
Abstract
Background and Purpose:
Although there is a strong biological rationale to electively treat the pelvic nodes during bladder preservation, its clinical benefit is uncertain. This may be explained by the incidental dose received by the nodal regions when treating the bladder alone. This study was conducted to investigate the doses received by the different pelvic nodal regions when the bladder alone is treated by standard conformal radiotherapy.
Methods and Materials:
The computed tomography data sets of 20 patients with node-negative muscle-invasive bladder cancer treated in a bladder preservation protocol were studied. Patients were originally treated with conformal radiotherapy to the bladder alone. Replanning was done with additional delineation of the pelvic nodal regions namely common iliac (upper and lower), presacral, internal iliac, obturator, and external iliac. Dose volume parameters such as Dmean, Dmax, D100%, D66%, D33%, V40, and V50 to each of the nodal regions were estimated for all patients.
Results:
The obturator nodes received the highest dose among all nodal regions. The mean dose received by obturator, external iliac, and internal iliac regions was 59, 45, and 36 Gy, respectively. The dose received by these 3 regions in the full bladder state was 63, 52, and 47 Gy, respectively. The dose received by all other pelvic nodal regions was low and not clinically relevant.
Conclusion:
The incidental dose received by obturator and external iliac nodes is clinically significant in bladder-only radiation, possibly enough to influence micrometastatic disease. This may be a reason for the lack of clear benefit seen with nodal irradiation in bladder cancer.
Advances in Knowledge:
This study highlights that the incidental dose received by obturator and external iliac nodes is clinically significant in bladder-only radiation. The obturator nodes received the highest dose among all nodal regions with mean dose of 59 Gy.
Introduction
Trimodality treatment approach of maximal transurethral resection of bladder tumor followed by concurrent chemoradiotherapy (CRT) has shown similar outcomes compared to radical cystectomy in large series. 1 The 5-year overall survival rates with trimodality treatment ranges from 50% to 65%, and approximately 60% of the patients maintain a functional bladder. 2 Bladder radiotherapy has evolved over the last few years with better definition of the bladder motion and integration of various adaptive strategies to improve therapeutic ratio. One unresolved issue, however, is the usefulness of prophylactic pelvic nodal irradiation in node-negative muscle-invasive bladder cancer (MIBC).
Biological rationale for elective nodal irradiation is strong. Evidence from cystectomy series shows that pathologically detected micrometastasis in clinically and radiologically negative pelvic nodes ranges from 25% to 44%. 3,4 The regional lymph nodes most at risk are those in the true pelvis, below the bifurcation of common iliac arteries, and include internal iliac, external iliac, obturator, perivesical, and presacral nodes. Extended pelvic nodal dissection with higher lymph nodal yield has shown improved outcomes. 5 However, for bladder conservation, there is variability in practice worldwide in terms of elective nodal irradiation. 6 In a series of Radiation Therapy Oncology Group (RTOG) trials, the radiation fields included a limited pelvic portal treated to 40 to 45 Gy followed by a boost to the bladder, 7 the rationale being that regional nodal involvement is not uncommon in MIBC. Among others, the UK-based BC 2001 trial comparing radiation with CRT did not use elective nodal radiotherapy (RT) and reported a nodal relapse rate of under 5% which is similar to the patterns of failure reported in the studies in which pelvic RT has been used. 8 This discordance between biological rationale and an apparent lack of clinical benefit with prophylactic pelvic irradiation could possibly be explained by the incidental dose received by the pelvic nodal regions, particularly the nodes lying along the external iliac, obturator, and internal iliac vessels.
The hypothesis of the present study is that pelvic nodes receive a significant “incidental” dose from conformal treatment of bladder only, which may influence or eradicate micrometastatic disease. The aim was to quantify the extent of the radiation delivered incidentally to the different pelvic nodal sites when treating the bladder alone using standard conformal radiotherapy.
Methods
Patient Selection
A cohort of 20 patients with clinicoradiologically node-negative MIBC who were treated in a prospective bladder preservation protocol, using image-guided conformal radiotherapy, were studied. Their computed tomography (CT) planning data sets were used for the purpose of this study. The steps of the original treatment planning and study-specific replanning are briefly described below.
