
Abstract
Cognitive training may be beneficial for individuals with Alzheimer’s disease (AD); however, the effects are modest with little evidence of carryover. Prior studies included limited hours and low intensity of training. The purpose of this study was to test the feasibility and efficacy of many hours of intensive cognitive training with adults in the early stages of AD. Twenty-one adults with very mild or mild AD participated in cognitive training for 10 days over 2 weeks with 4 to 5 hours of training each day. Participants significantly improved in practiced computer-based tasks including those involving working memory, sustained attention, and switching attention. Outcome measures that improved included the Mini-Mental State Examination, letter fluency, and 3 of 5 Trail-Making Tests. Gains in outcome measures were maintained at 2- and 4-month follow-up. Adults in early-stage AD can participate in intensive cognitive training and make modest gains in both practiced and unpracticed cognitive tasks.
Keywords
Introduction
More than 5 million people in the United States are estimated to have Alzheimer’s disease (AD), and this number is expected to reach 13.2 million in the year 2050. 1 There is an increasing interest in the role of cognitive training in potentially slowing the progression of AD. 2 Effects of cognitive training in AD are modest, 3,4 with little evidence of carryover to cognitive domains beyond those being trained. In these studies, gains in cognitive abilities may have been limited by training schedules.
A key feature of cognitive training is that tasks are chosen to challenge specific cognitive functions such as attention, memory, or processing speed, unlike nonspecific brain exercises that individuals may do as part of their everyday life, such as doing the newspaper crossword puzzle. 5 The training can be computerized or consist of oral and paper-and-pencil activities delivered by an on-site trainer. 4 Cognitive training can be offered individually or in groups; however, a recent meta-analysis of the literature concluded that individual training is relatively more effective. 3 Aging individuals without AD have been shown to benefit from cognitive training by significantly improving their memory, problem solving, speed of processing, 6 and daily function. 7
One of the primary considerations in designing cognitive training programs is to select a practice schedule that will produce measurable change and be acceptable to daily life schedules of the participants and in certain cases, their caregivers. Some of the least intensive programs provide cognitive training in a single 45-minute to 2-hour long sessions each week for a prescribed number of weeks. 5,8 –10 Some modest changes have been reported with these training programs including improvements in working memory, processing speed, and learning ability; 9 improvements in recall and recognition of practiced material; 8 recall and verbal attention; 10 and recall and face-name association tests. 11 Total time spent in training varies between studies in these weekly training schedules ranging from less than 5 hours to approximately 17 hours. A more recent study provided 24 hours of training for those with mild cognitive impairment (MCI) and reported significant improvements in most of the trained tasks. 12 It may be that more robust cognitive improvements could be achieved with more intense schedules.
Some studies have examined the efficacy of cognitive training with sessions provided more frequently than weekly. Adults with MCI attended six 1-hour sessions spread over 2 weeks with improvements in some trained tasks and transfer tasks. 13 Cipriani and colleagues provided thirteen 45-minute sessions delivered over 4 weeks for people with AD or MCI. 14 Those with AD improved in 19 of the 21 practiced measures, including tests of memory, perception, and attention. There was no improvement in working memory or psychomotor learning. These participants also improved in unpracticed tests including the Mini-Mental State Examination (MMSE), verbal fluency, and trail making. The participants with MCI improved in 16 of the 21 practiced measures. In contrast to those with AD, they did improve in working memory and psychomotor learning but not in divided attention or tests of perception. In unpracticed tests, those with MCI improved only in behavioral memory. 14 Total training time was still limited in these studies, totaling 6 to 8 hours.
In motor learning literature, it is well established that increased amounts of practice will lead to greater amounts of motor learning. 15 To maximize practice in a short amount of time, one approach used in physical rehabilitation is constraint-induced therapy (CIT), a successful model to regain upper extremity function after stroke. 16 In CIT, the unimpaired limb is restricted to prevent its use, a component not applicable in cognitive training. Other important components of CIT, however, include individualized training with 6 to 8 hours of practice a day for 10 days within 2 consecutive weeks. Another important part of CIT is shaping or increasing the difficulty of tasks as tasks are mastered. 16 Adaptations of CIT have been used with some success to treat language dysfunction after stroke, such as aphasia, 17 –19 and recall in healthy older adults 20 Together, these studies indicate some promise for incorporating aspects of CIT training in improving cognitive function. We were interested in the effects of longer training hours presented in an intense schedule; this increase in practice may produce more robust gains in both practiced and unpracticed cognitive tasks.
In the present study, we applied principles of the CIT model for training attention and memory function in people in the early stages of AD. The principles of an intensive schedule of practice and shaping with individualized training sessions were maintained. Our first aim was to assess feasibility; we hypothesized that participants would be able to participate and complete an intensive schedule of cognitive training. Second, we hypothesized that participants would show significant improvement over training in those cognitive tasks that were practiced. Finally, we hypothesized that improvements would generalize to other cognitive outcome measures that were not practiced.
