
Abstract
The Chanwuyi Lifestyle Medicine Program (CLMP) was found to enhance the memory and executive functions of older adults with or without subjective memory complaints. The present study investigated whether similar beneficial effects can be extended to mild cognitive impairment (MCI). Twenty-four older adults with MCI were randomly assigned to receive the CLMP (the experimental group) or strategic memory training (SMT; the active control group) for 10 weeks. They were assessed by neuropsychological tests at baseline and post-intervention. Older adults showed similar visual and verbal memory improvements after receiving the CLMP and SMT. Yet, only those who received the CLMP showed distinct improvements in planning/organization, working memory, and attention in terms of accuracy, with greater cognitive gains associated with older age and lower levels of education and baseline cognitive functions. This study provides preliminary evidence for the effects of the CLMP on improving memory, attention, and executive functions in MCI.
Keywords
Significance Statement
• Chanwuyi Lifestyle Medicine Program (CLMP) enhanced executive functions in mild cognitive impairment (MCI) • CLMP elicited a larger improvement in attention than strategic memory training (SMT) • CLMP was equally effective as SMT in enhancing visual and verbal memory in MCI
Introduction
Mild cognitive impairment (MCI) is considered a transitional stage between healthy aging and dementia, which affects approximately 15%–20% of adults aged 60 years and older. 1 Although individuals with MCI experience subjective cognitive deterioration and some of them show impaired performance on some objective cognitive tests, they can mostly live independently.2,3 Nevertheless, they have a higher risk of developing into dementia, with an annual conversion rate of approximately 8%–15%1,4 and around 30% conversion in 2 to 5 years.5,6 Impaired episodic verbal memory is a common clinical symptom detecting MCI and very early Alzheimer’s disease (AD)7,8 and predicting abnormal cognitive decline.7,9 Along with episodic memory, executive functions that are mediated by the frontal brain regions may be impaired preceding or coexisting with episodic memory deficits in MCI. 10 Executive function deficits significantly predict conversion from cognitively normal status to MCI11,12 and from MCI to dementia.13,14 In particular, executive functions of switching, category generation, and planning best distinguished between MCI converters and MCI without further progression. 14 Therefore, intervention that can effectively enhance episodic memory and executive functions may delay further cognitive decline, or may even prevent the development of dementia.
Vigorous research has been focusing on cognitive training for slowing cognitive decline or enhancing cognitive functions of MCI. Strategic memory training (SMT) is one of the most frequently studied interventions for patients with MCI and older adults at risk for MCI or dementia with promising memory-enhancing effects.15-24 SMT is an evidence-based training that teaches external and/or internal strategies to compensate for existing forgetfulness and to facilitate encoding, consolidating, and retrieval in memory processes. Repeated empirical evidence suggests that training focused on superordinate memory strategies and strategies in everyday life can facilitate objective memory performance in older adults with normal cognitive status,15,17,25 subjective memory complaints (SMC),22,23 and MCI.15,17,19,21,24 SMT helps older adults with MCI to store memories more efficiently and improve their retrieval process. Its memory-enhancing effect can be extended to non-practiced memory tasks (i.e., a near-transfer effect). 21 Nevertheless, whether SMT has a far-transfer effect (that is improving cognitive functions other than memory, such as attention and executive functions) remains controversial. A review of cognitive intervention programs for individuals with MCI concluded that teaching well-established mnemonic skills demonstrated statistically significant post-training improvements on 44% of memory measures but on only 12% of measures of other cognitive functions (such as attention, processing speed, and executive functions). 26 While some studies have evidenced positive effects of memory training on improving attention, 22 processing speed, 20 fluency of speech,23,24 and working memory 27 of older adults with normal cognitive status, SMC or MCI, other studies find only modest or null positive effects.21,28
In recent years, research has been focused on identifying modifiable risk factors affecting the conversion from MCI to dementia29-32 and protective factors facilitating reversion from MCI to normal cognitive status.33-36 The 2017 and 2020 Lancet Commission on dementia prevention,31,32 intervention, and care has identified 12 modifiable risk factors that account for around 40% of potentially preventable or deferrable dementias. Most of those risk factors (including hypertension, obesity, diabetes, depression, physical inactivity, low social contact, smoking, and excessive alcohol consumption) could potentially be modulated by changing one’s lifestyle behaviors. An observational longitudinal study following 769 older adults with MCI for 4 years revealed that older adults who continued to engage in integrated lifestyle activities and started new activities were more likely to revert from MCI to normal cognitive status. In contrast, converters were likely those who discontinued integrated lifestyle activities or were inactive. 37 It is believed that lifestyle interventions targeting reducing negative and promoting positive modifiable factors, such as diet, exercise, cognitive-stimulating activities, psychosocial health, and avoidance of harmful substances, may delay, prevent, or even revert progression to dementia.
An emerging line of research has investigated the effectiveness of lifestyle interventions in improving cognitive functions or preventing the cognitive decline of individuals with MCI, and the intervention outcomes are so far positive.38-43 For instance, an APOE ɛ4 homozygous carrier with MCI underwent a 4-year lifestyle intervention and showed significantly improved verbal memory and global cognitive functions. 43 A personalized therapeutic lifestyle intervention program (including modification of dietary, exercise, and sleep habits, management of stress, and engagement in cognitively stimulating activity) helped improve and reverse normal cognitive functions and occupational functioning in several patients with amnesic MCI within 3-6 months. 38 Marked improvements could be sustained after 2.5 years. In a 6-month randomized controlled trial (RCT), 80 older adults with MCI were randomly assigned to a Chinese integrative lifestyle intervention group or a treatment-as-usual control group. 40 After 6 months, older adults who received lifestyle intervention showed significantly greater improvement in global cognitive function than those in the control group. In another 12-month cluster RCT, 41 older adults with MCI-single domain deficit showed significantly greater improvements in their global cognitive functions and delayed memory recall after receiving an integrated lifestyle intervention. Another study also found significant improvement in global cognitive function in hypertensive adults with or without MCI after 2 years of lifestyle intervention administered alone or in combination with medication. 42
The Chanwuyi Lifestyle Medicine Program (CLMP) is an eastern-western integrative lifestyle intervention designed to improve cognitive functions and physical and psychological health. The model of the CLMP adheres to the definition of lifestyle medicine proposed by the American College of Lifestyle Medicine (ACLM) is an evidence-based approach comprising a predominantly whole food, plant-based diet, regular physical activity, stress management, adequate sleep, avoidance of risky substances and/or positive social connections for preventing and treating lifestyle-related chronic disease. 44 There are over 15 years of scientific evidence for the promising therapeutic effects of the CLMP on older adults with and without memory problems,45-48 adults with depressive mood 49 or major depressive disorders,50-52 and children with autism spectrum disorders (ASD).53-59 As a result, the CLMP was accredited by the ACLM as a certified lifestyle medicine program in 2021.
