
Abstract
Introduction:
Common protocols for the detection of sentinel lymph nodes in early breast cancer often include the injection of the tracer 1 day before surgery. In order to detect enough activity on the day of surgery, the applied activity in many protocols is as high as several hundred MBq. So far, very few protocols with an activity below 20 MBq have been reported. We developed an ultralow-dose 1-day protocol with a mean activity lower than 20 MBq in order to reduce radiation exposure for patients and staff. Here, we are presenting our experiences in 150 consecutive cases.
Materials and Methods:
A total of 150 patients with clinically and sonographically negative axilla and no multicentricity underwent a sentinel lymph node biopsy using an ultralow-dose protocol performed on the day of surgery. No patient received systemic therapy prior to sentinel node biopsy. After peritumoral injection of the tracer Technetium-99m, a lymphoscintigraphy was performed in all cases. Seven minutes before the first cut, we injected 5 mL of blue dye in the region of the areola.
Results:
In 148 (98.7%) of 150 patients, at least 1 sentinel lymph node could be identified by lymphoscintigraphy; the detection rate during surgery with combined tracers Technetium-99m and blue dye was 100%. The mean applied activity was 17.8 MBq (9-20). A mean number of 1.3 (0-5) sentinel lymph nodes were identified by lymphoscintigraphy and a mean number of 1.8 (1-5) sentinel lymph nodes were removed during sentinel lymph node biopsy.
Conclusion:
Ultralow-dose 1-day protocols with an activity lower than 20 MBq are a safe alternative to 1-day or 2-day protocols with significantly higher radiation doses in primary surgery for early breast cancer. Using Technetium-99m and blue dye in a dual tracer approach, detection rates of 100% are possible in clinical routine in order to reduce radiation exposure for patients and staff.
Keywords
Introduction
Sentinel lymph node biopsy (SLNB) has been introduced as a reliable staging tool for axillary lymph node involvement in breast cancer 20 years ago with published detection rates ranging between 92% and 98%. 1 –4 In patients with clinically negative lymph node status, SLNB has replaced axillary dissection during breast surgery worldwide. 5,6 However, protocols for the detection of SLNs are not standardized. Nanocolloid radiotracers, blue dye, a combination of both or as a recent development hybrid tracers combining radiotracers and fluorescent agents, are used as localizing agents; injection sites vary between intratumoral, peritumoral, intradermal, and subareolar application. 6 Injection of the localizing agent is either done on the same day in 1-day protocols or the day before surgery in 2-day protocols. 7,8 Sentinel lymph node detection rates have been reported to be equivalent in 1-day and 2-day protocols. 9 –12 Although it has been suggested that the minimum absolute activity for 1-day protocols should not be lower than 90 MBq, 13 the European Association of Nuclear Medicine and Society of Nuclear Medicine and Molecular Imaging practice guideline is reporting a range of activities between 3.7 and 370 MBq as being used in published protocols. Activities of 5 to 30 MBq in 1-day protocols and 150 MBq in 2-day protocols are stated to be generally considered sufficient in this guideline. 6 However, in the current guideline of the German Society of Nuclear Medicine, the recommended tracer activity for the detection of axillary SLNs in breast cancer is—depending on the protocol—100 to 200 MBq. The same guideline reports a radiation exposure per patient of 0.4 to 7.3 μSv for the breast surgeon, 0.4 to 0.9 μSv for the OR staff, and 0.5 to 0.7 μSv for the pathologist based on the assumption of a mean activity of 160 MBq. 14
So far, very few protocols with an activity below 20 MBq have been reported, although ultralow activities of 3.7 MBq for a 1-day protocol and 18.5 MBq for a 2-day protocol showed promising detection rates. 11,12 We developed an ultralow-dose 1-day protocol with a mean activity lower than 20 MBq combined with an injection of blue dye in order to reduce radiation exposure for patients and staff in comparison to the recommended activities in the current German guideline relevant to our daily practice. 14 Here, we are presenting the performance of our protocol in 150 consecutive cases.
Materials and Methods
In this retrospective single-arm cohort analysis, we are presenting the data of 150 patients with clinically and sonographically negative axillary lymph nodes, who underwent SLNB using an ultralow-dose protocol performed on the day of surgery at our institution between January 2012 and May 2013. All patients declared their informed consent in written form. No patient received systemic therapy before sentinel node biopsy. Fifty-two (34.7%) of the 150 patients underwent sentinel node biopsy prior to neoadjuvant therapy. The characteristics of the patients are shown in Table 1. On the day of surgery, the nanocolloid radiotracer Technetium-99m (Nanocoll, 8-10 MBq/0.5 mL , GE Healthcare Buchler GmbH & Co.KG) was injected guided by ultrasound in the periphery of the tumor at 8
Patients’ Characteristics.

Results
In 148 (98.7%) of 150 patients, at least 1 SLN could be identified by lymphoscintigraphy. The detection rate during surgery with combined tracers Technetium-99m and blue dye was 100% (150/150). These figures are also shown in Figure 1. In 124 (82.7%) of 150 cases, SLNs were positive for radioactivity and blue dye, and in 21 (14%) of 150 cases, SLNs were found by radioactivity only, whereas blue dye was negative and in 5 (3.3%) of 150 cases radioactivity was negative, and SLNs were detected by blue dye only. The mean applied activity was 17.8 MBq (9-20). A mean number of 1.3 (0-5) SLNs were identified by lymphoscintigraphy and a mean number of 1.8 (1-5) SLNs were identified and removed during SLNB. Thirty-two (21.3%) patients received a secondary axillary dissection according to the historical standard because of involved SLNs. In 9 (28.1%) of these 32 cases, additional involved lymph nodes were found.