Simulation
Simulation CT scanning was performed using 3-mm slice thickness and intravenous contrast. All patients were simulated in a supine position, and a bladder filling protocol (500 mL water, 45 minutes prior to procedure) was used for a reproducible, comfortably full bladder. Patients were instructed to empty their bowel prior to planning CT, and no laxative or enema was used for bowel preparation. Three lead fiducials were placed on the skin at points of laser intersection (1 at symphysis pubis and the other 2 at lateral aspect of thighs), and these points were tattooed for aiding in daily treatment setup. The scanned area was from the first lumbar vertebra to 5 cm below the ischial tuberosity.
Target volumes were contoured including the clinical target volume (CTV; whole bladder), planning target volume (PTV; a uniform margin of 1.5 cm around the CTV), and organs at risk (OARs; rectum, bowel, and bilateral femoral heads). The pelvic nodes were not part of the original target volumes. The CT data sets containing the contours of target volumes were dearchived, and pelvic nodal regions were additionally contoured for the purpose of this study.
Pelvic Nodal Region Delineation
To evaluate the incidental dose received by the nodal regions when bladder alone is treated, each pelvic nodal region was delineated separately. For uniformity, all contouring was done by 1 investigator (S.L.). The RTOG Genitourinary (GU) Radiation Oncology Specialists Consensus Statement on pelvic lymph node volumes and another consensus for pelvic regions for gynecologic malignancies were used to define each region in the study. 9,10 The detailed description of each nodal region is available in the Supplementary Table 1, and a representation is shown in Figure 1. The lymph nodal CTV was defined as the area encompassed by a 7-mm margin around the applicable pelvic vessels carefully excluding bowel, bladder, bone, and muscle. Each nodal area was modified to cover adjacent adipose tissues at risk of microscopic nodal metastases. The pelvic nodal regions delineated were bilateral common iliac (upper and lower), presacral, internal iliac, obturator, and external iliac. Presacral region was defined based on bony and muscle anatomy as there are no visible major vessels in that area.

Planning computed tomography (CT) images in axial view showing the pelvic nodal regions (a-d).
Treatment Planning
The 3-dimensional conformal radiotherapy (3DCRT) plans were made on the external beam planning system of Eclipse (ver.8.6.14; Varian Medical Systems, Palo Alto, California). The 3DCRT plans included 4 multileaf collimator (MLC)-shaped coplanar fields (anterior–posterior and 2 laterals with wedges 15°-30°) with 6 to 15 MV photons. A 7-mm margin around the beam’s eye view projection of the PTV was considered while shaping to fit the MLC to PTV. The prescribed dose was 64 Gy in 32 fractions at 2 Gy per fraction. It was ensured to cover the 95% of the PTV with 95% of the prescribed dose. The maximum dose was not to exceed 107% of the prescribed dose. The nodal CTVs were not part of the target coverage, but their dose volume histograms (DVHs) were generated and studied.
Dose to Nodal Regions
Estimation of dose to each of the pelvic nodal regions was done and the DVH was used to get the dose volume parameters. The parameters analyzed were Dmean, Dmax, D100% (dose in Gy received by 100% of volume), D66%, D33%, V40 (volume of the organ receiving 40 Gy), and V50.
Statistical Analysis
Statistical data were analyzed using SPSS version 20.0. Mean values are indicated with standard deviation (SD) or 95% confidence interval.
Results
The planning objectives and dose constraints for the OARs were met in all patients. The mean bladder volume was 292 cc (SD = 150). The obturator nodes, being in close proximity to the target volumes, received the highest dose among all regions. The mean dose received by obturator region was 59 Gy. The mean dose received by external iliac region was 45 Gy. The mean dose received by internal iliac region was 36 Gy. The dose received by all other pelvic nodal regions was clinically insignificant (Table 1). The dose received by obturator, external iliac, and internal iliac nodal regions were higher in patients with larger bladder volume at simulation (>300 cc, P = .01; Table 2)
Dose Volume Parameters of Pelvic Nodal Regions in 3DCRT Technique.
