
Abstract
Blood–brain barrier impairment and endothelial cell dysfunction have both been implicated in the pathogenesis of Alzheimer’s disease (AD). The presence of vascular risk factors is also known to increase the risk of AD. Soluble endothelial protein C receptor (sEPCR) should thus produce procoagulant and proinflammatory effects. Serum sEPCR levels have been found to be associated with several diseases. To date, no reports have been published regarding serum sEPCR levels in AD. In this study, we found that serum sEPCR levels were significantly increased in patients with AD when compared to control participants (P = .0005). There was no significant difference between patients with mild cognitive impairment (MCI) and healthy controls (P = .055) or between patients with AD and MCI (P = .054). Importantly, our results also indicate that the degree of cognitive impairment is significantly correlated with serum sEPCR levels in all patients and healthy controls. These findings suggest that serum sEPCR levels could be a potential candidate for a biomarker panel for AD diagnosis.
Introduction
Alzheimer’s disease (AD) is a progressive, irreversible neurodegenerative disease in the elderly individuals. It is characterized by the accumulation of amyloid plaques and neurofibrillary tangles and by massive neuronal loss in the brain. Epidemiological studies have shown that the presence of vascular risk factors increases the risk of AD. 1 Blood–brain barrier (BBB) impairment and endothelial cell dysfunction have both been implicated in the pathogenesis of AD. 2 It was also reported that patients with AD had more severe atherosclerosis in large cerebral arteries at the base of the brain (circle of Willis) than age-matched controls without AD. 3 Significantly increased serum angiopoietin 1 (Ang-1) levels were found in patients with AD when compared to control participants (P = .003), suggesting that serum Ang-1 could be a potential candidate for a biomarker panel for AD diagnosis. 4 However, little information has been reported regarding biomarkers associated with vascular diseases.
The protein C pathway plays an important role in regulating the blood coagulation system. 5 Activated protein C (APC) is generated from inactive protein C via proteolysis mediated by a complex of thrombin, thrombomodulin, and endothelial protein C receptor (EPCR) found primarily on the surface of the endothelium. The common feature shared by most of these protective effects is that they are dependent on EPCR. The EPCR not only binds protein C and increases the rate of protein C activation, 6 but is also involved in mediating the multiple cytoprotective effects of APC including anti-inflammatory and anti-apoptotic activities 7 and protection of endothelial barrier function. 8 The EPCR is a kind of type I transmembrane glycoprotein containing 2 domains in the extracellular region that are homologous to the α1 and α2 domains of CD1/major histocompatibility complex class 1 molecules. A soluble form of EPCR (sEPCR) is present in human plasma 9 due to cleavage of the membrane-bound molecule by a metalloprotease. 10 Soluble EPCR has affinity to its ligands similar to EPCR, such as protein C, APC, FVII/FVIIa, and so on. It has been reported that sEPCR-bound APC fails to inactivate FVa and loses its ability to regulate blood coagulation. 11 More importantly, if PC binds to sEPCR, it cannot be activated by the thrombin, thrombomodulin, and EPCR complex. 12 Thus, soluble EPCR would have procoagulant and proinflammatory effects. A recent study has shown that elevated sEPCR levels might represent a candidate risk factor for PE and, as in lupus, might contribute to the underlying vasculopathy. 13 To the best of our knowledge, there are no data in the literature describing a statistically significant difference between serum sEPCR levels of patients with AD, patients with MCI, and healthy elderly controls.
The current study aimed to examine serum sEPCR levels in patients with AD, patients with MCI, and healthy elderly controls and to examine its association with the degree of cognitive impairment as measured by the Mini-Mental State Examination (MMSE).
Materials and Methods
Participants
A total of 45 patients with AD, 36 patients with mild cognitive impairment (MCI), and 42 healthy elderly controls were recruited from the Department of Gerontology at the Huangshi Central Hospital Affiliated to Hubei Polytechnic University. This study was approved by the ethics committee of Hubei Polytechnic University, and written informed consent was obtained from each participant. Demographic parameters and baseline characteristics were investigated and are listed in Table 1. All enrolled patients with AD fulfilled the criteria of International Classification of Diseases, Tenth Revision, Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition), and National Institute of Neurologic and Communicative Disorders and Stroke and Alzheimer’s Disease and Related Disorders Association. 14 Patients with MCI fulfilled the criteria as described previously. 15 The standard MMSE method was used to assess the clinical severity of cognitive impairment. 16
Patients’ Demographic and Clinical Details.
