
Abstract
We aimed to confirm the effectiveness of brain-activating rehabilitation (BAR) performed in the day care setting at an acute hospital. Brain-activating rehabilitation is based on 5 principles: developing a pleasant atmosphere, promoting communication, praising patients, giving patients a social role, and providing supportive care. A total of 48 patients with dementia or cognitive impairment were selected and randomly divided into the intervention and control groups. The BAR-based intervention was conducted for 1 hour, 3 times a week. The patients’ score of the Multidimensional Observation Scale for Elderly Subjects (MOSES) were used as outcome measures. Repeated-measures analysis of covariance detected a significant interaction between the MOSES disorientation (F = 4.437, P = .041) and the withdrawal (F = 5.052, P = .030) subscales. A BAR-based intervention performed at our acute hospital was effective at maintaining and improving the cognitive and psychosocial functioning of patients with dementia or cognitive impairment.
Keywords
Introduction
Japan is one of the most rapidly aging societies in the world. Accordingly, the number of people with dementia or mild cognitive impairment has been increasing. As older patients are also susceptible to various physical conditions (eg, fractures after a fall, pneumonia), the number of patients with dementia admitted to acute hospitals will continue to increase. 1 In fact, in a study involving 616 patients aged ≥70 years who were being treated at a large urban acute general hospital, it was found that 42.4% of the patients had dementia. 2 In addition, some elderly patients have cognitive impairment. Although such patients will not be diagnosed with dementia, they might exhibit behavioral and psychological symptoms of dementia (BPSD). 3
Strong associations exist between delirium and long-term cognitive impairment or dementia, and it has been suggested that acute illnesses might account for these relationships. 4,5 In acute-care hospitals, it is often necessary to enforce bed rest and physically restrain patients for treatment purposes. However, elderly patients with cognitive impairment cannot adapt to changes in their environment, and hence, during periods of hospitalization, they experience high levels of anxiety, and physical restraint only adds to this. These strong stressors can cause BPSD. 6 Similarly, physical restraint and changes in the environment have been demonstrated to cause patients (70%∼87%) to have delirium in the intensive care unit. 7,8
The use of hospital day care to treat patients in acute-care hospitals is spreading rapidly. During hospital day care, elderly patients with dementia, cognitive impairment, and delirium perform activities designed to prevent cognitive impairment. 9 –11 Patients have performed various activities (eg, body exercise, handicraft, arts and crafts, coloring, and ringtoss) in the hospital day care. 9,10 However, the activities performed during hospital day care vary widely. Furthermore, the effects of hospital day care have not been examined in sufficient detail.
The 2010 guidelines for the treatment of dementia in Japan highlighted the need for the proper care and rehabilitation of patients with dementia. Rehabilitation activates the brain and reduces the effects of disuse by increasing residual brain function. This is effective at maintaining and improving the viability of cognitive functions and quality of life. As a result, rehabilitation leads to the maintenance of and improvement in cognitive function. 12
Yamaguchi et al advocated a particular type of rehabilitation called brain-activating rehabilitation (BAR). 13 The BAR is based on 5 principles: (1) enjoyable and comfortable activities should be performed in an accepting atmosphere; (2) the activities should be associated with empathetic 2-way communication between the staff and the patients as well as between the patients; (3) the patients should be praised to enhance their motivation; (4) the patients should be offered social roles that enhance their remaining abilities; and (5) supportive care should be provided to prevent task failure that causes confusion. Brain-activating rehabilitation is considered to enhance patients’ motivation, maximize the use of their residual functions, and prevent cognitive function disuse.
Brain-activating rehabilitation is also considered to enable participants to recover both a desire for life and their self-respect. The BAR-induced increases in motivation have been shown to ameliorate the BPSD and lead to improvements in activities of daily living. 14 Improvements in cognitive function can also be expected through BAR. 15
A previous randomized controlled trial demonstrated that an intervention based on the principles of BAR was effective at maintaining and improving daily life functions in elderly participants with dementia who were living in residential care homes. 16 Another study found that BAR was useful for maintaining and improving cognitive function, BPSD, depression, and motivation. 17 Furthermore, BAR was demonstrated to prevent dementia in elderly people with cognitive impairment. 18
There have not been any studies about the use of BAR in the acute hospital day care setting. In this study, we conducted a randomized controlled trial in which patients with dementia and cognitive impairment were subjected to an intervention based on the principles of BAR in the inpatient day-care setting at an acute hospital to demonstrate the effectiveness of BAR.