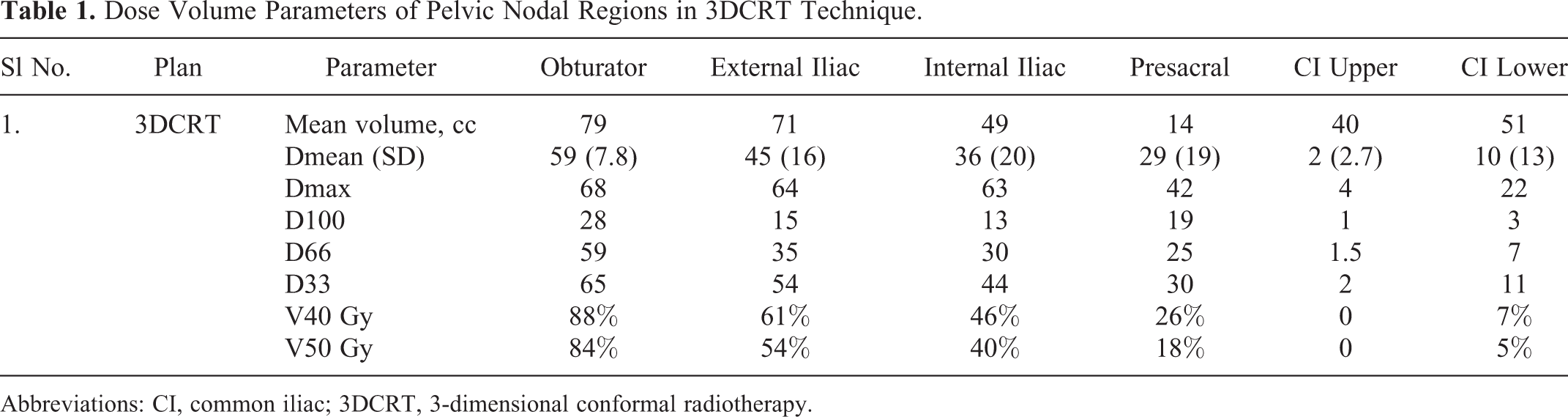
Abbreviations: CI, common iliac; 3DCRT, 3-dimensional conformal radiotherapy.
Dose Volume Parameters of Pelvic Nodal Regions Based on Bladder Filling.a

Abbreviations: DVH, dose volume histogram; SD, standard deviation.
a The bladder filling protocol used was 500 mL water after voiding, 45 minutes prior to simulation.
Discussion
In the present study, we report clinically significant incidental dose received by the obturator, external iliac, and the internal iliac nodes when bladder alone is irradiated in full or empty state. This incidental dose possibly explains the low incidence of nodal relapse seen in bladder only radiotherapy and the lack of clear benefit of pelvic nodal irradiation during bladder preservation.
The primary lymphatics in bladder cancer drain to the internal iliac, external iliac, obturator, and presacral nodes (65%-75%). 11 The second echelon nodes are the common iliac and paraaortic nodes (19%-21%). 12 The incidence of lymph nodal involvement in clinically node-negative muscle-invasive disease, as shown in large cystectomy cohorts, varies from 15% to 60% depending on the stage. 4 In a pathoanatomic study, of the 200 patients who underwent radical cystectomy and extended pelvic lymph node dissection (PLND), internal iliac, external iliac, and obturator groups of lymph nodes were identified as the primary drainage and referred to as the endopelvic sites. Any extrapelvic nodal involvement was always associated with involvement of pelvis areas, and skip lesions were not reported. 13 The lymph nodal mapping studies by Bochner et al showed that patients with positive nodes above the aortic bifurcation had pelvic nodal involvement, indicating that only extensive regional metastatic disease might lead to retroperitoneal nodal involvement. 14 Bilateral PLND with a higher lymph nodal yield has shown improvement in survival. 15,16 Based on these data and the benefit with PLND series, there is a strong biological rationale to treat the pelvic nodes with RT during bladder preservation.