Methods
Participants
Participants in the study were recruited from the University of Kansas Alzheimer’s Disease Center between 2008 and 2011. Potential participants were recruited if they were diagnosed with very mild or mild AD. The determination of a participant’s status of nondemented aging or early AD was based on clinical methods without reference to psychometric performance. 21 Participants were evaluated by an experienced neurologist with a semistructured interview of both the participant and the informant, usually a spouse or an offspring, to assess the course and characteristics of the cognitive decline. Diagnostic criteria for AD require the gradual onset and progression of impairment in memory and in at least one other cognitive and functional domain. 22 Dementia severity was determined using the clinical dementia rating (CDR) administered by the neurologist. 23 Individuals with very mild (CDR 0.5) and mild (CDR 1) dementia were eligible for the study. These clinical methods have been reported to have a diagnostic accuracy of 93% for predicting the presence of AD neuropathology at autopsy. 24 These methods have been shown to be accurate in identifying the subset of individuals meeting criteria for MCI due to early-stage AD. 21 A board-certified neurologist (JB) specializing in AD provided the diagnosis of AD and the disease stage.
To be included in our study, participants had to be free of any neurological disorder other than AD, be at least 60 years of age, right-hand dominant, and have normal or corrected visual acuity and color vision. A subset of these individuals also volunteered for functional imaging scans; the results of that portion of the study will be reported separately. Participants had to have their own transportation and be willing to come to the medical center daily for 2 weeks. Participants were compensated for transportation expenses and were provided lunch each day they attended. The study was approved by the university Human Subject Committee, and all participants provided oral and written informed consent prior to beginning the study.
Cognitive Training
Individualized training was performed with only 1 participant at a time in a quiet room. Training responsibilities were primarily shared by 3 investigators (SK, YC, and PP), and each participant had 2 of those trainers throughout their intervention. Detailed notes about participants’ performance were used to facilitate shaping. Each participant received training Monday through Friday over 2 consecutive weeks for a total of 10 days. Approximately 1 hour of the first morning and the last day of training were set aside to complete the outcome measures. These were completed by an investigator who did not participate in the training (JM). Participants were generally scheduled from 9
Training included custom computer-based cognitive training exercises adapted from previous work 25,26 and paper-and-pencil tasks. Computer-based activities targeted working memory, sustained attention, switching attention, and divided attention. Each of these training exercises was completed once each day on most days of training. Paper-and-pencil tasks provided practice in planning, memory, visual-spatial processing, sustained attention, and selective attention. Participants received verbal feedback on their performance, and encouragement guided them during each activity. Strategies for improved performance were discussed with participants if they were not progressing.
Computerized Training Tasks
Measures of interest for each computer task are presented in Table 1.
Computerized Training Tasks Measures of Interest.
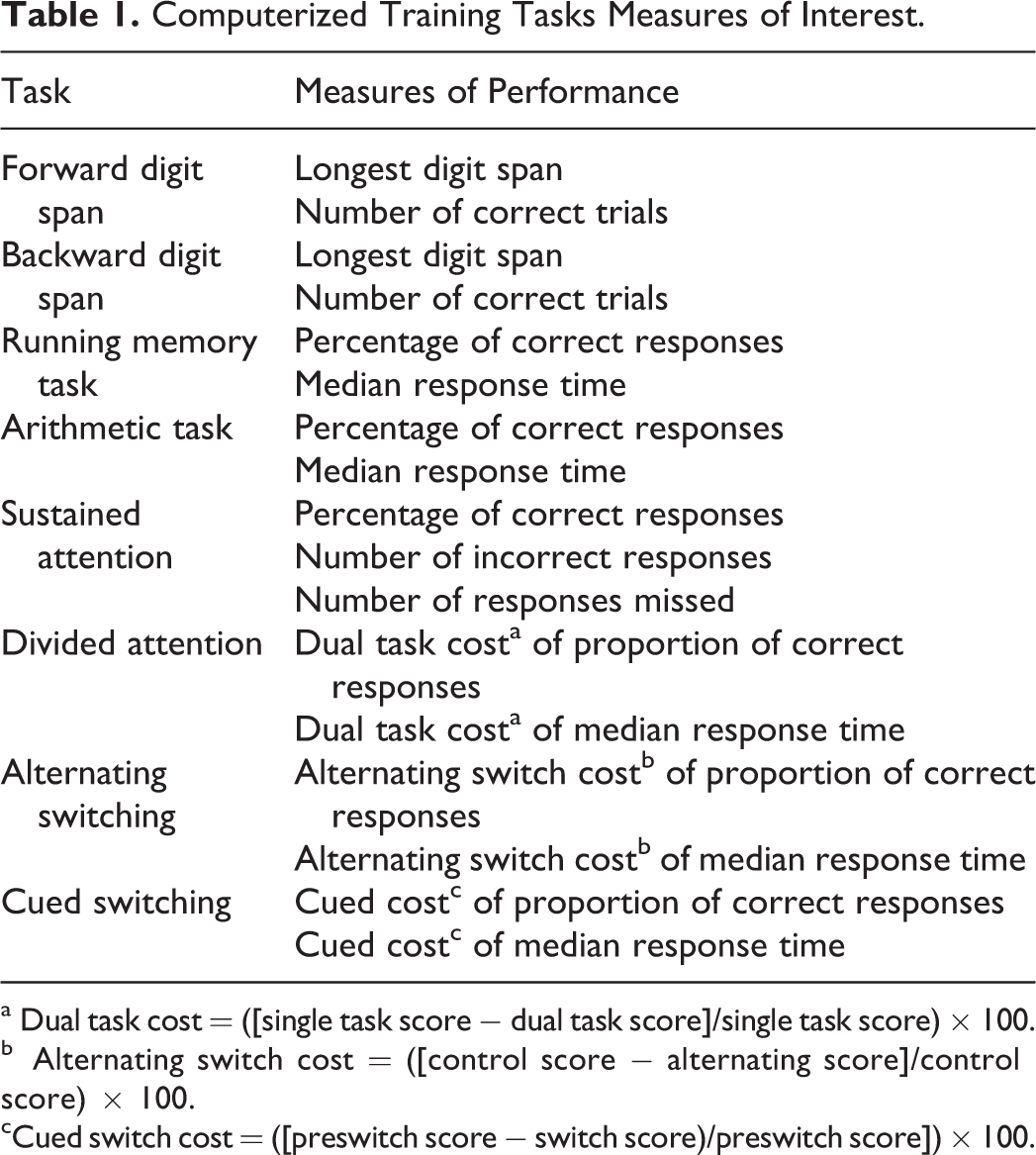
a Dual task cost = ([single task score − dual task score]/single task score) × 100.
