
Abstract
Objectives:
Pelvic lymph nodal regions receive an incidental dose from conformal treatment of the prostate. This study was conducted to investigate the doses received by the different pelvic nodal regions with varying techniques used for prostate radiotherapy.
Methods and Materials:
Twenty patients of high-risk node-negative prostate cancer treated with intensity-modulated radiotherapy to the prostate alone were studied. Replanning was done for intensity-modulated radiotherapy, 3-dimensional conformal treatment, and 2-dimensional conventional radiotherapy with additional delineation of the pelvic nodal regions, namely, common iliac (upper and lower), presacral, internal iliac, obturator, and external iliac. Dose–volume parameters such as Dmean, D100%, D66%, D33%, V40, and V50 to each of the nodal regions were estimated for all patients.
Results:
The obturator nodes received the highest dose among all nodal regions. The mean dose received by obturator nodal region was 44, 29, and 22 Gy from 2-dimensional conventional radiotherapy, 3-dimensional conformal treatment, and intensity-modulated radiotherapy, respectively. The mean dose was significantly higher when compared between 2-dimensional conventional radiotherapy and 3-dimensional conformal treatment (P < .001), 2-dimensional conventional radiotherapy and intensity-modulated radiotherapy (P < .001), and 3-dimensional conformal treatment and intensity-modulated radiotherapy (P < .001). The D33% of the obturator region was 64, 39, and 37 Gy from 2-dimensional conventional radiotherapy, 3-dimensional conformal treatment, and intensity-modulated radiotherapy, respectively. The dose received by all other pelvic nodal regions was low and not clinically relevant.
Conclusion:
The incidental dose received by obturator regions is significant especially with 2-dimensional conventional radiotherapy and 3-dimensional conformal treatment techniques as used in the trials studying elective pelvic nodal irradiation. However, with intensity-modulated radiotherapy, this dose is lower, making elective pelvic irradiation more relevant.
Advances in Knowledge:
This study highlights that incidental dose received by obturator regions is significant especially with 2-dimensional conventional radiotherapy and 3-dimensional conformal treatment techniques.
Introduction
Patients with high-risk prostate cancer benefit from aggressive treatment with a combination of radiotherapy (RT) and hormonal treatment. Primary RT of prostate with dose escalation improves biochemical disease-free survival, whereas the addition of hormonal treatment improves overall survival. 1 –4 The standard treatment consists of a combined androgen deprivation therapy with external beam RT. However, controversy exits among radiation oncologists regarding the volumes of radiation for clinically negative nodes in the pelvis. Although the role of elective pelvic node irradiation has been studied in 3 major randomized trials, the question still remains unanswered. 5 –7 The ongoing trials (RTOG 09-24-NCT01368588, PIVOTAL CRUK/10/022, and POP-RT NCT02302105) addressing this issue may help in resolving the issue better. Clinical practice, however, differs worldwide with divided opinion. 8,9
Elective nodal irradiation is considered the standard of care in malignancies of head and neck, rectal cancer, and gynecological sites but is now discredited in lung cancer and Hodgkin lymphoma treatment. 10,11 In lung cancer, a possible argument against elective nodal irradiation is the “incidental” irradiation of uninvolved mediastinal areas located in the proximity of the tumor, which effectively amounts to elective irradiation. 10 The same argument may hold true for prostate cancer as well, especially with conventional techniques, as predominantly used in the aforementioned trials. The contemporary, highly conformal RT to the prostate alone may result in much less incidental radiation dose to the pelvic lymph node regions than with conventional RT, making elective pelvic RT more relevant with modern techniques.
The premise of this study is that pelvic nodes may receive an incidental dose from conformal treatment of prostate only. The aim was to quantify the extent of the radiation administered incidentally to the different pelvic nodal sites with different techniques.
Materials and Methods
Patient Selection
Twenty patients with high-risk, node-negative prostate cancer treated with image-guided RT on tomotherapy were studied. The RT planning preparation and contouring were followed as described previously. 12 The steps are described briefly here.
Simulation
Simulation computed tomography (CT) scanning was performed using 3-mm-slice thickness and intravenous contrast. All patients were simulated in a supine position with a bladder-filling protocol (500 mL water prior to the procedure). Patients were instructed to empty their bowel prior to planning CT, and no laxative or enema was used for bowel preparation. Three lead fiducials were placed on the skin at points of laser intersection (1 at symphysis pubis and others at lateral aspect of the thighs), and these points were tattooed for aiding in daily treatment setup. The scanned area was from the L1 vertebra to 5 cm below the ischial tuberosity.