Specifically, a series of empirical studies on older adults with normal cognitive status 45 and those with SMC46,47 have found significant improvements in their objective memory performance after the CLMP. In the study of Chan et al., 45 44 healthy older adults with various levels of memory ability participated in a 12-week CLMP. Older adults with lower baseline memory function showed a reliable and clinically significant enhancement in verbal (50% improvement) and visual (49% improvement) memory performance. Their extents of memory improvement were greater than those with a medium to high level of baseline memory. It suggests that the CLMP can benefit older adults with a lower level of memory functioning. Further RCT study was performed on 56 older adults with SMC and found similar visual and verbal memory improvements after 10 weeks of the CLMP, to a degree similar to the training on teaching memory strategies. 46 Such beneficial effects could be sustained after 18 months. 47 In addition to the positive memory effects, repeated empirical evidence has supported the therapeutic effects of the CLMP on improving executive functions, such as flexible thinking in older adults with normal cognitive status, 45 inhibitory control, flexible thinking, and planning in children with ASD,53-56,58,59 and improving attention and emotional control in patients with depression.50,52 In specific, a 3-month CLMP significantly improved the flexible shifting of mental sets in normal older adults. 45 Patients with depression also showed better attention with a faster processing speed after 10 weeks of the CLMP. 50 Children with ASD receiving the CLMP for 6 months demonstrated better impulse control, more flexible thinking, and better planning after training. 59
The potential mechanisms underlying the CLMP effects on enhancing the cognitive functions of an individual could be related to its comprehensive approach in modifying multi-faceted life habits and living attitudes, from adopting a healthy whole-food plant-based dietary intake, being physically active, to managing stress and attaining emotional well-being by gaining self-awareness, cultivating gratitude and compassion, and fostering a peaceful mind through practicing the mind-body exercise called Nei Gong. All these components are positive modifiable lifestyle factors that are found to benefit the physical and mental health as well as the brain’s health, and that combat the risk factors for cognitive decline identified by the Lancet Commission on dementia prevention, intervention, and care.31,32 In addition, empirical studies on children with ASD has suggested the potential of the CLMP for cognitive enhancement by increasing the brain activity and connectivity of neural circuits mediating memory and executive processes. For instance, an elevated EEG theta coherence between frontal and posterior brain regions during a memory task was found in children with ASD who showed improvement in memory performance after receiving a 1-month training on Nei Gong. 57 Other EEG studies on the effects of the CLMP or a component of the CLMP also demonstrated an increase in event-related EEG activity in the prefrontal cortex and anterior cingulate cortex (brain regions mediating executive functions) associated with improved executive functions after the intervention.55,56,59
Although the CLMP has been found to benefit the memory and executive functions of cognitively normal older adults and those with SMC, the effects of CLMP on MCI remains largely unknown. Therefore, the present study aims to examine whether the CLMP can also enhance memory, executive functions, and attention of older adults with MCI. It is anticipated that older adults with MCI will demonstrate improvements in visual and verbal memory after receiving the CLMP, and their extent of memory improvements may be similar to those who have received training on memory strategies. In addition, the CLMP is also anticipated to benefit older adults with MCI in executive functions (i.e., working memory and planning/organization) and attention that are highly associated with learning and memory processes. As compared to older adults receiving memory training, those who received the CLMP will probably show a greater extent of improvement in executive functions and attention. This study may shed some light on the effectiveness and applicability of the MCI population.
Materials and Methods
Participants
Forty older adults aged between 61 and 79 were recruited from community health and social centers in the New Territories East regions in Hong Kong and through newspaper advertisements. The sample size was determined by power analysis based on the statistics of previous studies examining the CLMP effects on memory 46 and executive functions.51,59 With an alpha value of .05, a power of .8, and effect sizes ranging from .91 to 1.01, the minimum number of subjects per intervention group should be 10 to 12. To buffer for dropouts and cases not fulfilling the diagnostic criteria of MCI, the sample size was targeted at 40. To screen for older adults with MCI, they were individually assessed with a battery of comprehensive neuropsychological tests on their cognitive functions and standardized questionnaires/scales on their functional abilities and psychological functioning before the intervention by trained research assistants blinded to the experimental design.
The inclusion criteria for MCI were based on the definition of National Institute on Aging-Alzheimer’s Association workgroups, 2 which include: (1) a concern regarding a change in cognition; (2) an objective cognitive impairment; (3) preservation of independence in functional abilities; and (4) not being demented. The concern about the change in cognition was indicated by their above-cutoff total score (i.e., 3 or above) on the Abbreviated Memory Inventory for Chinese (AMIC), 60 which suggests significant subjective memory complaints. Objective cognitive impairment was defined as a score of more than 1 SD below the age- (and education-) corrected normative mean on at least one of the standardized neuropsychological tests, tapping cognitive functions of memory, attention, executive functions, language, and visuospatial perception. The Hong Kong List Learning Test (HKLLT) 61 and the Visual Reproduction subtest of the Wechsler Memory Scale, 3rd edition (WMS-III VR) 62 were adopted as measures of verbal and visual memory respectively. The Shape Trail Test – Trail A (STT-A) 63 was adopted as a measure of attention. For the executive functions, the Copy trial of the Rey-Osterrieth Complex Figure Test (RCFT) 64 was used as a measure of planning/organization. The language abilities in terms of fluency of speech and object naming were measured by the Category Fluency Test (CFT) 65 and the Boston Naming Test (BNT) 66 respectively. The Copy trial of the WMS-III VR (Wechsler) 62 was adopted as a measure of visuospatial function. The older adults’ level of independence in functional abilities was screened and measured by the self-report version of the Activities of Daily Living-Instrument Prevention (ADL-PI-Self). 67 Signs of dementia were suggested by their performance on the Chinese version of the Mattis Dementia Rating Scale (CDRS) 68 and the battery of neuropsychological tests. The CDRS evaluates the global cognitive function of older adults in terms of attention, memory, conceptualization, initiation/perseveration, and construction abilities. Older adults with a below-cutoff age- and education-adjusted CDRS composite score or those with significant impairments across all 5 cognitive domains measured by the neuropsychological tests were suggestive of having signs of dementia. Exclusion criteria were as follows: (1) positive history of head injury or neurological/psychiatric disorder; (2) detected signs of dementia (as defined above); (3) a score higher than 7 on the short form of the Chinese Geriatric Depression Scale (CGDS-SF)69,70; and (4) a score higher than 15 (i.e., in the moderate or severe range) on the Beck Anxiety Inventory (BAI). 71
Based on the inclusion and exclusion criteria, seven older adults did not meet the inclusion criteria while 5 older adults were excluded due to signs of dementia after screening at the baseline. The remaining 28 older adults met the abovementioned criteria of MCI. 2 They generally maintained their independence of functional abilities in daily life, with minimal aids or assistance required. Informed written consent was obtained from each older adult before the study. The study was conducted in accordance with the Helsinki Declaration of the World Medical Association Assembly. This study was approved by the Joint Chinese University of Hong Kong – New Territories East Cluster (CUHK-NTEC) Clinical Research Ethics Committee (CREC Ref. No.: 2015.337).