b Alternating switch cost = ([control score − alternating score]/control score) × 100.
cCued switch cost = ([preswitch score − switch score)/preswitch score]) × 100.
Working Memory
Forward and backward digit span: Participants were presented with a series of random digits from 1 to 9 on a computer screen and were asked to immediately recall the digits in the same order as presented in the forward digit span and in reverse order in the backward digit span. The number of digits presented was increased by 1 digit if the participant answered at least 1 of 2 trials correctly. Otherwise, the task ended. Running memory task: A continuous 10-minute sequence of letters was presented rapidly one at a time, and the participant had to respond whether the current letter was the same or different from the one just before it. Arithmetic Task: A simple addition or subtraction problem was presented on the computer screen, and the participant had to decide whether the answer was less than or greater than 5 as quickly as possible. The task typically lasted from 10 to 20 minutes depending on the speed of responses.
Sustained Attention
Participants performed a continuous 14-minute task in which numbers from 0 to 9 were presented randomly one at a time on the computer screen. The participant had to press the 0 key when the number 0 appeared on the screen and refrain from responding to all other numbers.
Divided Attention
There were 2 tasks. The first task was a memory task; single letters (A, B, C, D, and E) were presented one at a time on the screen. Six letters were presented randomly in a set and only 1 letter appeared twice. At the end of the 6 letters, the participant was instructed to enter the letter that was repeated using the computer keyboard. The second task was a speeded response task; the participant was presented with the letters that were colored red or green. The sequence of the colors was random. The participant had to press a green or red switch to indicate the color of the letter. The participant was instructed to respond as quickly and accurately as possible. There were 15 trials for each of the single tasks requiring a total of 30 responses which were completed before beginning the dual task.
In the dual task, the 2 tasks were delivered concurrently. The participants were instructed to respond to the color of the letter and to watch for the letter that was repeated. The participants were instructed to respond as quickly and accurately as possible. The participant responded to the color task using the color switches and at the end of the sequence answered which letter was repeated. The dual task was repeated 15 times.
Switching Attention
The switching task consisted of a series of trials in which 1, 2, 3, or 4 identically colored circles were presented on the computer monitor. Participants were instructed to respond as quickly and accurately as possible using custom color switches that were colored to match the circle colors of blue, red, green, or yellow, and numbered from 1 to 4. The participant had to respond to either the color of the circle or circles or the number of circles presented on each trial. Two conditions of switching were used. Practice was organized into blocks which consisted of a predetermined number of trials or responses.
Alternating
Participants had to alternate the type of response (ie, color, number, color, number, etc), or in a control condition, participants had to respond to either the number or the color of the circles without alternating the response. Participants performed 2 blocks of 12 trials each of the control condition and 1 block of 24 trials of the alternating condition. This was repeated twice for a total of 6 blocks which took approximately 10 minutes to complete.