Methods
Patients
Sixty-eight elderly patients (46 females; mean age: 87.3 ± 6.7 years) who were being treated at the Gunma Chuo hospital (acute hospital) participated in this study. The following inclusion criteria were applied: (1) the patients had to have been referred for rehabilitation by a doctor between June 18, 2014, and October 21, 2014; (2) the patients had to have been diagnosed with dementia or to have exhibited a clinical dementia rating (CDR) of 0.5 to 3 and complained of disorientation and memory loss (the patient themself or a family member) at the time of admission; (3) the patients had to be able to sit down; (4) the patients had to agree to participate in the study; and (5) the patients had to participate in the study for more than 1 week.
Randomization
At the time that the doctor referred the patient for rehabilitation, they were randomly assigned to the intervention or control group using a random number table. As a result, 68 participants were randomly allocated to the intervention group (n = 36) or control group (n = 32; Figure 1).
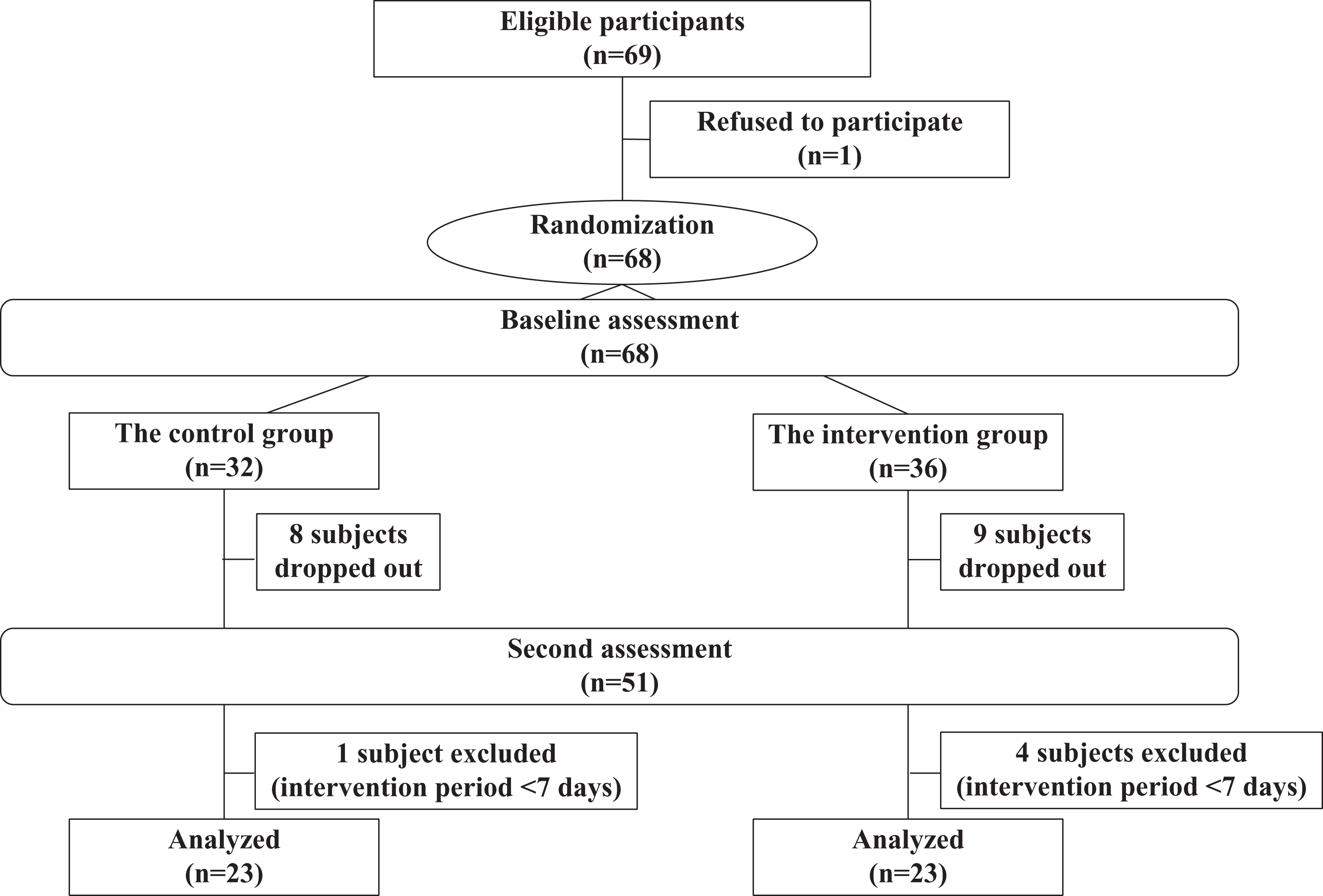
Flow of participants in the intervention and control groups.