The clinical benefit with nodal RT has however been uncertain in the literature, resulting in varying practice in different centers and even in large cooperative group trials. Rodel et al reported their 18-year experience of 415 patients with T1-T4 N0/N1 bladder cancer treated with conventional 4-field box technique to a dose of 54 Gy to bladder and 45 to 54 Gy to the nodes (pelvic and selectively, paraaortic). The 10-year bladder preservation rate was 64% with a pelvic failure rate of 3%. 17 Mak et al reported the long-term outcomes of MIBC treated with bladder preservation approaches with RTOG trials (5 phase II—8802, 9506, 9706, 9906, and 0233 and 1 phase III—8903). Radiation fields included the pelvic nodes (perivesical, internal iliac, obturator, and distal external iliac) in all the trials. The pooled analysis showed a 5- and 10-year nodal recurrence rates of 13% and 16%, respectively. 7 The long-term outcomes of 348 patients treated with bladder preservation on successive protocols from 1986 to 2006 at Massachusetts General Hospital showed the 10-year rate of pelvic recurrence of 11% with inclusion of pelvic nodes (perivesical, obturator, and external iliac) in the radiation portal. 18
The largest data for bladder-only radiation were reported in the multicentric BC 2001 trial in which 360 patients of MIBC were treated with bladder alone radiotherapy with or without chemotherapy. The radiation portal included the whole bladder or partial volume treated with 3DCRT plans, and pelvic nodes were not electively irradiated. The 2-year pelvic nodal relapse rate was 4.9%. 8 In another large phase II trial by Hoskin et al, 333 patients were treated with RT alone or RT with carbogen and nicotinamide. All patients received bladder-only RT. However, the nodal relapse rates were not reported. 19 In the only randomized trial addressing the issue of elective nodal irradiation, 230 patients of T2-T4 lymph node-negative patients with MIBC were randomized to whole pelvis (120) or bladder-only (110) cisplatin-based chemoradiation. In whole pelvic radiotherapy (WPRT) arm, whole pelvis was treated to a dose of 45 Gy in 25 fractions (from L5-S1) using 4-field box technique followed by boost to a dose of 20 Gy in 10 fractions. Bladder-only CRT showed similar rates of bladder preservation, disease-free survival, and overall survival rates as those of whole pelvis CRT. There was no difference in the regional recurrence between the 2 groups (12.5 vs 14.5, respectively). 20 These data suggest that in patients undergoing bladder preservation with or without pelvic RT, the nodal failure appears to be 4% to 14% (Table 3). The poor correlation between the strong biological rationale and clinical benefit could be explained by the incidental dose received by the lower pelvic nodal regions (external iliac, obturator, and internal iliac) as shown in the present study.
Pelvic Nodal Failure Rates With Various Bladder Preservation Trials.

Abbreviations: DFS, disease free survival; OS, Overall survival; PA, Paraaortic; WPRT, whole pelvic radiotherapy.
A standard dose of radiation for the eradication of microscopic disease is not appropriate. Fletcher originally reported the effectiveness of 30 to 50 Gy in sterilizing subclinical disease. 23 Low doses of radiation (40 Gy) may provide sterilization of tumor sites that have a low number of clonogens in general and differs based on the primary site. 24 In case of bladder cancer, there is no consensus about the effective elective dose to the pelvic nodal regions. A dose of 36 to 55 Gy dose have been prescribed in various trials. In addition, chemotherapy may have an effect on the nodal response and use more effective combination chemotherapy with radiation as in BC 2001 would lead to improved locoregional control. 8
Being a dosimetric study, the present work is limited by relatively small number of patients but possibly adequate as a proof of concept. The results of the present study using the standard 3D conformal RT technique may vary in the setting of use of nonconcentric PTV margins either as a single PTV or with the use of multiple PTVs with an adaptive approach. With intensity-modulated radiotherapy (IMRT), especially with online or offline adaptive treatment approaches, the PTV margins can be reduced and a sharper dose fall off may lead to a possible reduction in the incidental irradiation to adjoining areas. It is possible that with increasing use of IMRT, the need for pelvic RT may become more relevant due to reduced incidental doses. Murthy et al recently reported the clinical outcomes of patients with bladder cancer treated with adaptive radiotherapy. All 44, except the initial 12 patients, were treated with elective pelvic nodal. Two of the 12 patients without nodal RT and none of those receiving pelvic RT developed isolated pelvic lymph node relapses. 25
Conclusion
The incidental dose received by obturator and external iliac nodes is clinically significant in bladder-only radiation, possibly enough to influence micrometastatic disease. This may be a reason for the lack of clear benefit seen with nodal irradiation in bladder cancer treated with conformal radiotherapy. It is likely that with IMRT, the need for pelvic RT may become more relevant due to reduced incidental doses. Computational models that predict long-term outcome when lower pelvic nodal regions are included in conformal bladder treatment are needed from prospective trials.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.