Cued Switching
The type of response (color or number) required was presented as a written cue on the computer screen. Participants were instructed to continue with that response until a new cue appeared. Cues appeared after a variable number of responses (8-12) to reduce the predictability of the change. The participants responded to 4 blocks of 9 trials each of cued switching. The blocks were repeated 8 times and took about 30 minutes to complete.
Paper-and-Pencil Training Tasks
Paper-and-pencil exercises were used to supplement the cognitive training completed on the computer and targeted cognitive functions that were not part of the computer training. The exercises were adapted from various workbooks. 27 –35 Workbooks contained memory exercises including words, paragraphs, word lists, short stories, spatial, and shapes and pictures memory exercises with variable temporal memory retention including immediate, short, and long-term memory. We incorporated problem-solving tasks and different types of reasoning tasks including abstract and deductive reasoning. Other tasks in the training were concrete and abstract categorization, sequential and expressive organization, word list associations, and following written and oral directions. These tasks were tailored for each individual participant with harder versions of a task provided when easier versions were mastered. Approximately 2 hours per day were devoted to these exercises. Typically, computer tasks were split between the morning and the afternoon sessions and done first within each session. Paper-and-pencil training tasks were done during the remaining time in each session. Data from paper and pencil tasks were not recorded for statistical analysis.
Outcome Measures
The primary measures of interest were standardized assessments not specifically part of the training. The battery of neuropsychological assessments included the Wechsler Logical Memory Test, 36 category fluency, 37 letter fluency, 38 the MMSE, 39 and the Delis-Kaplan Executive Function System (D-KEFS) Trail-Making Test 40 , including the 5 components: visual scanning, number sequencing, letter sequencing, number-letter switching, and motor speed. In addition, participants completed the Quality of Life-AD (QOL-AD) survey. 41 Outcome measures were administered on the first day of training and on the last day of training. Two additional follow-up testing sessions were scheduled 2 and 4 months after the conclusion of training.
Data Analysis
Computerized Training Tasks
Each participant performed the computer activities for a minimum of 8 days of the 10 training days. Data from the first day of practice, when participants first became familiar with each activity, were not used for analysis. Since we had at least 8 days of practice data for each participant, the slope of performance for each participant for each task was calculated over the next 7 days of practice. To determine whether participants improved with practice, 1 sample, 1-tailed student t tests were used to assess whether the slopes were significantly different from 0.
Outcome Measures
The assessments were scored according to published protocols. Category and letter fluency performance were scored in terms of number of words generated in a 60-second trial. One-tailed paired t tests were used to determine whether participants improved from baseline to the end of training. Although not a primary outcome of our study, if significant improvements were made over training, 1-way repeated measures analyses of variance (ANOVA) were conducted to examine changes from the end of training to 2- and 4-month follow-ups to determine whether the improvements were sustained over time. Post hoc comparisons of compare baseline performance to follow-up performance were also completed.
PASW Statistics 20 (SPSS, Inc, 2009, Chicago, Illinois) was used for all statistical analyses. The significance level was set at P < .05.
Results
Twenty-one adults in the early stages of AD enrolled and completed the study. Four had mild AD with a CDR score of 1.0; the remaining had very mild AD with a CDR score of 0.5. Participants’ characteristics are provided in Table 2. All participants were able to participate in the intensive, 2-week cognitive training, although 2 participants missed one day of training due to medical appointments and 1 participant missed the last day of training due to an unrelated hospital admission. One participant missed 2 days of training due to inclement weather but made up the days in the third week. Total training time ranged from 40 to 50 hours. At the 2-month follow-up, 18 of the 21 participants were available for testing. At the 4-month follow-up, 20 of the 21 participated in testing.
Participants’ Characteristics.