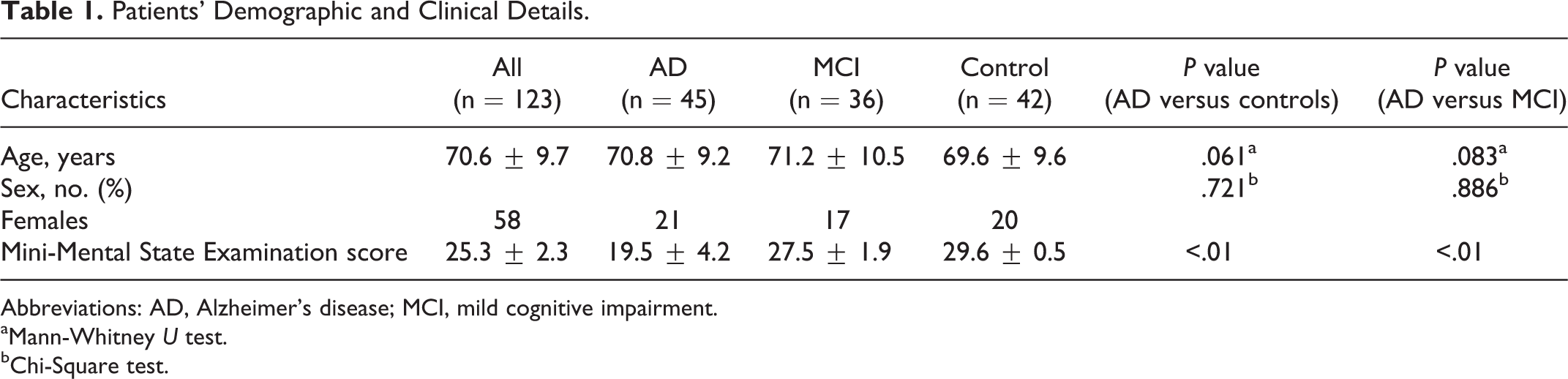
Abbreviations: AD, Alzheimer’s disease; MCI, mild cognitive impairment.
aMann-Whitney U test.
bChi-Square test.
Blood Sampling
Peripheral venous blood samples (12-15 mL) were collected between 08:00 and 09:00 hours (fasting state) in the morning in order to take into account any possible circadian rhythm. Collected samples were immediately immersed in melting ice. All the samples were centrifuged at 4°C for 15 minutes within 30 minutes after sampling in order to minimize the source of platelets and stored at −80°C until further analysis.
Measurement of Serum sEPCR Concentration
Serum sEPCR levels were measured using an enzyme-linked immunosorbent assay kit according to the manufacturer’s instructions (MyBioSource: San Diego, CA, USA). All measurements were performed in a blinded manner without knowledge of the diagnoses or disease status of the patients.
Data Analysis
The SPSS 19 was used to carry out all statistical analyses (SPSS, Munich, Germany). In order to compare serum sEPCR levels between patient groups (patients with AD, MCI, and healthy controls), a univariate analysis of variance (ANOVA) was calculated. The data are presented as means ± standard deviation (SD); P < .05 was considered to be statistically significant. A bivariate correlation analysis (Pearson correlation) between age, MMSE scores, and serum sEPCR levels was conducted. Differences between 2 groups in cases of normal distribution were assessed using the 2-tailed t test. The Mann-Whitney U test was used to assess differences between 2 groups in cases of nonnormal distribution. Differences in gender between the 2 groups were assessed using the chi-square test.
Results
Considering the age difference between controls and patients with AD, age was used as a covariate for the ANOVA. We found a difference in serum sEPCR levels between the 3 different groups (P = .004). Pairwise comparisons with an independent t test revealed a significant difference between patients with AD and controls (AD vs healthy controls [mean ± SD] 121.4 ± 38.2 vs 86.2 ± 38.4 ng/mL; P = .00005; Figure 1). There was no significant difference between patients with MCI (103.9 ± 41.8) and healthy controls (P = .055) nor between patients with AD and MCI (P = .054).