Instruments and Materials
At the baseline, the older adults were assessed individually by well-trained research assistants on their memory and memory-related cognitive functions (i.e., attention, planning/organization, and working memory) using standardized neuropsychological tests and a digit n-back task paradigm. Their test performances represent the outcome measures of the intervention effect. After the intervention, older adults were re-assessed by the same set of tests. The details of the outcome measures on various cognitive functions are stated below.
Learning and Memory
The older adults were assessed on their verbal and visual memory functions using the HKLLT 61 and the WMS-III VR 62 respectively. In the HKLLT, they were required to remember a list of 16 Chinese words across three learning trials and to recall the words after 30 minutes. The total learning score and delayed recall score were computed. In the WMS-III VR, they were asked to remember 5 sets of simple geometric forms and draw them from memory immediately after the presentation and then 30 minutes later. The immediate recall score and delayed recall score were computed. A higher score indicates better learning and memory.
Attention
The attention ability of the older adults was assessed by the STT-A63 and the 0-back condition of an n-back task paradigm.72,73 In the STT-A, they were required to connect 25 numbers, which were randomly arranged on a paper, in ascending order by drawing a line between numbers. The time in seconds taken to complete the task was recorded. The shorter the completion time, the better the performance.
The n-back task is a paradigm testing attention and working memory. It consisted of the 0-back (i.e., low working memory load) and 2-back (i.e., high working memory load) conditions. The 2 tasks were performed alternately in blocks for three rounds (i.e., either 0-2-0-2-0-2 or 2-0-2-0-2-0), each block separated by a 30-s rest block during which the older adults were instructed to relax to avoid fatigue. The order of the 0- and 2-back blocks was counterbalanced across older adults to avoid order effects. At the beginning of each task block, a 5-s instruction cue was presented at the center of a computer screen, followed by a display of a single digit for 20 trials (5 target and 15 non-target trials) in a pseudo-randomized order. Each digit appeared on the screen for 1 s, followed by an inter-stimulus interval of 1 s.
In the 0-back condition, the older adults were required to press the left mouse button if the digit was 0 (target) and press the right button for any other non-targeted digit. Given the unequal numbers of target and non-target trials, the nonparametric index of sensitivity A’ was computed to reduce the influence of response biases. 74 A’ takes into account both the hit rate (H) and the false alarm rate (FA). For H ≥ FA, this index is calculated as (.5 + [(H – FA) (1 + H – FA)]/[4H (1 – FA)]); whereas for FA ≥ H, this index is calculated as (.5 – [(FA – H) (1 + FA – H)]/[4FA (1 – H)]). The range of 0-back A’ is 0 to 1, and a larger 0-back A’ suggests better discriminability and attention.
Executive Functions
The Copy trial of the RCFT 64 was used as a measure of planning and organization. It required old adults to reproduce a complex geometric figure as accurately as possible. Given the high complexity of the task figure, the reproduction of such a complex figure involves cognitive processes of strategic planning and organization of a fractional figure into a meaningful perceptual one, which is related to executive function skills.75-78 The copy score was also found to be a sensitive measure of executive function deficits in patients with MCI. 79 The RCFT copy score was computed in terms of accuracy. A higher score indicates better planning and organization.
In the 2-back condition of the n-back task, the older adults were asked to press the left button if the current digit was the same as the digit presented 2 trials back (target) and press the right button if it was not (non-target). The 2-back condition elicits a higher working memory load, during which the individual has to keep the digits presented 2 trials back online and keep updating the memorized digits as the task progresses. Therefore, it requires more effortful executive control that highly relies on the functions of the frontal lobe. Similar to the 0-back condition, the 2-back A’ was computed. A larger 2-back A’ suggests better working memory ability.
Intervention
After the screening and assessment at the baseline, 28 older adults with MCI were randomly assigned into 2 intervention groups receiving 10 weekly sessions of either the CLMP (n = 14) or the SMT (n = 14). However, 2 older adults from each intervention group dropped out of the intervention with an attrition rate of 14.3%. Therefore, the final statistical analyses were based on 12 older adults from each of the 2 groups. The mean attendance rates (i.e., number of classes attended in proportion to the total number of classes) for the 2 groups were over 80% (CLMP: 83%; SMT: 84%) and comparable (t (22) = .22, P = .83). The 2 intervention groups were designed to parallel each other concerning their duration (i.e., 10 sessions, 1.5 hours each) and frequency of sessions (i.e., once a week), group size, in-session sharing, and discussions. The interventions were administered by 2 different clinical psychologists who had over 10 years of clinical experience and their progress was closely monitored by the therapist.
Chanwuyi Lifestyle Medicine Program
The CLMP was developed based on Chanwuyi, including the Chinese Chan tradition, Nei Gong (i.e., mind-body exercises), and the Chan medical principle. The CLMP aims to enhance cognitive functions and improve physical and psychological health through modification of lifestyle habits. Older adults learned the fundamental principles and practiced the CLMP techniques in the intervention sessions and at home. The Chinese Chan medical concept consists of four core elements, coincidentally similar to Western lifestyle medicine, that is diet, physical activity, stress management, and emotional well-being. However, Chinese Chan has its unique elements in the four core elements of lifestyle medicine. For instance, the CLMP encouraged the older adults (1) to adopt a healthy balanced diet that is incorporated with Chan medical concepts, including a whole food, plant-based diet with a high intake of whole grains, fruits, and vegetables from five color groups, legumes, and nuts; (2) to enhance physical health by modifying one’s diet through reducing the intake of food that generates excessive internal heat, such as chives, ginger, garlic, spicy food, and avoiding processed food, saturated fat, and trans fat; (3) to alleviate psychological distress and cultivate better emotional well-being by understanding the root of problems, thinking positively, and being grateful and compassionate; and (4) to manage stress by practicing the mind-body exercise, Nei Gong, and maintaining a physically active lifestyle. Nei Gong is some gentle and slow bodily movements to facilitate Qi and blood circulation, enhance muscle strength and joint flexibility, and attain a peaceful mind and better self-control.56,80
Strategic Memory Training
The training principles and techniques of the SMT were derived from Troyer et al.’s study. 81 The SMT aims to teach basic neuroscience knowledge about aging-related cognitive decline and MCI, and the use of evidence-based practical memory strategies that can facilitate everyday activities, such as getting to appointments, taking medications on time, and remembering the list of things to do. The intervention consisted of three main components: (1) psychoeducation: introduction of the nature of normal aging, MCI, and the associated risk of AD, overview of the memory strategies, and different types of everyday memory situations through lecture; (2) mnemonics training: introduction of some mnemonic strategies that are well established in the existing literature, including both external aids and internal strategies, along with hands-on practice. The use of external memory aids involves the use of memory books, calendars, dated pill containers, to-do lists, etc.82-84 Internal memory strategies include spaced retrieval (i.e., repeatedly recalling information at increasingly longer intervals),85-88 semantic association (i.e., adding meaning to the new information to ease memorization),89-91 and implementation intentions (i.e., visualizing and talking aloud the intention to perform a specific task). 92 Strategies that facilitate the organization and association of new information can enhance the depth of processing that secures memory storage and retrieval 18 ; and (3) provision of home assignments to facilitate the daily application of memory strategies. Older adults were encouraged to practice the learned skills on ecologically valid memory problems in daily life (e.g., remembering names and locations of objects) and record the changes in their everyday behaviors.