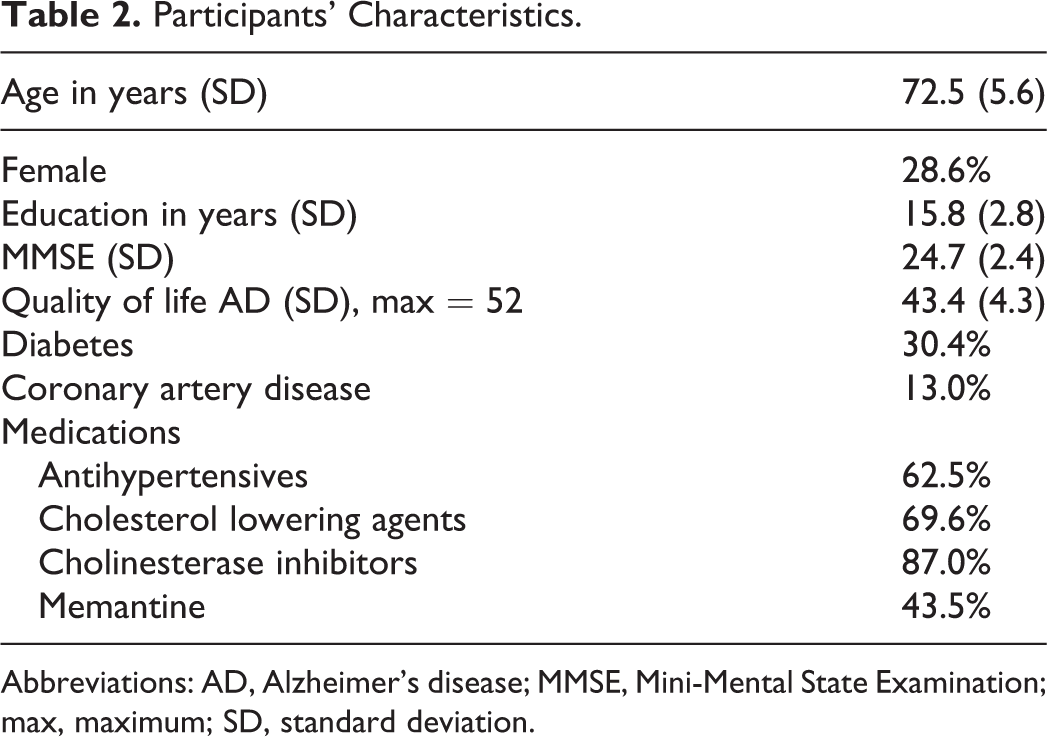
Abbreviations: AD, Alzheimer’s disease; MMSE, Mini-Mental State Examination; max, maximum; SD, standard deviation.
Computerized training tasks were completed between 7 and 9 times overall but not more than once per day. The variability in the practice time for any particular task was due to the nature of the individualized training program, with less time for tasks that were mastered and more time devoted for tasks that were difficult.
Computerized Training Tasks
A summary of changes over practice as indicated by the slope of performance is provided in Table 3.
Data Summary and Slope of Performance Over 7 Days of Training.a
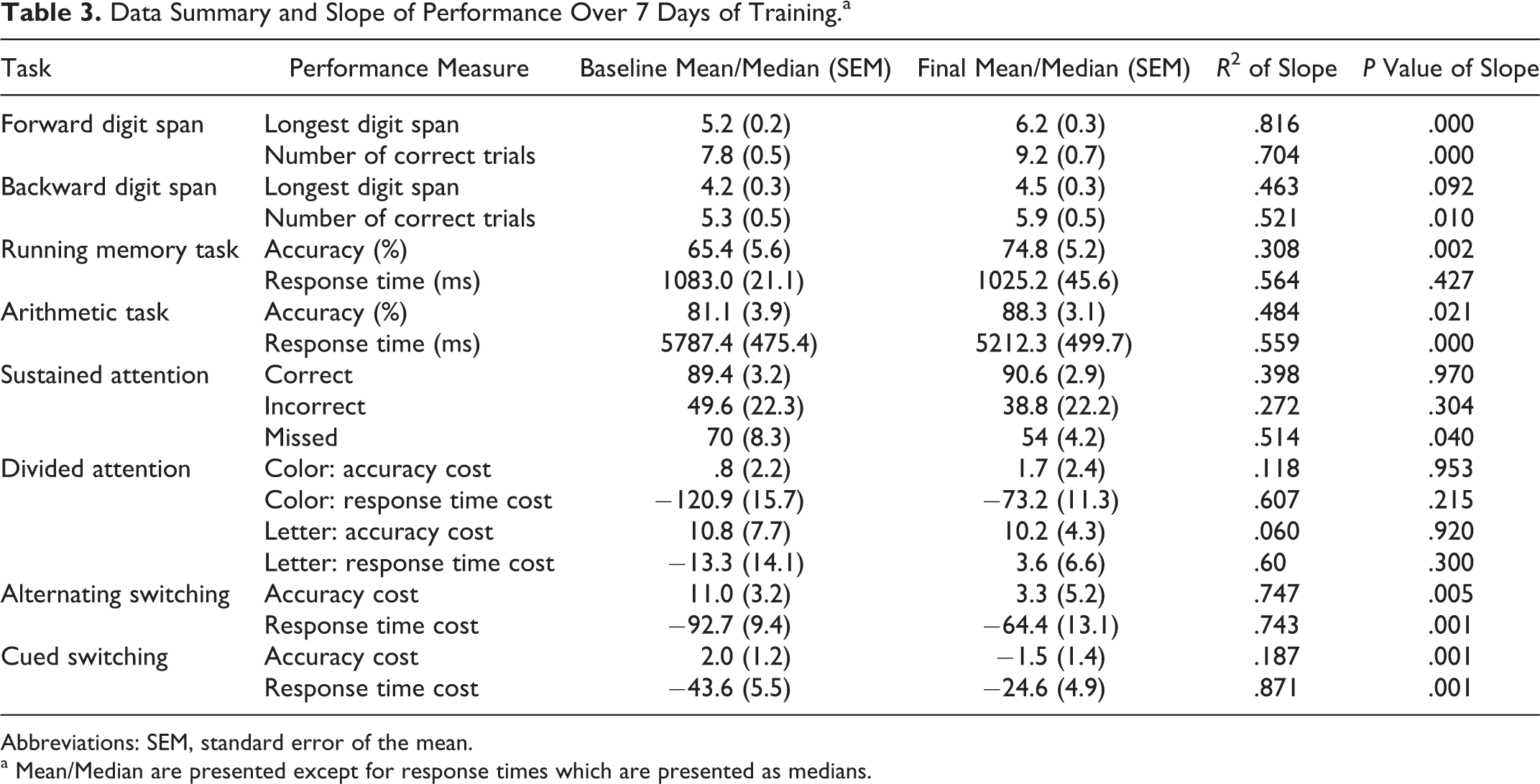
Abbreviations: SEM, standard error of the mean.
