toileting and incontinence were voiced by more than half (16) of the respondents (“I find it difficult because I cannot say my prayers and puja with that smell. I would have cleaned it in the morning and then again, she dirties it.” “He does not know where to go for the toilet, sometimes he goes, otherwise he does not and I have to clean it.”). Half (15) of the CGs identified unpredictable behavior as a particular difficulty (“He does not sit in one place, wants to go out. Suddenly he will get up and I do not think he understands what we speak”), and 11 pointed to other disruptive behaviors as being difficult (“My children are scared. She will not let them study … throws their books away and talks loudly. They want her hospitalized. I have to make them understand that she is ill.”).
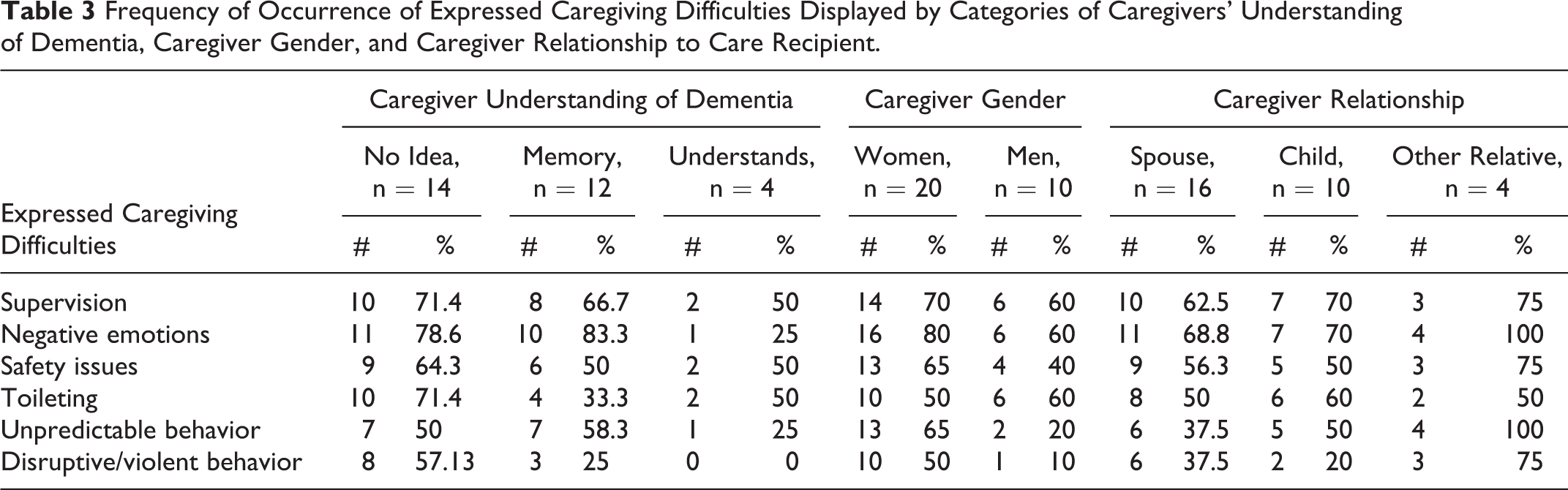
Table 3 displays the distribution of the 6 most frequently identified codes of expressed caregiving difficulties against 3 ways of categorizing the CGs—their understanding of dementia, gender, and relationship to the CR (spouse, child, or other relative). In general, few patterns emerged: CGs expressed caregiving difficulties equally, regardless of the categorizations. A few exceptions should be mentioned. Most noteworthy were differences in CGs’ expressed difficulties with unpredictable and disruptive/violent behaviors. The CGs whose discourse indicated a clear appreciation of the CR’s situation (ie, that she or he was affected by a progressive brain disorder) did not make any statements indicating they found the person’s behavior to be disruptive or violent. Furthermore, even when they mentioned other caregiving difficulties, this group of CGs generally did not indicate them to be troubling or distressing, whereas those who did not appreciate the disease-based nature of the behaviors did find them so. Women seemed to perceive the CR’s behavior as unpredictable and disruptive or violent more frequently than did male CGs. In regard to caregiving relationship, other relatives (daughters-in-law, niece by marriage) perceived unpredictability and disruptive or violent behavior more frequently than did spouses or children.
Frequency of Occurrence of Expressed Caregiving Difficulties Displayed by Categories of Caregivers’ Understanding of Dementia, Caregiver Gender, and Caregiver Relationship to Care Recipient.
Caregiver as a concept
Of special interest for the team’s efforts to develop a CG education program, none of the respondents could identify a word for “caregiver” in his or her language. They understood the English language term but could provide no similar term in their language. Respondents made it clear that what they were doing was related to their sense of family and for duty. (“I am able to please my God—my duty—and I will be rewarded later”). There was, however, no endorsement of the notion that caregiving was a separate and new role or that the work involved somehow different from what one would normally do in a family.