Target and Organ-at-Risk Delineation
The target volumes and organ at risk (OAR) were delineated in all patients in Oncentra Planning system (version 4.3; Nucletron, Veenendaal, Netherlands, An Elekta company). The clinical target volume (CTV) included the entire prostate and the base of the seminal vesicles (proximal 0.5 cm). In case of seminal vesicle involvement, entire seminal vesicle was included in the volume. Pelvic lymph nodes were not prophylactically treated. The planning target volume (PTV) was defined as CTV plus a 3-dimensional (3D) margin of 7 mm in all directions except 5 mm posteriorly. The OAR such as bladder, rectum, and bilateral femoral heads was contoured as per the standard guidelines.
The CT data sets containing these contours of target volumes (CTV and PTV) and OAR were dearchived, and pelvic nodal regions were additionally contoured for the purpose of this study. The entire process from patient selection to replanning is outlined in Figure 1 as a flowchart.

Workflow of the process from patient selection to dose estimation.
Pelvic Nodal Region Delineation
To evaluate the incidental dose received by the nodal regions, each pelvic nodal region was delineated separately. For uniformity, all contouring was done by 1 investigator (S.L.). The Radiation therapy oncology group (RTOG) genitourinary (GU) Radiation oncology specialists consensus statement on pelvic lymph node volumes and another consensus for pelvic regions for gynecologic malignancies were used to define each region in the study. 13,14 The detailed description of each nodal region is shown in Table 1 and a representation in Figure 2. The lymph node CTV was defined as the area encompassed by a 7-mm margin around the applicable pelvic vessels carefully excluding bowel, bladder, bone, and muscle. Each nodal area was modified to cover adjacent adipose tissues at risk of microscopic nodal metastases. The pelvic nodal regions delineated were bilateral common iliac (upper and lower), presacral, internal iliac, obturator, and external iliac. Presacral region was defined based on the bony and muscle anatomy as there are no visible major vessels in that area.
Clinical Target Volume of Pelvic Nodes Related to Anatomical Landmarks.


Planning computed tomography (CT) images in axial view showing the pelvic nodal regions (A-D).
Treatment Planning
Intensity-modulated RT replanning
The image and volume data sets were transferred to the tomotherapy treatment planning station (version 2.2.4; Tomotherapy Inc). The planning system uses the least square minimization function for optimization and convolution superposition algorithm for dose calculation. A field width of 2.5, pitch of 0.3, and modulation factor of 3 to 3.5 were used during optimization.
The patient’s original plan used for the treatment was not considered. Replanning was done after pelvic nodal contouring with the same planning objectives and constraints. The prescribed dose was 74 Gy in 37 fractions at 2 Gy per fraction. The goal was to ensure that at least 98% of the PTV received 95% of the prescribed dose. The maximum dose within the PTV was not allowed to exceed 105% of the prescribed dose.
Replanning with 3-dimensional conformal RT
The 3-dimensional conformal treatment (3DCRT) and conventional plans were made on the external beam planning system of Eclipse (version 8.6.14; Varian Medical Systems, Palo Alto, California). For the 3DCRT replanning, 1-cm margin to the CTV in all directions was given to generate the PTV. The 3DCRT plans included 3 multileaf collimator (MLC)-shaped coplanar fields (1 anterior and 2 laterals with wedges 15°-30°) with 6 to 15 MV photons. A 7-mm margin around the beam’s eye view projection of the PTV was considered while shaping to fit the MLC to PTV. The prescribed dose was 74 Gy in 37 fractions at 2 Gy per fraction. It was ensured to cover the 95% of the PTV with 95% of the prescribed dose. The maximum dose was not to exceed 107% of the prescribed dose. The dose constraints were followed as per Medical Research Council (MRC) RT01 trial.15,16
Replanning with conventional RT
For the 2-dimensional (2D) RT replanning, 1-cm margin to the CTV in all directions was given to generate the PTV. A 3-field technique, 1 anterior field and 2 laterals with wedges 15° to 30° were used. Appropriate field size with a margin of 1 to 1.5 cm to the PTV to account for penumbra were used. In all cases, field size was <10 × 11 cm. The prescribed dose was 74 Gy in 37 fractions at 2 Gy per fraction. It was ensured to cover the 95% of the PTV with 95% of the prescribed dose. The maximum dose was not to exceed 107% of the prescribed dose. The dose constraints were followed as per MRC RT 01 trial. 15,16
Dose to nodal regions
Estimation of dose to each of the pelvic nodal regions was done, and dose–volume histograms (DVHs) were used to obtain the dose–volume parameters. The DVH parameters were obtained for conventional, 3DCRT, and IMRT plans and were compared. The parameters analyzed were Dmean, D100% (dose in Gy received by 100% of volume), D66%, D33%, V40 (volume of the organ receiving 40% of prescribed dose), and V50.