a Mean/Median are presented except for response times which are presented as medians.
Working Memory
Participants significantly improved in the number of correct trials for the forward digit span (P = .000) and backward digit span (P = .01) and in the length of sequence in the forward digit span (P = .000). In the running memory task, participants did not alter their response times but improved their accuracy from 65% ( standard deviation [SD] = 25.7) to 75% (SD = 23.8); this change was significant, P = .002. In the arithmetic task, participants became more accurate (P = .021) and faster (P = .000) with practice.
Sustained Attention
There were no significant changes in the percentage of correct responses or in the number of incorrect responses. Improvement was seen in the number of missed 0 which significantly decreased with practice, P = .04.
Divided Attention
Analysis of the cost of doing both tasks revealed that there were no significant changes in divided attention costs in either accuracy or response time for either task with practice.
Switching Attention
Alternating Switching
Following the training, participants improved both their accuracy and their response time in the alternating condition as revealed by the significant changes in switching cost for accuracy (P = .005) and response time (P = .001).
Cued Switching
Analysis of the slope of cost of switching showed significant decreases in cost for both accuracy (P = .001) and response time (P = .001).
Outcome Measures
Performance after training was better than baseline for some of the tests in the outcome measures, specifically the MMSE scores, letter fluency, and 3 of the trail-making tasks: visual scanning, number sequencing, and letter sequencing (Table 4). There was no change in the Logical Memory test and 2 of the trail-making tasks: number-letter switching and motor speed. A significant decline in performance was found in 1 measure, category fluency. For those outcome measures that did significantly improve from baseline to posttraining, the posttraining scores were compared to those at 2- and 4-month follow-ups (Table 4) using 1-way repeated measures ANOVAs. There were no significant changes in scores from posttraining to follow-ups.
Mean and Standard Deviation of Outcome Measures at Each Time Point; P Values for Baseline to Posttraining Comparison.
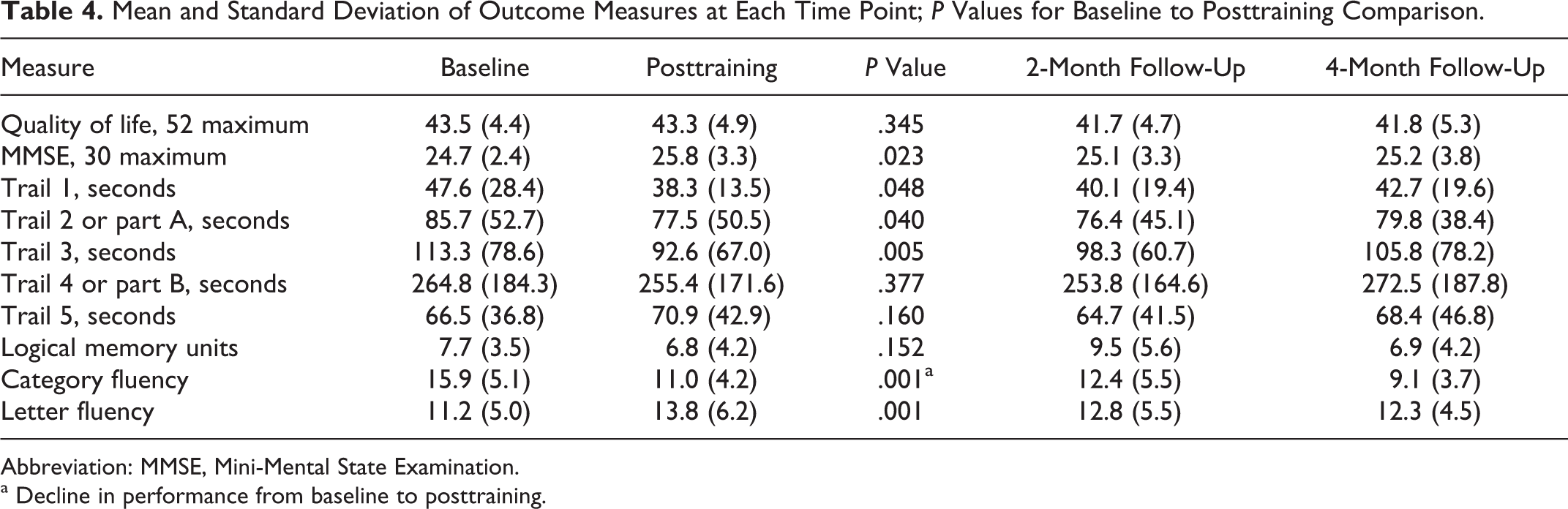
Abbreviation: MMSE, Mini-Mental State Examination.