Data Processing and Analysis
For the baseline comparisons, older adults in the CLMP and SMT groups were compared using independent samples t-tests for continuous variables and chi-squared tests for categorical variables. To examine the pre-post changes in outcome measures of memory, executive functions, and attention between 2 groups, separate mixed ANOVA with Time (pre vs post) as a within-subject factor and Group (CLMP vs SMT) as a between-subject factor was performed for each measure. Post-hoc pairwise comparisons with Bonferroni adjustment were performed to examine the pre-post change in performance in each group to avoid inflated Type I errors due to multiple statistical comparisons. The significance level was set at .05 for all tests with planned comparisons. To compare the extent of cognitive changes between the 2 intervention groups, the post-minus-pre difference score (i.e., post-intervention score minus pre-intervention score) of each outcome measure was calculated. Partial eta squared (η p 2) and Cohen’s d 93 were presented to indicate the effect size. In addition, to examine who can benefit more from the respective intervention approaches, separate Pearson’s correlations were performed between the post-minus-pre difference score of the outcome measures and the older adults’ age, level of education, and baseline cognitive performance. All statistical analyses were performed using SPSS 28.0 software.
Results
Baseline Performance
Baseline Demographic and Clinical Characteristics and Cognitive Performance of Older Adults in Strategic Memory Training (SMT) and Chanwuyi Lifestyle Medicine Program (CLMP) Groups.
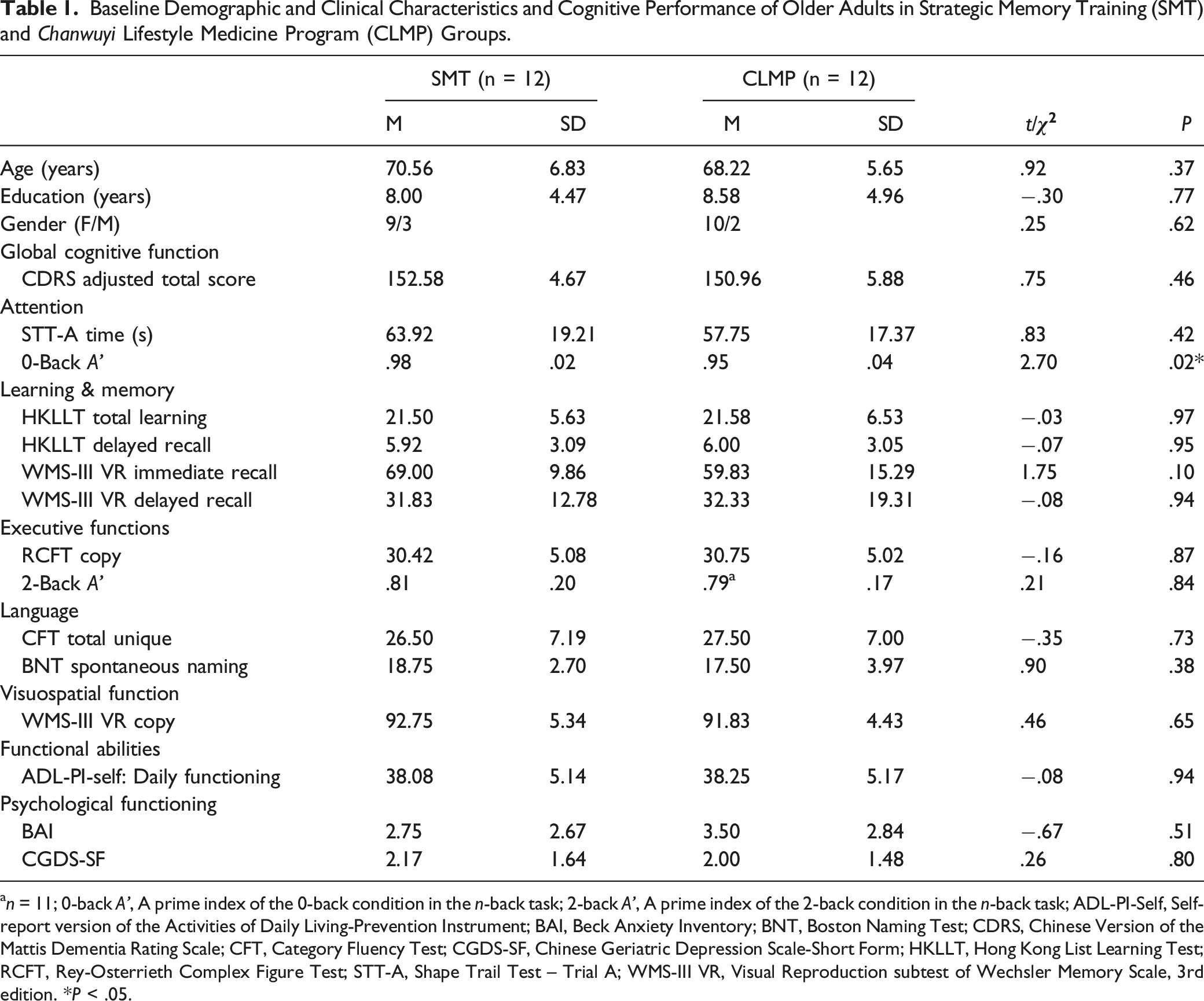
an = 11; 0-back A’, A prime index of the 0-back condition in the n-back task; 2-back A’, A prime index of the 2-back condition in the n-back task; ADL-PI-Self, Self-report version of the Activities of Daily Living-Prevention Instrument; BAI, Beck Anxiety Inventory; BNT, Boston Naming Test; CDRS, Chinese Version of the Mattis Dementia Rating Scale; CFT, Category Fluency Test; CGDS-SF, Chinese Geriatric Depression Scale-Short Form; HKLLT, Hong Kong List Learning Test; RCFT, Rey-Osterrieth Complex Figure Test; STT-A, Shape Trail Test – Trial A; WMS-III VR, Visual Reproduction subtest of Wechsler Memory Scale, 3rd edition. *P < .05.
Regarding their baseline cognitive performance (Table 1), they were matched on the measures of attention (STT-A time: t (22) = .83, P > .05), learning and memory (HKLLT total learning and delayed recall: t (22) = −.03 and −.07, P > .05; WMS-III VR immediate and delayed recall: t (22) = 1.75 and −.08, P > .05, respectively), executive functions (RCFT copy: t (22) = −.16, P > .05; 2-back A’: t (21) = .21, P > .05), language (CFT total unique: t (22) = −.35, P > .05; BNT spontaneous naming: t (22) = .90, P > .05), and visuospatial function (WMS-III VR copy: t (22) = .46, P > .05). However, the CLMP group showed a significantly lower 0-back A’ than the SMT group (t (22) = 2.70, P = .02).
Greater Extent of Improvement in Attention after CLMP
Comparison of the Cognitive Performance Between Strategic Memory Training (SMT) and Chanwuyi Lifestyle Medicine Program (CLMP) Groups Before and After the Intervention.