Statistical Analysis
Statistical data were analyzed using Statistical Package for Social Sciences (SPSS) version 20.0. Mean values are indicated with standard deviation or 95% confidence interval. The dose received by pelvic nodal regions was compared between the techniques using the paired Student t test as the means were normally distributed.
Results
The planning objectives and dose constraints for the OAR were met in all patients in all 3 techniques. The obturator nodal regions, being in close proximity to the target volumes, received the highest dose especially in the conventional technique. The mean volume of obturator region was 56.3 cm3. The mean dose received was 44, 29, and 22 Gy from 2D, 3DCRT, and IMRT, respectively (Figure 3). This was statistically significant when the mean dose was compared between 2D and 3D (P < .001), 2D and IMRT (P < .001), and 3D and IMRT (P < .001). The D33% was 64, 39, and 37 Gy with 2D, 3DCRT, and IMRT, respectively.
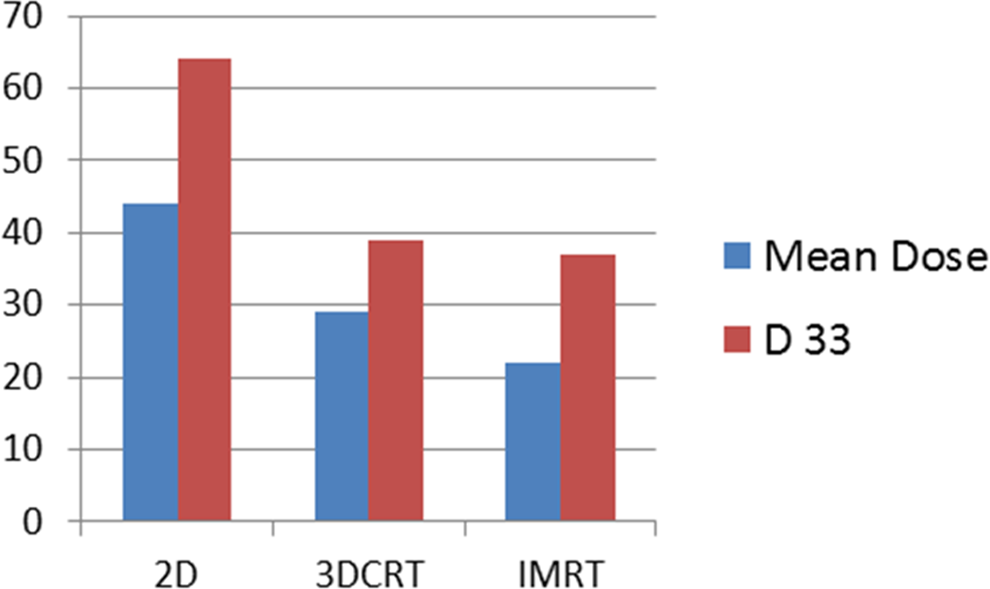
Mean dose and D33 in 2-dimensional conventional radiotherapy (2D), 3-dimensional conformal treatment (3DCRT), and intensity-modulated radiotherapy (IMRT) techniques.
Biological equivalent dose (BED) to primary and obturator nodes with α/β of 3 was calculated. The BED for the PTV prostate was 123.3 Gy3. The BED for obturator nodes with 2D, 3DCRT, and IMRT was 73.4, 48.43, and 36.7 Gy3, respectively.
The dose received by all other pelvic nodal regions was less (Table 2). Although the dose was significantly low with IMRT, they were not clinically relevant.
Dose–Volume Parameters of Pelvic Nodal Regions in 2D, 3DCRT, and IMRT Techniques.

Abbreviations: CI, common iliac; 2D, 2-dimensional conventional radiotherapy; 3DCRT, 3-dimensional conformal treatment; IMRT, intensity-modulated radiotherapy; SD, standard deviation.
Discussion
We have documented clinically significant incidental dose to the obturator region when the prostate alone is intended to be treated. This dose decreases with advancement in technique as a result of the use of smaller margins and steeper dose gradient. To the best of our knowledge, this is the first such data to report the incidental dose to predefined pelvic nodal regions in prostate cancer. This strengthens the hypothesis that the incidental dose may eradicate the micrometastatic disease in some of the sentinel nodal regions, thereby negating the possible benefit with pelvic RT in randomized trials. The result may be logical or expected, however, it is important to document the dose and provide one of the reasons for lack of benefit in randomized trials.