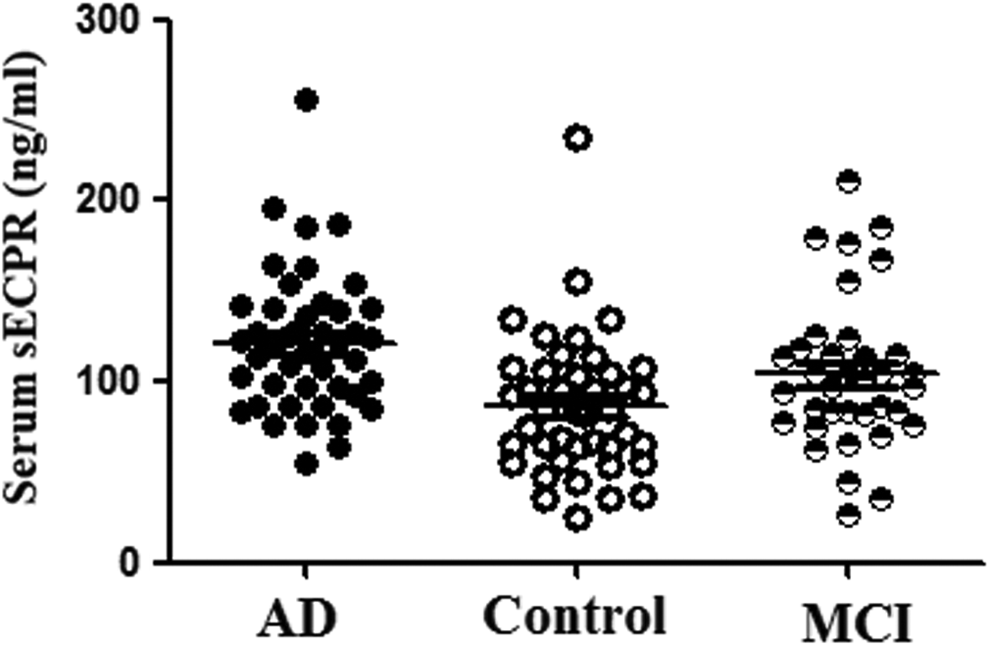
Serum soluble endothelial protein C receptor (sEPCR) levels (ng/mL) in patients with Alzheimer’s disease (AD), patients with mild cognitive impairment (MCI), and healthy elderly controls. Patients with AD showed significantly higher serum sEPCR levels when compared to healthy controls (P = .0005). There was no significant difference between patients with MCI and healthy controls (P = .055) nor between patients with AD and MCI (P = .054). The data are a mean value from 3 repeats.
There is a significant positive correlation between the MMSE scores (as a measure for cognitive status) and serum sEPCR levels seen in all patients and healthy controls (n = 123) (r = 0.70; P < 0.001; Figure 2). There was no significant correlation between serum sEPCR levels and MMSE scores in patients with AD.
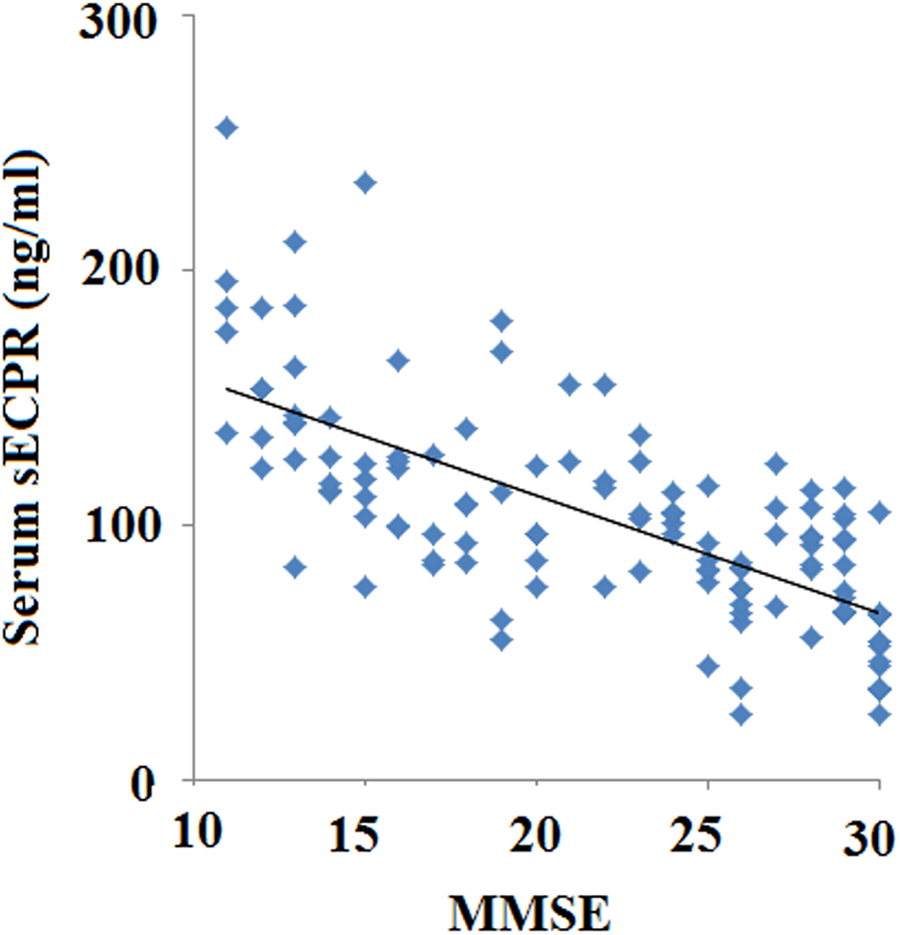
In all patients and healthy controls (n = 123), there is a significant correlation between the Mini-Mental Status Examination (MMSE) score (as a measure for cognitive status) and serum sEPCR levels (r = 0.70; P < .001). The data are a mean value from 3 repeats.