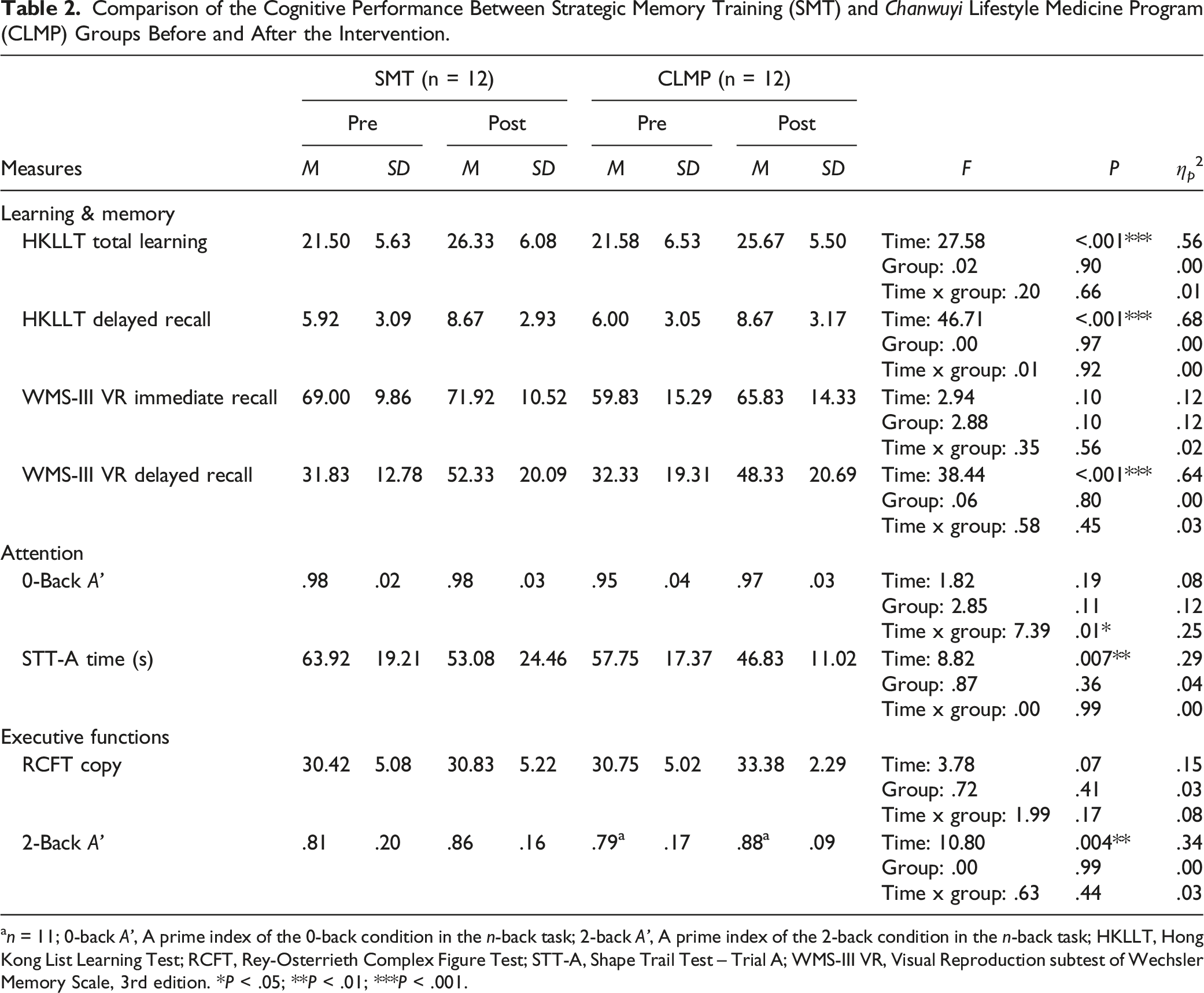
an = 11; 0-back A’, A prime index of the 0-back condition in the n-back task; 2-back A’, A prime index of the 2-back condition in the n-back task; HKLLT, Hong Kong List Learning Test; RCFT, Rey-Osterrieth Complex Figure Test; STT-A, Shape Trail Test – Trial A; WMS-III VR, Visual Reproduction subtest of Wechsler Memory Scale, 3rd edition. *P < .05; **P < .01; ***P < .001.
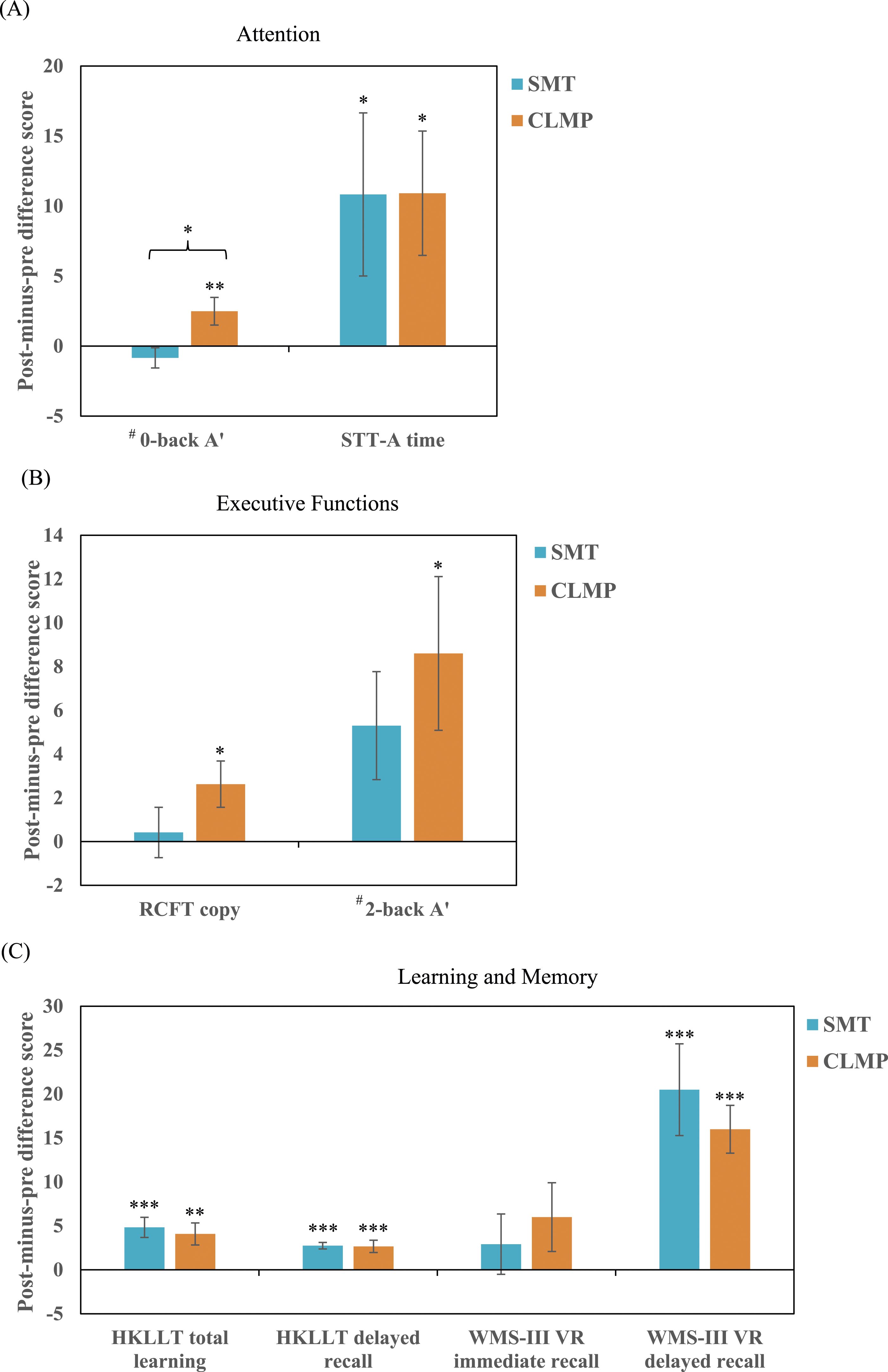
Performance changes on the outcome measures of (A) attention, (B) executive functions, and (C) learning and memory before and after the Strategic Memory Training (SMT; n = 12) and the Chanwuyi Lifestyle Medicine Program (CLMP; n = 12). (A positive value of post-minus-pre difference score indicates improved performance after the intervention, whereas a negative value indicates declined performance. The error bar represents the +/− 1 standard error of the mean. # For a better visual presentation, the mean values and standard errors of 0-back A’ and 2-back A’ are multiplied by 100. *P < .05, **P < .01, ***P < .001. The asterisk marked on top of a bar indicates a significant improvement in outcome measures after intervention based on pairwise comparisons with Bonferroni adjustment. The asterisk marked in between 2 bars indicates a significantly greater improvement in outcome measures of an intervention than the other intervention based on independent samples t test.