Intervention
Both the intervention group and the control group underwent the standard rehabilitation program, but only the intervention group underwent BAR. The BAR was conducted in the ward day room 3 times a week (Monday, Wednesday, and Friday; 14:30-15:30). Two staff members supervised the sessions (an occupational therapist and a nurse). The staff took a course in BAR before the intervention.
Various activities (body exercise, collage with traditional Japanese paper, singing, origami, coloring, haiku, tanka, and reality orientation) were selected based on the patients’ physical function, cognitive function, life history, and preferences. These were evaluated by 5 of the authors (K.T., M.T., A.H., Y.S., and H.S.). All of the interventions were carried out in accordance with the 5 principles of BAR.
Outcome Measures
The patients’ scores for the various domains of the Multidimensional Observation Scale for Elderly Subjects (MOSES) and the Mini-Mental State Examination (MMSE) were used as outcome measures. The MOSES is an observational scale of cognitive and psychosocial functioning, whereas the MMSE is a test of cognitive function. The patients were examined using these questionnaires at the time of their referral for rehabilitation and at discharge. The MOSES is comprised of 40 parameters covering 5 categories of cognitive and psychosocial functioning: (1) self-care; (2) disorientation; (3) depression; (4) irritability; and (5) withdrawal. The score for each category ranges from 8 to 32 points (each parameter is scored as follows: 1 = not at all; 2 = seldom; 3 = at times; and 4 = often), with higher scores indicating more severe disorders. The scale is reported to have high reliability. 19 Cognitive functioning was tested using the MMSE. The MMSE examines orientation, attention, calculation, immediate and short-term memory, language, and praxis and is considered to exhibit good reliability. 20 The MOSES and MMSE were administered by 5 of the authors (K.T., M.T., A.H., Y.S., and H.S.).
The following background factors were also assessed: age, gender, the reason for the patient’s hospitalization, dementia type, the intervention period, the Functional Independence Measure (FIM; a measure of functional independence during activities of daily living), and the CDR. Except for the CDR, all of the parameters were assessed based on the notes of the patients’ consultant physicians. The CDR was conducted by occupational therapists with sufficient clinical experience (K.T., M.T., A.H., Y.S., and H.S.).
Statistical Analysis
Comparisons were made between the intervention and the control groups. Data for the outcome measures that were obtained before and after the intervention were analyzed using the Japanese version of SPSS Statistics for Windows (version 20.0; IBM Corporation, New York). The independent t test or χ2 test was used for comparisons between the 2 groups at the baseline. We hypothesized that the MOSES and MMSE test scores of the patients in the intervention group would be better than those of the control group after the intervention period. Repeated-measures analysis of covariance was performed with age, sex, and the intervention period as covariates at the end of the study. In this study, the intervention period of each patient was not the same because of the difference in the days of hospital stay. We think the intervention period is an important confounding factor that influences intervention effects. Therefore, we adjusted the intervention periods of 2 groups by taking it as a covariate. Post hoc analyses of “between participants” and “within participants” factors were conducted using Bonferroni’s correction.
Procedure
This study was approved by the institutional research board of the Gunma Chuo Hospital (No.2014-009). Written consent was obtained from each patient and their families after full information regarding the purpose of this study, its risks and benefits, the data confidentiality and anonymity procedures used, and the patients’ freedom to participate (or not) had been provided.