Caregiving roles
For Indian CGs rooted in the extended family system and living in their respective communities, CG roles are either assigned or accepted. Most of the CGs verbalized assuming the CG role out of sense of duty and obligation. As one of the participants said “It is my duty as a wife, so I expected to look after him eventually,” while siblings caring for their mother stated “Yeah definitely, because she cared for us when we were a child. She gave birth to us … It is our duty and affection”. A couple of CGs, both adult children, indicated they were motivated to provide care by feelings of attachment to the CR (“We love her very much.” “My mother is everything to me ….”)
On the other hand, some CGs assumed this role as either no one else was available or they were assigned this role by family or community expectations. One participant pointed out that “We wanted her to go back but my sister-in-law is very strict, she will not take her back,” while other participant replied, “There is no one to help her. I have to do it … I am the only daughter-in-law so I have to do it.”
A third of the sample reported receiving no assistance with caregiving from family or others. The remaining respondents reported receiving help from family member, friends, or maid servants. Assistance was mainly in the form of practical help with housework, shopping, and monitoring the person with dementia. A few CGs (10%) reported that others provided emotional support or financial assistance.
Thirty-seven percent of the CGs indicated that they were the ones responsible for making decisions related to their relative’s memory problems. Most (70%) of the decisions concerning the affected relative were made in consultation with other family members, while 10% of the CGs did not consult anyone else. Two CGs reported consulting a psychiatrist before making decisions.
What caregivers want to know
Because the US curriculum is geared so heavily to the development of caregiving strategies that are grounded in enhanced knowledge and skill, the interviews asked family members to identify what they would like to learn. The responses were notable in that very few reflected any notion that the CG might exercise some control over the situation. Many were unrealistic—given the true nature of the disease. Some wanted the condition to be reversed (“She should get better; that’s all the help I want.”) (“I just want him to get stronger, stop passing in his clothes.… I want to know more about it and help him get better.”) (“We just want her to get better.”) Others sought to learn strategies that are inconsistent with the nature of the disease (“I want to know how to make him go to the toilet every time.”)
(“I am trying to teach him to improve his memory.”) (“I want to teach him … to get up on his own.”). Still others seem at a complete loss about what kind of learning to seek (“I don’t know what to do with him at all.”) (“Only God can reverse it, we should not give up hope.”). Only one response reflected a holistic understanding of the situation (“… now that we know, we are more patient and don’t argue, take it with a pinch of salt—don’t make an issue of it.”).
Feedback on program components
Participants were asked about the usefulness of 5 program components, namely, (a) information about dementing diseases and their effect on the person, (b) developing strategies for day-to-day life with a person having a dementing illness, (c) setting realistic goals for the work of caregiving, (d) developing a “clinician’s attitude” and being the person who is in control in the situation, and (e) strategies for making long-term and immediate decisions. Twenty-seven (90%) CGs expressed interest in a program on family caregiving for persons with dementia; 3 were not interested. Over half of the CGs made a blanket statement that the components appeared to be useful without explicitly stating a preference for one or more components. The component most frequently endorsed was information about dementia and its effects on the person.
Of the 27 CGs who expressed an interest in an educational program, 9 (33.3%) CGs preferred a group format, 8 (29.6%) did not want a group format, and 4 (13.3%) had no preference between the 2 formats. The remaining 6 CGs suggested other formats (eg, Internet group and television) or did not indicate a specific format. Several CGs had concerns about the logistics of attending a program including their inability to leave the person with dementia alone at home and the distance and cost of travel to NIMHANS.