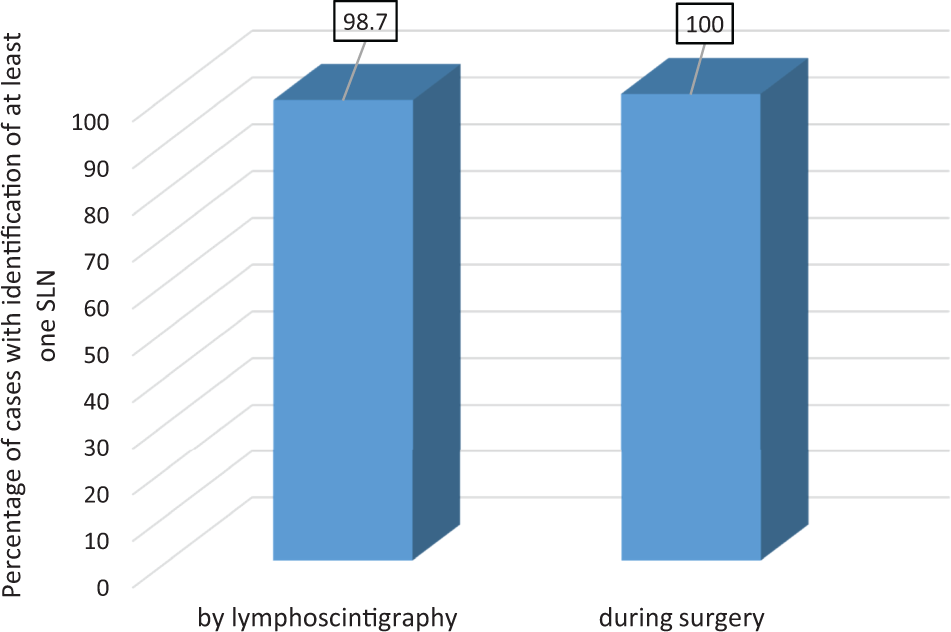
Detection rates.
Discussion
In the current analysis, we are presenting an intraoperative detection rate for sentinel nodes in early breast cancer of 100% using a dual tracer approach in an ultralow-dose 1-day protocol with an activity of below 20 MBq. Blue dye added only slightly to the detection of at least 1 SLN in every patient. Although it has been proposed that peritumoral injection of the radioactive tracer yields lower detection rates (91%) than dermal/subdermal and subareolar/periareolar injection (96.7% and 97.0%, respectively), 13 our results of peritumoral injection were as high as 98.7% for lymphoscintigraphy and 96.7% for intraoperative detection for the radioactive tracer. Published comparisons of 1-day and 2-day protocols demonstrated intraoperative detection rates of 85% for the 1-day protocol and 91% for the 2-day protocol using a standard tracer dose 10 and 99.3% for the 1-day protocol and 96% for the 2-day protocol using a protocol with mean doses of 22.3 (1-day protocol) and 40.4 MBq (2-day protocol). 9 Interestingly, the detection rate for the 1-day protocol with the mentioned mean activity of 22.3 MBq in this study is very similar to our results with a mean activity of 17.8 MBq and a detection rate of 100%. Due to the fact that there are no published data regarding a comparison of a low-dose protocol and a standard protocol and due to the retrospective design of our study, we cannot draw the conclusion that these data are indicating a superior detection rate of low-dose protocols, but they are suggesting that using lower activities is not inferior to higher activities and therefore feasible in clinical practice when using a combined tracer approach including blue dye.
Regarding the mean number of removed sentinel nodes, there was no statistically significant difference between 1-day and 2-day protocols; however, the 1-day protocols trended to harvest more nodes. Furthermore, the number of detected SLNs seems to be higher in low-dose protocols. Using a standard activity protocol, the 1-day approach resulted in a mean number of detected sentinel nodes of 1.64 (0-6) versus 1.61 (0-4) in the 2-day approach. 10 The mean number of sentinel nodes detected with a low-dose protocol was generally higher than the results of standard protocols (1-day protocol 2 [0-6]; 2-day protocol 1 [0-11]) also trending for a higher number of sentinel nodes detected with the 1-day protocol. 9 Our own results are in line with the data for using a 1-day protocol with a low activity, yet our mean activity was still lower than in most protocols published yet, indicating that it is possible to use activities lower than 20 MBq without compromising detection rates or number of detected SLNs.
Although we tried to reduce radiation exposure by low tracer activities in our trial as a step of de-escalation, the current directions of de-escalation of axillary staging are going even further. The INSEMA trial is investigating the complete omission of axillary staging versus SLNB in a 1:4 randomized design and recruited the first 1000 patients in only a few months. 15 However, there will still be a role for sentinel node biopsies in early breast cancer in the future.
We believe that the data we are presenting here are helping to reduce radiation exposure for staff and patients without compromising detection rates of SLNs in patients with early breast cancer undergoing primary surgery and thus are a potential step in the concept of de-escalation of diagnostic and therapeutic procedures.
Conclusion
Our ultralow-dose 1-day protocol with an activity lower than 20 MBq is a safe alternative to other 1-day or 2-day-protocols with significantly higher radiation doses in primary surgery and SLNB for early breast cancer. Using ultralow-dose Technetium-99m and blue dye in a dual tracer approach, detection rates of 100% are possible in clinical routine in order to reduce radiation exposure for patients and staff. The number of removed SLNs is comparable to the data from previous trials using significantly higher activities. We will now test our ultralow-dose 1-day protocol in the postneoadjuvant setting.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.