For another attention measure, the STT-A, older adults were 17% and 19% faster in completing the connection of numbers in ascending order after receiving the CLMP and SMT respectively. The extents of improvement were comparable between 2 groups. Results of mixed ANOVA showed a significant main effect of Time (F (1,22) = 8.82, P = .007, η p 2 = .29; Table 2) and a significant pairwise pre-post difference with Bonferroni adjustment for both groups (F (1,22) = 4.38 and 4.44, P = .048 and .047, η p 2 = .17; Figure 1(A)). It suggests that older adults demonstrated better attention in terms of processing speed after the CLMP and SMT.
Specific Improvement in Executive Functions after CLMP
Older adults who received the CLMP showed a unique improvement in executive functions in terms of planning/organization and working memory, which are crucial for successful memory encoding and retrieval. For the RCFT measure of planning/organization, there was a marginally significant main effect of Time (F (1,22) = 3.78, P = .07) with a large size effect (η p 2 = .15) (Table 2). Although the Time by Group interaction effect in the mixed ANOVAs was not significant (F (1,22) = 1.99, P = .17), the effect size was medium (η p 2 = .08). Therefore, the non-significant interaction and main effects may be due to the small sample size. Given the medium effect size, a post-hoc power analysis estimates that at least 45 subjects per group are needed to attain a significant time-by-group interaction effect. Pairwise comparisons with Bonferroni adjustment showed a significant 8.6% increase in RCFT copy score specific to the CLMP group (F (1,22) = 5.63, P = .03, η p 2 = .20), but not the SMT group (increased by 1.4%; F (1,22) = .14, P = .71, η p 2 = .01) (Figure 1(B)).
For the 2-back A’ measure of working memory, there was a significant main effect of Time (F (1,21) = 10.80, P = .004) with a large effect size (η p 2 = .34) in the mixed ANOVA (Table 2). The Time by Group interaction effect (F (1,21) = .63, P = .44, η p 2 = .03) and the Group effect (F (1,21) = 0, P = .99, η p 2 = .00) were not significant. A post-hoc power analysis estimates a minimum total of 270 subjects are needed to attain a significant interaction effect. Pairwise comparisons with Bonferroni adjustment showed that older adults, after receiving the CLMP, had a significant 10.9% increase in 2-back A’ (F (1,21) = 7.98, P = .01, η p 2 = .28); whereas those receiving the SMT demonstrated a 6.5% increment, which is non-significant in the same measure after the intervention (F (1,21) = 3.25, P = .09, η p 2 = .13) (Figure 1(B)). The percentage of improvement of 2-back A’ in the CLMP group was 1.7 times that of the SMT group.
CLMP and SMT Improve Visual and Verbal Memory Functions
Older adults with MCI demonstrated significantly improved visual and verbal memory functions after the CLMP as well as the SMT. Regarding verbal learning and memory, results of mixed ANOVAs yielded a significant main effect of Time (HKLLT total learning and delayed recall: F (1,22) = 27.58 and 46.71, P < .001, η p 2 = .56 and .68, respectively), but a non-significant Time by Group interaction effect (F (1,22) = .20 and .01, P > .05) (Table 2). Pairwise comparisons with Bonferroni adjustment showed a robust positive effect of the CLMP (total learning: F (1,22) = 11.57, P = .003, η p 2 = .35; delayed recall: F (1,22) = 22.64, P < .001, η p 2 = .51) as well as SMT (total learning: F (1,22) = 16.21, P < .001, η p 2 = .42; delayed recall: F (1,22) = 24.08, P < .001, η p 2 = .52) with a large effect size (Figure 1(C)). On average, after the interventions, both groups of older adults could recall 19% more words across the three learning trials and 33% more words at the delayed recall trial.
For the visual learning and memory as assessed by the WMS-III VR, results of mixed ANOVAs showed a non-significant Time by Group interaction effect on the WMS-III VR immediate recall score (F (1,22) = .35, P > .05) and delayed recall score (F (1,22) = .58, P > .05) (Table 2). However, the main effect of Time was significant for visual delayed recall (F (1,22) = 38.44, P < .001, η p 2 = .64), suggesting that both intervention groups demonstrated significant improvement in visual delayed recall to a similar extent. Pairwise comparisons with Bonferroni adjustment found a significant increase in delayed recall after the CLMP by 49% (F (1,22) = 14.77, P < .001, η p 2 = .40) and SMT by 64% (F (1,22) = 24.25, P < .001, η p 2 = .52) at a large effect size (Figure 1(C)). For the visual learning ability measured by the WMS-III VR immediate recall score, despite the non-significant main effect of Time (F (1,22) = 2.94, P = .10) and Group effect (F = 2.88, P = .10), their effect size was large (η p 2 = .12; Table 2). Older adults who received the CLMP showed a 10% improvement in immediate recall performance, which is 2.5 times that of those who have learned memory strategies (Figure 1(C)). The non-significant results in WMS-III VR immediate recall may be due to the relatively small sample size and large within-group variabilities as reflected by their SD.