Results
Patients’ Baseline Characteristics
The study patients were 68 elderly patients who either had been diagnosed with dementia or were suspected to have dementia (36 in the intervention group and 32 in the control group). Eight patients from the control group and 9 patients from the intervention group dropped out due to worsening of their disease and/or death. In addition, 5 patients (1 from the control group and 4 from the intervention group) were excluded because they underwent rehabilitation for <1 week, which was not considered to be long enough to have a marked therapeutic effect. Thus, the outcome measures were analyzed in 46 patients: 23 from the intervention group and 23 from the control group. None of the demographic variables differed significantly between the groups at the baseline (Table 1).
Demographics of the Study Patients.a,b
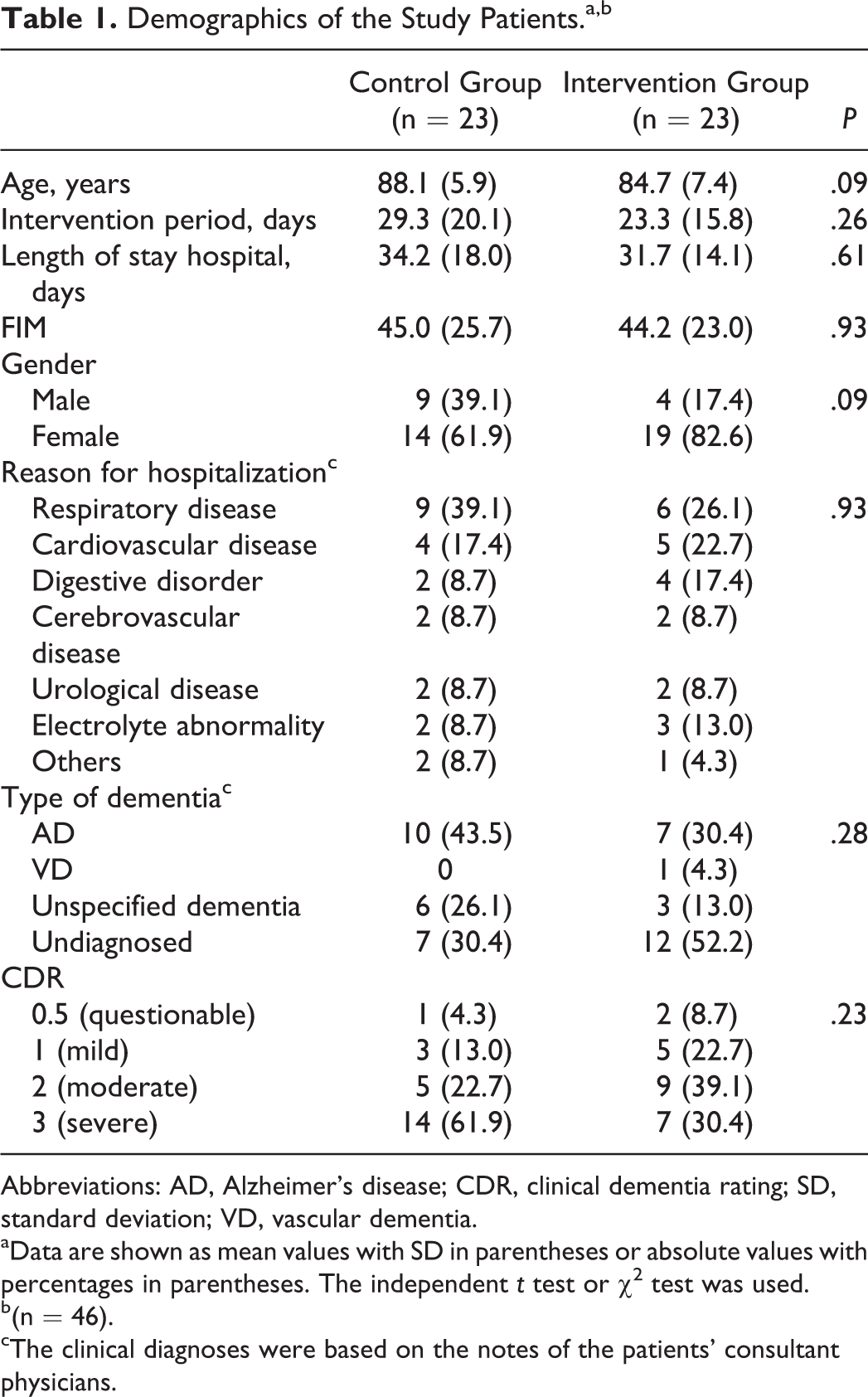
Abbreviations: AD, Alzheimer’s disease; CDR, clinical dementia rating; SD, standard deviation; VD, vascular dementia.
aData are shown as mean values with SD in parentheses or absolute values with percentages in parentheses. The independent t test or χ2 test was used.
b(n = 46).
cThe clinical diagnoses were based on the notes of the patients’ consultant physicians.