a Decline in performance from baseline to posttraining.
The comparison of baseline to follow-up scores revealed no significant difference in the MMSE score. Letter fluency at follow-up was significantly better than baseline but only at the 2-month test. For the visual scanning, number sequencing, and letter sequencing components of the Trail-Making Test, only performance on visual scanning remained faster at follow-up, and this was significant at both 2- and 4-month testing.
Discussion
To our knowledge, this study is the first to investigate the feasibility of an intensive schedule of cognitive training in participants in the early stages of AD. The results of this study support the first hypothesis that participants can participate and complete an intensive cognitive training program. A challenging part of this program was the long hours of cognitive training which can cause physical and mental fatigue. 4 Despite the rigors of long training sessions, our participants with AD were able to complete 4 to 5 hours of training each day for a total of 40 to 50 hours of cognitive training. Participants did not complain of undue fatigue at the end of a day of training, and continued efforts throughout the day seemed to be facilitated by the variety of activities and the one-on-one training. Other studies that have reported successful less intensive cognitive training for those with AD for a total of 36 to 45 hours spread the sessions out over 6 weeks 42 to 6 months. 43 It is not known whether the intensive schedule of practice is better for training than shorter sessions, but it does appear that day-long cognitive training sessions can be successful, at least for a subset of those with mild or very mild AD.
One of the advantages of shaping is that each session is focused on appropriate cognitive tasks. Easy tasks were introduced first with the difficulty of the tasks gradually increasing as participants were successful and gained mastery. Participants were given feedback on their performance and improvements from previous sessions. Delivering the training in both paper-and-pencil and computerized forms helped hold the participants’ attention and likely aided as a motivation to complete the training. If participants lost focus, became frustrated, or fatigued with 1 activity, the one-on-one training program provided avenues for modifications with the cognitive tasks planned for the session. This design likely facilitated participants’ compliance and participation.
Our second hypothesis that participants would show significant improvement over training in practiced tasks, was partially supported. Participants with mild and very mild AD improved in all but one of the computer-based cognitive tasks that were practiced daily. The participants in this study improved in the computer tasks that involved working memory, sustained attention, and switching attention tasks. Improvements in memory with cognitive training have been reported for healthy elderly individuals, 6,7,44 those with age-related cognitive impairment, 9 MCI, 11,45,46 and probable AD. 8 Less is known about cognitive training effects for those with AD on sustained and switching attention. Sustained attention and switching attention are important cognitive abilities, and participants with AD have deficits in sustained attention 47 and switching attention 48 when compared to age-matched healthy controls. Adults with MCI have demonstrated improvement in switching abilities when those tasks were practiced 48 and even when not specifically practiced in the training. 13 In contrast, participants with mild to moderate AD have not improved switching abilities with practice. 48 Similar to reports of those with MCI, our group of early AD participants did improve switching abilities with practice, which may have been due to the intensive schedule of practice or the early stage of AD of our participants.
Of the practiced computer tasks, only the divided attention task performance remained unchanged. It is not clear why participants failed to show expected practice effects in this task. Improvements with practice in divided attention tasks have been reported for participants with MCI 12 –14 and those with AD. 14 It is possible that our task was too easy and left little room for improvement. Accuracy was high for the color responses in both the single and the dual task situations resulting in a small cost calculation. Even so, participants could have gotten faster with practice, as they did in the arithmetic task, alternating switching, and cued switching. Each computer task was practiced no more than once per day. There was a tendency for faster response times with practice in the divided attention task; analyses of the slopes of response times resulted in an R 2 of .6 for both color and letter, but these changes were not significant.