As expected, both CLMP and SMT can effectively enhance verbal and visual memory to a similar extent in older adults with MCI. It is not surprising that older adults demonstrated significant memory improvements after learning multiple strategies to facilitate their memory acquisition and retrieval in the SMT group. Interestingly, the CLMP group, without specific training on memory strategies, also showed similar robust improvements in verbal and visual memory and a trend of improvement in visual learning after the intervention. It suggests that the CLMP is at least equally effective as the SMT for enhancing the verbal and visual memory of older adults with MCI.
Factors Associated with Cognitive Enhancements
Results of Pearson’s correlations showed that older adults with certain baseline characteristics were likely to benefit more from a specific intervention. Regarding the effect of age, older adults at an older age were associated with a greater extent of improvement (as measured by the post-minus-pre difference score) in n-back task performance (0-back A’: r = .68, P = .02; 2-back A’: r = .96, P < .001) in the CLMP group, but not the SMT group (0-back A’: r = −.25, P = .43; 2-back A’: r = .36, P = .25). Regarding the effect of education level, while more educated older adults yielded a greater improvement in WMS-III VR immediate recall (r = .68, P = .02) in the SMT group, less educated older adults yielded a greater improvement in WMS-III VR delayed recall (r = −.63, P = .04) in the CLMP group. There was also a trend of negative correlation between education level and extent of improvement in HKLLT total learning (r = −.54, P = .09) and delayed recall (r = −.56, P = .07) and 0-back A’ (r = −.53, P = .10) in the CLMP group, suggesting that less-educated older adults tended to benefit more from the CLMP in the domains of verbal learning and memory and attention.
Regarding the baseline level of cognitive performance, older adults with MCI who scored lower in the measures of attention and executive functions demonstrated higher cognitive gains, particularly after the CLMP. Results of Pearson’s correlation between the pre-intervention score and the post-minus-pre difference score of each outcome measure showed that the CLMP group demonstrated significant correlations in five out of eight outcome measures, whereas the SMT group demonstrated a significant correlation only in one outcome measure. Older adults with lower baseline performance level of attention (0-back A’: r = −.77, P = .005; STT-A time: r = −.82, P = .002) and executive functions (RCFT copy: r = −.91, P < .001; 2-back A’: r = −.86, P < .001) demonstrated a greater extent of improvement in the respective cognitive measures after the CLMP, but not the SMT. A greater visual learning improvement was associated with a lower baseline visual learning performance in older adults after receiving the CLMP and SMT (WMS-III VR immediate recall: r = −.65 and −.66, P = .03 and .02 for SMT and CLMP respectively). Interestingly, the extent of improvement in verbal learning (HKLLT total learning: r = −.24, P = .46 for SMT, r = −.46, P = .16 for CLMP), verbal memory (HKLLT delayed recall: r = −.33, P = .30 for SMT, r = −.16, P = .65 for CLMP), and visual memory (WMS-III VR delayed recall: r = −.19, P = .56 for SMT, r = −.23, P = .50 for CLMP) was not associated with their baseline measures in any of the intervention groups. It suggests that the CLMP and SMT helped improve the visual and verbal memory of older adults with MCI, regardless of their baseline memory functioning. Rather, in the CLMP group, older adults with a lower baseline performance in verbal learning and memory showed a greater improvement in visual memory (WMS-III VR delayed recall difference score significantly correlated with pre-intervention HKLLT total learning and delayed recall: r = −.65 and −.61, P = .03 and .045, respectively) and planning/organization (RCFT copy difference score significantly correlated with pre-intervention HKLLT delayed recall: r = −.65, P = .03). Such a pattern of association was not observed in older adults who received memory training.
To sum up, after changing lifestyle habits, older adults at an older age improved more in attention and working memory, and those with a lower education level tended to improve more in attention, verbal learning and memory, and visual memory. Besides, older adults with lower baseline visual learning, attention, and executive functions demonstrated greater cognitive gains after lifestyle changes. On the contrary, after learning memory strategies, a greater improvement in visual learning was associated with older adults having a higher education level and a lower baseline visual learning performance.
Discussion
The present study provided preliminary empirical support for the effects of the CLMP, an eastern-western integrative lifestyle intervention, on enhancing memory, attention, and executive functions of older adults with MCI. The findings of this study have added new knowledge that the cognitive-enhancing effects of the CLMP are not restricted to older adults with normal cognitive status or SMC,45-47 but also to those with MCI. The CLMP-associated improvements in visual memory and verbal learning and memory were comparable to those associated with well-established memory strategies training. In addition, the CLMP showed a unique significant improvement in such executive functions as planning/organization and working memory and a greater extent of improvement in attention in terms of accuracy rate as compared to memory training. In sum, as expected, the CLMP was as effective as the SMT in enhancing memory functions and more effective than the SMT in enhancing the executive functions and attention of older adults with MCI. Besides, older adults with MCI who were older, less educated, or had a lower baseline level of visual learning, attention, and executive functions tended to have a larger extent of cognitive gains after modifying their lifestyle habits based on the Chanwuyi principles. Yet, the influence of age, educational level, and baseline cognitive performance on the extent of cognitive enhancements was relatively less pronounced among older adults who have received training on memory strategies.
The memory-enhancing effects of the CLMP are in line with our previous CLMP studies45,46 and other studies on lifestyle intervention.38,41 A two-to-three-month CLMP intervention was found to improve verbal and visual memory delayed recall by around 50% in cognitively healthy older adults 45 and by 37% and 28% respectively in those with SMC. 46 In the present study, the delayed recall improvements (45% in verbal memory and 49% in visual memory) of older adults with MCI after the CLMP were surprisingly closer to the extent reported in healthy older adults 45 and greater than that of older adults with SMC. 46 Lam et al.’s study also reported a 56% - 75% enhancement in verbal delayed recall performance among older adults with MCI after a 12-month integrated lifestyle intervention composed of cognitively stimulating activities and physical activities. 41 These findings are encouraging and clinically significant because they have implicated the potential benefits of the CLMP in ameliorating memory functions of MCI. Impaired delayed recall indicating episodic memory loss is a common clinical symptom detecting MCI and very early dementia of AD7,8 and predicting abnormal cognitive decline.7,9 Individuals with MCI having memory deficits are at a much higher risk of progression to dementia than those without. 6 In addition to MCI-related deficits in delayed memory recall, impaired learning indicating acquisition deficiency is also a common symptom differentiating MCI from normal individuals94,95 and AD patients. 94 The present findings of a significant improvement in verbal learning and a trend of improving visual learning after changing lifestyle habits may be suggestive of the potential therapeutic effects of the CLMP on memory acquisition in MCI. Therefore, an intervention that can enhance or maintain the episodic learning and memory function of MCI could probably prevent or delay further cognitive decline or development of dementia, which may hence reduce the incidence of dementia in the long run.