Change in the Outcome Measures
Compared to the control group, the intervention group exhibited significant improvements in the MOSES subscales for disorientation, F (1, 41) = 4.437, P = .041; post hoc analysis: intervention group, P = .001; control group, P = .635, and withdrawal, F (1, 41) = 5.052, P = .030; post hoc analysis: intervention group, P = .001; control group, P = .297, at the end of the study (Table 2).
Changes in the Outcome Measures in the Intervention (n = 23) and Control Groups (n = 23).a
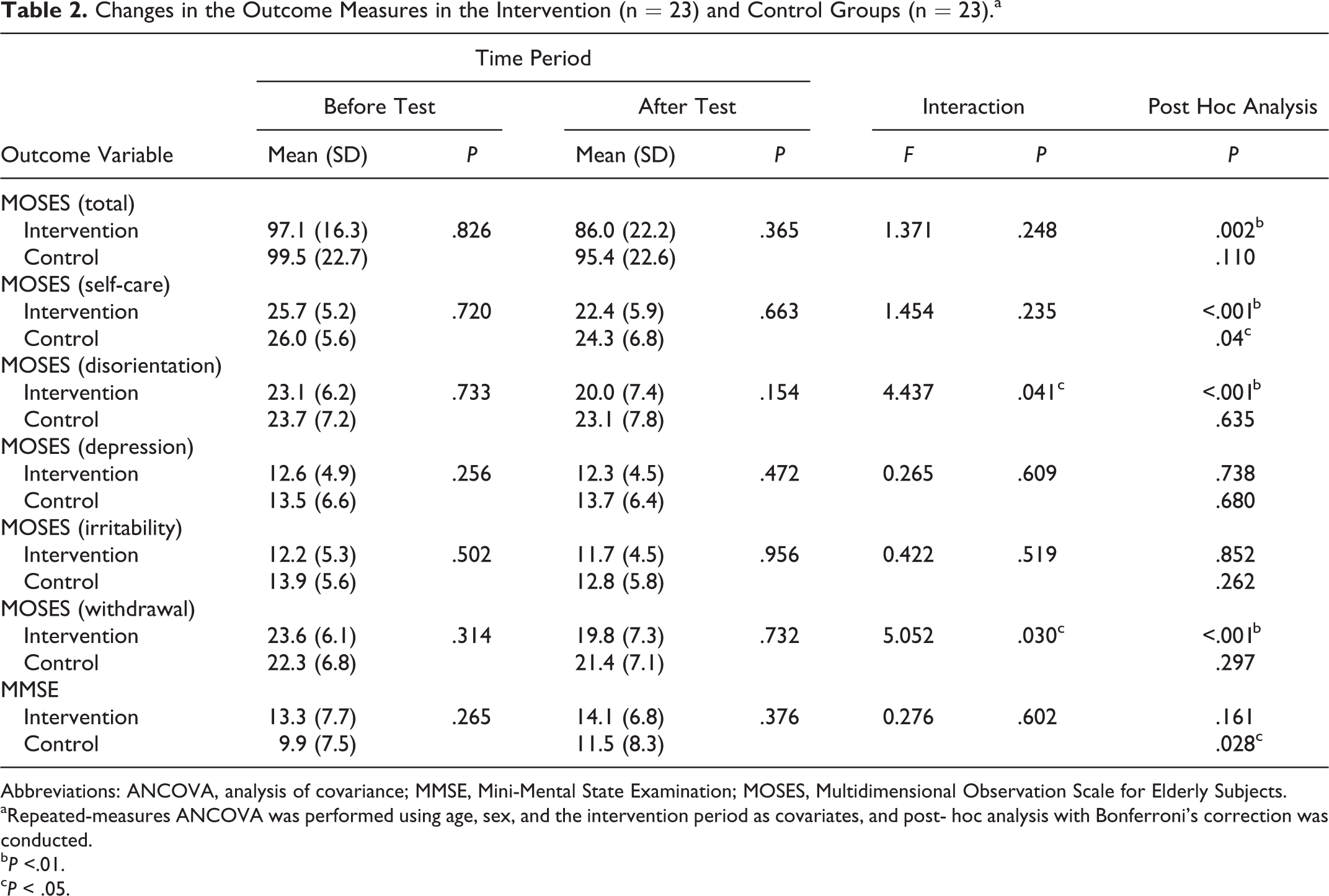
Abbreviations: ANCOVA, analysis of covariance; MMSE, Mini-Mental State Examination; MOSES, Multidimensional Observation Scale for Elderly Subjects.