In addition to improvements at practiced tasks, a broader benefit of cognitive training would be evident if improvements were more generalizable or found in global measures of cognition. Our third hypothesis, that improvements would be found from baseline to post-training in cognitive activities not practiced, was partly supported. Some positive gains in cognitive performance for those with AD in cognitive tasks that were not part of the computer activities practiced daily were seen. A significant improvement was found in the MMSE from the baseline average of 24.7 (2.4) to the posttraining average of 25.8 (3.3), an average increase in 1.1 points. In addition, there was no significant loss in MMSE score at 2 and 4 months after training was complete, with scores declining slightly at 25.2 (3.2) and 25.5 (3.8), respectively. To understand the impact of the magnitude of this decline, a post hoc analysis was done to compare the MMSE score at baseline with the 2- and 4-month scores. There was no significant difference, suggesting that the gain made in the MMSE at posttraining was not sustained. Our results for posttraining improvements were similar to the adults with MCI who underwent cognitive training, demonstrating an increase of 0.9 in the MMSE from 28.1 to 29.0. 46 Other studies have reported maintaining MMSE scores 49 or have reported larger gains in MMSE in participants with lower baseline scores than our participants. Adults with AD who were treated with cognitive training and donepezil had an average baseline MMSE of 17.1 that increased to 20.8 following intervention. 50 It may be that individuals with lower MMSE scores who participate in cognitive training can make larger gains in their scores than those in the early stages of AD.
Participants improved in the letter fluency test, a task that was not practiced in the 2 weeks of training. At 2- and 4-month follow-up testing, the score achieved at the end of training declined, albeit slightly; the 2- and 4-month scores were not different from the post-training score. Post-hoc analyses revealed that the score at 2 months was significantly better than the baseline score, but this difference was lost at the 4-month follow-up. Improvements in letter fluency were not mirrored in the category fluency test where performance became significantly worse in posttraining compared to baseline. The letters and categories given to participants were standardized, differed between testing sessions, and randomized between participants. Other work has also shown greater AD-related impairment in category fluency compared to letter fluency, suggesting that the semantic fluency task may be the more difficult one for people with AD. 51
In the D-KEFS Trail-Making Test, significant improvements were made in some but not all components of the test. Participants improved in visual scanning, number sequencing, and letter sequencing but did not change their performance in the most complex portion of the test, the number-letter switching task known as part B, or in motor speed. The lack of change in the motor speed component supports a cognitive underpinning to the faster performance in the number and letter sequencing tasks, supporting a positive effect of the training program. Interestingly, poor performance for those with mild AD on the sequencing portion of the test, also known as part A in the literature, has been associated with greater functional deficits in activities such as preparing a meal or handling finances. 52 Our participants did improve their speed in sequencing, but there was no change in their QOL as measured by the QOL-AD scale. Other studies have reported that participants with AD who participated in cognitive training were able to decrease their errors in part B of the Trail-Making Test, 14 a measure that we did not analyze in our study. Not all studies have shown cognitive improvements in tasks that were not practiced. 8,53,54 Changes in functional activities or QOL have been demonstrated in few studies. Some improvement in daily activities was found for a group of healthy elderly individuals who participated in reasoning training 36 and for those with MCI who participated in a program including cognitive training, cognitive stimulation, and psychotherapeutic intervention. 46 Faster times to perform activities of daily living were achieved following a procedural memory training program for adults with mild and mild to moderate AD. 55 In the current study, no changes were detected in QOL, and functional abilities were not assessed.
There were limitations in the current study. With our focus on feasibility, we did not complete a power analysis to determine sample size, and we did not have a control group to determine whether the intensive practice schedule results in greater cognitive improvements compared to a more traditional practice format. Given the number of statistical comparisons, the results should be interpreted with caution, and statistical differences may not be clinically significant. The individual who participated in this study limits the generalizability of the results. The sample size was small and predominantly male. Our participants were highly educated, which may have affected their performance in the training. The day-long schedule of practice is very labor intensive. On most days, 1 researcher was available for the morning session and another for the afternoon session. To continue such a schedule over time, although not impossible, would require substantial personnel resources. Our follow-up data were restricted to the outcome measures. It is not known whether participants maintained improvements in the computer-based tasks after the training concluded. Finally, we have no data on the translation of the measured improvements in cognitive tasks to the everyday lives of our participants. Studies that have paired cognitive training with pharmacological interventions have shown some benefit of the combination of these treatments. 49,56 We did not monitor or control participants’ pharmacological treatments during the course of the study, treatments which may have influenced the participants’ response to cognitive training.
Conclusion
Our results suggest that high-intensity, short duration cognitive training is feasible in individuals in the earliest stages of AD and results in clear training-related improvements in practiced tasks. Moreover, modest cognitive benefits were present in unpracticed tasks suggesting some carryover to more generalizable cognitive domains, with some evidence of durability of these benefits at 2- and 4-month follow-up. These findings support further development and testing of the effectiveness of cognitive training in those with cognitive impairment.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an Investigator-Initiated Research Grant from the Alzheimer’s Association [IIRG-07-57789] awarded to PSP; ClinicalTrials.gov identifier: NCP00611312.