One may argue whether the improvement in memory functions may be due to repeated testing or the passing of time. According to the previous CLMP study, 46 older adults with SMC reported an average improvement in the scaled scores of 1.8 (i.e., equivalent to an increase of 11.3 raw scores) in delayed visual memory assessed by the WMS-III VR after 10 weekly sessions of the CLMP. Such improvement in scaled scores was larger than the increase of 1.4 scaled scores at 2-to-12-week test-retest intervals listed in the WMS-III technical manual. 62 It suggested that factor(s) over and above the influence of practice effect should be contributing to the improvement in visual memory delayed recall score associated with the CLMP. In the present study, the average improvement in the visual memory of 16 raw scores in WMS-III VR after 10 sessions of the CLMP was even higher than the increase (11.3 raw scores) reported in older adults with SMC. 46 Similarly, the influence of practice effects is probably not robust enough to generate a 45% increase in verbal memory delayed recall score for MCI. In a recent RCT, which adopted HKLLT delayed recall score as a measure of verbal memory performance, 96 healthy Chinese older adults in the control group (who watched videos and engaged in physical exercise) showed only a 12% increase in delayed recall score after 12 weeks. Even among older adults of the experimental groups engaging in cognitive training plus physical exercise, the score increment ranged from 18% to 26%, which is about half of the improvement in verbal memory associated with the CLMP in the present study. Another study exploring memory performance change across time in healthy older adults also reported a lesser extent of increase in delayed recall score of a list learning test. 97 Older adults without any memory decline in 2-year time showed an average increase of 8.8% at the 6-month test-retest interval and 13% at the 24-month interval as assessed by the same verbal memory test. Their extent of memory improvements, which is probably impacted by the practice effects, is far below that (45% increase) reported in this study. Therefore, the extent of visual and verbal memory improvements in the CLMP group was unlikely to solely result from practice effects.
Apart from memory, older adults with MCI demonstrated distinct improvements in planning/organization, working memory, and attention in terms of accuracy after changing lifestyle habits. The benefits of the CLMP on executive functions and attention have also been reported in previous studies on older adults with normal cognitive status, 45 adults with depression,50,52 and children with ASD.53-56,58,59 Similarly, 2 previous integrative lifestyle intervention studies also revealed significant improvements in global cognitive functions (involving attention and executive functions) of older adults with MCI after lifestyle changes.40,41 Ngandu et al. also reported improved processing speed and executive functions in addition to complex memory processing among older adults with an elevated risk of dementia after a 2-year integrative lifestyle intervention. 98 Intact functioning of attention, organization, and working memory is particularly important for successful memory encoding and retrieval processes.99,100 According to the information processing model of memory processes, information that can be learned and recalled after a delay requires intact acquisition, retention, and retrieval processes. These memory processes are closely related to our ability to discriminate relevant and important information from distractions (i.e., attention) and temporally hold the information online while manipulating/categorizing it in a meaningful way (i.e., working memory and planning/organization). Although memory strategies training also improved processing speed (as measured by the STT-A time) in the present study, which is consistent with previous findings of SMT improving processing speed in MCI, 20 the effect of SMT on accurate attentional responses and working memory was less salient than that of the CLMP. Besides, the RCFT copy score, as a measure of planning/organization, was found to be associated with the clinical progression of cognitively normal older adults to MCI. 12 Older adults with higher RCFT copy scores had a 6.7 times higher probability of retaining normal cognitive status than those with lower RCFT copy scores. It implies that alteration in executive function in terms of planning/organization may be a very early marker of MCI. Therefore, our present study finding a significant improvement in RCFT copy score of MCI specific to the CLMP intervention is clinically significant and may be suggestive of the potential effect of the CLMP on reducing the risk of further progression from MCI to dementia. Nevertheless, it should be noted that this study has just provided preliminary support for the potential effects of CLMP on memory, attention, and executive functions based on a relatively small sample of MCI patients. The robustness of CLMP effects requires further validation in future studies with a larger sample size.
More importantly, the CLMP was generally well-accepted by Chinese older adults with over 90% adherence rate 48 and its techniques could be easily comprehended and practiced even by older adults at an older age with a lower level of educational attainment and baseline cognitive abilities. In the correlational analyses of the present study, older adults at an older age improved more in attention and working memory, and those with a lower education level tended to improve more in attention and visual and verbal memory after modifying their lifestyle habits. Specifically, older adults with lower baseline levels of executive functions and attention demonstrated greater cognitive gains after lifestyle changes. Given that some studies have reported limitations of SMT for mostly benefiting older adults with a higher education level and better baseline memory and cognitive resources (e.g., crystallized and fluid abilities, executive functioning),17,25,28 the CLMP may be a possible alternative intervention for improving memory, attention, and executive functions of older adults with less education and poorer baseline cognitive functions.
Despite the encouraging preliminary empirical support for the therapeutic effects of the CLMP for older adults with MCI, there are several limitations in the present study. First of all, this study included a relatively small sample of older adults with MCI and investigated the short-term effects in outcome measures after the intervention. Further studies with a larger sample size and longitudinal follow-up are warranted to explore its sustainability over time. Given the 18-month sustainable positive effects of the CLMP on older adults with SMC, 47 it is anticipated that the improvement in memory, attention, and executive functions associated with the CLMP for MCI revealed in the present study could be maintained in future follow-up studies. It is also worthwhile to follow older adults with MCI for a longer period (e.g., 2 to 5 years) to examine the association between their adherence to the lifestyle changes and their conversion rate of dementia, which may shed some light on the potential efficacy and applicability of the CLMP as a preventive intervention for dementia. In addition, it would be interesting to explore the association between the therapeutic effects of the CLMP and the degree of risk of dementia in a larger sample of the MCI population. The CAIDE risk score indicating the degree of risk of dementia can be computed to examine whether the effectiveness of the CLMP varies with increasing risk.101,102 Finally, neuroimaging or neurophysiological techniques can be considered to evaluate the neural mechanisms underlying the current positive effects associated with the CLMP in older adults. Given the unique positive effects of the CLMP on the measures of executive functions that are primarily mediated by the frontal lobe, it is believed that changing lifestyle habits may probably induce neural-activity alteration in the frontal brain region, similar to those demonstrated in previous studies on children with ASD. 55,56,59
Conclusion
The present study has added knowledge to the research on lifestyle intervention by examining the effects of the CLMP, an eastern-western integrative lifestyle intervention for Chinese older adults with MCI. The positive outcomes provided preliminary empirical support for the beneficial effects of the CLMP on enhancing verbal learning and memory, visual memory, attention, planning/organization, and working memory of older adults with MCI. Older adults who were older, less educated, or with lower baseline cognitive functions tended to have a larger extent of cognitive gains after receiving the CLMP. Therefore, the CLMP may be a potential lifestyle intervention for older adults at risk of dementia. Given the relatively small sample size, further RCTs with a larger sample are needed to confirm its potential and sustainability over time.
Footnotes
Acknowledgments
The authors would like to thank the older adults for their participation in the study and the community health and social centers for their assistance in the subject recruitment process.
Author Contributions
Conceptualization, AC; methodology, AC, SS; formal analysis, M-CC, SS; data curation, M-CC, SS; writing—original draft preparation, AC, M-CC, SS; writing—review and editing, AC, M-CC, SS; supervision, AC; project administration, AC, SS; funding acquisition, AC. All authors contributed to the article and approved the submitted version.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Social Science Collaborative Research Fund (SSCRF) from the Faculty of Social Science of the Chinese University of Hong Kong (PSY).
Ethical Statement
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.