aRepeated-measures ANCOVA was performed using age, sex, and the intervention period as covariates, and post- hoc analysis with Bonferroni’s correction was conducted.
b P <.01.
c P < .05.
Discussion
Our results indicate that an intervention based on the 5 principles of BAR brought about improvements in the MOSES subscales for disorientation and withdrawal but did not result in any improvement in cognitive ability according to the MMSE. In this study, patients were divided randomly in order to minimize the influences of spontaneous recovery. As a result, the intervention group improved more than the control group in the MOSES subscales for disorientation and withdrawal. Therefore, we interpreted this improvement as the effect of BAR, not spontaneous recovery. In a previous randomized controlled trial, the effects of an intervention based on the principles of BAR were examined using the MOSES and Hasegawa dementia scale-revised (HDS-R, a cognitive test) as outcome measures. 16 The latter study detected improvements in the MOSES subscales for disorientation and withdrawal but did not detect any improvements in the HDS-R score.
Interventions based on the principles of BAR provide patients with support, empathy, and acceptance. Brain-activating rehabilitation is considered to enable participants to recover their self-respect and increase their motivation. 14 Although the majority of the patients had dementia in this study, some patients hadcognitive impairment. In the previous study of BAR, apathy seen in patients with cognitive impairment was improved. 18 Reality orientation has been demonstrated to improve patients ability to communicate effectively and to respond to their environment and other people. 21,22 In addition, an intervention based on the BAR principles enhanced the degree of understanding between staff and patients, as well as between patients, which had generalized beneficial effects on the patients’ daily lives. Therefore, individuals who take part in such interventions might develop an increased sense of self-worth and a greater desire to live, and their behavioral and psychological symptoms might be ameliorated. 16
During hospitalization, the patient’s environment changes and illness can also cause alterations in their body. In elderly patients with cognitive impairment, such changes can make it difficult for them to recognize their current situation, which can lead to delusions. In addition, such patients might not be able to perform activities of daily living as easily as they were before and often find themselves being directed from children and caregivers, which causes stress (a loss of confidence, anxiety, tension, etc). 23 Increased vulnerability to stressors can result in agitation, depression, apathy, repetitive questioning, psychosis, aggression, sleep problems, wandering, and a variety of socially inappropriate behaviors. 6 The patients in this study were in just such a state. However, the BAR-based intervention reduced their anxiety and stress levels and improved their motivation, which alleviated their withdrawal.
Ameliorating withdrawal is a basic tenet of preventive care and was found to decrease the frequency of verbally disruptive behaviors during social interactions. 24 In addition, the extent of social networks was demonstrated to modify the relationships between some measures of Alzheimer’s disease pathology and cognitive function. 25 Ameliorating withdrawal also helps to prevent dementia. In the present study, an intervention based on BAR performed in the inpatient day care setting at an acute hospital was found to be effective at maintaining the cognitive abilities and improving the psychosocial functioning of patients with dementia and cognitive impairment.
We demonstrated the effectiveness of dementia rehabilitation based on the principles of BAR in a quasi-randomized controlled trial. We expect that BAR will become widely accepted as a useful tool for rehabilitating patients with dementia and cognitive impairment.
In this study, the patients’ cognitive function levels and diseases were variegated markedly. We could not screen the patients according to their cognitive function levels and diseases. And all the patients in this study were in 1 acute hospital. So we need to verify our findings in a more homogeneous study population.
Footnotes
Acknowledgments
The authors would like to thank Rui Horiguchi, Kayoko Okoshi, Sayoko Aoki, Kaori Negishi, Chiaki Yokote, and Kunie Yarita (ward nurses) for their cooperation during the BAR-based intervention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: T. Yamaguchi was supported by a grant from the JSPS KAKENHI, Japan.