Discussion
In the present study, 2 major findings emerged, that is, (1) serum sEPCR levels are significantly higher in patients with AD when compared to healthy controls and (2) serum sEPCR levels are significantly inversely correlated with MMSE as a measure for cognitive status throughout the whole study population, indicating that a lower degree of cognitive functioning is associated with higher serum sEPCR levels. Endothelial dysfunction is a possible causal factor in the developmental process of AD. The relationship between AD and the endothelium is a new area of investigation which can elicit important findings about the development, progression, and even prevention of the disease.
A previous study reported that sEPCR could be identified in normal human plasma and retains its full ligand-binding capability. 17 APC protects the brain endothelium from divergent inducers of apoptosis by first binding to the EPCR. The sEPCR has a competitive affinity to protein C and prevents protein C activation through thrombin and thrombomodulin. In addition, sEPCR has been demonstrated to block the interaction of APC with phospholipids and alter the active site of the APC, most likely by changing its substrate specificity. Moreover, increased levels of sEPCR in plasma lead to dysfunction of EPCR-mediated coagulation. Alterations in soluble EPCR have been associated with several diseases. A recent study has just reported that alteration in soluble EPCR has been associated with late arteriovenous fistula stenosis in chronic hemodialysis patients with arteriovenous fistula. 18 In addition, the expression of EPCR and its soluble form (sEPCR) released into plasma as a result of proteolytic cleavage was investigated in ovarian, breast, lung, and colorectal cancer biopsies as well as in ascitic cell clusters and peritoneal fluid from ovarian cancer samples. And the results indicate that the levels of sEPCR are significantly higher than the normal range in patients with cancer than healthy volunteers. 19
Impaired peripheral endothelial alteration has been found in patients with AD by measuring the response to acetylcholine iontophoresed into the skin using laser Doppler flowmetry. 20 It was put forward that the toxic effect of amyloid-β (Aβ) may affect endothelial cells and cause endothelial-dependent vasoconstriction. 21,22 In AD, neurovascular damage includes BBB disruption at the level of brain capillaries 23 and the presence of cerebral arterial microbleeds. 24 Intravital brain imaging of clot formation and dissolution revealed abnormal thrombosis and fibrinolysis in AD mice. 25 Previous studies demonstrated that the transport equilibrium of Aβ at the BBB depends on an influx of plasma-derived Aβ from blood to brain and clearance of Aβ from brain to blood. 26 Thus, biomarkers that influence the integrity of the vascular endothelium may be important in detecting early vascular injury and may thus be a marker for early AD detection. The physiological importance and influence of sEPCR levels in vivo are unknown; however, elevated serum sEPCR levels have been found in patients with systematic inflammation diseases including sepsis and systemic lupus erythematosus. 27 Some biomarkers indicating endothelial dysfunction and vascular damage have been studied, and previous studies have reported that inflammation factors intercellular adhesion molecule 1 and interleukin 6 were elevated in patients with AD. 28,29 The clinical importance of the protein C pathway is evidenced by the multitude of dysfunctions in this pathway that result in thrombosis. 30 As BBB dysfunction has been associated with the pathogenesis of AD, 31 the generation of sEPCR leads to blockade of APC-binding site on EPCR, preventing APC crossing the BBB to reach its therapeutic targets in the brain. 32 Based on these findings, the clinical relevance of serum sEPCR in patients with AD deserves further study. Thus, the increase in serum sEPCR levels in patients with AD as demonstrated in the present study could be interpreted as an attempt of the human organism to counter the vascular inflammation and leakage seen in AD.
There are several limitations of this study. This is a single-center study, and the cases studied were limited. Further studies with larger samples of patients with AD are required. Second, this study does not allow determination of mechanism. Future research will provide us a complete picture of the underlying mechanism. Third, this is a retrospective study. A prospective and comprehensive study to validate clinical significance of serum sEPCR in AD would be required.
In conclusion, we found significantly increased serum sEPCR levels in patients with AD. We could also show an association between serum sEPCR levels and cognitive status in all patients and healthy controls. Thus, serum sEPCR could be a potential candidate for a possible marker panel for diagnosis of AD.
Footnotes
Authors’ Note
Yongjian Zhu and Zhilong Chen are co-first authors who contributed equally to this work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.