The primary lymphatic drainage of the prostate consists of the internal iliac, obturator, external iliac, and presacral lymphatic nodes. Mapping studies of lymph node drainage in prostate cancer show that in spite of a variable drainage pattern, there exists a hierarchical order of distribution of these nodes. 17 Based on the data from sentinel node series, the first region to be involved is obturator in 32% (24%-43%), internal iliac in 29% (20%-38%), and external iliac in 30% (12%-40%). The obturator fossa, together with internal iliac and external iliac, account for 91% of positive sentinel nodes. 18 Joniau et al treated intermediate to high-risk patients with a “superextended” lymph node dissection, which included common iliac (below aortic bifurcation), internal and external iliac region, obturator fossa region, and presacral region. Metastatic yield was low in presacral region (9%), common iliac region (3%), and aortic bifurcation region (1%). 17 In the present study, while the dose to external and internal iliac was not significant with any of the techniques, dose to obturator region was about 36 to 40 Gy especially with conventional techniques, which may be relevant to the hypothesis being tested.
The dose required for eradicating occult micrometastatic disease in prostate cancer is not clear. Fletcher originally reported the effectiveness of 30 to 50 Gy in sterilizing subclinical disease. 19 Mark illustrated that there is no such thing as a “uniform dose for the control of microscopic disease.” They inferred that relatively low doses of radiation (<40 Gy) will provide sterilization of tumor sites that have a low number of clonogens in general and differs based on the site of primary. In case of prostate adenocarcinoma, there is no consensus about the effective elective dose to the pelvic nodal regions. 20 Perez et al reported a nonrandomized comparison of pelvic nodal irradiation (40-45 Gy vs 50-55 Gy) in localized carcinoma prostate with definitive RT alone. There was no difference in pelvic failure rates between the 2 dose levels irrespective of stage and differentiation, but for T3 poorly differentiated tumors, a higher dose was useful. However, this group of patients was treated with RT alone with low doses (64 Gy) to the prostate without hormone therapy. 21 The RTOG 9413 have used 50.4 Gy in 1.8 Gy per fraction, and Urogenital tumour study group (GETUG) trial have used 46 Gy in 2 Gy per fraction. 6,7 In both trials, the pelvic failure rates were low (8%-9.5%). Moreover, concurrent androgen deprivation is known to have a radiosensitizing effect on the primary. 22,23 Extrapolating this to the nodes, and based on the above data, it is likely that incidental dose of about 36 to 40 Gy received by the obturator region in the present study may be adequate in eradicating microscopic disease.
In the RTOG 9413, the prostate-only RT included the prostate and the seminal vesicles with an unblocked field size of 11 × 11 cm. Fields covering the true pelvis called as mini-pelvis are often thought to be adequate with the premise that extensive nodal involvement is unlikely to benefit from larger fields. 24 In GETUG trial, 3D plans with 4 field techniques using shielded blocks or MLC were made for prostate-only RT, with CTV encompassing prostate and seminal vesicles with a 1-cm expansion given for PTV. 7 In both trials, it is likely that the portals would have covered the obturator nodes and partially the internal iliac and external iliac nodes. The more recent ongoing trials (RTOG 0924, MRC-PIVOTAL trial, and the Indian POP-RT) testing the role of elective pelvic nodal irradiation use highly conformal techniques like IMRT resulting in much less incidental doses (based on the present data, approximately 21 Gy) to the obturator lymph node, which may not be enough to sterilize microscopic disease. If the hypothesis of incidental dose influencing microscopic disease is correct, these trials, in time, may show a benefit favoring pelvic nodal irradiation.
Being a dosimetric study, the present work is limited by a relatively small number of patients but possibly adequate as a proof-of-concept study. In addition, while the lymph node regions were delineated with RTOG GU consensus atlas for pelvic lymph nodes, it is possible to delineate the nodes in different ways leading to different doses in these regions. 25 This is, however, unlikely to affect the dose in these regions significantly. Interestingly, the sentinel node studies indicate that the entire lymph node area may not be relevant and the nodes were found to cluster around bifurcation of external and internal iliac arteries, thus involving parts of obturator fossa, internal iliac, and external iliac regions. 18 This will also affect the results when using fixed volumes for different lymph node regions.
Conclusion
The incidental dose received by obturator nodes is clinically significant especially with 2D and 3D techniques, possibly enough to influence micrometastatic disease. However, with IMRT, this dose is lesser, and this incidental dose may be less important in the current trials evaluating elective nodal irradiation in prostate cancer. Dose to other nodal regions is small and not clinically relevant with any technique.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.