Discussion
Findings from the study confirmed that Indian and Western CGs are similar in several respects. In our sample, the vast majority of CGs were women, mostly spouses and daughters, as are most CGs in Western countries. 33 -35 The Indian family CGs in this study were frustrated, depressed, and overwhelmed with caregiving, responses similar to those expressed by dementia CGs from Europe and the United States. 36 -39 There is substantial functional equivalence between caregiving in the United States and India. The CGs in both countries provide assistance with ADL and IADL. One area of difference was that only 1 Indian CG mentioned concerns about driving which is a major consideration for many US family CGs. The most likely explanation for this difference is that very few Indians, regardless of age, drive cars. The rate of car ownership in India is 11 passenger cars per 1000 persons compared to 403 passenger cars per 1000 persons in the United States. 40 The most frequently mentioned caregiving difficulties were the impact of negative emotions and the need for constant supervision of the person with dementia followed by concerns about safety, dealing with incontinence, and behavior problems (eg, unpredictable or disruptive behaviors). These findings are consistent with both the Indian literature 10,41 and the literature from developed countries. 42 -44
There were few patterns in how CGs perceived caregiving difficulties. One noteworthy finding was that CGs who recognized that the CR had a brain disorder did not make any statements about the CR’s behavior being disruptive. One possible explanation is that because these CGs have a better understanding of the disease, they recognize the triggers for disruptive behavior and are able to de-escalate the situation before the CR becomes agitated or violent. It must be acknowledged that disruptive behaviors were the least frequently mentioned caregiving difficulties and by chance this group of CGs may not have encountered disruptive behaviors in their relative with dementia. Two gender differences were noted; more women CGs mentioned unpredictable and disruptive or violent behaviors than did men. These differences are congruent with the findings from previous research. 16,44,45 Two kinship differences were seen; CGs categorized as other relatives (mostly daughters-in-law) perceived unpredictable and disruptive or violent behaviors more frequently than spouses or adult children. There are some inconsistencies in findings from earlier studies that addressed kinship differences in perception of CR problem behaviors. For instance, in a study of Japanese caregiving spouses, adult children, and daughters-in-law, researchers found that daughters-in-law reported more CR behavioral problems than did other kin. 46 Findings from a meta-analysis of 168 studies showed that both caregiving adult children and children-in-law reported significantly more instances of CR behavioral problems than spouses did. 47 However, there were no significant differences between the children and the children-in-law’s reports of CR problem behaviors. Pinquart and Sorenson suggested that spouses may underreport CR behavior problems. Additionally, they pointed out that CRs cared for by spouses were on average 5 years younger than those cared for by children or children-in-law. Since dementia is a progressive, age-related illness, “it may be that spouses experience fewer dementia-related symptoms than adult children and children-in-law, due to their CRs’ younger age.”47(p8) In our study, the CRs cared for by in-laws were on average about 10 years older than those cared for by spouses and 8 years older than those cared for by children. Therefore, it may the older age of the in-law’s CRs that accounts for the greater frequency of problem behaviors reported by in-laws.
Few of our CGs had an accurate understanding of dementia and its causes. Many explained dementia as memory loss and forgetfulness that some attributed to old age. There was little recognition that dementia is a condition of global deterioration of cognition that impairs thought and social functioning. This finding was consistent with previous studies of Indian 48 -51 and Pakistani 52 CGs who reported limited knowledge of dementia. In contrast, people from Western countries (eg, Australia, Europe, and the United States.) showed greater awareness of dementia as a disease. 37,38,53 Additionally, most Western subjects recognized that Alzheimer’s disease was not due to a normal aging process. 37,38,54
A noteworthy cultural difference that emerged from the study was that CGs did not have a word in their own language for caregiving. Caregiving was not seen as a separate role but rather part of their responsibilities as a family member. This situation contrasts with the West where the caregiving role is widely acknowledged and efforts have been devoted to studying acquisition of this role. 55 -57 Since taking on the caregiving role is not recognized as a role change, Indian CGs may not recognize that it is possible and necessary to learn caregiving skills and how to take care of themselves. Therefore, it would be appropriate to build on these family CGs’ cultural expectations by helping them better fulfill their familial responsibilities (eg, be a better daughter-in-law).
Among our group of CGs, the most frequently expressed motivation for caregiving was a sense of duty or obligation followed by affection for the CR. Some took on caregiving because no one else was available. These findings were consistent with the findings from other studies of Indian CGs. 41,48,58 In Western studies, feelings of affection and love for the CR were mentioned more often than in our sample or the other studies of Indian CGs, 59 -61 although CGs in Western studies also mentioned marital duty or filial responsibility as motivations for caregiving. 62,63
Most CGs in our study were interested in an educational program on dementia caregiving, and over half agreed on the usefulness of all of the components. There was no clear preference for a group or individual format for an intervention. The CGs wanted information on dementia, but many of their expectations for what they want to learn were not realistic. Few recognized that the CG could exercise any control over the situation. These CGs would benefit from education about dementia/Alzheimer’s disease, its causes, and progressive nature. Additionally, education is needed regarding appropriate strategies for dealing with CRs’ troubling behaviors and issues such as incontinence.
Family CGs raised several concerns that need to be considered in developing an educational intervention. Although many participants spoke English or Kannada, several other languages were represented. In designing a group intervention, consideration would need to be taken regarding a common language to be used. Several CGs were concerned about who would look after their relative with dementia while they attended the program. Provision of an activity for CRs or someone to watch them may be needed during educational sessions. It may also be necessary to offer a stipend for travel to attendees to cover the cost of transportation to NIMHANS, an issue raised by several CGs.
This study had several limitations. A small convenience sample of CGs was selected from a single geriatric clinic at a large urban mental health facility which may not fully represent the target population of Indian CGs. Participants were seeking assistance from the geriatric clinic at NIMHANS and had met with health care professionals about their relative with dementia. The study results may not reflect the experiences of CGs who have not discussed their family member’s condition with a health care provider. Only a third of the sample was from a rural location, therefore it was not possible to draw meaningful conclusions about this subsample.
This article has reported the findings from the needs assessment, the first phase of a project to transform the Savvy Caregiver program to meet the requirements of dementia family CGs in South India. The next step will be to use this information to revise the Savvy Caregiver curriculum and to pilot test it on a small scale.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Fogarty International Research Collaborative Award (Grant #7R03TW001498-04).